Author's Note
The Men and Women Who Built an Institution
Every institution has two histories. One is written in annual reports and official records. The other lives in the memories of those who taught, healed, discovered, mentored and led — and that history is the more fragile of the two, for it dies with the people who carry it.
This website is an attempt to save it.
Architects of MGIMS is a tribute to the men and women who laid the foundations of the Mahatma Gandhi Institute of Medical Sciences, Sevagram. They came from every part of India, and chose to spend the most productive years of their lives on an audacious experiment: building a world-class medical college in the small village where Gandhi had lived and worked.
Some became teachers whose influence outlasted their classrooms. Others built departments that would go on to earn national reputations. Many simply gave decades of quiet, competent service to their patients and their students. Together, they turned an idea into one of India's most respected medical institutions.
When Gandhi made Sevagram his home in 1936, he turned an obscure village into a place of national significance. Here he refined his philosophy of truth, self-reliance and service — convinced that India's future would be shaped in its villages, not its cities.
Dr. Sushila Nayar, a physician, freedom fighter and one of Gandhi's closest associates, shared that conviction. Sevagram already had Kasturba Hospital, built to serve the surrounding villages. But Dr. Nayar imagined something bolder still: a medical college that would combine scientific rigour with rural service, and modern medicine with Gandhian values.
Many called the idea impractical. Why build a medical college in a remote village? Would good teachers leave the cities for it? Would good students choose it? Could it ever be excellent?
In 1969, MGIMS opened its doors as India's first rural medical college — an experiment in the belief that excellence and social commitment could strengthen each other rather than compete. More than five decades later, that experiment still stands.
A great institution is often remembered by its buildings — the lecture theatres, the laboratories, the wards where lives were saved. But bricks do not create excellence. They acquire meaning only when animated by people.
Those who came to Sevagram in its early years found little to make the choice easy: modest infrastructure, scarce resources, professional isolation, better offers elsewhere. Many stayed anyway, believing they were building something larger than a career — and that medicine was a vocation, not merely a profession.
The institution that stands today is the sum of those decisions.
This archive follows the visionaries whose ideals shaped MGIMS, the founders who built it, and the deans, principals and department heads who steered its growth. It honours the clinicians, surgeons and teachers whose classrooms and operating theatres shaped generations of doctors.
It also records those who rarely appear in official histories: the nurses, laboratory scientists, librarians, administrators and support staff whose daily work kept the institution running. Their names are not always in the textbooks. Their contribution was no smaller for that.
Together, these lives built something beyond departments and services — a culture that valued intellectual honesty, clinical excellence and respect for every patient, regardless of means.
Each biography here is a chapter in a larger story: how one rural institution, against considerable odds, became one of India's finest.
If you studied, taught, worked or received care at MGIMS, you are part of this story. I invite you to share photographs, letters, memoirs and recollections from its early years — each one preserves a voice that would otherwise be lost.
The buildings across the Sevagram campus mark the institute's growth. Its true architecture lies elsewhere — in the people whose lives gave its ideals lasting form. This website is dedicated to them.
Contents
Dr. Sushila Nayar
DrPH, Johns Hopkins University, USA (1950)

Dr Sushila Nayar (1914–2001) was the physician who turned a Gandhian village experiment into one of India’s most influential rural medical institutions. Personal doctor to Mahatma Gandhi, Union Health Minister, and founder‑director of MGIMS, she spent a lifetime proving that modern medicine and social justice could walk together.
In the winter of 1938, a twenty‑four‑year‑old woman stepped off a train at Sevagram clutching a stethoscope, a blood pressure cuff, and a single drug—reserpine. She had barely finished her MBBS; her clinical experience was thin, her confidence still tentative. Dr. B.C. Roy, personal physician to Mahatma Gandhi, had sent her to monitor the most important man in India through a dangerous spike in blood pressure—an assignment he could just as easily have given to more seasoned doctors.
Why he chose her, history does not record. But she went, taking a month’s leave from her studies in Calcutta, with no one at hand to brief her, no senior colleague to lean on, no phone line to call back if things went wrong. In that remote village, cut off from the comforts and certainties of the city, she was suddenly on her own. That month stretched into two years.
She was Sushila Nayar — doctor, freedom fighter, cabinet minister, institution builder. She would return to Sevagram again and again across six decades, drawn back each time by the same conviction: that medicine's truest work happened not in city hospitals but in villages, not in lecture theatres but in the houses of the poor. When she died on January 3, 2001, the day after her 86th birthday, she had spent the better part of her life making that conviction into brick, mortar, and a living institution.
Sushila was born on December 26, 1914, in Kunjah, a small town in the Gujarat district of West Punjab — a place now part of Pakistan. Her father was a judge in the Punjab Civil Service. Her brother Pyarelal, fifteen years her senior, would become Gandhi's personal secretary, the closest of confidants, the man who would spend his life recording the Mahatma's words. It was through Pyarelal that Sushila's path first crossed Gandhi's — briefly, when she was six years old, during his Punjab tour after the launch of the Non-Cooperation Movement in 1920.
She came to medicine almost by accident. On a childhood train journey, a lady doctor asked what she wanted to be. Sushila answered carelessly, the way children do: a doctor. The family laughed at the innocent remark. Then she went and became one.
She completed her schooling in Lahore, enrolled at Lahore College for Women, and eventually made her way to Lady Hardinge Medical College in Delhi — the institution whose foundation stone had been laid in 1914, the very year of her birth. She graduated in 1936. She was twenty-two.
After graduation, she joined the All-India Institute of Hygiene and Public Health in Calcutta for further studies. It was there that Dr. B.C. Roy found her and sent her to Sevagram to care for Gandhi.
Wardha in those years was plagued by malaria. Every monsoon, fevers swept through households, through the ashram, through the surrounding villages. Temperatures climbed past 102 degrees. Patients needed a week of careful nursing before they could stand. Natural treatments were tried — mud packings on the forehead and abdomen, enemas — alongside whatever medicines she had brought. She worked alongside Prabhakarji, an old ashramite who went about in a short dhoti and cared for patients with the quiet devotion of someone who had chosen simplicity as a philosophy. Together, they set up a small dispensary in one of the ashram's rooms: a microscope, disinfectants, a few medicines, a willingness to learn.
Patients came. More followed.
Then cholera broke out in the surrounding villages. Gandhi told her simply: treat the village as the hospital and the houses as the wards. She was twenty-five, alone, without colleagues to consult or seniors to guide her. The experience taught her something that no textbook had: that curative medicine was the door through which you earned a village's trust, and that once you had their trust, you could speak to them about prevention. The two could not be separated. It was a lesson she would spend the rest of her life teaching others.
She remained in Sevagram for nearly two years before returning to Lady Hardinge as a registrar to pursue postgraduate studies. In 1942, she completed her MD in Medicine.
On August 9, 1942, Sushila Nayar was arrested in Bombay. Three days later, she was transported with Gandhi, Kasturba, and other Congress leaders to the Aga Khan Palace in Pune. She would spend twenty-one months there.
In the palace, she was doctor to everyone — to Gandhi, to Kasturba, to Mahadev Desai who died of a heart attack on August 15, 1942, just days after their arrival. She attended to sixty prisoners from Yerwada jail who tended the palace gardens. She treated the police officers standing guard. She nursed Kasturba through the bronchitis that worsened through that long detention until, on February 22, 1944, it killed her. She stayed with Gandhi through severe malaria that left his kidneys damaged.
When they were finally released on May 6, 1944, Sushila emerged from the palace with something that could not be taught in any institution: the knowledge of how human beings behave under extreme conditions, what they need from a doctor, and what a doctor must be willing to give.
After Gandhi's assassination on January 30, 1948, Sushila did what she had always done when grief threatened paralysis — she went back to work. A WHO scholarship took her to the Johns Hopkins School of Hygiene and Public Health in Baltimore. She had planned to specialize in cardiology. Her professors persuaded her otherwise: India needed public health specialists, not more cardiologists. She stayed on, completing a master's degree and then a doctorate.
When her funds ran out in the final months, providence intervened in a characteristically unlikely form. The Quakers, moved by her dedication, invited her on a speaking tour across the United States. For two and a half months she traveled the length of the country, speaking about Gandhi, about India, about what she had witnessed. The honorarium she received — perhaps five hundred dollars, perhaps a thousand, she was never quite sure — was enough to complete her studies, visit Europe, and return home.
She arrived back in India in 1950 ready to rebuild Kasturba Hospital, the small institution she had helped establish in Sevagram. Instead, she found that those managing the hospital had quietly accepted her resignation — a resignation she had never submitted. The mystery was never resolved. She accepted the decision without bitterness. "Bapu had taught us," she said, "that the field of service is as large as the Earth itself, and that it is not necessary to rub shoulders."
She took up the post of Chief Medical Officer at Badshah Khan Hospital near Faridabad, worked in surrounding villages, started a tuberculosis wing in tents. Then came politics. She won a Delhi assembly seat in 1952, became Delhi's Health Minister, entered Parliament in 1957, and from 1962 to 1967 served as India's Union Minister for Health — one of the few women in Nehru's cabinet, responsible for the health of four hundred million people.
In 1964, two visitors arrived at her Delhi office and refused to leave. Manimala Chaudhary, then matron of Kasturba Hospital, and Dr. Anant Ranade, the hospital's young medical officer, had traveled from Sevagram with a specific purpose. Gandhi Smarak Nidhi, which had been managing Kasturba Hospital, wanted to hand it over to the government. The workers did not want that. They wanted Sushila Nayar.
"You must not refuse to help," they told her.
She didn't. On September 11, 1964, the Kasturba Health Society was registered in Nagpur, with Sushila Nayar as its president. The founding trustees were a small, faithful group: Manimala Chaudhary, Anant Ranade, Nalinbhai Mehta, Raghunath Dhotre, Shriman Narayan and Secretary Gandhi Smarak Nidhi who had kept the hospital alive through years of uncertainty. The Gandhi Smarak Nidhi transferred the hospital's management and an endowment of ten lakh rupees to the new society.
The first rural medical college in India was beginning to take shape on the horizon.

The idea had been forming for years. As Health Minister, she had confronted an arithmetic of failure: five thousand primary health centres across India sat without doctors, while ten thousand new graduates emerged from medical colleges every year. The graduates would not go to villages. They had been trained in cities, for cities. What if, she reasoned, you trained them in a village from the start — in the dust and heat and reality of rural India?
Prime Minister Lal Bahadur Shastri heard her out in 1965 and agreed. Chief Minister Vasantrao Naik agreed. They visited Sevagram and approved the site. Then Shastri died. Naik lost power. The project stalled.
She persisted. For three years she navigated ministries, state governments, and funding committees. On August 8, 1968, Deputy Prime Minister Morarji Desai convened a meeting that finally produced a formula: fifty percent of costs from the central government, twenty-five percent from Maharashtra, twenty-five percent from the Kasturba Health Society. Her share came to one crore rupees. She had no idea where it would come from.
An old ashramite named Anant Ram laughed when she worried aloud one evening. Upar Wala deta hai to chappar phad ke deta hai, he said. God gives, and when He gives, He breaks through the roof.
The next morning, a health ministry official told her about a USAID fund looking to support developmental projects in India. Too much of the money was going to Christian organisations, he noted. Why not apply? She applied for two crores, expecting to receive one. They sanctioned two.
On August 12, 1969 — Gandhi's centenary year — the first batch of sixty students was admitted to the Mahatma Gandhi Institute of Medical Sciences, Sevagram. The old Kasturba Hospital, founded in 1945, its walls repaired and rooms repurposed, became the heart of the new institution. The GD Birla guest house that had once hosted dignitaries now contained the dissection hall, the laboratories, the labour room, the operation theatre, and the library, all within its modest walls.
There was resistance from the village. Locals objected to dissecting frogs in Gandhi's Sevagram. Vinoba Bhave, who lived at Pavnar nearby, stepped in and gently explained that if this was to be Gandhi's medical college, it must have everything modern medicine required. The dissections continued.

She recruited faculty with the same directness she applied to everything. Using her connections at AIIMS and PGI Chandigarh, she invited distinguished physicians to visit Sevagram and then persuaded some to stay. She secured deputation of faculty from Nagpur's Government Medical College — Dr. ML Sharma, Dr. RV Agrawal, Dr. K.N. Ingle, Dr. MD Khapre, Dr. GM Indurkar among them. On a train journey back from Delhi, she encountered Professor PS Vaishwanar, head of Physiology at Government Medical College Nagpur, and recruited his help before they reached their destination.
She brought faculty from across the country — north and south, east and west — deliberately, insisting that MGIMS would transcend barriers of caste, language, and community. The early salaries were modest, lower than government medical colleges, and it took years to bring them to parity. People came anyway.
The institution she designed reflected everything she had learned since that first year in Sevagram. Every student spent two weeks in Gandhi's Ashram after admission — learning to live simply, to work with their hands, to know the village before they knew the hospital. Community medicine was renamed from Preventive and Social Medicine, not merely as a semantic change but as a philosophical one: the community was not a subject, it was the patient. Health insurance, first collected in jowar grain from bullock carts traveling village lanes, was formalised into a scheme that covered thousands of rural families for an annual premium that began at six rupees.
She required graduates to serve two years in villages before qualifying for postgraduate studies at MGIMS. She prohibited meat on campus. She attended evening prayers and expected others to. She wore khadi.
Students sometimes found her code difficult. They appreciated the orientation camps and village postings but struggled with the khadi, the shramdan, the prayers. She remained unmoved. Her consistency between belief and action was, those who worked with her agreed, without parallel.

In 1995, she suffered a myocardial infarction. Congestive heart failure and osteoarthritis followed, severely limiting her mobility. Most people would have withdrawn. She did not. She continued working, continued thinking, continued implementing. At eighty-six, she accepted the chancellorship of Gujarat Vidyapeeth and promptly set about resolving the problems that had paralysed the institution.
She was deeply influenced by Gandhi's enumeration of seven deadly sins — commerce without ethics, pleasure without conscience, politics without principle, knowledge without character, science without humanity, wealth without work, worship without sacrifice. She did not cite them as abstractions. She used them as a diagnostic tool, holding institutions and individuals up to each one in turn.
She was also a gifted writer. She completed several volumes of the unfinished biography of Mahatma Gandhi that her brother Pyarelal had left incomplete. Her own book on Gandhi's imprisonment remains a precise and moving account. Those who heard her speak remembered a voice they called majestic — warm, authoritative, lit by a natural wit that made even difficult truths easier to receive.
Her relationship with Indira Gandhi, once close as sisters, fractured irreparably over the political manoeuvres around the 1969 presidential election. She never reconciled herself to it. She was capable of absolute loyalty and, when she felt that loyalty betrayed, absolute distance.
She endured five years after her heart attack, dying on January 3, 2001—just a week after her 86th birthday—at Prerna Kutir, her Sevagram home, encircled by those she had devoted her life to. As former Union Health Minister and founder-director of a medical college, she could have summoned the nation's top cardiologists from AIIMS, PGI, or elite corporate sanctuaries. Yet she entrusted herself wholly to her Sevagram colleagues, heeding only Dr. A.P. Jain—a Professor of Medicine, not a specialist—for those years, without a whisper of doubt or second opinion. Decades before "palliative care" entered the medical lexicon, she embraced death with profound dignity: no ICU's sterile chill, but the warmth of home and loved ones. In her final breath, not a millimeter divided her convictions from her life.
The institution she founded now serves a thousand villages, trains hundreds of doctors each year, and carries her name in everything it does — in its rural orientation, its community health programme, its insurance scheme, its insistence that medicine is not merely a profession but a form of service. She did not build MGIMS as a monument to Gandhi. She built it as a continuation of his work, the most durable kind of memorial: one that keeps doing things.
| 1914 | Born, 26 December, Kunjah, West Punjab |
| 1936 | Graduated MBBS, Lady Hardinge Medical College, Delhi |
| 1938 | Arrived Sevagram — sent by Dr. B.C. Roy to care for Gandhi, aged twenty-four |
| 1942 | Completed MD in Medicine, Lady Hardinge Medical College |
| 1942 | Arrested, 9 August — imprisoned at Aga Khan Palace, Pune |
| 1944 | Released, 6 May — after twenty-one months |
| 1948 | WHO scholarship — Johns Hopkins School of Hygiene and Public Health, Baltimore |
| 1950 | Returned to India with DrPH from Johns Hopkins |
| 1952 | Elected to Delhi Legislative Assembly |
| 1957 | Elected to Parliament |
| 1962 | Appointed Union Minister for Health, Government of India |
| 1964 | Kasturba Health Society registered, 11 September, Nagpur |
| 1969 | MGIMS admitted its first batch of fifty students, 12 August |
| 1995 | Suffered myocardial infarction — continued working |
| 2001 | Died, 3 January, Prerna Kutir, Sevagram — aged 86 |
A Study of post vaccination tuberculin reactions in relation to nutritional status in young children Pujai village
A study of Frontline workers and health cooperative in health delivery.
Weight gain in pregnancy
Nutritional Status of Primary School Children
Prevalence of pulmonary tuberculosis in the rural area around Sevagram
Prevalence of ocular morbidity in preschool and school going children around Sevagram
Measurement of clinical bacteriological response of leprosy patients to multidrug regimen in Wardha district
A study and evaluation of the existing pattern of health care delivery system in 3 representative villages of the primary health centre Talegaon (taluka) in Wardha district
Tuberculosis in nursing students of Kasturba Nursing School
An epidemiological study of endemic goiter in district Wardha
Epidemiologic study of deformities in leprosy in around Sevagram rural area
Assessment of Nutritional Status of Preschool Children
Epidemiology of respiratory tract infections in symptomatic suspected of pulmonary TB In urban rural area in Wardha
Study of medico social problems of elderly old people residing in a rural area of Wardha district
Prospective study of neurological deformities in leprosy with special reference to drugs their neurotoxicity
An epidemiologic study of defaulters among the short term intermittent chemotherapy of sputum positive cases of pulmonary tuberculosis in Wardha district
Prevalence of anemia of pregnancy role of iron folic acid as a prophylactic measures
Study of the determinants of birthweight in rural semi urban communities
An epidemiological study of pediatric dermatoses ( 0 -14 yrs) in a rural community
An epidemiological study of orodental diseases among school children in rural area of Wardha districts
Determination of fetal birth weight by ultrasound and its correlations with actual birth weight
An epidemiological study of xerophthalmia in preschool children in rural area Wardha dist.
A Study of Ocular Morbidity in the Elderly Population in Rural Areas Of Wardha District
Study of various parameters of water analysis in and around Sevagram Wardha
Knowledge, attitudes practice of breastfeeding in rural community
Study of health status of employees of KHS students of MGIMS Sevagram
Longitudinal study of acute respiratory infections in rural area among under 5 children
A descriptive study of Orthopaedics problems in rural adult population
Study of effect of maternal health on birth weight health of infant
An epidemiological study of low birth weight
Dhirubhai Mehta
B.Com (Sydenham College, Mumbai) [1957]
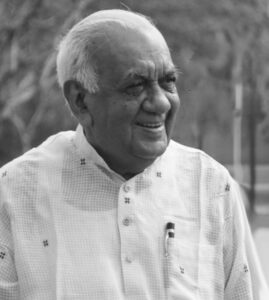
President, Kasturba Health Society · Chartered Accountant · Gandhian · The Last of the Founding Generation
"When Dr. Sushila Nayar met me in the summer of 1982 and asked me to oversee MGIMS, I was taken aback. I didn't even know how to pronounce the names of half the departments, let alone understand what they did."
He said this often, and with his characteristic candor — half laughing at the improbability of it, half genuinely awed by the chain of events that had led a seasoned corporate chartered accountant from Bombay to a rural medical college in Wardha. It was, by any reckoning, an unlikely appointment. And yet Dhirubhai Mehta spent the next four decades proving it was exactly the right one.
He died on April 22, 2024, in Bombay Hospital, forty-eight hours after being admitted for what they thought was viral pneumonia. He was eighty-seven. His son Nirad and daughter Maitri were beside him. Five days short of his eighty-eighth birthday, he was gone — and with him closed the last chapter of the founding generation of MGIMS.
Dhirubhai was born on April 27, 1936, in Songath, a small village in Gujarat's Bhavnagar district. His father Shantilal was a schoolteacher at Gurukul High School — an Arya Samaj institution — the first in his village to have passed matriculation, struggling to support nine children on a teacher's salary. Eventually, Bombay beckoned. Shantilal left the family behind, found work at the stock exchange, switched to accounting at a trading firm, saved every rupee, and gradually built enough security to move the family to a small apartment in Borivali.
His mother Savitaben had studied only to fourth standard, was engaged at five and married at thirteen. But she was, as Dhirubhai always maintained, no ordinary rural woman. When her daughter's marriage began to fail within a year, Savitaben — in a time and place where divorce was taboo and family honour paramount — told her daughter to walk away. Choose dignity over tradition. It was a kind of courage that Dhirubhai never forgot and tried, in his own fashion, to replicate.
He schooled in Gujarati medium, moved to Borivali for high school, and chose Sydenham College of Commerce and Economics in Churchgate for his degree — drawn partly by its prestige and partly, he admitted, by the fact that it spared him Zoology. He could not bear dissections. The irony of spending four decades at a medical college was not lost on him.
He graduated in 1957, began his three-year articleship at a firm in Fort, tutored students and took part-time work to fund his studies, and in 1961 cleared the Chartered Accountancy examination on his first attempt before turning twenty-five. He was India's 5,635th Chartered Accountant. He wore it lightly but earned it without shortcuts.
As a teenager, while peers chased fashion, Dhirubhai chose khadi. Not as an ideology performance — as a settled conviction. He opened khadi shops in Borivali. He caught the attention of Vaikunthbhai Mehta, walked into rooms where Dada Dharmadhikari and Narayan Desai spoke, and found his Gandhian formation alongside his commercial one.
After qualifying, he navigated three companies before joining the Bajaj Group in 1966 — the year he also married Nandini Bajaj, daughter of Radhakrishnaji Bajaj and granddaughter of Shrikrishnadas Jajoo, the revered freedom fighter and Gandhian leader. She was fluent in Hindi, Marathi, Marwari, and English, educated across Wardha, Banaras, and Lucknow. The marriage connected him to Wardha in ways that would prove consequential.
At Bajaj Auto, he rose steadily. Sharp in finance, investment, and taxation, he earned the trust of Kamalnayan, Ramakrishna, and Rahul Bajaj over two decades. In the early 1970s, he played a pivotal role in the Bajaj-Piaggio legal battle over the Vespa scooter. He held directorships beyond Bajaj, advised regulatory bodies, and served on committees shaping transparency and corporate governance at SEBI, CII, and FICCI.
During the Emergency of 1975, he stood with Jayaprakash Narayan at personal and financial risk — funding and sustaining the movement while thousands were jailed. He admired Vinoba Bhave but wrote him blunt letters questioning his support for the Emergency, which Vinoba had called a Festival of Discipline. Dhirubhai called it India's darkest hour. He was not a man who moderated his views for the sake of comfort, even when the person on the other end was someone he revered.
At fifty, with a successful corporate career available to him for however long he wanted it, he walked away.
"It wasn't easy," he later said. "Nirad and Maitri were still studying. Nirad had his sights set on top American universities — an expensive dream. But my family stood by me." His children both became chartered accountants. "Must be in the genes," he would say, "but they did it on their own — without ever asking for help."
Until 1982, Dhirubhai Mehta and Dr. Sushila Nayar had never met.
The connection was made by Sarla Parekh, who had managed MGIMS's finances for years and watched the institution's funding position worsen through the late 1970s. She had known Dhirubhai for decades, admired his financial acumen and his Gandhian instincts, and heard that he was leaving Bajaj Auto. She went to Dr. Nayar. Why not bring Dhirubhai to Sevagram?
Nalinibhai Mehta and Tapdiya arranged a lunch. Dr. Nayar and Dhirubhai met. Conversations turned into shared visions. What began as an introduction became a calling.
He was already familiar with Wardha — his wife's family was from there, the Bajaj Group had deep roots in the district. But familiarity with a place and choosing to give your working life to it are different things. He chose. He joined the Kasturba Health Society's governing board, began visiting Sevagram regularly, and started the long process of understanding an institution whose departments he still couldn't pronounce.
He never sought to overshadow Dr. Nayar. Where others with his corporate background might have arrived with a mandate for transformation, he arrived with humility. He worked quietly, offered his expertise where it was useful, and deferred to her vision without resentment. She, in turn, recognised what he offered — not just financial acumen but integrity, and the particular authority of a man who had no personal stake in the institution's money.
"She shaped the institution's ideals," those who watched them work together said. "He secured its foundation."
By the late 1990s, as Dr. Nayar's health declined after her heart attack, she had ceded almost all operational authority to Dhirubhai. When she died on January 3, 2001, the governing body of the Kasturba Health Society looked to no one else.
He inherited an institution built on Gandhian ideals in a landscape that was changing fast around it. Private medical colleges were multiplying. For-profit hospitals were appearing near Sevagram. The commercial logic of Indian healthcare was encroaching from every direction. Dhirubhai's task — the task he set himself — was to hold the line.
He held it.
MGIMS under his presidency cut ties with the pharmaceutical industry — a decision that alarmed many who feared the resulting loss of revenue. The money did not dry up. The institution's ethical standing strengthened. He was not a man who governed by committee consensus; he made decisions and stood behind them.
The infrastructure he built across those twenty-three years was substantial: trauma centres, ICUs, a Cath Lab, dialysis units, a de-addiction centre, a mother and child centre, a palliative care unit, proper hostels for students and residents. A low-cost drug initiative that made treatment affordable for patients who had previously struggled to buy medicines. A unit for abandoned newborns. Healthcare outreach into Melghat — the tribal Korku Adivasi communities in the Satpura hills, where malnutrition and neglect had long gone unaddressed. He secured five crore rupees for the Melghat centre, went there himself on visits that were not for show, and stood behind the doctors and nurses on the ground when the work became difficult.
He brought distinguished academics onto the KHS board, wanting MGIMS to develop not just clinical excellence but scientific temper. He strengthened community medicine. He ensured every incoming batch of students underwent the Gandhi Ashram orientation — waking before dawn for prayers, cleaning, spinning yarn, learning service before they learned surgery. This mattered to him not as ritual but as formation.
Every month, he visited Sevagram. He walked the campus. He kept his door open. He drank tea with anyone who came. His wit was quick, his stories effortless, his ability to put people at ease genuine. He saw no hierarchy worth maintaining in casual human encounter.
He was not without flaws, and a portrait that ignored them would do him a disservice.
He was susceptible to sycophancy — could be quick to form attachments to those who flattered him, sometimes misjudging people whose charm exceeded their reliability. He enjoyed dropping names — Vinoba Bhave, Jayaprakash Narayan, ministers, bureaucrats — and in his later years these stories became a refrain, repeated with a frequency that those close to him recognised but could not always redirect. As president, he had a mandate to guide and preach, and he used it with an enthusiasm that occasionally crossed into self-righteousness.
He relished the role. The access it provided, the visitors it brought, the influence it carried — he was not indifferent to any of it. And he struggled, as his final years arrived and memory began to soften his grip on administration, to do what every leader must eventually do: identify a successor and let go. He could not, or would not. He held the chair into his late eighties, when the institution needed something different from what he could still offer.
These are not small failings in a man who led an institution for twenty-three years. They should be recorded alongside his achievements, because an honest portrait serves memory better than a hagiography, and because Dhirubhai himself — who never softened the truth to spare someone's comfort — would have expected no less.
What he was not, and never became, was corrupt. In a landscape where institutional leadership and personal enrichment so often moved together, Dhirubhai remained untouched. He donated crores to MGIMS quietly, without fanfare. The house he built on campus — his home in Sevagram for decades — he willed to the institution. He left no wealth extracted from the place. He left the place better than he found it.
"All I want," he once said, "is for MGIMS to offer quality education and healthcare that everyone can afford."
One sentence. His life's work in it.
His wife Nandini died in August 2022. He grieved, and kept going. MGIMS meetings continued. Plans moved forward. On April 20, 2024, he was admitted to Bombay Hospital with what appeared to be viral pneumonia. Forty-eight hours later, on April 22, he was gone.
He had given forty years to Sevagram — more than half his life. He had arrived not knowing how to pronounce the departments. He left having built some of them.
In the 2001 MGIMS bulletin, written when he first assumed the presidency, Dr. S.P. Kalantri wrote of the responsibility Dhirubhai was taking on — to uphold Dr. Sushila Nayar's legacy, to keep the bright torch of MGIMS aloft, undimmed and untarnished, ensuring its light reached the poorest of the poor.
He kept it. Not perfectly — no one does — but faithfully, and with an integrity that the institution will measure its future leaders against for a long time to come.
| 1936 | Born, 27 April, Songath, Gujarat |
| 1957 | Graduates, Sydenham College of Commerce |
| 1961 | Clears CA examination — India’s 5,635th CA |
| 1966 | Joins Bajaj Group — rises over two decades |
| 1966 | Marries Nandini Bajaj — granddaughter of Shrikrishnadas Jajoo |
| 1975 | Stands with Jayaprakash Narayan during the Emergency |
| 1982 | Nalinibhai Mehta arranges lunch with Dr. Sushila Nayar |
| 1982 | Joins KHS governing board — begins visiting Sevagram |
| 1990 | Vice President, then President, Kasturba Health Society |
| 2001 | Dr. Sushila Nayar dies — Dhirubhai assumes full presidency |
| 2001 | Severs institutional ties with pharmaceutical industry |
| 2001 | Donates home on campus to MGIMS in his will |
| 2022 | Nandini dies, August — he grieves and keeps going |
| 2024 | Dies 22 April, Bombay Hospital — five days short of 88th birthday |
P.L. Tapdiya
Chartered Accountant (ICAI) [1967]

President, Kasturba Health Society
In the winter of 1966, the world of Indian finance was a kingdom of polished leather, starched collars, and an unspoken code of urban elitism. Into this world stepped Parmanand Tapdiya, a twenty-one-year-old who had just performed a feat of intellectual levitation: clearing the final Chartered Accountancy examinations on his first attempt. For a boy from Pimpalkhuta, a village so obscure it seemed to defy cartography, this was not merely a result; it was a miracle.
However, the "Everest of exams" was only the first gate. The second was aesthetic. To join the prestigious firm of K.K. Mankeshwar & Co. in Nagpur, Tapdiya was told he must abandon his rural attire. No pyjamas, no loose shirts. The firm, steeped in British professional tradition, demanded a visual manifestation of competence. Tapdiya, whose pockets were as empty as his ledgers were precise, had to borrow fifty rupees—a significant sum at the time—to buy his first pair of trousers.
This borrowed suit was more than a change of clothes; it was a uniform of a new life. It marked the birth of a man who would spend the next six decades ensuring that the grand, sprawling dreams of Sevagram were properly clothed in financial reality. While others in the Mahatma’s shadow spoke of grand visions and spiritual missions, Tapdiya understood a fundamental truth: even the most selfless institution requires a balanced balance sheet to survive the friction of the real world.
To understand the President, one must understand the absolute silence of Wai—a village thirty kilometers south of Akola that in the 1950s lacked electricity, a post office, and a sense of belonging to the modern world. Here, Tapdiya learned what we might call the "mathematics of scarcity." Water was not a utility; it was a hard-won prize from two shared wells where humans and livestock drank in a communal struggle for survival.
Strachey often looked for the moment a character’s "inner steel" was forged. For Tapdiya, it was the kerosene lamp. In the total darkness of rural Maharashtra, that small, flickering flame was his only ally against the night. It was here he learned his mother Dhanibai’s first commandment: Trust numbers, not guesswork. Unlettered and widowed when Parmanand was only two, she possessed a visceral understanding of accountability. She knew that in poverty, a single miscalculated paisa could lead to hunger.
By the age of fifteen, Tapdiya had ranked 24th out of 325,000 students. He was a boy moving at the speed of light in a world of mud paths. Yet, misfortune was his constant companion. Mentors like Principal Javadekar and Radha Krishnaji Toshniwal would enter his life, offer a glimpse of hope, and then be snatched away by death. These early losses created a man who did not rely on the permanence of people, but on the permanence of principles. He chose the CA path—where only one in fifty survived—not for the wealth it promised, but for the order it imposed on a chaotic world.
The collision between the formidable Dr. Sushila Nayar and the nineteen-year-old intern Tapdiya in 1965 is the foundational myth of the MGIMS accounts department. Dr. Nayar was a colossus—a Gandhian revolutionary, a close associate of the Mahatma, and India’s Health Minister. She possessed an iron will and a visionary’s impatience. She had a British consultant’s report from Parsons and Company filled with dense, foreign projections for her proposed rural medical college.
She needed this report translated—not just into Indian rupees, but into the myriad languages of global donors: Yen for Japan, Lira for Italy, and Dollars for the United States. Tapdiya, the intern, was assigned the task. He sat in a modest room with a stone floor and a kavelu (tiled) roof. Without a calculator, without a spreadsheet, and with no formal degree yet to his name, he manually converted the lifeblood of the future MGIMS.
He was the "Human Computer" of Sevagram. He didn't just translate currencies; he translated Dr. Nayar’s fierce drive into a 150-page document that the Vatican and the Japanese could understand. He typed and retyped drafts late into the night, the rhythmic clatter of the typewriter echoing the heartbeat of an institution yet to be born. When he finally cleared his exams in 1969, the "corporate czars" of Mumbai and Delhi came calling. They offered the prestige of the metropolis; they offered the fast track. Tapdiya looked at the corridors of power and then looked back at the dusty road to Sevagram. He chose the latter, becoming an honorary consultant—a man who would manage millions without ever drawing a salary.
The early 1970s at MGIMS were a period of "Primitive Accumulation." The accounts department bore no resemblance to the clinical, digital hubs of today. It resembled a scene from a R.K. Narayan novel—a small, dedicated group working in a world of paper and ink. There was Tapdiya, the young, sharp mentor, and a trio of unlikely disciples: Dadarao Shingare, Bhimrao Pradhan, and a man known simply as Kanakdas.
The story of Kanakdas is essential to the Stracheyan narrative of MGIMS. He was a wanderer from Kerala who had stepped off a train at Wardha, penniless and searching for food. Manimala Choudhary had noticed him and given him a bell to ring to mark the hours. From ringer of bells to Chief Accountant, Kanakdas’s journey was overseen by Tapdiya.
None of these men had studied beyond the tenth grade. None had formal training in finance. Yet, under Tapdiya’s tutelage, they became the "Guardians of the Paisa." They worked with Remington typewriters and red pens, mastering the art of the ledger through sheer, dogged perseverance. In this Zen-like austerity, Tapdiya instilled a philosophy: Money is not currency; it is lifeblood. To misplace a single rupee was to bleed the institution. He taught them that in a rural hospital, a ledger entry was as vital as a surgeon's knot.
In an era where educated grooms—particularly Chartered Accountants—were traded like blue-chip stocks, Tapdiya staged his most quiet and significant rebellion. As families lined up with lucrative dowry proposals, he made a stance that was unequivocally Stracheyan in its rejection of social vanity. He declared he would only marry into a family that could not afford a dowry.
Wealth held no appeal; status meant nothing. He sought a partner whose convictions matched his own "unyielding steel." In 1969, he married Shobha Rathi in a ceremony that was a study in minimalist integrity. No gold, no lavish feast—just a coconut and a rupee.
Shobha, a scholar of Sanskrit and Political Science, became the silent partner in his mission. While he built the financial scaffolding of a medical college, she built a home that remained stubbornly simple. Their three children—Mugdha, Vaibhav, and Sourabh—grew up in an environment where "value" was measured in character, not in bank balances. This personal domestic "audit" ensured that Tapdiya remained unencumbered by the greed that often fells men in positions of financial power.
The Tapdiya of the 1980s and 90s was not the mellowed elder we see today. He was described by colleagues as impatient, tough, and at times, unyielding. He was the "Grand Inquisitor" of the balance sheet. In a Gandhian institution where "service" could sometimes be used as an excuse for administrative sloppiness, Tapdiya was the corrective force.
He called a spade a spade, and if the spade was over-budget, he was merciless. He set a standard of perfection that few could meet. This "toughness" was not a character flaw; it was a strategic necessity. For thirty-one years, he served as the internal auditor, a hawk-like presence that saw through every inflated estimate and every misplaced expense.
Yet, as the decades passed, a transformation occurred—the "surgical" biographer’s favorite theme. The man who once demanded perfection began to practice patience. He learned to bend without breaking. He realized that to lead a community of doctors and teachers, one had to lead with the heart as much as the calculator. He shed the sharp edges of the auditor for the steady hand of the trustee.
When Tapdiya took the baton as President of the Kasturba Health Society in 2024, at the age of seventy-seven, he was the third runner in a sixty-year relay. Dr. Sushila Nayar had been the Architect; Dhirubhai Mehta had been the Builder; Tapdiya became the Custodian.
The transition was not merely a change in name, but a change in "class." Dr. Nayar was a political giant; Dhirubhai was a corporate titan. Tapdiya was, as he called himself, a "homespun" professional. He had neither political backing in Delhi nor a corporate network in Mumbai. He was a "Son of the Soil," rooted in the realities of Wardha.
He inherited an institution facing unprecedented challenges. The "Golden Age" of government funding had passed. Private medical colleges were sprouting like weeds, offering salaries that a mission-based hospital could never match. Faculty recruitment became a battle; maintaining the Gandhian "Code of Conduct" in a consumerist age felt like holding back the tide.
Tapdiya met these challenges with the same "first principles" he had used in the 1960s. He didn't look for flashy consultants; he looked at the numbers. He trimmed waste with a surgeon's precision. He reminded everyone that medicine at MGIMS was a calling, not just a career. Under his stewardship, the budget, which once stood at a single lakh, now exceeded 250 crores. But to Tapdiya, the complexity hadn't changed—the discipline remained the same.
In the final analysis, Parmanand Tapdiya’s life is a testament to the power of "Meticulous Integrity." Most biographies of great leaders focus on their speeches or their grand gestures. Tapdiya’s greatness is found in the quiet of the night, in the thousands of ledgers he reviewed, and in the "No" he said to wasteful expenditures that would have compromised the hospital's mission.
Dhirubhai Mehta once remarked that while he looked at the big picture, Tapdiya moved step-by-step. It is this "Zen of the Detail" that has saved MGIMS during its darkest financial hours. He is the leader MGIMS trusts because he is the only one who knows exactly where every brick is buried and how much it cost.
As he sits today in the President's chair, the boy who once studied by a kerosene lamp is now the man who ensures the lights stay on for thousands of patients and students. He remains an iconoclast—a man who rejects the pretension of power in favor of the clarity of logic. In the history of MGIMS, many have provided the vision, but Tapdiya provided the ground upon which that vision could stand. For sixty years, he has been the man with whom the buck stops, and history bears witness: no challenge is too great for a man who turns adversity into the most disciplined form of opportunity.
| 1944 | Born, Wai village, near Akola — no electricity, no post office |
| 1959 | Ranks 24th out of 325,000 students — age fifteen |
| 1965 | Arrives at MGIMS as CA intern — age nineteen |
| 1965 | Translates Parsons & Co. report into Yen, Lira, Dollars for Dr. Nayar |
| 1966 | Clears CA examinations — first attempt, first in class |
| 1966 | Joins K.K. Mankeshwar & Co., Nagpur — borrows ₹50 for first trousers |
| 1969 | Marries Shobha Rathi — ceremony: one coconut, one rupee |
| 1969 | Chooses Sevagram over Mumbai and Delhi — honorary consultant, no salary |
| 1970s | Trains Kanakdas, Dadarao Shingare, Bhimrao Pradhan — the accounts trio |
| 1982 | Arranges lunch with Nalinibhai Mehta — brings Dhirubhai Mehta to KHS |
| 1967 | Trustee, Kasturba Health Society |
| 1967 | Internal auditor — 31 years of hawk-eyed review |
| 2024 | Assumes presidency, KHS — age seventy-seven |
Manimala Choudhary

Founder of Kasturba Health Society • Builder of MGIMS • Chhoti Behenji of Sevagram
A Woman of Sevagram
The year 2023 marked the birth centenary of Manimala Roy Choudhary — "Chhoti Behenji" of Sevagram. Hers was a remarkable life: one of struggle, dedication, and quiet devotion.
She was born in Bengal in 1923, though the exact date of her birth is not known. Her early years were spent in Calcutta. She came from an elite family of judges, but her childhood was shadowed by absence. After her mother's death, her father renounced the world and left as a sanyasi, leaving behind four young children. Manimala, her sister, and her two brothers were raised by their maternal uncle — Chhoto Mama, a distinguished High Court judge — and their aunt, Shejo Mashi, who had been a neighbour of Subhash Chandra Bose in Cuttack. Under their careful guidance, Manimala grew into a woman of compassion, resilience, and determination. Both brothers were sent to England to study law, and returned as barristers — but also brought back tuberculosis. The younger brother did not survive.
Marriage, Illness, and the Road to Nursing
After completing her matriculation, Manimala was married to a doctor employed by the French government in Kakinada District. Within a few years, she too contracted pulmonary tuberculosis. Still in her teens, she was compelled to leave her one-year-old daughter in the care of her mother-in-law and travel to a tuberculosis sanatorium in Kausani, Uttarakhand, for treatment. This was an era before antitubercular drugs — before Streptomycin, Isoniazid, Rifampicin, and Ethambutol. The only remedies available were rest, fresh air, and nourishing food.
She remained in Kausani for nearly four years. Her family could sustain her expenses for only a year or two. Realising that her recovery would require a longer stay — and eventually a lobectomy — she turned to herself for support. She began knitting sweaters and shawls, and took to educating fellow patients about their health. Her zeal caught the attention of the surgeon in charge, who offered to send her to Lahore for nursing training at the medical college there. She accepted without hesitation, staying four years to complete the course. During that time, she also learned to read and write both Gurmukhi and Urdu.
The Wandering Years: From Lahore to Sevagram
Driven by an indomitable spirit, Manimala continued to push herself further. From Lahore, she travelled to Patna and Solapur to acquire skills in nursing administration and surgical nursing. By now her daughter, aged around ten, was waiting in Kakinada for her mother to come home.
Manimala did return — for a few months. She lived as a respected doctor's wife, comfortable and secure. But the comfort felt like a cage. Something in her remained restless, unsatisfied, unable to settle. It was at this point that she came in contact with Padmaja Naidu — a distant relative through her sister's marriage — daughter of Sarojini Naidu, the celebrated poet and political leader. Padmaja suggested that Manimala visit Mahatma Gandhi at the Sevagram Ashram, which lay close to Nagpur, where her sister lived.
Barely twenty-seven years old, and with her sister's help, Manimala made her way to Sevagram. Gandhiji advised her to work with Dr. Sushila Nayar, who had recently established a modest five-bed facility called Kasturba Hospital at Sevagram. The encounter transformed her. She chose to give up a comfortable, well-established life and take a path few would have chosen — much to the dismay of her family and society. Yet both her husband and mother-in-law gave her their blessing, a generosity she never forgot. Having made her choice, she worked, for the rest of her life, to keep her family relationships whole.
The Assassination, and an Unshaken Resolve
Manimala had returned to Calcutta after meeting Gandhiji, to pack her belongings. On her way back to Sevagram, she heard the news of his assassination. She did not waver. She arrived at the Ashram and began her nursing career under the tutelage of Barbara Hartland — renamed Vasantiben by Gandhiji himself — who had been running the Ashram's dispensary and self-help groups since 1945. When Barbara returned to England after Gandhiji's death, she handed all responsibilities to Manimala. Manimala assumed the role of Matron, overseeing both the hospital and the maternity and child welfare centre at Kasturba Hospital.
Learning to Belong
Coming from a privileged background, Manimala was initially shaken by the poverty around her — the scarcity of water, the sparse diet, the unfamiliar customs of Vidarbha. She bristled at being called "Bai," a word she understood as derogatory in northern and eastern India. But she learned Marathi quickly, and before long the villagers were calling her "Mothi Daktarin Bai" — the big lady doctor — a reference to her height compared to Dr. Sushila Nayar. With time, she came to understand that in this part of the country, "Bai" carried deep respect. The word had humbled her.
She worked closely with Dr. Sushila Nayar, with Asha Devi Aryanayakam — founder of the Nayi Taleem Sangh — and with Prabhakarji, Secretary of the Ashram, who was intimately involved with the hospital's affairs. Together they approached the local government and established a nursing school for ANM training at Kasturba Hospital — one of the first of its kind in rural India.
Beyond the Hospital Walls
Manimala's commitment to healthcare extended well beyond the wards. She worked in villages to promote microinsurance, self-help groups, disease prevention, and health education. Through these efforts — steady, unhurried, year after year — she rose from Matron of Kasturba Hospital to Nursing Superintendent, and eventually to Secretary of the Kasturba Health Society, established in September 1964.

The formation of that Society was itself a milestone. After Gandhiji's death, Dr. Sushila Nayar had left for the United States in June 1948 to pursue a degree in public health at Johns Hopkins University. During her absence, Kasturba Hospital passed through several phases of management — first under the Sevagram Ashram with Prabhakarji, Dr. Wardekar, and Dr. Ranade; then under the Gandhi Smarak Nidhi. Manimala was a trusted associate through each of these transitions. When the time came to give the hospital a permanent, independent home, it was Manimala, together with Shri R.R. Diwakar, Dr. A.D. Ranade, and Nalinbhai Mehta, who persuaded Dr. Sushila Nayar to lead the newly constituted Kasturba Health Society. On September 11, 1964, the Society came into existence. The Gandhi Smarak Nidhi transferred to it the land, buildings, equipment, and a founding contribution of ten lakh rupees. A new chapter had begun.
Building a Medical College
Dr. Sushila Nayar's vision reached further still. In August 1969, the Mahatma Gandhi Institute of Medical Sciences — MGIMS — admitted its first batch of students, becoming India's first rural medical college. What followed was a decade of extraordinary labour. Together, Dr. Nayar and Manimala undertook the daunting work of constructing the hospital, designing lecture halls, outpatient departments, hostels, and laboratories — equipping every department, recruiting every faculty member.
Their temperaments were opposite, and perfectly matched. Dr. Sushila Nayar blazed with impulsive energy; Manimala moved with serene calm. Together — "Badi Behenji" and "Chhoti Behenji" — they functioned like yin and yang. Manimala personally supervised the construction of operation theatres, wards, the kitchen, the library, the water supply, and the solar electric installations. Together they turned an audacious vision into a functioning institution.
A Trusted Confidante
Manimala's bond with Dr. Sushila Nayar was one of deep mutual trust. She was among the very few people who could speak her mind to Dr. Nayar without reservation, offering honest counsel where others might have held back. She served as a sounding board, a conscience, and a quiet anchor.
Dr. Nayar's vision for MGIMS was not merely medical. It was Gandhian — rooted in austerity, simplicity, and humility. She asked Manimala to ensure these values lived in the institution's daily rhythms. Every appointment, every purchase, every construction decision, she insisted, must serve society first. In this spirit, Manimala was willing to bend conventional rules — to the irritation of her more formally qualified colleagues — when she recognised in a man or woman from a neighbouring village a talent or dedication that no certificate could confer. She had a gift for seeing potential in ordinary people, and she used it to make MGIMS an institution that belonged to its surroundings.
Nurse, Builder, Visionary
Manimala was pivotal in establishing a partnership with the Catholic Mission to advance general nursing training, and helped found the first nursing school in rural India — an institution that has since grown into a degree college. She also created Kasturba Vidyamandir, a school for the children of the hospital's doctors and staff, sustained in its early years by the voluntary effort of the senior doctors' wives. She encouraged her staff to form a cooperative housing society, enabling families to own homes after retirement.
A Gandhian in both letter and spirit, she wore khadi, took part in community meals, convened prayer meetings, promoted shramdaan, yoga, and Ayurvedic sciences. MGIMS, under her stewardship, became a health resource not only for its own community but for neighbouring ashrams such as Vinoba Bhave's Ashram at Pawnar.
Her influence over the institution's administration was singular. Beginning with Dr. B.G. Kane, MGIMS's first principal, successive principals — Dr. I.D. Singh, Dr. M.L. Sharma, Dr. K.S. Sachdeva — all reported, in practical terms, to a nurse. They respected her not because of a degree but because of her integrity, her transparency, and the quiet authority of a life lived without compromise.
Stepping Back
In the mid-1980s, her health beginning to fail, Manimala handed over her responsibilities to Ms. Kamala Desikan — a trusted colleague from the Ashram's earliest days. By then, MGIMS had seen sixteen batches of medical students graduate, with over a thousand trained within its walls. She continued to live in Sevagram as a life member of the Kasturba Health Society, remaining close to the institution she had helped build for another seventeen years.
The doctors and staff of MGIMS were, in every meaningful sense, her family. Her only daughter, Bithika — who had grown up without her mother and harboured, for a long time, a resentment towards medicine and Gandhiji for the same reason — chose not to enter the profession. Yet Manimala lived to see her two granddaughters, Prabhati Lahiri (1983 batch) and Deepika Lahiri (1990 batch), receive their degrees from MGIMS. Something had come full circle.
A Gracious Farewell
Manimala Choudhary, twice nominated for the Jamnalal Bajaj Foundation Award for lifetime achievement, passed away peacefully at her home in Guru Nanak Colony, Sevagram, on 26th February 2002. Nearly all of Sevagram, along with people from the surrounding villages, came to pay their respects. The woman they mourned had arrived among them more than half a century earlier as an outsider — a Bengali widow from Calcutta — and had given herself entirely to the land and its people.
She left behind no institution in her name, no endowed chair, no statue. She left behind MGIMS.
| 1923 | Born in Bengal |
| 1940s | Tuberculosis — four years in Kausani sanatorium |
| ~1944 | Nursing training, Lahore Medical College |
| ~1946 | Pulmonary lobectomy — recovered |
| 1948 | Gandhi assassinated — she came to Sevagram anyway |
| 1948 | Matron, Kasturba Hospital |
| 1950s | Bullock cart insurance rounds with Dr. Ranade |
| 1964 | Secretary, Kasturba Health Society (founding) |
| 1969 | Supervised construction of MGIMS |
| 1969 | Co-founded first nursing school in rural India |
| 1970s | Founded Kasturba Vidya Mandir school |
| 1983 | Granddaughter Prabhati Lahiri graduates MGIMS |
| 1988 | Stepped down as Secretary |
| 1990 | Granddaughter Deepika Lahiri graduates MGIMS |
| 2001 | Dr. Sushila Nayar dies — present at her side |
| 2002 | Died 26 February, Guru Nanak Colony, Sevagram |
Kamala Desikan

Kamala Desikan’s story begins in 1927, in the quiet village of Nalluru in Andhra Pradesh. She was the only child of her parents, but her mother’s death from tuberculosis within months of her birth left her in the care of her grandmother. Her father remarried, but his influence on Kamala was profound. An intelligent landlord with a sharp interest in politics, he wore khadi with pride and spoke passionately about Sarvodaya and Gandhi. As a little girl, Kamala sat beside him during these discussions, absorbing the ideals of justice, simplicity, and service. Gandhi’s vision became her own, and the dream of living in his ashram took root early.
When she was nearing twenty, she chose to follow that dream. Moving to Sewagram Ashram, she entered a world of discipline and service. Under the guidance of Prabhakarji, a veteran Gandhian, and Dr. Sushila Nayar, she trained as a nurse at Kasturba Hospital. She cared for patients with quiet dedication, and in a twist of fate, became the hospital’s first surgical patient when Dr. Nayar operated on her tonsils. Gandhi himself visited her afterwards, a moment that eclipsed her pain and etched itself into her memory. Her bond with fellow Gandhian Smt. Manimala Choudhary began here, a friendship that lasted a lifetime.
Her years at Sewagram shaped her spirit. She worked with refugees after Partition along with Dr. Sushila Nayar. Later, when Vinoba Bhave began his Bhoodan Yatra, she was inspired by his vision of Gramdaan—villages gifted for the poor. She volunteered to serve in Garanda, a remote tribal settlement in the Koraput district of Orissa. The journey to Garanda itself was arduous: trains, buses, and finally a sixteen-kilometre walk through dense forests. Life in Garanda was spartan—rice, dal, and brinjal were the only staples, malaria was rampant, and huts were their shelter. Kamala, the only trained health care provider, administered quinine injections to everyone, including herself. Yet she found fulfilment in this hardship, serving the tribals with courage and compassion.
In 1957, her life took a new turn. She married Dr. K.V. Desikan, a leprologist she had met at Sewagram, in a simple Gandhian wedding that cost only thirteen rupees. Together, they moved to Chilakalapalle village, where leprosy was widespread. While Desikan treated patients, Kamala immersed herself in the harijan colony. She brought spinning machines to train women, taught embroidery and painting, and encouraged girls to study beyond primary school. She co-founded Gramodaya Samiti to support education, healthcare, and women’s emancipation. At night, she tutored mischievous boys at home, giving them guidance and shelter. Years later, when those boys returned as successful professionals, the reunion was joyous proof of her quiet influence.
Her work soon extended beyond India. In the early sixties, Shri Jayaprakash Narayan, a Gandhian socialist and political leader, had visited Israel. He had been very impressed by the community working groups – the “Kibbutz”, in that country. He felt that the concept of the Kibbutz could be applied to Vinoba’s “Gramdaan” villages, and decided to send a team of Sarvodaya workers to Israel. In view of her work in the “Gramdaan” village, Goranda, in Orissa, Kamala was selected to the team. She spent six months in Israel, studying the way of life in a Kibbutz, participating in community work, visiting villages, and learning about the travails faced during the holocaust. Once, the then Prime Minister of Israel, Ben Gurion, addressed the group. Kamala sketched a picture of him as he was addressing them. Ben Gurion saw the sketch and, with a broad smile, autographed it. Later, Golda Meir, then a member of the Israeli Knesset, interacted with the group. A photograph of Kamala talking to her captured the warmth between them. Kamala returned to India with a broader vision and renewed energy, convinced that grassroots cooperation could transform villages back home.
Soon after Kamala’s return, Desikan and Kamala moved to Vellore. Desikan joined the MD Pathology course in the Christian Medical College (CMC), at Vellore. Kamala joined an ICMR project on Streptococci under Dr. Grace Koshy, Professor of Microbiology at CMC, involving community work. While working in an urban slum in Vellore, Kamala encountered a woman burdened with caring for her late sister’s four children in addition to her own, while her husband, disabled by leprosy, could not contribute. The woman struggled as the sole breadwinner, working as a domestic help in many households. Kamala stepped in with characteristic compassion and pragmatism: she arranged for two of the children to be cared for by relatives, placed another in a children’s home linked to an ICMR nutrition project, and personally supported one herself. The faculty at CMC responded generously whenever Kamala sought help, and through these efforts, she not only eased the family’s hardship but also forged enduring friendships with colleagues—bonds that lasted throughout her life.
After completing his MD in Pathology, Desikan joined the Central Leprosy Teaching and Research Institute at Chengalapattu, Tamil Nadu, in 1967. Around this time, Kamala was expecting their first child, and for the delivery she returned to the familiar surroundings of CMC Vellore. In July that year, their daughter was born—a little girl they named Prabha, in honour of Prabhakarji, Kamala’s mentor from Sewagram, who had guided her so deeply in her early years.
The family settled in Chengalapattu, where they lived for the next ten years. Kamala devoted herself wholeheartedly to raising Prabha, pouring her energy into motherhood with the same compassion and commitment she had always shown in her social work. Yet even in those years, she continued to nurture her own passions. For a brief period, she enrolled in an art school in Madras, honing her skills in painting and exploring her creative side. It was a time of balance—between family and personal growth, between nurturing her child and cultivating her own talents, a reflection of the rich, multifaceted life she would continue to lead.
In 1976, Desikan was appointed Director of the ICMR’s Central JALMA Institute for Leprosy in Agra, and the family—Desikan, Kamala, and their daughter Prabha—moved there. For Kamala, Agra became a new chapter of service. She quickly noticed that many children of class IV employees were not attending school. Concerned, she began teaching them the alphabet in the verandah of her home. Word spread, and soon more children arrived daily. When her home could no longer accommodate them, she turned an empty garage at the institute into a makeshift classroom. As the numbers grew, she enlisted the wives and daughters of JALMA staff and scientists to help teach. Before long, children from neighbouring villages were flocking to the little garage school, which soon ran out of space.
Recognising the need for a proper institution, ICMR permitted the use of land on the JALMA premises, but Kamala had to raise funds for construction. She met the challenge head-on, bargaining tirelessly for building materials and drawing support from unexpected quarters, including Rev. Tokiwa, the high priest of the Tsubosaka Dera temple in Nara, Japan. With such generosity and her persistence, the school was built. Named Lopamudra Vidya Mandir, it began as a primary school, grew into a secondary school, and eventually a high school. Recognised by the Government of Uttar Pradesh, it quickly became a respected local institution. Rev. Tokiwa later invited Kamala to Japan to share her experiences, and with his help, she arranged for teachers from the school to visit Japan and learn from the practices there. To this day, the school continues to provide education to children who might otherwise have had none.
Her compassion extended beyond education. Kamala noticed that leprosy patients arriving from distant towns had nowhere to stay if they reached Agra on weekends. Lodges refused them rooms, forcing them to sleep under trees or in makeshift shelters. She discovered an old leprosy home near JALMA, a fortress-like eighteenth-century building with rooms around a central courtyard, then housing only a handful of patients. Meeting with the municipal commissioner, she secured permission to revive the place. She formed the Kushth Sewa Samiti, gathered prominent locals, and renamed the building Kushth Sewa Sadan. The municipal corporation provided food for existing inmates, while JALMA supported referred patients, but Kamala knew more was needed. With help from LEPRA and Rev. Shoken Tokiwa, she arranged funds for food and clothing. She even procured a cow, cared for by one of the patients, whose milk provided both nourishment and a small income. She encouraged carpet weaving among patients, giving them dignity and purpose. Her regular visits built bonds of trust so deep that some patients, abandoned by their families, asked her to perform their funeral rites. She honoured their wishes, accompanying their bodies to the cremation ground and carrying out the rites herself.
In Agra, Kamala became affectionately known as “Mataji”—mother to all whose lives she touched. When she was diagnosed with an acoustic neuroma and underwent surgery at AIIMS, New Delhi, many of those she had helped volunteered to donate blood. The operation was successful, though it left her with facial palsy. Where others might have retreated, Kamala trained a domestic helper to perform daily physiotherapy massages and simply carried on with her work, undeterred.
Her interests were as varied as her service. She played the sitar and violin, loved both Carnatic and Hindustani music, and encouraged Prabha to train in Bharatanatyam. Painting was a passion—she created watercolours and oils of portraits, still life, landscapes, and scenes that moved her: the Taj Mahal, Gandhi from photographs, her lodgings in London and Japan, Niagara Falls, and the Himalayas in every shade of daylight. Gardening was another love. With guidance from the superintendent of the Taj Mahal gardens, she developed JALMA’s grounds into prize-winning displays. Her ikebana flower arrangements filled entire pavilions at Agra’s annual flower show, becoming star attractions. Even Agra’s famed carpet industry inspired her—she installed a loom at home and wove two hand-knotted Persian carpets, or “galeechas,” with her own hands.
Another defining chapter of her life came when she returned to Sewagram as Secretary of the Kasturba Health Society after Dr. Desikan retired. It was a role that demanded courage, conviction, and vision. She managed both the hospital and the Mahatma Gandhi Institute of Medical Sciences, ensuring that Gandhian simplicity guided modern medical education. Dealing with the administrative issues of a larger institution brought its own challenges, from managing the hospital and medical college staff to confronting politically motivated agitators who sought to disrupt the work of the Kasturba Health Society. Kamala faced disputes over land, unrest among employees, and the constant need to balance Gandhian simplicity with the demands of modern medical education. Yet she met each challenge with courage and clarity, resolving conflicts before they escalated, and ensuring that the institution remained a sanctuary of service. Her leadership was marked by both strength and compassion—she could be unyielding when defending principles, but equally nurturing when creating opportunities for women, students, and the disadvantaged.
When politically motivated groups tried to seize land belonging to the Society, Kamala confronted them directly, unflinching even when her male colleagues feared violence. Her presence alone was enough to make the agitators retreat. She dealt with staff disputes and quelled unrest before it could disrupt the institution. At the same time, she created opportunities for disadvantaged women by founding Udyami Mahila Mandal, a cooperative that provided hot meals and employment. She set up a crèche for working mothers, ensuring that women could balance family and career. She also encouraged the development of a bakery and food stalls, run by destitute women, which became a lifeline for students and staff. Her initiatives combined practicality with compassion, strengthening the institution while uplifting those who needed support most.
Her vision extended beyond administration. She believed the campus should be a living example of Gandhian ideals, where self-reliance and community flourished. She promoted horticulture, organized flower shows that brought families together, and encouraged staff to participate in cultural activities. She was fearless in defending the institution’s integrity, but equally nurturing in creating spaces where women, children, and the disadvantaged could thrive.
Kamala stepped down from the post of Secretary, KHS, in 2002. On the 15th of October, 2004, she started the Soundari Smriti Shikshan Kendra, in memory of a much loved sister-in-law, to provide free tuition classes to village school children who could not afford such classes. By evening, that day, she was no more. She had passed on just the way she wanted, graciously, in the service of society. Her daughter, Prabha Desikan, and son-in-law, Skand Trivedi, both alumni of MGIMS, survive her.
| 1926 | Born, Nalluru, Andhra Pradesh |
| 1946 | Arrives at Sevagram Ashram, age twenty |
| 1946 | Gandhi visits her bedside after tonsillectomy |
| 1948 | Refugee rehabilitation work with Dr. Nayar |
| ~1950 | Goranda, Koraput — five years in the forest |
| 1957 | Marries Dr. K.V. Desikan — total cost: ₹13 |
| 1957 | Chilakalapalle — Ambar Charkha programme for harijan women |
| 1960 | Six months in Israel studying kibbutz model |
| 1976 | JALMA Institute, Agra — garage school begins |
| 1976 | Lopamudra Vidya Mandir — school built from nothing |
| 1976 | Kushth Sewa Sadan — hostel for leprosy patients |
| 1988 | Returns to Sevagram — Secretary, Kasturba Health Society |
| 1988 | Founds Udyami Mahila Mandal canteen, MGIMS |
| 2003 | Resigns as Secretary, KHS |
| 2004 | Dies 15 October, Sevagram — founding a school that morning |
Annasaheb Sahastrabuddhe
Vice President, Kasturba Health Society (1968–1980)
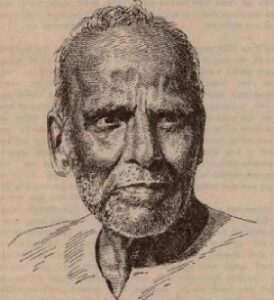
Most people walking past the quiet stretch along the Dean’s office at MGIMS today do not know the story behind Anna Sagar. They see a serene pond, but they do not hear the echo of the hands that dug it—medical students, nurses, clerks, technicians, doctors, petty shopkeepers, and villagers, all working side by side in the soil. Fewer still know the man whose vision brought that water to the surface: Annasaheb Sahastrabuddhe. He was a man who actively avoided the limelight, yet possessed a willpower that fundamentally shaped the soul of Sevagram.
Between 1968 and 1980, the first and most fragile decade of the Mahatma Gandhi Institute of Medical Sciences, Annasaheb served as the Vice President of the Kasturba Health Society. His name rarely appeared in official administrative records. He was not one to sit at the center of group photographs. But behind the scenes, he was an unshakable pillar of strength for Dr. Sushila Nayar. As she navigated the colossal task of building India’s first rural medical college, Annasaheb offered the quiet advice, encouragement, and moral clarity required to keep the institution anchored to its village roots.
* * *
Anant Vasudev Sahastrabuddhe was born on 7 October 1897 in Gupchup Wada, Shaniwar Peth, Pune. His father, a primary school teacher, was subjected to frequent postings across the remote villages of the Amravati district—Daryapur, Elichpur (now Achalpur), and Karajgaon. Each transfer meant packing the family’s meager belongings into a bullock cart and journeying over muddy, unforgiving tracks. Consequently, young Anant attended a new school nearly every year until the sixth grade.
In 1910, he returned to Pune to live with his grandfather and study at the New English School. There, he was taught by Ram Ganesh Gadkari, though it was only years later that Anant realized he had been in the presence of the great Marathi dramatist. Academically, the boy struggled, finding far more joy in the physicality of sports and the discipline of wrestling.
“The worst period in my life was 1908 to 1914,” he would later write in his autobiography. Following his grandfather’s death, Anant and his mother were forced to live in tiny, cramped rented homes while his father continued teaching in distant Vidarbha. Milk became an unattainable luxury. Dignity was hard to find. Yet, this intense poverty did not break him; it opened his eyes to the profound suffering of others.
The true turning point of his youth occurred when he began teaching in the Mang colony in Pune. Brought face to face with brutal caste-based discrimination and utter deprivation, young Anant found his life’s purpose. He organized night schools for Harijan children, offering them not merely literacy, but a radical sense of self-worth. The psychological impact of this experience never left him.
By 1920, deeply inspired by the fiery intellect of Lokmanya Tilak and moved by Mahatma Gandhi’s call for non-cooperation, he took two vows that would dictate the rest of his life: he would never accept a government job, and he would never marry. From that moment forward, service became his only calling.
* * *
Annasaheb spent transformative time at the Sabarmati Ashram, internalizing the rigors of khadi and the inherent dignity of voluntary physical labor. Between 1921 and 1925, he taught at the National School in Chinchwad and worked in agriculture in Belapur. In 1926, he formally immersed himself in the khadi movement. Unlike those who merely spun yarn symbolically, Annasaheb learned the hard, practical ropes of both production and marketing, training extensively at the Kalbadevi Khadi Bhandar.
In 1929, at the invitation of Jamnalal Bajaj, he moved to Wardha. He would remain spiritually and physically bound to this region for the rest of his life. He became the secretary of the Charkha Sangh in 1935 and later established a Khadi Vidyalaya in Mul, Vidarbha.
During the tumultuous decades of the 1930s and '40s, Annasaheb threw himself into the thick of India’s freedom struggle. He marched in the Salt Satyagraha, faced repeated imprisonments, and operated underground during the Quit India movement under the alias “Sunderlal.” Though he was initially convinced that bombs and conspiracies were the only way to shatter British rule, he soon underwent a profound shift, aligning entirely with Gandhiji’s long-term vision of constructive village work. In 1942, he was imprisoned once again in connection with the Capital Bomb Case.
When independence finally dawned, Annasaheb did not seek political office. Instead, he poured his boundless energy into village upliftment—championing Bhudan, Gramdan, Sarvodaya, and Khadi. Working closely with the Sarva Seva Sangh, he traveled the length and breadth of the country to spread Gandhian ideals of equity.
* * *
In 1959, Annasaheb returned to Sevagram and launched a new chapter focused on rural development through agriculture. He was instrumental in helping the Nai Talim educational philosophy rise like a phoenix from the ashes of neglect, establishing a regional planning institute in 1960. As Vice President of the Khadi and Village Industries Commission, and later as head of the Planning Commission’s rural industries committee, he fought to completely reimagine how the Indian state planned for its villages. Though bureaucratic red tape frequently blocked his vision, his persistence was absolute.
He worked alongside stalwarts like Shrikrishnadas Jajoo, Raghunath Dhotre, and Achyut Patwardhan, and drew deep inspiration from Vinoba Bhave and Sane Guruji. Yet, Annasaheb was entirely unique in his independence of thought. Although Vinoba was only two years his senior, Annasaheb considered him a contemporary rather than a guru to be followed unquestioningly.
Throughout his life, he steadfastly refused to be a blind follower—even of Gandhi or Vinoba. He relied on his own accumulated wisdom and grounded insight to choose paths that were both appropriate and pragmatic. He was guided by an unyielding internal compass: honesty, ethical conduct in public life, total accountability, and self-effacement. Having witnessed it up close in his youth, he viewed poverty as a grave, systemic affliction. His life’s mission was to help the poor escape the vicious cycle of debt and become fiercely self-reliant.
Collaborating with economists like Dr. D.R. Gadgil and Dr. Prabhakar Nair, he built grassroots district planning models that sought to integrate small, forgotten workers—tea sellers, barbers, grocers—into the formal village economy. His visionary Panchsutra framework, tested in Koraput, Odisha, tackled alcoholism, illiteracy, fear, poverty, and dependence simultaneously. It offered the young Indian nation one of its earliest and most holistic templates for rural development.
* * *
When Dr. Sushila Nayar set out to build MGIMS, Annasaheb was immediately by her side. True to his nature, he was not found in boardrooms or posed for press photographs; he was out in the field. He advised her on land use, helped shape the rural ethos of the college, and quietly ensured that the village and the campus grew in tandem, rather than the hospital swallowing the community.
Anna Sagar, the campus pond, was born of his philosophy. He envisioned it not merely as a functional water source, but as a profound symbol of collective ownership. When villagers, hospital staff, and medical students picked up shovels together, it ceased to be an act of charity. It became the forging of a community.
Annasaheb held numerous high-profile positions over his life—chief secretary of the Gandhi Seva Sangh, president of the Sevagram Ashram, and advisor to national boards. Yet, power and prestige slid off him like water. When Prime Minister Indira Gandhi offered him the prestigious Padma Bhushan in 1970, he accepted it quietly, and never mentioned it again.
He was a man who had mastered the rare art of loving people freely—without drama, without conditions. He seamlessly blended into the lives of those he met, sharing their joys and sorrows with a calm, deeply attentive presence.
He had no family, no home, and no property. He lived by the maxim: “Nadi behti bhali, sadhu chalta bhala”—a flowing river is good, a wandering sadhu even better. He lived exactly like that river, always in motion, never tied down.
Among the many Gandhians of his era, Anna stood apart. Publicity meant nothing to him. Dressed in a simple khadi shirt, a dhoti, and worn-out chappals, he carried only an extra pair of clothes. Any money he received, he quietly routed to those in need. He rarely stayed more than two nights in one place, except when he returned to Sevagram or the ashrams he considered his spiritual home. In those ashrams, he was not a guest; he was the patriarch. He helped people solve their everyday domestic problems with the exact same gravity he brought to international economic issues.
Once, a curious observer asked him why he had never married. Anna smiled warmly and replied, “When I was of marriageable age, I was in love with social work. And when that fire settled… it was too late.”
* * *
Anna Saheb earned national respect as an authority on rural development not through academic theory, but through calloused hands. He had tilled land, raised cattle, and worked alongside laborers. In 1961, when Prime Minister Nehru launched the Planning Commission’s efforts on rural development, Anna was invited to join a working group tasked with defining a national minimum standard of living. Alongside experts like D.R. Gadgil and Ashok Mehta, he helped draft a landmark report recommending a poverty line of Rs. 100 per month for a five-member household, calculated on essential needs like food, clothing, housing, and fuel. (They notably excluded health and education, firmly believing the State was morally obligated to provide those for free).
However, the sterile bureaucracy of Delhi clashed violently with his action-oriented soul. Frustrated by endless red tape and political inertia, he quietly resigned and took the train back to Sevagram—preferring to serve in the dirt rather than sit in an office. Even during that short, lucrative government stint, he lived on a floor mat and sent his entire salary, by money order, to support eight impoverished children.
His connection to Sevagram was visceral. It was the laboratory where he proved that even the most modest village activity could become self-sustaining. When Prof. Madhu Dandavate became Minister of Railways in 1977, Anna personally insisted that local vendors be allowed to sell fresh cow’s milk at Wardha and nearby railway stations—a small, highly specific victory that perfectly illustrated his insistence on rural economic independence.
He was not trapped by historical ideology. He admired E.F. Schumacher’s philosophy of Small is Beautiful and personally brought the famed economist to Sevagram. He also invited two agricultural scientists from Israel to the ashram, deeply believing in “appropriate technology”—modern solutions specifically tailored to suit the rural poor.
* * *
In his later years, Anna’s body grew frail. A serious accident left his hands trembling and his neck shaking, but he refused to slow down. His speeches remained simple, clear, and full of nishtha—unshakable commitment. His eyes still burned with quiet determination.
He found profound comfort in spiritual practice, regularly reciting the Vishnu Sahasranama. Often, he would pause mid-verse, chanting with deep, overwhelming feeling, drawing immense solace from its sacred rhythm.
At the age of 83, his heart began to fail, its rhythm fluctuating dangerously. True to the vows he took in 1920, he flatly refused to spend a single rupee on his own medical treatment. It was only through the desperate insistence of his well-wishers that he was finally taken to Bombay Hospital to receive a pacemaker.
He passed away in that hospital on 11 March 1980, before the procedure could be completed.
Annasaheb Sahastrabuddhe left behind more than writings or institutions; he left behind a blueprint for living. For decades, the student who topped the Gandhian Thought paper in the MGIMS medical entrance exam was awarded the Annasaheb Sahastrabuddhe Medal.
His was the kind of work that rarely makes the evening news. But if one walks through Sevagram today, and looks closely at the soil, the water, and the walls of MGIMS, his presence is everywhere. In silence. In the soil. In the spirit.
| 1897 | Born, 7 October, Pune |
| 1920 | Two vows taken — no government job, no marriage |
| 1921 | Sabarmati Ashram — khadi and voluntary labour |
| 1929 | Moves to Wardha at Jamnalal Bajaj’s invitation |
| 1930 | Salt Satyagraha — repeated imprisonment |
| 1935 | Secretary, Charkha Sangh |
| 1942 | Underground during Quit India — alias Sunderlal |
| 1942 | Imprisoned — Capital Bomb Case |
| 1959 | Returns to Sevagram — regional planning institute, 1960 |
| 1961 | Planning Commission working group — drafts India’s first poverty line |
| 1964 | Brings E.F. Schumacher to Sevagram |
| 1968 | Vice President, Kasturba Health Society |
| 1969 | Anna Sagar dug — MGIMS campus pond, collective labour |
| 1970 | Padma Bhushan — accepted quietly, never mentioned again |
| 1980 | Dies 11 March, Bombay Hospital — before pacemaker could be fitted |
Prabhakarji
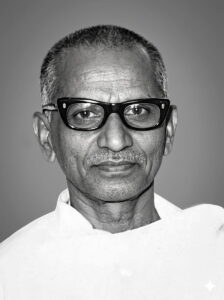
No one knew where Prabhakarji was born, or when. No one knew his family name, his caste, or his religion. He never told anyone. It was as if he simply arrived in Wardha one day in 1935, quietly blending with the dusty roads and neem trees, drawn by the sound of Mahatma Gandhi's voice at the Grama Sevak Vidyalaya in Maganwadi. He stayed for the rest of his life.
In a book of portraits — lives defined by dates, degrees, and departments — Prabhakarji defies the form entirely. He had no qualifications to list, no titles to record, no salary scale to document. What he had was something rarer: an absolute, uncomplicated devotion to whoever was suffering in front of him. He nursed malaria patients with mud packs and enemas when there was nothing else. He helped found a five-bed dispensary that became a thousand-bed teaching hospital. He brought Manimala Chaudhary to Sevagram and set her on the path that would make her a founding trustee of the Kasturba Health Society. He managed Kasturba Hospital alone when Dr. Sushila Nayar was in prison with Gandhi and later in America pursuing her doctorate.
He died in Andhra Pradesh in June 1979, in the middle of relief work after a cyclone. He was removed from the ashram shortly before his death, dismissed without ceremony for supporting workers in a wage dispute. He accepted this without protest and went straight back to serving people. He owned nothing. He left nothing. Except everything that MGIMS stands on.
His full name was Prabhakaran Joseph. He had, at some point, converted to Christianity. He had been born into a community in Andhra Pradesh where meat consumption — including carrion — was customary. His mother was a hospital attendant who drank toddy to cope with the difficulty of their lives. He failed the matriculation examination twice.
At the Andhra Jateeya Kalasala, he encountered Young India, Gandhi's publication. Something in Gandhi's writing on cow protection and non-violence reached him where nothing else had. He gave up meat, gave up toddy, and set about remaking himself through the slow discipline of Gandhian practice. He was a young man then, with six years of schooling, whose entire understanding of the world was about to change.
In 1940, he came to Maganwadi in Wardha as a Harijan student, learning paper-making, bee-keeping, and soap-making. Mahadev Desai noticed him. He introduced the boy to Gandhi. A letter in the Harijan dated September 15, 1940, records a characteristic exchange: Prabhakar confessed to Gandhi about his past — his diet, his upbringing — and announced he intended to abstain from milk as penance. Gandhi, moved by the sincerity but practical as always, told him to resume milk consumption. The cow's service to humanity, he said, was too valuable to be declined.
Gandhi agreed to let him stay in the ashram. He never left — not really, not even after he was pushed out forty years later.
In those years, Wardha was notorious for malaria. Every monsoon swept through households and the ashram alike, leaving patients bedridden with fevers above 102 degrees. Recovery required a week of devoted nursing. There were no antibiotics. There was mud — applied in packs to foreheads and abdomens. There were enemas. There was Prabhakarji, moving between cots with a mother's unhurried tenderness.
His work brought him close to Dr. Sushila Nayar, who had arrived in Sevagram as Gandhi's doctor and was building what would become Kasturba Hospital. Together, they set up a small dispensary in one of the ashram's rooms — a few medicines, some disinfectants, a willingness to try. Patients came. More followed. Gandhi eventually suggested moving the dispensary out of the ashram to a newly constructed guest house built by G.D. Birla a few furlongs away. The guest house became a five-bed hospital. That five-bed hospital is today a thousand-bed teaching institution affiliated with MGIMS.
When Dr. Sushila Nayar was imprisoned at the Aga Khan Palace with Gandhi and Kasturba in 1942, Prabhakarji ran the hospital. When she left for America in 1948 to pursue her doctorate at Johns Hopkins, he continued to manage it, assisted by Dr. R.V. Wardekar. Around him also worked Dr. Anant Ranade and Manimala Chaudhary — but it was Prabhakarji who held the centre, who kept the institution functional through years of uncertainty when it had no secure funding, no institutional backing, and no guarantee of survival.
He recruited staff from the surrounding villages, trained them, and turned them into dependable healthcare workers. Many of them later became the backbone of MGIMS when the medical college opened in 1969.
Prabhakarji was what he himself called a Pawanvasi — like the wind, rootless and free. He owned nothing of consequence. Whatever he had, he spent on others. Whatever energy he carried, he directed toward whoever needed it most. He travelled constantly across Maharashtra and Andhra Pradesh, training young volunteers and health workers, setting up leprosy services, responding to disasters. When he traveled, he never stayed in guest houses or hotels — always in the homes of friends, sharing their meals and their moments.
He carried a small basket of fruit when he traveled. Children always knew the basket was theirs.
He never delivered lectures. He never wrote articles. "His life was his message," those who knew him said, "and his actions were his teachings." He met the Prime Minister with the same simplicity with which he met the most destitute villager in the most remote hamlet. The uniform treatment was not performance — it was how he saw people.
He formed bonds that lasted decades. It was Prabhakarji who first brought Manimala Chaudhary to Sevagram and encouraged her to train in nursing — an act whose consequences neither of them could have foreseen. She would go on to become matron of Kasturba Hospital, founding trustee of the Kasturba Health Society, and one of the central figures in the founding of MGIMS. The thread that connects Prabhakarji to the modern medical institution is direct and unbroken.
When Gandhi began treating Sushila Shastri and others with leprosy in Sevagram, Prabhakarji stood beside him, caring for the sick without hesitation or fear. He worked at Datta Pura Leprosy Hospital, at Gandhi Memorial Leprosy Foundation, at the small hospital in Pavnar that Gandhi opened and that Dr. Krishna Nair later expanded. Wherever the need was greatest and the glamour least, Prabhakarji went.
He had a phrase he used to describe his rhythm of life: "Thirty days a month, I travel to serve. Thirty nights a month, I return to sleep at Sevagram Ashram after taking Bapuji's blessings."
It was not a boast. It was simply the schedule.
He never married. He had no children, no property, no wealth. He found joy — genuine, uncomplicated joy — in the smallest tasks: working in the fields, cleaning the kitchen, nursing a patient, mending a labourer's torn shirt. Ego never found a home in him. He was perhaps the purest embodiment of Gandhi's ashram ideal that the ashram itself produced.
His models were Gandhi and Vinoba Bhave, and he lived their principles of non-attachment without apparent effort, as if it required no discipline at all — as if it was simply who he was.
In 1978, the ashram faced internal unrest. Workers were demanding wage parity with employees at the neighbouring medical college. Prabhakarji, always an advocate for those without power, supported their demands. His position put him at odds with the ashram management. In a decision that those who loved him found deeply contrary to Gandhian values of dialogue and consensus, he was removed from his post as Secretary of Sevagram Ashram Pratishthan — dismissed without ceremony, without the conversation his decades of service deserved.
He accepted the decision without protest. He left the ashram. And then he went back to work.
Despite his declining health, he traveled to Andhra Pradesh to help in the aftermath of a cyclone. He died there on June 17, 1979, still serving, still moving, as he had for more than four decades.
After his death, Dr. K.V. Desikan — a pioneering figure in leprosy medicine and later a key figure at MGIMS — instituted an award in Prabhakarji's memory, given to distinguished social workers in leprosy care. The Desikans' feeling for Prabhakarji ran so deep that when their daughter was born in 1967, they named her Prabha in his honour. She would go on to become a doctor herself, an alumna of MGIMS.
These are small monuments to an unmonumental man. Prabhakarji would have found them touching and faintly embarrassing in equal measure.
He arrived in Wardha in 1935 with six years of schooling and no plan beyond the desire to be useful. He left behind a hospital, a trained workforce, an institution, and an example of how completely a human life can be given to others. He never asked what he would get in return. The question would not have occurred to him.
In a book about the men and women who built MGIMS, most are remembered for what they created — departments, curricula, research programmes, clinical protocols. Prabhakarji is remembered for something harder to name and impossible to replicate: a quality of presence, an unconditional availability to human need, a life in which the distance between belief and action was, as far as anyone could tell, exactly zero.
| 1935 | Arrived in Wardha — drawn to Gandhi’s voice at Grama Sevak Vidyalaya, Maganwadi; stayed for the rest of his life |
| 1940 | Came to Maganwadi as Harijan student — paper-making, bee-keeping, soap-making; introduced to Gandhi by Mahadev Desai |
| 1940 | Letter in Harijan, 15 September — confessed his past to Gandhi; Gandhi let him stay |
| 1942 | Dr. Nayar imprisoned, Aga Khan Palace — Prabhakarji ran Kasturba Hospital alone |
| 1948 | Dr. Nayar left for Johns Hopkins — continued to manage hospital with Dr. R.V. Wardekar |
| 1950s | Brought Manimala Chaudhary to Sevagram — encouraged her to train in nursing; she became matron of Kasturba Hospital and founding trustee of KHS |
| 1964 | Founding Trustee, Kasturba Health Society — the legal body that created MGIMS |
| 1967 | Dr. K.V. Desikan named his daughter Prabha in his honour |
| 1969 | MGIMS admitted its first students — built on the workforce Prabhakarji had trained from surrounding villages |
| 1978 | Dismissed from post as Secretary, Sevagram Ashram Pratishthan — supported workers in wage dispute; accepted without protest; went straight back to work |
| 1979 | Died, 17 June, Andhra Pradesh — cyclone relief work; still serving; still moving |
Raghunath Shridhar Dhotre
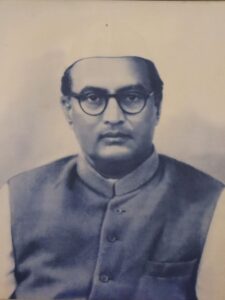
Founding Trustee, Kasturba Health Society · Secretary to Jamnalal Bajaj · Disciple of Vinoba Bhave · The Continuity of Sevagram
When Raghunath Shridhar Dhotre died in Wardha on May 16, 1967, the President of India sent condolences to his widow. It was a gesture that would have puzzled Dhotre himself, a man who spent fifty years in deliberate retreat from public recognition. He had never contested an election, never sought a platform, never written the memoir his friends urged him to set down. He served — quietly, precisely, behind the scenes of the freedom struggle and its Gandhian aftermath — and then he was gone, his name already fading by the time the condolences arrived.
He deserves to be remembered.
Dhotre was born on June 10, 1897, into a generation that would spend its youth fighting for a country that did not yet exist. In 1918, he came to Sabarmati Ashram alongside Acharya Vinoba Bhave — not as a famous arrival but as a committed young man beginning a life organised around khadi, village upliftment, and service without ambition.
When Vinoba founded Param Dham Ashram in Wardha in 1921 as a branch of the Sabarmati Satyagraha Ashram, Dhotre was with him. Together, they taught at the Ruia Shram School for Women, established by Jamnalal Bajaj. For Dhotre, teaching was not a profession — it was his contribution to what Gandhi called constructive work: the patient, unglamorous nation-building that continued regardless of whether the British were being confronted or not.
Jamnalal Bajaj, who had a sharp eye for reliable men, appointed Dhotre his secretary. It was a role that suited him exactly — administrative, trust-based, demanding precision and discretion rather than oratory or ambition. Under Bajaj's leadership, Dhotre developed organisational skills that would serve Gandhian institutions for decades: the ability to hold multiple threads simultaneously, to keep records impeccably, and to move between the visionary and the practical without losing either.
In the 1920s, as secretary of the Maharashtra Charkha Sangh, Dhotre helped turn spinning into something more than a cottage industry. The charkha was Gandhi's symbol of economic self-reliance and rural dignity — the act of spinning one's own cloth as a political statement against colonial dependency. Dhotre's work was to make this symbol operational: organising, training, distributing, sustaining the infrastructure of a movement that required as much administrative support as ideological conviction.
He was no orator. He inspired not through speeches but through the consistency of his own example and the quality of his quiet encouragement. One of those he influenced was Annasaheb Sahasrabuddhe, who would go on to devote his life to village work in the remote districts of Wardha and later serve as Vice President of the Kasturba Health Society. The thread that runs from Dhotre's mentorship to Sahasrabuddhe's decades of rural work to the founding of MGIMS is direct, even if it is invisible in any formal record.
In 1940, Dhotre served as Secretary of the Gandhi Seva Sangh, bringing him into close working contact with Sardar Vallabhbhai Patel, P.C. Ghosh, and Gangadharrao Deshpande — the senior generation of the freedom struggle. After independence, when Dadasaheb Mavlankar became President of the Gandhi Smarak Nidhi, Dhotre was appointed its Secretary, traveling across India to support constructive initiatives and advise the Khadi Board, of which he was a respected informal member though never formally constituted.
Through it all — Sabarmati, Wardha, Delhi, Tryambak — he remained a man without political ambition. He never contested an election. He never sought a public platform. He found his purpose elsewhere.
The Dhotres' home in Sevagram, adjacent to Jamnalalji's guest house, was known to everyone who passed through the ashram world as a place of unusual warmth. The ashram itself could be austere, demanding, occasionally overwhelming to visitors unaccustomed to its rhythms. Dhotre's house was different.
His wife Sharayutai — born August 5, 1910, known to everyone as Akka — ran the household with a gracious hospitality that seemed effortless. There were always refreshments, always laughter, always conversation that moved freely between the serious and the ordinary. Akka never appeared tired or flustered. Every guest was received with the same attentive dignity, whether they were a passing Sarvodaya worker or a senior Congress leader.
Visitors who felt daunted by the moral gravity of Gandhian ashram life found particular comfort in one of Dhotre's characteristic remarks: "We are ordinary householders, just like you." It was not false modesty. It was a genuine hospitality — an invitation to lay down the performative weight of ideology and simply be a person among people.
Their home became a sanctuary. In a world of causes and commitments, it offered the rarer thing: welcome.
In September 1964, when the Kasturba Health Society was registered in Nagpur to take formal charge of what would become MGIMS, Dhotre was among its seven founding trustees. He joined Dr. Sushila Nayar, Manimala Chaudhary, Dr. Anant Ranade, Shriman Narayan of the Planning Commission, Laxmidas Shrikant of the Gandhi Smarak Nidhi, and Nalinibhai Mehta — a group bound not by institutional affiliation but by a shared formation in Gandhian values and decades of acquaintance with each other's character.
Dhotre represented something specific in that group: continuity. He had been in Wardha since 1921. He had known Jamnalal Bajaj personally. He had worked with Vinoba Bhave at the beginning of the Param Dham Ashram. He carried the institutional memory of the ashram world in a way that the others, many of whom had come to Sevagram later, could not. His presence on the founding board was a form of testimony — that this new medical institution was not a departure from the Gandhian tradition but its continuation.
He died on May 16, 1967, three years after the Kasturba Health Society's founding and two years before MGIMS admitted its first students. Heart and kidney failure. He had been hospitalised in Nagpur, barely conscious in his final days. He did not live to see what the institution became.
His daughter's daughter did. Bhakti — granddaughter of Raghunath and Sharayutai Dhotre — was a member of the first batch of MGIMS in 1969. The Gandhian values had passed from generation to generation, from khadi to stethoscope, in exactly the way the founders had hoped they would.
In his later years, friends urged Dhotre to write down his memories. He had the material. He had been present at enough significant moments, alongside enough significant people, to fill a substantial volume. His recollections were sharp, his observations — of great men and their contradictions, of meetings that shaped the nation's course — reportedly candid and illuminating.
He never wrote it. The memoir was planned, discussed, and left undone. Whether from modesty, from the press of continuing work, or simply from the sense that his life had been lived rather than narrated, the record was never set down. What remains is fragmentary — the testimonies of those who knew him, the institutional traces of his work, the charkhas still turned by hand in Sevagram homes.
It is one of the quiet losses of that generation: the men and women who were present at the founding of things, who knew everything and wrote down nothing, trusting instead that the work itself would be sufficient testimony.
For Dhotre, it mostly was. The Kasturba Health Society endures. MGIMS endures. The school of thought that placed rural healthcare and rural education at the centre of post-independence nation-building endures, however battered. He was part of its planting.
He never sought the limelight. In that retreat, he became — as those who remember him say — the flame by which others found their way. Akka outlived him by thirty-two years, dying on January 29, 1999, still in Sevagram, still the warm centre of whatever company gathered around her. She was, in her way, as much a part of the institution's founding as her husband — the hospitality that made idealism liveable, the household that gave the movement a human face.
| 1897 | Born, 10 June |
| 1918 | Arrives at Sabarmati Ashram with Vinoba Bhave |
| 1921 | Param Dham Ashram, Wardha — with Vinoba from the start |
| 1921 | Teaches at Ruia Shram School for Women, Jamnalal Bajaj’s school |
| 1920s | Secretary, Maharashtra Charkha Sangh |
| 1929 | Secretary to Jamnalal Bajaj |
| 1940 | Secretary, Gandhi Seva Sangh — works with Patel, Ghosh, Deshpande |
| 1947 | Secretary, Gandhi Smarak Nidhi under Dadasaheb Mavlankar |
| 1964 | Founding trustee, Kasturba Health Society, Nagpur |
| 1967 | Dies 16 May, Wardha — President of India sends condolences |
| 1969 | Granddaughter Bhakti joins MGIMS first batch |
| 1999 | Sharayutai (Akka) dies, 29 January, Sevagram |
Nalinikant Mayashankar Mehta
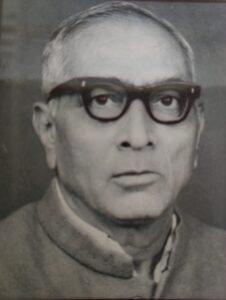
Founding Trustee & Finance Manager, Kasturba Health Society · Disciple of J.C. Kumarappa · The Third Pillar of MGIMS
He began work at four in the morning.
"Son," he would chuckle, "four a.m. — that was my happy hour. Three quiet hours, just me and the numbers. No phone calls, no meetings, no interruptions. I could balance the books, track every paisa, and get things in order. Once the office opened, it was chaos. I had to be ready."
In the dim hours before Sevagram woke, Nalinibhai Mehta sat with his ledgers and made the numbers yield their truth. He had been doing this, in one form or another, since he was a teenager apprenticing under a photographer in Surendranagar because there was no money for college. Numbers had always spoken to him — not as abstractions but as instruments of discipline, of accountability, of institutional survival. Without sound finances, he understood, a dream remained a dream. With them, MGIMS took shape.
He was the third pillar of the founding trio, less celebrated than Dr. Sushila Nayar or Manimala Chaudhary, rarely photographed, seldom quoted. But when Dr. Nayar visited him after his stroke in 1991 and found him confined to his home, unable to move his right arm and leg, she wept. "Nalinbhai," she said, "I had no idea how meticulously you kept the accounts. Where will I find someone like you?"
She never did.
Nalinibhai was born on January 17, 1917, in Karachi. His mother died when he was three. His father — a merchant trading fine crockery between Karachi and Bombay — lost his entire inventory in 1922 when the ship carrying it sank. The family went bankrupt. His father died when Nalinibhai was seven. He was sent to Halvad, a small town in Gujarat's Morbi district, to be raised by a stepmother and an uncle.
He schooled in Surendranagar, worked as an apprentice to a photographer named J.J. Mehta to pay his way, and at nineteen joined the freedom struggle. He spent four months in a British prison — a steep price for a teenager, one he never regretted. Somewhere in those years of scarcity and self-reliance, he developed what would become his defining quality: an almost physical aversion to waste.
In 1936, a Sarvodaya worker named Babalbhai Mehta urged him to visit Sevagram and meet Gandhi. He went. Gandhi sent him to the Khadi Gramodyog Vidyalaya to work under J.C. Kumarappa — economist, freedom fighter, and one of Gandhi's closest intellectual collaborators. The apprenticeship transformed him.
Kumarappa's vision was of self-sufficient villages built on local resources and diversified skills. His financial philosophy was equally exacting: precision in record-keeping, rigour in balancing accounts, the discipline of making every rupee yield its maximum worth. Nalinibhai did not merely absorb these lessons — he lived them. He shaved his head to save on haircuts. He wore simple clothes to conserve fabric. He treated every paisa as a moral responsibility.
The bond between mentor and disciple deepened into something like family. When Nalinibhai married Madhu Lata, Kumarappa marked the occasion with rare warmth — gifting her a gold armlet, and presenting Nalinibhai with two prized possessions: an Omega watch and a Zeiss Ikon camera. They were, as Nalinibhai understood them, not gifts but tokens of trust.
When Nalinibhai arrived at MGIMS in 1969 as founding trustee and member in-charge of finance, the accounts office was two cramped rooms under a sloping kavelu roof. Stone floors cool against the Vidarbha heat. A flickering tubelight. Wooden shelves sagging under the weight of thick ledgers. A noisy table fan pushing warm air over yellowing files. The smell of ink and old paper.
Three men shared a single battered wooden desk: Dadarao Shingare, who had left school after sixth grade but handled the hospital's cash flow with meticulous care; Kanakdas, a boy from Kerala who had arrived in Wardha in the mid-sixties nearly illiterate and orphaned, found by Manimala Chaudhary lingering near the ashram kitchen, given a job ringing the hourly chime, who then taught himself Hindi and English and the General Financial Rules by kerosene lamplight until the bell boy became the chief accountant; and Bhimrao Pradhan, who had studied to tenth grade in Yavatmal and worked his way from laboratory attendant to accountant through sheer observation and persistence.
None had studied commerce. None had trained under an accountant. Together, they managed an annual budget of one lakh rupees.
"Am I to blame," Dr. Sushila Nayar once said, defending these men, "if I entrust sensitive jobs to men who may not be very bright but on whom I can rely?"
Nalinibhai understood exactly what she meant, because he had built his own career on the same principle — that reliability, precision, and integrity were worth more than any qualification. He supervised the three men, trained them further, and stood behind them when anyone questioned their credentials. The accounts office under his watch was impenetrable. Auditors found nothing to fault. Not once.
The founding years of MGIMS were financially precarious in ways that those who joined the institution later can scarcely imagine. The Gandhi Smarak Nidhi provided a one-time grant of one million rupees when MGIMS opened in 1969, with a clear condition attached: no further funds. The institution had to become self-sustaining from that moment.
Nalinibhai accepted this as a challenge, not a constraint. Government grants, hospital revenues, donations, interest from the KHS endowment — he tracked every source, stretched every allocation, and maintained balance sheets of such clarity that they served as models of institutional transparency. He convinced Dr. Nayar that the three of them — she, Manimala Chaudhary, and himself — would accept only a nominal honorarium of ₹500 per month. This increased in small increments over the years, reaching ₹2,000 by the time his stroke ended his working life. For a man who had access to an institution's entire finances, the restraint was extraordinary and deliberate.
For five years he shuttled between Delhi and Sevagram — Delhi for the Gandhi Centenary Year programmes and the Gandhi Smarak Nidhi's fundraising work, Sevagram for the accounts. When in Sevagram, he slept on the floor and rode a bicycle to inspect the society's agricultural land. He kept the same hours — four in the morning, ledger open, pencil moving — regardless of which city he was in.
In 1970 he settled permanently in Sevagram. He was fifty-three years old. He would spend the next twenty-one years managing the finances of a growing medical institution, never wavering in precision or principle.
His desk, those who worked alongside him recall, was not merely a workstation. It was a stronghold. A single misplaced digit in a ledger would prompt a sharp glance. An unclear expense would summon a booming interrogation. He was frank, outspoken, and sometimes blunt — a man who called a spade a spade without social lubrication. Nobody minded, because the frankness came from conviction, not malice. He had no personal stake in any financial decision. He had only the institution.
He built relationships with donors through the same quality. With Sarla Parekh — who became a holding trustee of the Kasturba Health Society — and with contributors large and small, he understood that fundraising was not about solicitation but about trust. A small gift from a local shopkeeper mattered as much as a corporate donation. He treated every donor with identical respect. People gave not just money but faith, because Nalinibhai made the institution's integrity visible in his own person.
In 1982, he and P.L. Tapdiya — who had come to MGIMS as a young chartered accountancy apprentice in 1965 and stayed for six decades — arranged a lunch between Dr. Sushila Nayar and Dhirubhai Mehta. That meeting brought Dhirubhai into the KHS fold. After Annasaheb Sahastrabuddhe's death, Dhirubhai became Vice President, then Dr. Nayar's most trusted ally, and after her death led the institution for twenty-four years. One lunch, arranged by Nalinibhai, shaped the next quarter century of MGIMS governance.
Through the working years, Madhu Lata was beside him — battling rheumatic heart disease for nearly thirty years, her heart weakened by a blocked valve, yet maintaining the household and raising their three children: sons Rajiv Lochan and Bharat Bhushan, and a daughter, Vrinda. On May 19, 1987, in Ahmedabad, she died. The family she had built and held together remained her lasting legacy. Nalinibhai, who had balanced institutional accounts with iron discipline for decades, was less equipped for this particular loss. It was his daughter-in-law Lata who held things together then, and who would do so again when the stroke came.
In 1991, while in Gujarat, Nalinibhai suffered a stroke. It took his voice — that booming, interrogating, never-uncertain voice — and left him unable to move his right arm and leg. He was seventy-four years old. He came home to Ramdas Colony in Sevagram and did not leave again.
Lata cared for him through the final decade with unwavering devotion. He spent his days confined to home, the ledgers gone, the four o'clock mornings gone, the chaos of office hours that he had always been three hours ahead of — all of it gone.
Dr. Sushila Nayar visited him. She wept. She had not known, she said, how meticulous he had been. It was a strange thing to say about a man she had worked alongside for twenty-seven years — but perhaps the full dimension of his precision only became visible in its absence, when the accounts had to be managed without him.
He died on June 17, 2000, at home in Ramdas Colony, surrounded by Lata, Bharat, and his family. Six months later, Dr. Sushila Nayar followed him.
They had both witnessed MGIMS entire — from the two cramped rooms under the kavelu roof to the thousand-bed teaching hospital it became. Between them, they had held the institution's vision and its finances, its direction and its discipline, in careful, complementary hands for more than three decades. One without the other would have been insufficient. Together, they built something that outlasted them both.
| 1917 | Born, Karachi, 17 January |
| 1920 | Mother dies — father bankrupt by 1922 |
| 1924 | Father dies — sent to Halvad, raised by uncle |
| 1936 | Visits Sevagram — Gandhi sends him to J.C. Kumarappa |
| 1936 | Four months in British prison for freedom movement |
| 1936 | Apprenticeship under Kumarappa, Khadi Gramodyog Vidyalaya |
| 1964 | Founding trustee, Kasturba Health Society |
| 1969 | MGIMS opens — Finance member, founding team |
| 1970 | Settles permanently in Sevagram |
| 1982 | Arranges lunch — brings Dhirubhai Mehta into KHS |
| 1987 | Madhu Lata dies, Ahmedabad, 19 May |
| 1988 | Steps down as Finance Manager |
| 1991 | Stroke — confined to home, Ramdas Colony |
| 1991 | Dr. Nayar visits — weeps at his bedside |
| 2000 | Dies 17 June, Ramdas Colony, Sevagram |
Laxman Radhakrishna Pandit
Warden · Orientation In-Charge · Eight Years at Sevagram · The Kettle Was Always On
Laxman Radhakrishna Pandit — known to every student, nurse, clerk, driver, and doctor who passed through the early years of MGIMS as Pandit Kaka — was the quiet human infrastructure of the institution's founding years. His door was always open. A kettle of tea was always on the boil. When students missed their mothers, his wife Manorama Tai ensured they got warm, homely meals. When hostel corridors filled with homesickness in the small hours, Pandit Kaka would appear in his unhurried way and remind them, in a voice so calm it was almost a form of reassurance in itself: "You are here to serve, to learn, and to grow."
He was not a strict warden. He understood that boys would be boys, that discipline earned through kindness went deeper than discipline imposed by authority. He had been living this understanding since before most of them were born.
Pandit Kaka was born on April 4, 1909, in the princely state of Bastar in what is now Chhattisgarh. His father died young. His mother raised him with a fierce insistence on education. He grew up mastering English, Hindi, Marathi, Sanskrit, mathematics, and economics, and learned agriculture alongside his studies — a combination of skills that would serve him across five decades of institutional work.
Gandhi's message was sweeping across India in his formative years, and Pandit Kaka made an early vow: he would never work for the British government. He meant it. While still a young man, he built a modest school in his village and began teaching — the quiet nation-building that Gandhi called constructive work, carried out in ordinary places by ordinary people with extraordinary commitment.
In 1935, a khadi salesman came through. His name was Annasaheb Sahastrabuddhe. He was selling cloth, but what he carried was something more compelling — a vision of village self-reliance and a life of purposeful service. Pandit Kaka left with him. He traveled to Wardha, joined the Charkha Sangh, and never really left. Branches of the Sangh began springing up in Metpally, Savali, and Mul — each a quiet testament to his ability to get things done without seeking recognition for doing them.
By 1944, he had become secretary of the Charkha Sangh and took charge as principal of the Sevagram Khadi Vidyalaya. He had married Manorama Mainkar of Nagpur in 1936. Together, recruited by Jamnalal Bajaj and Vinoba Bhave, they ran the Vidyalaya as a shared act of service — Pandit Kaka teaching and administering, Manorama Tai overseeing the kitchen, teaching children, and ensuring the school felt more like a home than an institution. Students came from across India and found not just education but warmth, structure, and the strange comfort of discipline tempered by care.
There is a less-known chapter.
While Pandit Kaka was working in Mul, a group of freedom fighters raided a British bank. They did not keep the money. They brought it to him. It was a vote of trust — the kind extended only to men whose reliability is beyond question. He took the bundle, silent and steady, as the British police got wind of the operation.
For several days, he lay low. Beside him were Dattoba Dastane and Apte Guruji — watchful, moving with purpose but without panic. The money, meant for the underground resistance, had to reach its destination. How he eluded the police dragnet, how he moved through their perimeter and smuggled the funds where they needed to go — he never boasted, never wrote it down. Those who knew, knew.
In that moment, he was not merely a Gandhian teacher. He was a krantikari in khadi — waging revolution without violence, practicing rebellion with restraint. He then returned to his school, his charkha, his ledgers, as if nothing had happened.
In 1955, he moved briefly to Nashik as principal of the Khadi Grama Vidyalaya before returning to Sevagram to head the Regional Planning Institute founded by Annasaheb Sahastrabuddhe. He became a central figure in the Gandhi Research Centre and helped organise the Gandhi Centenary programmes of 1969 with meticulous care.
When Dr. Sushila Nayar started MGIMS that same year, Pandit Kaka became her man Friday — a phrase that understates the reality. He took on the role of director for students during their Gandhi Ashram orientation month, ensuring that their introduction to Gandhian philosophy was practical and felt rather than theoretical and imposed. He participated in the Gyan Yatras. He was instrumental in starting Vinoba Bhave's Bhoodan Yatra from Sevagram. He did everything, all the time, without announcement.
And then came the administrative work that only someone of his particular combination of qualities could have managed: when MGIMS began conducting its pre-medical entrance examinations, it was Pandit Kaka who published the forms, oversaw applications, verified details, organised the examination centres, checked the marks, and prepared the merit lists. This was not glamorous work. It required precision, patience, and an absolute incorruptibility in an era when government admissions were routinely manipulated by political pressure and family influence. Under his watch, merit meant merit.
He also managed accounts, maintained hostel discipline, assisted with admissions, and still found time to sit with individual students who were struggling in their first weeks. He multitasked with the effortless grace of someone who never distinguished between important work and ordinary work — who understood that an institution is held together as much by the man who checks the merit list as by the woman who builds the hospital.
Students from the early batches of MGIMS remember his house beside the Principal's office — modest, door perpetually open, kettle perpetually on. They remember his khadi, the same fabric every day, worn without self-consciousness. They remember his voice — not loud, not declamatory, but with the particular quality of speech that comes from a man who has thought carefully before opening his mouth.
He was a fine orator in the Gandhian mode: speeches rooted in philosophy, designed to stir the conscience rather than dazzle the ear. He believed in simple living and high thinking, and he embodied it in every gesture — not as a performance but as a settled way of being that had been arrived at early in life and never questioned.
He moved through the campus with quiet dignity, never seeking attention, always available. Annasaheb Sahastrabuddhe was more than a mentor to him — friend, philosopher, guide, and eventually something close to family: Annasaheb's niece married Pandit Kaka's son Ratnakar. The bond between the two men was one of the deep, sustaining friendships that give institutions their invisible strength.
His brother Shivram aligned himself with the Rashtriya Swayamsevak Sangh. Pandit Kaka followed Gandhi. Their ideologies diverged completely. Their affection for each other did not. It was, those who knew both men said, a study in how genuine love can hold across genuine difference.
Cancer claimed him on September 1, 1977, in Sevagram — the place where he had poured his life's work, where his door had always been open and the kettle always on. He was sixty-eight years old. Manorama Tai survived him. They had five children: daughters Vijaya Potnis and Nandini Dewaikar, and sons Madhukar, Sudhakar, and Ratnakar.
MGIMS instituted the L.R. Pandit and Smt. Manorama Pandit Award — ₹500 to a first MBBS student for best performance in the Gandhi Ashram orientation camp held each year. It is a small memorial for a large presence.
Those who were there in the early years — the batch of 1969 to 1976 particularly — do not speak of Pandit Kaka as a memory. They speak of him as a presence. In every quiet act of institutional kindness, in every corner of Sevagram where a student sits at a charkha, in every merit list published without interference, something of him remains.
He never sought titles. He never raised his voice. He never wrote down the story of the bank money or the days of hiding with Dastane and Apte Guruji. He simply did what needed doing, with whatever the day required — an underground courier when the freedom struggle needed one, a warm presence when homesick eighteen-year-olds needed one, a meticulous accountant when a new institution needed one.
The kettle was always on. The door was always open. That was enough. That was everything.
- While working in Mul, a group of freedom fighters raided a British bank — they brought the money to him
- It was a vote of trust extended only to men whose reliability is beyond question
- For several days he lay low — alongside Dattoba Dastane and Apte Guruji — as British police got wind of the operation
- The funds reached their destination; the police dragnet was evaded
- He never boasted, never wrote it down — then returned to his school, his charkha, his ledgers, as if nothing had happened
- A krantikari in khadi — waging revolution without violence, practising rebellion with restraint
Dr Anant Damodar Ranade
Trained Eye Surgeon (Kasturba Hospital, Sevagram)
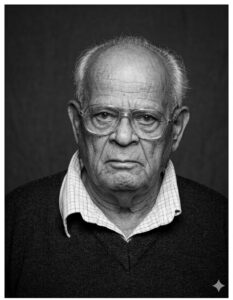
The bullock cart left before dawn. Two figures sat in it as it lurched down the red dirt roads of Vidarbha — a young doctor in white khadi and a determined nurse named Manimala Chaudhary. They were going to the villages to collect the harvest premium. Not cash. Jowar. A handful from one family, a sack from another, sometimes nothing but a smile and a promise. From this humble barter — grain for healthcare, goodwill for medicine — one of rural India's most enduring health insurance schemes was born.
The doctor was Anant Damodar Ranade. He was in his thirties. He would spend the next three and a half decades doing variations of this same thing: riding into villages, listening to people, operating on their eyes, delivering their children, and quietly building an institution around them. He never sought recognition. He wore the same white khadi shirt and plain chappals every day of his working life. When he finally left Sevagram in 1982, the institution he had helped found was training hundreds of doctors a year. He moved to Nagpur to live with his son and spent his days spinning on a charkha.
He died on April 29, 2019, one year short of a hundred.
Anant was born on February 22, 1920, in Jamkhandi, a princely state in what is now northern Karnataka's Bagalkot district. His father, Damodar Ranade, served as a superintendent under the local raja. The family were Chitpavan Brahmins, but their deeper allegiance was to Lokmanya Tilak's brand of nationalism. When Anant was old enough for school, his family sent him not to a government institution but to the National School in Chinchwad — a deliberate choice, rooted in the conviction that colonial education served colonial ends.
In the school library and in the magazines edited by Mahatma Gandhi, young Anant found his intellectual formation. At the urging of Annasaheb Sahastrabuddhe, he later visited Sabarmati Ashram, where he learned to farm, cook, clean latrines, maintain sanitation, and spin khadi. In 1930, when he was ten years old, the entire Ranade family adopted khadi. Anant would wear it every day for the rest of his life.
After matriculating in 1939, he enrolled at the Ayurveda Mahavidyalaya in Pune. While studying, he worked with the Rashtra Seva Dal and Congress Seva Dal. He earned the title Ayurveda Visharad and trained in eye surgery — a journey, as someone who knew him later put it, from pulse to scalpel. But history called louder than either.
In August 1942, Gandhi announced the Quit India Movement from Bombay. Anant, then in his final year of Ayurvedic training, threw down his books and joined the struggle. He was imprisoned for six months. When he was released and completed his training in 1943, he travelled to Bengal, where famine had already killed millions. While the British government diverted food to the military, ordinary people died in the streets. Anant worked among them. What he witnessed in Bengal — the geometry of poverty, hunger, and preventable disease — would never leave him.
He returned from Bengal and began working at Wai Hospital. On the suggestion of Dr. Lagoo, he travelled to Pune to meet Gandhi. Dr. Lagoo told the Mahatma simply: this boy wants to work in Sevagram. Gandhi turned to Dr. Sushila Nayar and asked whether she would take him on. She agreed without hesitation.
On January 10, 1946, Anant Ranade arrived in Sevagram. He was twenty-five years old.
The Kasturba Hospital at that point was still finding its feet — a small dispensary that had moved from a room in the ashram to Birla House, a modest building a few furlongs away. Dr. Sushila Nayar, trained in Western medicine, was managing the clinical work. Gandhi, characteristically, continued to advocate for naturopathy and traditional healing alongside her. The patients who came were desperately poor. Malaria, typhoid, leprosy, complicated deliveries, cataracts — illness was as present in Sevagram as the dust and heat. Many died young and unnecessarily.
Anant began by doing what the hospital needed: everything. He rode bullock carts to surrounding villages to provide primary care. He assisted with deliveries. He watched, learned, and steadily acquired clinical skills that his Ayurvedic training had not given him. He trained in cataract surgery. Later, he went to Calcutta to study leprosy management. He was methodical and unhurried in everything, qualities that made patients trust him and colleagues rely on him.
One early lesson came directly from Gandhi. Anant had carefully prepared a hospital budget — a total of ₹25,000, with ₹5,000 allocated to preventive care and ₹20,000 to curative services. He presented it to Gandhi with some pride. Gandhi glanced at it, frowned, and said: this belongs in the wastepaper basket.
Anant was shaken. Where had he gone wrong?
Gandhi explained: reverse the figures. Put four-fifths of your resources into prevention, one-fifth into cure. Only then can a society be truly healthy.
It was a principle Anant would carry into every initiative for the rest of his working life.
In 1948, Dr. Sushila Nayar left for a WHO scholarship at Johns Hopkins. She had entrusted Kasturba Hospital — wards, staff, supplies, accounts, and the surrounding community — to a man barely thirty years old. He managed it not with bureaucratic efficiency but with the quiet authority of someone whose commitment no one doubted.
The years that followed were difficult ones for the hospital. Gandhi Smarak Nidhi, which had taken over management after Gandhi's death, found the expenses high and considered handing the hospital to the government. The staff were alarmed. This was not a government institution — it was built on an idea, on community participation, on the Gandhian conviction that health belonged to the people it served.
Dr. Ranade and Manimala Chaudhary climbed back into the bullock cart. They went from village to village during harvest time, not demanding fixed contributions but inviting what people could give. Grain, coins, blessings. Out of these offerings, the health insurance scheme took its first organised shape. Families paid a small annual premium — initially twenty-five percent of already modest hospital charges — in exchange for reliable, affordable care. It was not a policy. It was a people's promise.
By 1955, the scheme was formalised. A family could insure itself for ₹10 a year. The currency was not profit but dignity. When ₹10 became ₹35 in 1985, and ₹600 in 2022, the principle remained intact. By 2024, the scheme covered nearly four lakh individuals. Over fifty thousand health insurance cards had been issued. What began with a cart and a bag of jowar had become one of India's oldest and most studied models of community-based health insurance.
For two decades, Anant Ranade was Kasturba Hospital's only eye surgeon. In the 1950s and 1960s, he conducted eye camps every Sunday across Vidarbha, often accompanied by ophthalmologists from Nagpur — Dr. Sutaria, Dr. Joshi, Dr. Kelkar — who came out of respect for him and the work. Villagers traveled miles, some on foot, some in bullock carts, drawn by word that this doctor's hands could restore sight.
He organized each camp with the precision of someone who understood that logistics were not separate from care — they were care. Days before a camp, he would visit the village, meet the sarpanch, identify a suitable site, arrange food for the patients and the medical team, and confirm transport. Then he would stay for the duration, operating through the day and sleeping in the village until the last patient had been seen.
His cataract surgery was performed with techniques far more rudimentary than those available today. What he had instead were steady hands, deep patience, and an intuitive grasp of what each patient needed. His outcomes spoke for themselves. People who had been blind for years left his camps able to see.
Dr. K.K. Trivedi, head of surgery at MGIMS and one of the first patients ever treated at Kasturba Hospital, recalls Ranade with the particular tenderness reserved for those who shaped you. "He was my closest friend in Sevagram," Trivedi says. "Whenever my parents visited, he would sit with them for hours. They spoke the same language — simplicity, service, rural India." Trivedi adds, with a soft laugh: "He even taught me to do cataract surgery. I may have operated on a patient or two under his watchful eye."
When MGIMS opened in 1969, a formally qualified ophthalmologist with an MS degree from Chandigarh was appointed. The new head was direct with Dr. Sushila Nayar: he could not tolerate an Ayurvedic practitioner performing cataract surgeries in a modern medical college. Either Ranade operated or he did. Not both.
What followed was a quiet, painful surrender. Years of service were set aside without ceremony. Dr. Ranade was given charge of the Ayurveda Outpatient Department, inaugurated on Makar Sankranti in 1976. He managed it without complaint, seeing patients six days a week, supported by Dr. C. Dwarkanath, one of India's most respected Ayurvedic practitioners, who served as honorary advisor. In 1976 alone, the OPD recorded more than four thousand patient visits.
He was also placed in charge of the hospital's medical store. He managed it with the same meticulous attention he brought to everything, knowing which suppliers in Bombay could be trusted, which lanes in Kalbadevi Street offered good instruments at honest prices. "He once took me to a tiny galli off Kalbadevi where Jamnalal and Sons operated," Trivedi recalls. "He negotiated fiercely. We never wasted a paisa."
By the early 1960s, it was clear that Kasturba Hospital needed a permanent, independent home — an institution capable of outlasting any individual. Dr. Ranade was central to the conversations that led to the founding of the Kasturba Health Society on September 11, 1964. The founding trustees were a small faithful group: Dr. Sushila Nayar, Manimala Chaudhary, Nalinbhai Mehta, Raghunath Shridhar Dhotre, Shriman Narayan of the Planning Commission, Laxmidas Shrikant of Gandhi Smarak Nidhi, and Dr. Anant Ranade.
It was Ranade, along with Manimala and Nalinbhai Mehta, who travelled to Delhi to persuade Dr. Sushila Nayar to lead the Society. She was hesitant. They would not leave until she agreed. The Gandhi Smarak Nidhi transferred hospital management to the new Society along with an endowment of ten lakh rupees, the interest from which covered the hospital's annual deficit. It was a quiet but decisive transformation — from an ashram-style institution sustained by goodwill into a professionally managed, community-rooted organisation. Five years later, in 1969, that organisation became the parent body of MGIMS.
Those who lived alongside Anant Ranade in Sevagram remember not just the physician but the person. He lived in Guru Nanak Colony, between the homes of Dr. G.R.K. Hari Rao and Manimala Chaudhary. His wife Nalini, trained in nursing and Indian classical music, gave evening baithaks in their modest home — gatherings where colleagues lost themselves in khayals and ragas. The house was a place of warmth in a community that could otherwise feel demanding and austere.
He was a Brahmin by birth who ate food prepared by Harijans, cleaned his own utensils, and participated in the ashram's prayers without theatrical devotion — simply, as part of daily life. He spun on a charkha. He attended community meetings and, as he once said, listened happily even to criticism. "I always believed we need people to point out what's wrong in the system," he said. "Without them, the hospital wouldn't run."
He never claimed credit and rarely spoke about himself. His famous remark — "I never hesitated in my life, never stepped back, and not for a moment was I bored with the work" — was made almost in passing, in writing, as if it required no elaboration.
No portrait of Anant Ranade is complete without Nalini. Born on November 10, 1931, in Dewas, she grew up in a household where her father — a bank employee and committed Gandhian — ensured that everyone wore khadi and that a khadi bhandar operated wherever he was posted. She attended Rashtriya Shala in Nadiad, a school following Gandhi's Nai Talim model, where education engaged the hand and the heart alongside the mind. She had learned classical music under Pandit Moreshwar Khare, and once danced before Gandhi at her father's request — and Gandhi laughed and encouraged the little girl warmly.
When she married Anant in 1949 and came to Sevagram, she became warden of the girls' hostel, leading all-religion prayers, nursing patients without squeamishness about cleaning wards or washing the sick, earning a BA while managing the hostel, learning multiple languages, and fostering generations of young women students with the same quiet strength she brought to everything. She left Sevagram with her husband in 1982.
His son Dr. Sharad Ranade — an ophthalmologist trained at IGMC Nagpur — settled in Nagpur with his wife Dr. Charulata, a practising gynaecologist. Their daughter Amruta, born in 1979, married Devendra Fadnavis, who would go on to become Chief Minister of Maharashtra. It is one of those quiet ironies that history occasionally produces: the granddaughter of a man who rode bullock carts through Vidarbha villages in a white khadi shirt, collecting jowar as health insurance premium, became the Chief Minister's wife. Anant Ranade would have found it faintly amusing, and then gone back to his charkha.
In his final years in Nagpur, Anant Ranade spun khadi, tended his garden, and read. His memory remained sharp into his late nineties. In 2019, he returned to Sevagram for a family function. He remembered the besan laddus made by Mrs. Gupta. He asked after Dr. Dhawan. He was ninety-nine years old.
"His departure from Sevagram wasn't how it should have been," Dr. Trivedi says quietly. "Sevagram forgot too easily. But I didn't. He was cut from the same cloth as Dr. Wardekar — spiritual, Gandhian, inspired by Vinoba Bhave. What he gave to Kasturba Hospital and later to MGIMS cannot be measured in years or posts. It was the soul of service."
He was not the kind of man institutions build statues for. He was the kind of man institutions are actually built by — in the before-dawn hours, on the back of a bullock cart, riding toward a village that needed someone to come.
Nalini Ranade was born on 10 November 1931 in Dewas, to Vishnu Narayan Bankar and Gangubai. Her parents later moved to Bilimora, Gujarat, where her father worked in a bank. But he was, above all, a stubborn Gandhian. Clad always in pure khadi, with a white khadi cap perched firmly on his head, he would go to the bank each day and, wherever he was posted, ensure a khadi bhandar was opened to promote the sale of khadi. Everyone at home wore khadi—it was not a choice but a way of life.
Nalini grew up in this environment. Instead of attending a government school, she went to Rashtriya Shala in Nadiad, a school that followed the Wardha Nai Talim Yojana, focusing on agriculture, craft, cleanliness, and self-reliance. Alongside academics, students learned drawing, music, sports, and practical skills—an education that shaped head, heart, and hand. She had just cleared her Class 10 exams when Dr. Anand Ranade from Wardha visited Nadiad, and soon after, they were married.
Nalini’s formative years had already been shaped by Gandhian institutions. Before coming to Nadiad, she had spent two years as a young girl at Sabarmati Ashram, learning various skills. Under the guidance of Panditrao Khare and his family, she received training in classical music and learned to sing mythological songs and bhajans, a love that would stay with her for life.
On a visit to Sevagram with her father, she met Gandhiji. At her father’s request, she danced before Gandhiji to a song composed in his honour. Gandhiji laughed, encouraging the little girl warmly.
Another turning point came when she was travelling by train to Wardha, singing softly to herself in the compartment. In that same compartment was Asha Devi Aryanayakam, who ran the Nai Talim school in Sevagram Ashram. Asha Devi, charmed by Nalini’s singing, invited her to Sevagram. There, at the end of the school’s evening prayer, Nalini was asked to sing a bhajan, an experience that gave her confidence and strengthened her bond with music.
After her marriage, Nalini moved to Sevagram. There, she became the warden of the girls’ hostel, where she actively participated in daily all-religion prayers and led bhajans. Sevagram was, in many ways, an extension of Sabarmati Ashram: a place where everyone shared in the mundane tasks of daily life without hesitation. She learned multiple languages, pursued arts, earned her BA, and received nursing training to serve in the Kasturba Hospital.
In the hospital, she did not hesitate to wash patients or clean wards, believing deeply that cleanliness was next to godliness—a virtue Sevagram reinforced in her. Whether it was caring for patients, leading prayers, or participating in community activities, Nalini Ranade embodied the spirit of silent, selfless service, nurturing countless young women under her care and carrying forward the Gandhian ideals she had imbibed as a child.
<p>1920 — Born in Jamkhandi, Karnataka<br />
1942 — Imprisoned in Quit India movement<br />
1943 — Worked during Bengal famine<br />
1946 — Joined Kasturba Hospital Sevagram<br />
1955 — Health insurance scheme formalised<br />
1964 — Kasturba Health Society founded<br />
1969 — MGIMS established<br />
1982 — Left Sevagram<br />
2019 — Died in Nagpur</p>
Dr. Ishar Dayal Singh
MBBS (King Edward Medical College, Lahore, 1937)
MD Physiology (Government Medical College, Amritsar / Punjab University, 1952)
PhD Physiology (University of Birmingham, UK, 1955)
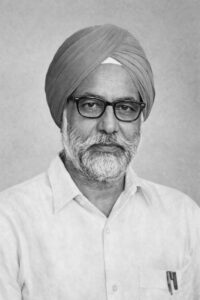
First Principal of MGIMS · Professor of Physiology · Soldier · Scientist · The Man Who Gave MGIMS Its Academic Spine
On September 1, 1969, a man in a neatly tied turban stepped onto the sun-baked platform at Wardha station. He had traveled a thousand kilometres from Punjab on a slow-moving train. He carried the quiet composure of someone who had already lived several demanding lives — soldier, researcher, teacher — and was now being asked to live another: the first principal of a medical college that did not yet fully exist.
Dr. Ishar Dayal Singh was not what people expected when they pictured a Punjabi. There was no bluster, no large presence filling the room. He was measured, deliberate, soft-spoken. He listened more than he spoke, and when he did speak, his words arrived with the particular weight of someone who had chosen them carefully. Dr. Sushila Nayar had asked the Punjab government to depute him for one year. He stayed for five. In those five years, he gave MGIMS its academic skeleton and something harder to name — a tone, a culture, a way of being an institution.
He was born on June 11, 1913, in Dharamsala, in the cool hills of Himachal Pradesh. His lineage carried a remarkable distinction: he was descended from Bhai Nand Lal Goya, the seventeenth-century Persian poet and devoted disciple of Guru Gobind Singh, the tenth Sikh Guru. Bhai Nand Lal had migrated from Persia some three hundred years earlier and settled in Multan. After Partition, the family settled in Patiala.
Singh completed his BSc with honours in Biology from Christian College, Lahore, and his MBBS from King Edward Medical College, Lahore, in 1937 — standing first in Medicine, Ophthalmology, and Surgery. His MD in Physiology came in 1952, delayed by the interruptions of history. A PhD from the University of Birmingham followed in 1955.
Between his MBBS and his MD, the world had gone to war. Singh served in the British Indian Army Medical Corps, rising to the rank of Major. The war shaped him — his discipline, his steadiness under pressure, his ability to function in conditions of uncertainty and scarcity. These were precisely the qualities that Sevagram would demand of him.
After the war, he returned to academia. An ICMR-funded research project. A Colombo Plan Fellowship that took him to Birmingham. A Wellcome Trust Fellowship in 1961 that carried him across the United Kingdom, Europe, Australia, Singapore, and the United States, building the international network of a serious scientist. He guided more than twenty postgraduate students. He published thirty-four original papers. His work on hepatic coma, published in The Lancet in 1954, established him as a researcher of international standing. He served on the editorial board of the Indian Journal of Physiology and Pharmacology.
By 1969, he was a man of considerable academic achievement, settled in Punjab, with no obvious reason to uproot himself for a half-built medical college in a Vidarbha village. Dr. Sushila Nayar asked anyway. He said yes.
What he found when he arrived bore little resemblance to the institutions he had known. There were no grand lecture halls. Laboratories were rudimentary. The first batch of fifty students had arrived, eager and uncertain. Faculty members recruited from across the country were still adjusting to life in a village — to the dust and heat, to the absence of urban conveniences, to the particular demands of an ashram-influenced campus where khadi was worn and evening prayers were attended.
The hospital was finding its rhythm. Patients arrived from surrounding villages with conditions that reflected the full weight of rural poverty and neglect. Courses needed to be structured, hostels set up, university affiliations secured, a culture of learning built from almost nothing.
Singh met each challenge without drama. He walked through half-built corridors, checked classrooms still smelling of fresh paint, sat with young faculty under neem trees to discuss syllabi. He drafted letters to government officials and university administrators, navigated the bureaucratic requirements of affiliation, and ensured the academic calendar ran on time. He was simultaneously Head of the Department of Physiology — teaching, guiding students, maintaining the research standards he had spent a career establishing — and the administrative anchor of the entire institution.
His most significant academic contribution was structural: he championed and helped design a two-year postgraduate programme in Community Medicine, ensuring that MGIMS graduated doctors who understood healthcare not merely as clinical treatment but as service to communities. It was a vision entirely consonant with Dr. Nayar's founding philosophy, and Singh gave it academic rigour and institutional form.
His salary was ₹1,710 per month, with a principal's allowance of ₹50. He never mentioned it.
There was another dimension to Dr. Singh that those who knew him in Sevagram remember with particular warmth.
He had been trained in Indian classical music since childhood. His instrument was the harmonium. In the evenings, when the day's clinical and academic work was done, students and faculty gathered in the ashram-style campus. Voices rose in bhajans — the devotional songs that had been part of ashram life since Gandhi's time.

In their midst, seated cross-legged on the floor, turban neat, fingers moving effortlessly across the keys, was the Principal. He led them in Vaishnav Jan To — Gandhi's favourite hymn, the one that describes the truly virtuous person as one who feels others' pain as their own. It was a sight that stayed with every student who witnessed it. A senior scientist, a man of international academic standing, a former army officer — sitting on the floor, playing music with his students, in a village in Vidarbha.
It said something essential about the institution he was helping to build, and about the man himself.
The campus in those early years was, as one who was there described it, a mosaic of many Indias. Banias and Brahmins, Dalits and Thakurs, Sikhs, Punjabis, Bengalis, and Marathas walked its shaded paths. Language, caste, and region — the usual fault lines of Indian institutional life — gave way here to the quiet solidarity of shared purpose. Harmony was not an aspiration. It was daily lived experience. Singh embodied it and quietly enforced it, not through policy but through his own person.
He retired as Principal in August 1974, handing over an institution that had found its footing. In 1975, his scholarly restlessness took him to Nigeria, where he joined A.B.U. Zaria as a visiting professor. When he applied for a professorship at the University of Ilorin, Dr. Sushila Nayar wrote him a letter of recommendation. It is worth reading in full for what it reveals — not just about Singh, but about how she assessed the people who had built something with her:
"Dr. I.D. Singh is an upright man of honesty, integrity, and ability. His conduct was always above board. He is an outstanding teacher whose research has received international recognition. He played a crucial role in establishing this institution, ensuring the primacy of community medicine and rural services. He is an able administrator and a fine human being."
She was not given to effusive praise. That letter, in its restraint and precision, was the highest endorsement she offered.
His wife came from Jhelum, now in Pakistan. His son settled in the United Kingdom as a physician. His younger daughter was admitted to MGIMS and later moved to Srinagar, where she completed her MBBS.
Dr. Ishar Dayal Singh came to Sevagram as a man of science — a decorated researcher, an experienced teacher, a former soldier. He left as something the institution needed more urgently than any of those things: its first steady hand, the person who had held the building together while it was still deciding what it wanted to be.The students who gathered around him in the evenings, listening to the harmonium fill the Vidarbha night with Vaishnav Jan To, were learning medicine. They were also, without quite knowing it, learning what kind of doctors they were meant to become.
| 1913 | Born, 11 June, Dharamsala — descended from Bhai Nand Lal Goya, poet-disciple of Guru Gobind Singh |
| 1937 | MBBS, King Edward Medical College, Lahore — first in Medicine, Ophthalmology, Surgery |
| 1939 | Joins British Indian Army Medical Corps — rises to Major |
| 1952 | MD in Physiology |
| 1954 | Paper on hepatic coma published in The Lancet |
| 1955 | PhD, University of Birmingham |
| 1961 | Wellcome Trust Fellowship — UK, Europe, Australia, Singapore, USA |
| 1969 | Arrives Wardha, 1 September — First Principal, MGIMS |
| 1969 | Designs two-year PG programme in Community Medicine |
| 1969 | Evening bhajans — harmonium, Vaishnav Jan To, students at his feet |
| 1974 | Retires as Principal, August — institution standing on its own |
| 1975 | Visiting Professor, A.B.U. Zaria, Nigeria |
Dr. M.L. Sharma
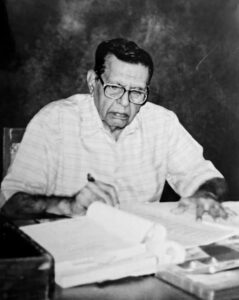
Professor & Head of Pharmacology · Principal · Forty Years at Sevagram · The Man Who Found the Place Where He Belonged
Twenty-five years after teaching their first pharmacology class, the 1970 batch of MGIMS invited Dr. M.L. Sharma to teach them again. He accepted. He was in his late seventies. His scalp hair was meticulously dyed, as it always had been. He stepped into the familiar classroom, now filled with former students and their families — the same people who had sat in those seats as nervous first-years, now doctors themselves, some of them senior enough to have students of their own. It was as if no time had intervened. The applause, as always, was thunderous.
This is a small story, but it contains the essential facts. A man who taught pharmacology at MGIMS for four decades was remembered well enough, and loved enough, that his former students wanted — decades later, with their own children present — to be in his classroom one more time. Not to honour him from a distance, not to give him a plaque, but to sit in the seats and hear him teach again. The invitation was itself a form of tribute: the highest one available, the one that said we want more of what you gave us.
"My class is an orchestra," he used to say, "and I just make sure everyone plays their part."
Mohan Lal Sharma was born on July 12, 1929, in Barwani, a town in Madhya Pradesh on the banks of the Narmada. His father was an Ayurveda physician — a household immersed in the logic of remedies and their relationship to the body's functioning, an early apprenticeship in thinking about how substances change the human condition. He graduated from Victoria High School in Barwani in 1947, distinguished in Mathematics and Chemistry.
In 1949, India had twenty-eight medical colleges. GMC Nagpur was the only one in central India, and he entered it at a time when Indian medical training was still finding its modern shape. He earned his MBBS in 1954, and it was during these years that Pharmacology asserted its claim on him — the discipline that examined not what was wrong with the body but what could be done about it, the science of mechanism and intervention, of how drugs acted at the cellular level and what they produced at the clinical level. He completed his MD in Pharmacology in 1958 under senior faculty at GMC, learning a discipline that was itself still developing its research identity.
His teaching career began during his postgraduate years and continued through a lectureship and then a Readership at GMC Nagpur. By 1970, he was forty-one years old, experienced, well-regarded, and formed in his understanding of what pharmacology education could be. That year, the Government of Maharashtra deputed him to Sevagram.
He arrived at MGIMS on December 24, 1970 — Christmas Eve — joining a founding group of faculty who were building an institution that was barely twelve months old. Around him were Dr. I.D. Singh in Physiology, Dr. B.V. Deshkar, Dr. K.N. Ingley, Dr. R.V. Agrawal, Dr. B.C. Harinath, and others — a collection of people who had agreed, for various reasons, to trade the established corridors of Nagpur for the dust and ambition of a Gandhian village. His departmental colleague Dr. M.D. Khapre would become the partnership that built Pharmacology at MGIMS. Their immediate task was teaching sixty first-year students — half from Maharashtra, the classroom a mix of Marathi, Hindi, and Punjabi speakers, all encountering medical pharmacology for the first time. Dr. Sharma and Dr. Khapre were the department's all-rounders: batting, bowling, fielding at every position, no task too small, no undertaking too large.
Dr. V.K. Gupta, who studied Pharmacology under him, tried to explain what it was like: "He made it stick. It wasn't just lectures. It was a show — funny, sharp, and always practical. A joke here, a story there, and suddenly, you understood. 'Forget memorizing,' he'd say, 'think practical.' He believed in showing us, not just telling us. Dogs, frogs — he brought the lab to life."
He did bring the lab to life. He conducted experiments with dogs and frogs — the standard animal pharmacology of that era — and made the mechanisms visible rather than merely describable. He published research in the British Journal of Pharmacology on adrenaline receptors and in studies involving pigeons — doing genuine science in a rural medical college, contributing to a literature that extended beyond MGIMS's walls.
His teaching method was deliberate. He understood that fear of a difficult subject was the first obstacle and that humour was not a distraction from learning but a dissolvent of the anxiety that prevented it. "People ask me how I teach," he said. "Honestly, it's as much about me learning as about them. You can't take yourself too seriously. Don't put yourself on a pedestal. A few jokes, even if they're on me, loosen things up. Shows them you're human, not some perfect figure with your own little quirks."
This was not false modesty. It was a considered pedagogy, applied for four decades without variation. The mock seriousness, the sudden infectious laughter, the shift between gravity and playfulness — these were how he kept sixty students in the same room with a difficult subject and left them understanding it. He held special sessions before examinations not to cover additional material but to address anxiety — to sit with frightened students and rebuild their confidence before the moment of testing.
Holi in Sevagram in the 1970s and 1980s carried a particular meaning: Dr. Sharma's jokes. He sat cross-legged on the ground while students drenched him in colour and spun stories that had the entire campus roaring. The teacher and the festival merged into a single composite memory that former students still carry decades later — the colours, his voice, the quality of the laughter, which was the laughter of people in the presence of someone who made them feel fully at ease.
From 1970 to 1974, he served as Vice Principal. From 1974 to 1984, he was Principal — taking over from Dr. I.D. Singh and leading MGIMS through a decade of consolidation, when the institution was moving from its improvised founding energy into a more established shape. He was also Founder Principal of Amravati Medical College. As Principal, his office was a place where grievances were received with humour and empathy. He understood when mischief needed to be checked, when leeway could be extended, when something was better left to resolve itself. He put people at ease without abandoning authority — a combination that is rarer than it sounds and that he exercised without apparent effort across a decade of leadership.
His relationship with Dr. Sushila Nayar was one of deep mutual respect expressed in the daily, physical language of conduct rather than declaration. He never walked beside her — always a step behind, arms folded behind his back, matching her pace with deliberate slowness. An unspoken acknowledgement of her stature, sustained not as ceremony but as genuine feeling, repeated every time they walked together across the campus for decades. She called on him to recite the Sunderkand — the chapter of the Ramayana celebrating Hanuman's devotion and strength — and he performed all the rituals with the meticulousness of a seasoned Brahmin: the pooja, the havan, the distribution of prasad.
He spent forty years on the MGIMS campus in rented housing. He never purchased a flat, built a bungalow, bought a scooter, owned a car, or boarded a plane. He said this not with the performance of virtue but with a quiet pride in the consistency between his stated values and his actual conduct. "My students are my true wealth," he said. "I've taught generations, and they're my biggest contribution to the college and to the world. I didn't practice medicine for money or obligation, but because I loved it."
He wore simple khadi bush shirts, trousers, and sandals. His hair was carefully dyed — a vanity he never apologised for and which the campus found charming rather than incongruous, the one concession to appearance in an otherwise entirely unadorned life. His eyes were described by those who knew him as the most expressive feature: compassionate, warm, the part of him that communicated before he spoke.
In 2009, he suffered a severe heart attack requiring bypass surgery in Hyderabad. The recovery was difficult. He returned to MGIMS and continued contributing. Then his wife died in 2012. Her loss was the heavier blow. Loneliness came, and health steadily declined. He chose to spend his final years at home in Sevagram, surrounded by what was familiar — the campus, the lanes he had walked for four decades, the institution he had helped build.
He died on August 10, 2015, in his Sevagram home. He is predeceased by his wife and by his son Dinesh, who had been in the MGIMS 1972 batch. He is survived by his son Satish, Professor of Pathology at MGIMS, and grandsons Pavan and Vijay, both MGIMS alumni — the pharmacologist's family embedded in the institution across three generations.
He had never left Sevagram in any meaningful sense. That was, perhaps, the truest thing that could be said about him: he had found the place where he belonged and stayed in it, completely, for forty years.
| 1929 | Born, 12 July, Barwani, Madhya Pradesh |
| 1947 | Graduated Victoria High School, Barwani — distinguished in Mathematics and Chemistry |
| 1949 | Entered Government Medical College, Nagpur |
| 1954 | Completed MBBS |
| 1958 | Completed MD Pharmacology, GMC Nagpur |
| 1970 | Arrived MGIMS, 24 December — founding faculty, established Department of Pharmacology |
| 1970 | Vice Principal, MGIMS — until 1974 |
| 1974 | Principal, MGIMS — until 1984 |
| 1974 | Founder Principal, Amravati Medical College |
| 2009 | Severe heart attack — bypass surgery, Hyderabad; returned to MGIMS |
| 2010 | Retired, 31 December — after forty years at MGIMS |
| 2012 | Wife died — the heavier blow |
| 2015 | Died, 10 August, at home in Sevagram |
Mechanism of peristaltic activity its modification by drugs
Effect of some important group of drugs on peristaltic activation in frog stomach, guinea pig ileum, goat ureter
Effect of some important metals, drugs on peristaltic activity in frogs stomach guinea pig ileum, goat ureter
Some of the Pharmacodynamic effects of Calcium channel blockers and Dopamine antagonists
Effect of some anti diarrhoeal drugs on peristaltic activity in frog stomach and guinea pig ileum
Dr. Kharak Singh Sachdeva
Postdoctoral Research (Vanderbilt University, Nashville, 1964)
First Dean of MGIMS · Principal · Professor of Physiology · The Man Who Gave the Institution Its Administrative Spine
Anyone who walked into Dr. Kharak Singh Sachdeva's office at MGIMS for the first time learned quickly that the first thirty seconds were the most important. He was a tall man, traditionally turbaned, salt-and-pepper beard, thick glasses behind which sat eyes that were large, piercing, and entirely without social lubrication. He would scan the visitor from head to toe, unhurried, before asking in a quiet but entirely firm voice: "Why have you come?"
It was not hostility. It was discipline expressed as a greeting — the manner of a man who had spent four decades in institutions and had no patience for time wasted or purposes unstated. Those who knew what they wanted got what they came for. Those who didn't generally left without it.
He was fifty-eight years old when he arrived in Sevagram in 1983. He had already retired as Director of Medical Education and Research for Punjab. He had founded a medical college, led departments, shaped curricula, and received a Rockefeller Foundation scholarship to Vanderbilt University in Nashville for postdoctoral research. He had, by any reckoning, done enough. He came anyway.
Sachdeva received his early medical education at the Sikh National College in Lahore and his MBBS from Glancy Medical College — now Government Medical College — in Amritsar. He joined the faculty there in 1950, the same year he married Bhupinder Kaur, a woman outside the medical profession who would stand steadily beside him through every transition his restless career would bring.
He spent eighteen years as Professor and Head of Physiology in Amritsar — a tenure that established his reputation as both an academician and an administrator. He ran the Boys' Hostel for five years, served as principal of the medical college for three, and by the time the Punjab government appointed him Director of Research and Medical Education, he had touched nearly every aspect of institutional life that a medical college contained.
In 1962, the Rockefeller Foundation scholarship took him to Vanderbilt University, where he spent two years in postdoctoral research. It was the kind of exposure that sharpened what was already sharp — bringing back not just new knowledge but the broader perspective of someone who had seen how medical education was conceived and delivered elsewhere. He returned to Punjab and continued building.
His most significant act of institution-building before Sevagram was the founding of Faridkot Medical College, where he served as principal and helped construct a new institution from the ground up. It was a role he would replicate, in a different register, at MGIMS.
He came to Sevagram in 1983 not as a candidate for leadership but as an emeritus professor of Physiology and warden of the Boys' Hostel — a quiet advisory role, appropriate for a man of his age and standing who had earned the right to work at a gentler pace. Dr. Sushila Nayar had other ideas.
On August 1, 1983, he was appointed Additional Professor of Physiology and Principal of MGIMS, stepping into the role previously held by Dr. G.R.K. Hari Rao. How the transition from hostel warden to principal occurred remained, to those around him, somewhat mysterious — one of those institutional evolutions that seems inevitable only in retrospect. He accepted the responsibility as he accepted everything: without drama, with steady resolve.
For nearly fifteen years, MGIMS had functioned without a Dean — only a Principal. The absence of the post was an unusual gap in the institutional structure of a medical college. In 1984, the management committee resolved to fill it. On February 8, Dr. Sachdeva appeared before a selection board that included Dr. Sushila Nayar, Dr. L.P. Agarwal of AIIMS, the Vice Chancellor of Nagpur University, the Director of Medical Education and Research, and the Director General of Health Services, New Delhi. He was the sole candidate. Six days later, on February 14, 1984, he became the first Dean of MGIMS.

He led the institution until April 3, 1990 — six years during which MGIMS consolidated what the founding decade had built and began preparing for what would come next. Despite his background in Physiology, he did not teach during this period. He gave himself entirely to administration, which was perhaps the truest expression of where his gifts lay.
His style of leadership was nothing like his predecessor Dr. M.L. Sharma's — whose warmth and humor made his office a place of easy conversation, where students came not just with problems but for company. Sachdeva maintained a strict, almost military-like distance. He was reserved, spoke rarely, kept professional boundaries firm. He never gossiped. He never sought camaraderie. He was often perceived as a loner by those who did not know him well, and as someone of formidable authority by those who did.
What he upheld, rigorously, were the founding principles of the institution. Khadi was worn on campus — by students, faculty, staff — and he led by example. Alcohol and non-vegetarian food remained absent from the premises. He attended the Friday all-religion prayer without fail, sitting cross-legged on the floor, listening intently as verses from Guru Nanak's teachings were recited alongside passages from other traditions. For Sachdeva, Dr. Sushila Nayar's requests were not requests. They were orders. His official circulars invariably opened with the phrase: As ordered by the competent authority. It was not obsequiousness — it was the expression of a man who had decided, upon arriving, that the institution's vision was worth his complete fidelity.
He lived in MLK Colony, a short walk from his office, and rarely used official vehicles. He moved slowly, always alone, acknowledging those he passed with a graceful nod. His life outside the office was marked by the same simplicity that governed it.
He was not an easy man to know, and did not particularly wish to be. Students found his office intimidating and his manner impenetrable. Faculty respected him without always finding him accessible. He was not the kind of dean who remembered birthdays or asked after families or created the warmth that makes institutional life feel like community.
What he created instead was something rarer and in its own way more valuable: an absolute consistency. Everyone knew where they stood. The rules were clear. The expectations were stated once. He did not need to repeat himself.
Those who came to him knowing what they wanted — a decision, a resource, a resolution — found him efficient, fair, and entirely free of the political maneuvering that bedevils institutional administration. He had no personal agenda beyond the institution's functioning. He wanted it to run well, to uphold its principles, and to be ready for whatever came next. By the time he handed the reins to Dr. M.L. Sharma on April 3, 1990, it was.
He and Bhupinder Kaur moved to the United States after leaving MGIMS — first Philadelphia, then Long Island, where a quieter chapter of life opened. Gardening. Travel. Family. The grandsons that six decades of institutional work had been conducted alongside, invisibly, as they grew.
He died at his home in the United States on November 11, 2012, surrounded by his family. Bhupinder Kaur survived him. Their three daughters — Navjeet, Manjeet, and Kulveen — and their families were his inheritance.
He had come to Sevagram at fifty-eight, when most men in his position were managing their decline, and spent six years building the administrative foundation that a young institution needed to stand securely. He asked for nothing in return except that the work be done properly. In an institution built by people who gave more than was asked of them, Kharak Singh Sachdeva was entirely characteristic — and entirely himself.
| c.1925 | Born, Punjab |
| ~1948 | MBBS, Glancy Medical College (now Govt. Medical College), Amritsar |
| 1950 | Joins faculty, Amritsar — marries Bhupinder Kaur |
| 1950 | Professor & Head of Physiology — eighteen years |
| 1962 | Rockefeller Foundation scholarship — two years, Vanderbilt University, Nashville |
| ~1970 | Founding Principal, Faridkot Medical College |
| ~1975 | Director, Medical Education and Research, Punjab |
| 1983 | Arrives Sevagram — emeritus professor and hostel warden |
| 1983 | Appointed Additional Professor of Physiology and Principal, MGIMS |
| 1984 | First Dean of MGIMS — appointed 14 February 1984 |
| 1984 | Friday all-religion prayer — cross-legged on the floor, every week without fail |
| 1990 | Hands over to Dr. M.L. Sharma, 3 April |
| 1990 | Moves to United States — Philadelphia, then Long Island |
| 2012 | Dies 11 November, at home in the United States |
Dr. Govind Manohar Indurkar
MBBS (Government Medical College, Nagpur) [1955]
MS Anatomy (Government Medical College, Nagpur) [1963]
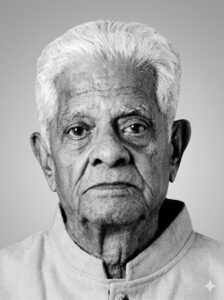
Professor & Head of Anatomy · Literary Critic · Playwright · Painter · The Anatomist Who Wrote About the Gita at 3am
At three in the morning, when Sevagram was entirely still, Dr. Govind Manohar Indurkar would sit at his desk and write about the Bhagavad Gita.
The house was quiet, the grandchildren asleep, the campus outside dark and unhurried. In those hours — before the dissection hall, before the students, before the day's demands assembled themselves — he found the stillness he needed for reflection. He had been waking this early for years, long before the Gita writing began. It was simply how he was constituted: a man who needed the predawn hours to think, to read, to be alone with what mattered to him most.
What mattered to him, it turned out, was a great deal. Human anatomy, certainly — he had spent a lifetime in its precise service. But also Kalidasa's poetry, Sanskrit scholarship, Marathi theatre, classical music, the flute, painting, anatomical illustration, and the philosophical teachings of the Gita which he eventually rendered into three books in Marathi, one written especially for young readers. He was an anatomist who could write literary criticism. A scientist who directed plays. A professor who painted murals.
He wore none of it for effect. He wore it all as naturally as he wore his simple white khadi kurta.
Govind Manohar Indurkar was born on June 12, 1928, in Nagpur, into an orthodox middle-class Brahmin family. His father worked for the Indian Railways and was posted to Adra, a railway colony in the Purulia district of West Bengal, where young Govind spent his early childhood. When financial pressures and the desire to give him a traditionally Maharashtrian upbringing converged, he was sent back to Nagpur to live with his grandfather and step-uncle. He completed his schooling at New English High School, passing matriculation with distinction.
His maternal grandfather — a schoolteacher of quiet discipline and intellectual rigour — was the formative influence of his childhood. The values he absorbed from that relationship — the steady daily routine, the primacy of learning, the idea that teaching was a form of service — stayed with him for eighty-three years.
He began medical studies at Mayo Hospital, then Robertson Medical College, now Indira Gandhi Government Medical College, in Nagpur, earning his LMP in 1949. Eager to advance and support his family, he joined the first batch of the shorter MBBS course at Government Medical College, Nagpur, completing his MBBS in 1955. He worked as an MMS Class II officer at a primary health centre in Amravati district, as a Medical Officer at Nagpur Central Jail, and ran a private clinic — accumulating the early-career variety that characterised his generation before he found his true direction.
That direction was anatomy. He returned to GMC Nagpur and in 1963, under the guidance of Dr. D.K. Kadasne, completed his MS in Anatomy. His thesis examined the spatial arrangement of the hepatic artery, bile duct, and portal vein within the liver — meticulous, structural, characteristically precise. He began teaching as a Lecturer in Anatomy at GMC Nagpur in 1961, was transferred to the newly opened GMC Aurangabad in 1963–64, and became a Reader in 1968.
In 1969, the Government of Maharashtra deputed Dr. Indurkar to the Mahatma Gandhi Institute of Medical Sciences, Sevagram — one of several faculty members sent to help establish what was to become India's first rural medical college. He arrived as a Reader in Anatomy in July 1969, two months before the first batch of medical students, and helped build the department from the ground up.
The colleague he worked alongside most closely in those early years was Dr. M.G. Kane, the first Professor and Head of Anatomy. They could not have been more different. Dr. Kane was strict, disciplined, and exacting — a man who wore his standards on his sleeve and did not suffer fools. Dr. Indurkar was quiet, humble, and gentle — a warm presence who made students feel safe enough to be confused without shame. Their temperamental contrast almost certainly served the department well: the rigour and the warmth, in combination, producing the balance that a new institution needs to take root.
What Dr. Indurkar brought that no other faculty member could replicate was an artist's eye applied to a scientist's subject. He created an impressive collection of surgically carved specimens and worked with the local artist Gajanan Ambulkar to produce anatomical murals based on Gray's Anatomy for the walls of the dissection hall. These murals — large, detailed, technically accurate, aesthetically considered — transformed a functional space into something more. Students memorising the brachial plexus or the branches of the aorta did so under the gaze of illustrations that had been made with care, not merely reproduced from a textbook. It was Dr. Indurkar's way of saying that the human body was worth looking at beautifully, not just correctly.
He left MGIMS when his deputation ended in August 1973 and returned to government service — posted through GMC Aurangabad, then Pune, Ambajogai, and Solapur, finally serving his last government appointment at GMC Nagpur before retiring in June 1986.
He was fifty-eight when he retired from government service. Within a month, he was back in Sevagram.
In July 1986, he joined MGIMS as Professor and Head of the Anatomy Department — his second tenure at the institution, seventeen years after his first. Dr. G.R.K. Hari Rao was still present as Emeritus Professor, Mr. J. Anbalagan served as Reader, and Mrs. R.R. Fulzele as Lecturer. He led the department for two years, steadily transferring responsibility to the younger generation before passing the headship to Mr. Anbalagan in June 1988.
He was quieter this time, more observer than driver. He had supervised PhD scholars including Dr. Palikundwar and Dr. Khanzode, contributed to doctoral work across institutions, and now watched his students take the reins. The department he had helped found in 1969 was now eighteen years old and producing its own researchers. He had seen it grow from nothing to this. It was enough.
In 1972, during his first tenure at MGIMS, he contributed an eight-page essay to Sushruta, the college's annual magazine. The essay was titled Meghadutatil Kavya-Saundarya — The Poetic Beauty of Meghaduta. It was a sustained literary-critical engagement with Kalidasa's poem, quoting extensively from the Sanskrit, offering translations and interpretations that read not like an academic exercise but like the work of someone who had lived with the text for years and found in it a genuine emotional home.
It surprised his colleagues. How could a professor of anatomy — a man who spent his days in the dissection hall, working with cadavers and memorisation charts and blackboard diagrams — write with this literary grace?
The answer, in retrospect, was simple: he had always been both things. He wrote essays for college publications throughout his career, including a memorable contribution to the MGIMS batch of 1969–70 souvenir. He wrote a critical appreciation of Shanta Shelke's Varsha Nayika. He contributed to a government project producing medical anatomy textbooks in Marathi. He translated Ratnakar Matkari's play Eka Olya Raatri into Hindi as Ek Bhigi Bhigi Si Raat. He directed Marathi plays for college and public events. He was a classical singer and a flute player.
He was fluent in Marathi, Sanskrit, Hindi, English, and Bengali. Marathi remained closest to his heart — the language in which he wrote his three books on the Gita, the language of his literary essays, the tongue of his maternal grandfather's household. The Gita books occupied his predawn hours for years, the third written specifically to make the text accessible to young readers.
There is a particular kind of person who moves with equal fluency between the rigour of science and the beauty of verse, between dissection and devotion, between structure and soul. They are rare. Dr. Indurkar was one of them, and the combination made him a richer teacher than either faculty alone could have produced.
After his second departure from MGIMS in 1988, he taught at Bijapur Medical College in Karnataka for about a year, then at Panjabrao Deshmukh Medical College in Amravati for two years, then at NKP Salve Institute of Medical Sciences in Nagpur. He stepped back from formal teaching around 1994–95, when the college shifted to a distant campus and his deteriorating vision and hearing made the travel unmanageable alone.
He did not stop teaching. He offered informal lessons at home to a few chosen students, free of charge, well into his later years. The last classroom was his own house. The students sat where his grandchildren sat. The textbooks were the same ones he had carried for forty years.
In June 2011, he was diagnosed with advanced metastatic cancer. He chose not to pursue aggressive treatment — a decision entirely consistent with the values that had guided his life. He died peacefully on August 31, 2011, the day before Ganesh Chaturthi. He was eighty-three.
He is survived by his wife Sushila, whom he married in 1952, their five children — three daughters, Sunanda, Vasanti, and the late Smita, and two sons — and his younger son Shrikant, who studied at MGIMS in the 1983 batch, sitting in the department his father had helped found fourteen years before he arrived.
| 1928 | Born, 12 June, Nagpur |
| 1949 | LMP, Robertson Medical College (now IGGMC), Nagpur |
| 1955 | MBBS, Government Medical College, Nagpur |
| 1961 | Lecturer in Anatomy, GMC Nagpur — begins teaching career |
| 1963 | MS in Anatomy, GMC Nagpur — thesis on hepatic artery, bile duct, portal vein |
| 1968 | Reader in Anatomy |
| 1969 | Arrives MGIMS, July — Reader in Anatomy, helps build department from nothing |
| 1969 | Anatomical murals for dissection hall — with artist Gajanan Ambulkar |
| 1972 | Essay on Kalidasa’s Meghaduta published in Sushruta — surprises his colleagues |
| 1973 | Leaves MGIMS — deputation ends, returns to government service |
| 1986 | Retires from government service, June |
| 1986 | Returns to MGIMS, July — Professor & Head of Anatomy |
| 1988 | Passes headship to Mr. Anbalagan — second departure |
| 1994 | Steps back from formal teaching — deteriorating vision and hearing |
| 1994 | Continues teaching informally at home — free of charge |
| 2011 | Diagnosed with advanced metastatic cancer, June — declines aggressive treatment |
| 2011 | Dies peacefully, 31 August — eve of Ganesh Chaturthi, age 83 |
Dr. G.R.K. Hari Rao
MSc Anatomy (Madras University) [1960]

Professor & Head of Anatomy · Discoverer of the Rao & Rao Artery · The Professor Who Asked If You Had Eaten Breakfast
He addressed every student as Babu.
It was a Telugu term of affection — warm, familial, entirely at odds with the chilly formality that anatomy departments typically maintained. Before an examination, Dr. G.R.K. Hari Rao would move through the hall asking each student individually whether they had eaten breakfast. He was short and slim, benign in manner, approachable despite his seniority. Students who had braced themselves for the severity of an anatomy professor found instead someone who seemed genuinely interested in whether they had slept, eaten, and arrived without too much anxiety.
He was not what they expected. He was considerably better.
Gopalakrishna Raghavendra Krishna Hari Rao was born on September 24, 1920. He earned his MBBS in 1949 and an MSc from Madras University in 1960 — at a time when a formal MS in Anatomy did not yet exist, which meant he found the nearest available qualification and worked within its constraints. He began teaching as a Demonstrator at Guntur Medical College in October 1950, and rose steadily — Tutor in 1953, Lecturer in 1958, Professor and Head in January 1962. Each promotion added a little more reserve to his manner, a little more measured weight to his words, as though responsibility had to be carried with the precision of the discipline he taught.
He did not merely teach anatomy. Alongside his colleague Dr. Vissa Ramachandra Rao at Rangaraya Medical College in Kakinada, he discovered a previously unrecorded blood vessel in the human body. The vessel was named the Rao & Rao Artery. Their paper — Dorso-Epithrochlearis Brachii — was published in the Journal of the Anatomical Society of India in 1956 and earned an invitation from the Royal College. It was the kind of contribution that settles a career's reputation in a discipline: quiet, precise, enduring.
By the time he retired from government service in Andhra Pradesh on September 30, 1975, he had published twenty-two research papers, served as Vice President of the Anatomical Society of India from 1971 to 1972, and in 1963 had been sent to the United States as a visiting professor on a USAID fellowship. He had supervised postgraduate theses, shaped a department for thirteen years, and earned a standing in Indian anatomical science that few of his contemporaries matched.
Retirement did not suit him. He took up a temporary post at Rangaraya Medical College in Kakinada. Then, in December 1976, he saw an advertisement in The Indian Express for a Professor of Anatomy at MGIMS, Sevagram. He was fifty-six years old. He applied.
The interview was held in Sevagram on January 12, 1977. Dr. M.L. Sharma, the Principal, informed him — almost apologetically — that the selection committee had recommended another candidate, placing Dr. Hari Rao on the waiting list. The chosen candidate declined the offer for personal reasons. The opportunity circled back. He was offered the post at ₹1,600 per month. His telegram of acceptance was characteristically brief: Will join the first week of July. On July 7, 1977, he arrived in Sevagram — steady, dependable, and at fifty-eight, just getting started.
The department he joined was seven years old. It had been shaped successively by Dr. M.G. Kane, the first professor and head, followed by Dr. D.T. Kolte, Dr. M.S. Parthasarathy, and Dr. G.M. Indurkar. The teaching staff included Mrs. P.R. Agarwal and Mrs. Belsare. It was a small department serving a medical college still in its first decade, with all the resource constraints that implied — persistent shortage of cadavers, no radiological imaging, no modern teaching technology. Anatomy education meant the dissection hall, the blackboard, and the text: Gray's, Sahana, Kadasne, Cunningham. Origins, insertions, nerve supplies, memorised with the thoroughness that the examination required.
In this environment, Dr. Hari Rao's teaching style stood apart from his predecessors. Where Dr. Parthasarathy had been strict and exacting — a man of discipline who kept the department in a state of brisk attentiveness — Dr. Hari Rao was something different. He brought anatomy to life not through authority but through genuine enthusiasm for the subject, illustrated teaching, and a quality of human warmth that made the dissection hall less forbidding. He guided his students through the body's intricacies with the patience of someone who had been doing this for thirty years and found it no less interesting than when he began.
He guided the PhD research of Mr. J. Anbalagan on the comparative anatomy of the pituitary gland — a study of structural variations across species, focusing on the onset of foetal pituitary function through the appearance of secretory granules in pituitary cells. It was the kind of research that requires a supervisor with both specialist depth and genuine investment in a student's development. Dr. Hari Rao provided both.
Under Nagpur University regulations and Kasturba Health Society rules, faculty retired at sixty. Dr. Hari Rao reached that age in September 1980. The university and society recognised what they had, and granted annual extensions. He continued as Emeritus Professor, receiving a nominal honorarium of ₹1,000 per year, teaching and supervising with the same engagement he had brought on his first day. MGIMS retained him until he was sixty-seven — a seven-year extension that reflected both institutional flexibility and the simple fact that good teachers are not easily replaced.
In July 1985, he found himself no longer Head of Department and unsettled by the requirement that all his correspondence to the Dean be routed through the new head. It was not, he reasoned carefully, a question of pride. It was a question of seniority — thirty-four years in service, twenty-four as a department head. The arrangement seemed impractical. He expressed a wish to be relieved.
Then Dr. Sushil Kumar Saxena, who had briefly joined the department, left in February 1986 — and Dr. Hari Rao found himself back in charge, as though the department could not quite release him and he could not quite release it.
By July 4, 1987, he knew the chapter was ending. He was sixty-seven, and the time had come to return to Guntur, where he had already built a home. On July 22, he wrote to Manimala Chaudhary — not an official resignation letter but something more personal, the letter of a man whose professional life and emotional life had become inseparable.
"We feel very sad. We miss you, dear Mithu and Behenji. Not a day passed in Sevagram without meeting and greeting each other. Such love, bond, and affection — we always enjoyed it. We also miss our good neighbors and friends."
Dr. Sushila Nayar wrote back on July 20 — a letter warm with the understanding of inevitable transitions, expressing wishes that he would bring his children to visit Sevagram, asking after his daughter Asha, passing on greetings from P. Nayar Behenji and Manimala Behenji.
These letters tell you something important about what MGIMS was, in those years, for the people who worked there. It was not merely an institution they were employed by. It was a community they belonged to — one that generated the kind of friendships, the daily encounters and small rituals of collegial life, that leave a real absence when they end. Dr. Hari Rao's sadness on leaving was not sentiment. It was the accurate recognition of what he was giving up.
He had lived in Guru Nanak Colony, next door to Dr. Anant Ranade and near others who had been his neighbours for a decade. He had walked the same lanes, attended the same prayers, shared the same modest institutional life that Sevagram offered. For ten years, it had been home.
He returned to Guntur, settled into the house he had prepared for this chapter, and lived the quieter life that retirement in one's hometown allows. He died in 2002. The Rao & Rao Artery — the blood vessel he and Dr. Ramachandra Rao had identified and named nearly fifty years earlier — remains in the anatomical literature, the most durable of his many contributions to a discipline he served with precision, dedication, and the particular warmth of a man who always asked his students whether they had eaten breakfast.
| 1920 | Born, 24 September, Guntur, Andhra Pradesh |
| 1949 | MBBS |
| 1950 | Demonstrator, Guntur Medical College — begins teaching career |
| 1953 | Tutor, Guntur Medical College |
| 1956 | Rao & Rao Artery named — paper in Journal of Anatomical Society of India |
| 1958 | Lecturer, Guntur Medical College |
| 1960 | MSc, Madras University |
| 1962 | Professor & Head of Anatomy, Guntur Medical College |
| 1963 | Visiting Professor, United States — USAID fellowship |
| 1971 | Vice President, Anatomical Society of India |
| 1975 | Retires from Andhra Pradesh government service, 30 September |
| 1976 | Sees MGIMS advertisement in The Indian Express — applies at age 56 |
| 1977 | Arrives Sevagram, 7 July — placed second, chosen when first declined |
| 1980 | Reaches retirement age — granted annual extensions as Emeritus Professor |
| 1987 | Writes farewell letter to Manimala Chaudhary — returns to Guntur |
| 2002 | Dies, Guntur |
Dr. Meena Ramdas Belsare
MS Anatomy (MGIMS, Sevagram) [1979]

Reader in of Anatomy · MGIMS · The Teacher Who Made the Subject Navigable
Twice in her life, a man decided what she would do with it.
The first time, her father — an architect who believed engineering was unsuitable for women — pointed her toward medicine. She complied without protest. The second time, her husband — a surgeon who felt clinical work would be too demanding for a woman — steered her away from anaesthesia toward anatomy. She complied again.
What is remarkable is not the compliance. That was the world she lived in, the one most women of her generation navigated without the vocabulary to name what was happening. What is remarkable is what she built inside the boundaries others drew. She arrived at MGIMS in 1975 with only an MBBS, no postgraduate qualification, no prior experience in anatomy. She left in 1983 as a Reader, with an MS earned mid-career while still teaching, having shaped seven batches of medical students — nearly 450 young doctors — in a discipline she had not chosen but had made entirely her own.
Meena Mhatre was born on September 24, 1941, in Murud Janjira, a coastal town in Maharashtra known for its formidable island fort rising from the sea. Her early years were spent in Palghar, then Mumbai, where she attended Parle Tilak Vidyalaya — known for its strict discipline — and studied Inter Science at Parle College under Bombay University.
She was a bright student who prepared simultaneously for the Group A mathematics path and the Group B biology path, keeping her options open. Her father closed one of them. She took the other and in 1962 secured admission to Topiwala National Medical College in Bombay, graduating in April 1967. A six-month house job at National Hospital followed, then rotations at G.T. Hospital, then three years as a Medical Officer with the Bombay Municipal Corporation's Health Department — the steady, unglamorous work of urban public health in a city that never slowed down.
In 1971, she married Dr. Ramdas Belsare. When he joined the Surgery Department at MGIMS, she followed him to Sevagram — a world away from Bombay in every respect that mattered. She took up a house job in anaesthesia, found her footing in the operation theatre, and seemed to be settling into clinical work when her husband suggested otherwise. She transitioned to Anatomy.
She joined the Anatomy department on July 5, 1975, appointed Lecturer on the strength of an MBBS alone — an appointment that required both Dr. Sushila Nayar's willingness to see potential where credentials were thin, and Meena Belsare's willingness to prove it warranted.
The department she entered was a formidable place. Dr. G.R.K. Hari Rao, Dr. Kolte, Dr. Kane, Dr. Parthasarathy — these were academics of strong personalities and strong opinions, who ran the dissection hall with an exacting discipline. No student entered without a proper dissection kit and a copy of Cunningham's anatomy text. Hair neatly trimmed, faces clean-shaven, white khadi aprons spotless, shoes polished. The atmosphere was one of rigorous, almost military, academic precision.
Among these more flamboyant figures — teachers who commanded attention through oratory, theatrics, and sheer force of presence — Meena Belsare found a different register entirely. She was quiet, unobtrusive, methodical. She did not perform anatomy. She taught it. Where her colleagues swept students along on the current of a powerful personality, she made the subject itself navigable — a map that could be read without fear, bone by bone, pathway by pathway, in the steady company of someone who would not make them feel foolish for not yet knowing their way.
"The students back then were a different breed," she recalled years later. "Disciplined, diligent, utterly focused. We lived and breathed anatomy — Gray's, Sahana, Kadasne, Cunningham. Page by page, we etched its intricacies into young minds."
She pursued her MS in Anatomy while teaching, completing it in 1979 under the guidance of Dr. Hari Rao. Her thesis examined the morphology of motor plates in fast and slow muscle fibres across several species — a quietly meticulous piece of research entirely characteristic of the woman. On November 5, 1981, she was promoted to Reader. She had arrived without a postgraduate degree and climbed the academic ladder through teaching, research, and persistent competence.
Those who were her students remember not just what she taught but how she looked teaching it. A prominent bindi on her forehead. A simple khadi sari. A mangalsutra. A single bangle. Modest chappals. She was the embodiment of the Sevagram aesthetic — simplicity worn without ideology, as a natural expression of who she was.
She lived in MLK Colony, a short walk from the department. She was so thoroughly embedded in the rhythms of the campus that to encounter her anywhere felt like encountering the institution itself — unhurried, purposeful, entirely without pretension.
Her husband Dr. Ramdas Belsare presented a striking contrast: broad-shouldered, confident, carrying the unmistakable authority of a senior surgeon. She was petite, soft-spoken, effortlessly self-effacing. They were not opposites so much as different expressions of the same dedicated impulse — one outward and declarative, the other inward and steady.
Arrogance never found a home in her. She sought no recognition, held no interest in institutional power, did not aspire to be larger than what the work required. Her world was the dissection hall, the first-year student standing before a cadaver for the first time, the particular combination of anxiety and curiosity that anatomy produces in young doctors who have not yet made peace with the fact of mortality. She met them there, in that combination, and helped them through it.
When Dr. Ramdas Belsare decided to leave MGIMS and open a private practice in Amravati, she followed him. On February 20, 1983, she submitted her resignation. Three months later, she left Sevagram.
It was the third time the shape of her professional life was determined by someone else's decision. She accepted it with the same grace she had brought to the previous two. She had, by then, learned that the geography of a career matters less than the quality of work done within it. She had taught nearly 450 students in eight years. She had earned her postgraduate degree mid-career. She had risen from Lecturer to Reader. Whatever Amravati held, she had established what she was capable of.
The transition was not smooth. At Panjabrao Deshmukh Medical College in Amravati, she began again as a Lecturer — a step backward in title, a wound that any academic would feel. The recognition came eventually. She was reinstated as Reader, then became Professor, then Head of Department, then Dean — retiring in 1999 having reached, through a longer and more circuitous route, the seniority she had earned.
Dr. Ramdas Belsare developed Parkinson's disease and dementia in his later years. She cared for him through the long decline until his death on May 26, 2019. Their three children took different paths: their elder daughter Sharmishtha became an ENT specialist in Amravati; their son Chaitanya earned a PhD in fruit science; and their younger daughter Sukanya, born in Sevagram, trained as a computer engineer before finding her calling as a spiritual teacher in San Francisco. Something of the quiet inward quality her mother embodied seemed to pass, in a different form, to the youngest.
In the memory of the students she taught — the batches of 1975 through 1982, now middle-aged doctors spread across the country — Dr. Meena Belsare occupies a particular kind of space. Not the legendary teacher whose lectures electrify a lecture hall. The other kind: the one whose patient, unhurried presence in the dissection hall made the subject feel manageable, whose quiet confidence in the student's ability was itself a form of teaching, and whose lessons — spoken in gentle tones, over cadavers and textbooks, in a dusty department in a village in Vidarbha — linger long after the words have faded.
| 1941 | Born, 24 September, Murud Janjira, Maharashtra |
| 1962 | Admitted, Topiwala National Medical College, Bombay |
| 1967 | MBBS — house job, National Hospital; rotations, G.T. Hospital |
| 1968 | Medical Officer, Bombay Municipal Corporation Health Department |
| 1971 | Marries Dr. Ramdas Belsare — moves to Sevagram |
| 1971 | House job in anaesthesia — steered by husband toward Anatomy |
| 1975 | Joins Anatomy department, MGIMS, 5 July — Lecturer on MBBS alone |
| 1979 | MS in Anatomy — thesis on motor plate morphology in fast and slow muscle fibres |
| 1981 | Promoted to Reader, 5 November |
| 1983 | Resigns 20 February — follows husband to Amravati private practice |
| 1983 | Joins Panjabrao Deshmukh Medical College — begins again as Lecturer |
| — | Reader → Professor → Head of Department → Dean, PDMC Amravati |
| 1999 | Retires as Dean, Panjabrao Deshmukh Medical College |
| 2019 | Dr. Ramdas Belsare dies, 26 May — she had cared for him through Parkinson’s and dementia |
Dr. Samit Kumar Ghosh
MS Anatomy (Maulana Azad Medical College, New Delhi) [1971]
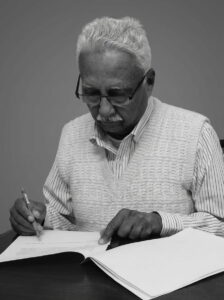
One evening around half past nine, the phone rang in Dr. S.K. Ghosh's quarters. The boys' hostel mess had run out of aloo sabzi. Without deliberation, he pulled on his kurta and dhoti and walked over. He cooked a fresh batch for twenty or thirty students himself, right there in the hostel kitchen. They stood watching, wide-eyed — this commanding professor, the man whose dissection hall presence made first-years straighten their spines involuntarily, standing over a pot of potatoes at ten in the evening because the boys needed to eat.
He told the story later with a smile. It was not, for him, a remarkable thing. It was simply what the situation required.
This quality — the complete absence of a gap between his public authority and his private generosity — was what those who knew Dr. Samit Kumar Ghosh most consistently described. He was fiery and exacting in the classroom, outspoken to the point of bluntness in meetings, capable of a temper that students found memorable. He was also the man who cooked for the hostel, adopted the stray dogs, watched the birds on Sunday mornings, and treated orderlies and artists and fellow professors as members of the same family. Both things were equally true. Neither cancelled the other.
Samit Kumar Ghosh was born on April 20, 1942, in Jalpaiguri, West Bengal, moving to Kolkata as a boy when his father's medical career required it. He grew up in a small fishing village — an upbringing that gave him a naturalist's attentiveness to the world around him and a self-reliance that came from having to find his own way. His relationship with his father was strained, a chasm he described as difficult to span. He decided early that he would be a self-made man.
His academic record was not distinguished. Third division in HSC, second division in Inter Science. In 1960, he joined Calcutta National Medical College — India's oldest, founded in 1848 — and struggled there too, failing his Medicine practicals on the first attempt. He graduated, completed two years of house jobs in General Surgery, Orthopaedics, and Cardiac Surgery in Kolkata, and harboured ambitions of going to Britain for further training. The plan did not materialise. He pivoted.
In 1968, he enrolled in the MS Anatomy programme at Maulana Azad Medical College in New Delhi — a decision that would define the rest of his working life. He completed the degree in 1971, began as a Demonstrator, and moved to the University College of Medical Sciences in December 1976 as Lecturer. By 1986, he was a Reader. He had spent nearly two decades building a solid academic reputation, and the professorship he had earned by any measure of merit remained out of reach — institutional politics at UCMS held more sway than qualification. Year after year, the promotion slipped past him.
By 1990, Delhi had begun to feel suffocating.
Then a colleague — a Professor of Gynaecology who sensed his restlessness — sent him a postcard. The message was brief: You might think of shifting to Sevagram. It's a place you might like. The following day, as if in orchestrated confirmation, he saw an advertisement on the UCMS Dean's notice board. MGIMS was looking for a Professor of Anatomy.
He met Dr. Sushila Nayar at her Connaught Place office in Delhi. She listened, assessed, and urged him to apply. He interviewed in Sevagram against one other candidate. His name alone appeared on the appointment list.
He stepped off the train at Sevagram station into a quiet so complete it startled him. No rush, no exhaust, no urban noise. The air smelled of earth. Nights were dark, broken only by owls. Mornings brought birdsong. As he walked the ashram's dusty lanes and took in the hospital's whitewashed walls, he felt — unexpectedly, immediately — at home.
It was not the life he had been living. It was the life that suited him.
The Anatomy department he inherited in September 1990 was small: Dr. Anbalagan, who had been serving as acting head, Mrs. R.R. Fulzele, and Mrs. K. Padmawathy, who joined shortly after. The department had a modest research culture, some teaching infrastructure, and the accumulated foundation laid by Dr. Hari Rao and others who had preceded him. Dr. Ghosh set about transforming it with the focused energy of someone who had spent nineteen years waiting for a department to lead.
He brought teaching, research, and academic ambition to the forefront simultaneously. He worked with Gajanan Ambulkar — the artist who had collaborated with Dr. Indurkar on the dissection hall murals — to develop histological resources and museum specimens. He worked with Khan, the orderly who handled cadavers, with the same directness and respect he gave his academic colleagues. He guided Dr. Anbalagan through the completion of his PhD a year after arriving. Within three years, postgraduate seats in the department — previously unfilled — were occupied, largely by Bengali students whom he had personally contacted and encouraged to apply. Dissection tables that had sat idle were now in use. Research on animal models was underway.
His teaching was precise, demanding, and memorable. He preferred chalk and blackboard to PowerPoint — not from technophobia but from conviction that the act of drawing structures in real time, visible to students as they emerged, was pedagogically superior to the finished image on a slide. His Bengali-accented English became, for generations of MGIMS students, the voice in which they first understood the brachial plexus or the anatomy of the posterior triangle.
He was strict. Punctuality was non-negotiable. Standards in the dissection hall were absolute. Students stood up straighter when they heard his footsteps in the corridor. And yet — as those who moved past initial apprehension consistently discovered — beneath the demanding exterior was a teacher who genuinely wanted them to succeed and a person capable of unexpected warmth.
From 2000 to 2007, he served as Warden of the Boys' Hostel — a seven-year tenure, the longest of any warden in the institution's history. Unaware that a furnished warden's quarters existed within the hostel, he continued living in his own home and came to the hostel each evening for two hours: reviewing documents, checking mess accounts, meeting parents, addressing student complaints, and maintaining the kind of steady, engaged oversight that a residential institution requires from those nominally responsible for it. The aloo sabzi episode was characteristic.
His major organisational achievements included the 1994 national conference of the Anatomical Society of India — hosted in Sevagram with minimal resources, successful enough that the delegates remembered the rural hospitality long after they had forgotten the academic proceedings — and the 2002 All India Cytogenetic Conference, which helped establish the genetics laboratory that would become a lasting feature of the institution. He guided Dr. Indra Ingole through her MD and PhD degrees, established postgraduate programmes, and built a departmental culture that outlasted his own tenure.
He was also responsible, in a quieter way, for the institution of Durga Puja celebrations in Sevagram — helping organise the annual festival for the Bengali community that had grown around the medical college, clad always in his signature white kurta and dhoti, as much a cultural anchor as an academic one.
On Sunday mornings, he sat in his backyard and watched birds. He had a trained ear for them — knew species by their calls as readily as by their appearance, could hear the presence of birds that remained invisible in the canopy. He grew plants and kept fish. When two street dogs appeared near his quarters, he and his wife Laxmi took them in — Kali and Lali — feeding them, giving them freedom, eventually bringing them on a train journey from Sevagram to Kolkata. They stayed with the family until 2015.
His wife Laxmi, from Barasat in the Ganges delta, had taught Bangla at Union Academy Senior Secondary School in New Delhi for twenty-eight years before retiring in 1998. She spent her retirement years in Sevagram, where she became a beloved figure — warm, generous, devoted to the dogs and to the community around her. She battled diabetes, high blood pressure, and heart disease with the same grace she brought to everything. When the family left Sevagram in 2007, she carried Sevagram with her. She died in Kolkata on January 13, 2009.
In 1999, drawn by a fascination with Tagore's writings and their connection to Kangra in Himachal Pradesh, he traveled there and found in its pine forests and tea plantations a landscape that gave him a peace he described as permanent. He returned to it in memory.
He retired from MGIMS on December 22, 2007 — the same year Dr. Anbalagan left, the two departures marking the end of an era in the department they had built together. He moved to Kathmandu, joining Nepal Medical College as Professor and Head of Anatomy, where he taught for another twelve years. His career in anatomical science spanned five decades, from 1969 to 2019 — beginning in a Delhi demonstration room and ending in Nepal, with seventeen years in a Gandhian village at its centre.
His son Saurav — MBBS from Maulana Azad Medical College, MS and MCh in Oncosurgery from Tata Memorial Hospital — briefly lectured at MGIMS before becoming Professor and Head of Surgery at Kolkata Medical College. The son of an anatomy professor who had to leave Delhi to find a professorship became, in his own right, a professor in Kolkata. The arc had straightened.
Dr. Ghosh was, as those who worked alongside him said, impossible to overlook and impossible to summarise easily. The old oak tree metaphor — towering and commanding above, rooted deep in kindness below — captures something true. What it does not capture is the Sunday morning stillness in the backyard, the ear cocked for a bird call, the man who had spent a week making sure a national conference ran properly in a village without infrastructure, now entirely quiet, watching the trees.
| 1942 | Born, 20 April, Jalpaiguri, West Bengal |
| 1960 | Joins Calcutta National Medical College — India’s oldest, founded 1848 |
| 1968 | MS Anatomy, Maulana Azad Medical College, New Delhi |
| 1971 | Demonstrator — begins academic career |
| 1976 | Lecturer, University College of Medical Sciences, Delhi |
| 1986 | Reader, UCMS — professorship blocked by institutional politics |
| 1990 | Postcard from a colleague — You might think of shifting to Sevagram |
| 1990 | Meets Dr. Sushila Nayar at Connaught Place — she urges him to apply |
| 1990 | Arrives MGIMS, September — Professor & Head of Anatomy |
| 1991 | Guides Dr. Anbalagan through PhD completion |
| 1994 | Hosts 43rd National Conference, Anatomical Society of India — Sevagram |
| 2000 | Warden, Boys’ Hostel — seven years, longest in MGIMS history |
| 2002 | All India Cytogenetic Conference — establishes genetics laboratory |
| 2007 | Retires from MGIMS, 22 December |
| 2008 | Professor & Head of Anatomy, Nepal Medical College, Kathmandu |
| 2009 | Laxmi dies, Kolkata, 13 January |
| 2019 | Retires from Nepal Medical College — five decades in anatomical science |
Effect of nicotine on developing chick embryo : A histological study of neural tissue
Effect of ethanol on neural tissue of mice :a histological study
Effect of ethanol on myocardium of mice: A histological study
Cytogenetic study in azoospermic oligozoospermic men
Effect of prenatal sound over stimulation on hippocampal area of chick brain Gallus domesticus
Morphological and histological studies of placentas associated with intrauterine growth retarded fetuses
Digito Palmar dermatoglyphics in vitiligo and alopecia areata
Long term effects of Monosodium glutamate in the gonads of adult mice following neonatal exposure- the histological study with assessment of reproductive performance.
Study of teratological effects of ultra high frequency (UHF) electromagnetic radiation on developing tissue of chick embryo. (PhD)
Dr. Jayaram Anbalagan
PhD Anatomy (MGIMS, Sevagram) [1994]

When the 1985 batch of MGIMS alumni planned their twenty-fifth reunion, there was no debate about who should be brought back to Sevagram. They flew him in from Puducherry. Not a founding trustee, not a dean, not a hospital administrator — an anatomy teacher. The gesture said everything about what Dr. Jayaram Anbalagan had been to the people who sat in his classes.
He was not what the role traditionally produced. The anatomy professor of institutional legend is a figure of severity — exacting, intimidating, the keeper of a discipline that first-year students find overwhelming and often fear. Anbalagan was something different. He was quiet, unhurried, possessed of a calm authority that never needed raising its voice. In the dissection hall, his chalk moved across the blackboard with a precision that turned complex structures into clear visual stories. Students who arrived anxious and confused left his classes with the specific relief of having understood something they thought was beyond them.
"Some people don't just leave impressions behind," a former student, Sadhana Bose, said of him. "They are the impression."
Jayaram Anbalagan was born on August 6, 1948, in Pondicherry — now Puducherry — to Jayaram and Duraikannu Ammal. He did not set out to be a doctor. In the 1960s, AIIMS, PGI, and JIPMER launched MSc programmes in Anatomy, Physiology, and other basic sciences to address India's acute shortage of medical teachers. The programmes offered a generous stipend — ₹500 a month — to attract bright science graduates. Anbalagan joined JIPMER's Anatomy programme, initially drawn by practical considerations, and stayed for reasons that had nothing to do with them.
He completed his MSc in Anatomy from JIPMER in 1974. In 1975, he left Puducherry and traveled 2,500 kilometres north to Faridkot, Punjab, to join the newly established Guru Gobind Singh Medical College as a Demonstrator. The first batch of MBBS students was arriving, the Anatomy department needed to be built from nothing, and Anbalagan threw himself into both — teaching by day, helping construct a department by incremental institutional effort, learning that building something from scratch required a different kind of stamina than inheriting something already standing.
He was promoted to Lecturer in 1980. By then, Punjab was changing. Militant violence and government crackdowns had made daily life unpredictable for those from outside the state. The unrest came closer. Safety could no longer be assumed. He made the difficult decision to leave — moving south to Vijayawada, where he joined Siddhartha Medical College as Assistant Professor of Anatomy.
He was still settling into the new city when a telegram arrived. It was from Dr. K.S. Sachdeva — his former principal at Guru Gobind Singh Medical College, now Dean of MGIMS in Sevagram. The message was brief: Come to Sevagram.
He was puzzled. How had Dr. Sachdeva found his address in Vijayawada?
When his train arrived at Sevagram station, he found Dr. Sachdeva on the platform, waiting to receive him. That personal gesture — a Dean coming to the station — told him something about the institution before anyone had explained it in words. Over the next few days, he met Dr. Sushila Nayar, Manimala Chaudhary, and Dr. G.R.K. Hari Rao. He felt, as he later described it, a sense of purpose in the place — a rhythm of life that settled something in him. He accepted the post.
In December 1983, he arrived at MGIMS as Reader in Anatomy. He would stay for twenty-one years.
He stepped into a department led by Dr. G.R.K. Hari Rao, with Mrs. R.R. Fulzele as Tutor and Mrs. Belsare as faculty. The department was small, the resources limited, the cadaver shortage a chronic constraint that made every dissection a carefully rationed learning opportunity. Anatomy education at MGIMS in the 1980s was traditional and rigorous — blackboard, chalk, Gray's Anatomy, Cunningham, and the expectation that students would memorise origins, insertions, and nerve supplies with thoroughness.
Within this environment, Anbalagan's teaching style found its fullest expression. His blackboard diagrams were exceptional — drawn freehand with a precision that made them more useful than most illustrations in textbooks, emerging structure by structure as he narrated what the body was doing and why it mattered. He knew when to push students deeper and when to ease back. He understood the specific anxiety of first-year students confronting a cadaver for the first time and calibrated his manner accordingly — never soft enough to allow complacency, never severe enough to produce the paralysis that prevents learning.
He was fluent in Tamil, Hindi, Punjabi, and Telugu when he arrived. He added Marathi at Sevagram — a language learned not from necessity but from the desire to belong more completely to the community he had joined.
In 1984, he began his PhD under Dr. Hari Rao's supervision, studying the histology of the pituitary gland — specifically the structural variations in its cells across species and the onset of foetal pituitary function through secretory granule appearance. When Dr. Hari Rao left MGIMS in 1987, Anbalagan found a new guide in Dr. S.S. Navgiri, Professor and Head of Anatomy at Government Medical College, Nagpur. He completed his doctorate in 1992 — eight years of part-time research conducted alongside full-time teaching, a demonstration of the particular persistence required to build an academic career without institutional support.
One of his most consequential contributions was establishing a PhD programme in Anatomy at MGIMS — a process that proved far harder than anyone anticipated. When the department first applied to Nagpur University for research recognition, the inspection committee rejected the proposal, citing inadequate facilities and the absence of a recognised guide. It was a significant setback.
Anbalagan did not accept it as permanent. Working with Dr. Narendra Samal, Head of Pathology, and Dr. Ved Prakash Mishra, he systematically addressed every deficiency the university had identified — upgrading the laboratory, strengthening the academic framework, satisfying each specific requirement. The approval came. The department produced its first PhD scholars, and the research culture Anbalagan had fought to establish became a lasting feature of the department's identity.
His partnership with Dr. S.K. Ghosh — who led the department from the late 1980s until 2007 — was the central professional relationship of his MGIMS years. They were temperamentally opposite: Ghosh was a passionate Bengali, outspoken and quick to express himself; Anbalagan was a soft-spoken Tamilian who preferred silence to confrontation. What they shared was an unshakable commitment to the discipline and an identical standard of expectation for their students. Their complementarity gave the department a stability and coherence that carried it through nearly two decades.
When Dr. Ghosh decided to host the 43rd National Conference of the Anatomical Society of India in Sevagram in 1994 — a national event in a small village with minimal infrastructure — he entrusted the organisation entirely to Anbalagan. As organising secretary, Anbalagan managed delegate registration, guest speakers, fundraising, accommodation, food, train bookings, and the logistics of hosting hundreds of academics in a place that was not built for conferences. The event was a success. Every delegate was treated, as those who attended remembered, like family.
He served as Vice President of the Anatomical Society of India in 1998–99, co-led symposia at the All India Congress of Cytology and Genetics held at MGIMS in 1996 and 2001, and attended the International Congress of Vertebrate Morphology in Delhi in 1994. His research contributions in microdissection and stereological methodology extended his influence beyond the institution.
In 2005, he made the decision to leave. His mother was frail and needed care. His sons, Vinod Kumar and Karthik Kumar, were preparing for college. The balance of obligation had shifted. He submitted his resignation and left Sevagram on March 9, 2005 — not to retire, but to continue teaching at Mahatma Gandhi Medical College and Research Institute in Puducherry, where Mahatma Gandhi's name, as he noted with quiet humour, followed him from Sevagram back to his birthplace.
Dr. Ghosh left MGIMS himself in December 2007, just months after Anbalagan. The two departures, so closely spaced, marked the end of the department's longest sustained period of academic coherence. The lecture halls they had filled for two decades stood quiet in a different way.
At MGMCRI Puducherry, Anbalagan became Professor, then Vice Principal, then Professor Emeritus after retiring in 2019 — continuing to guide students and doctoral scholars well past formal retirement. The medical faculty of the institution nominated him for the Dronacharya Award, the recognition for exceptional teaching. It was, characteristically, his colleagues who put his name forward. He would not have done it himself.
He still wears khadi. Asked about his years in Sevagram, he does not speak of research output or departmental achievements. He speaks of the community. "MGIMS was more than a workplace — it was a family," he has said. "Life in Sevagram was simple yet deeply fulfilling, with shared moments binding us together. It taught me that true contentment comes not from what we have, but from the purpose we serve."
Twenty-four batches of MGIMS medical students learned anatomy from him. Many of them are now doctors approaching the end of their own careers, their bodies carrying the knowledge he gave them in their bones and hands — knowledge acquired in a dissection hall in a village in Vidarbha, from a Tamil man who came to Sevagram on a telegram and stayed for twenty-one years.
| 1948 | Born, 6 August, Puducherry |
| 1974 | MSc in Anatomy, JIPMER, Puducherry |
| 1975 | Demonstrator, Guru Gobind Singh Medical College, Faridkot — builds department from nothing |
| 1980 | Promoted to Lecturer — leaves Punjab amid militant unrest |
| 1983 | Assistant Professor, Siddhartha Medical College, Vijayawada |
| 1983 | Telegram from Dr. K.S. Sachdeva — Come to Sevagram |
| 1983 | Dr. Sachdeva on the platform at Sevagram station — waiting to receive him |
| 1983 | Joins MGIMS, December — Reader in Anatomy |
| 1984 | Begins PhD under Dr. G.R.K. Hari Rao — pituitary gland histology |
| 1988 | Assumes headship of Anatomy department |
| 1992 | PhD completed — eight years of part-time research |
| 1994 | Organising Secretary — 43rd National Conference, Anatomical Society of India, Sevagram |
| 1998 | Vice President, Anatomical Society of India |
| 2005 | Leaves MGIMS, 9 March — returns to Puducherry for mother and sons |
| 2005 | Professor, MGMCRI Puducherry — Mahatma Gandhi’s name follows him home |
| 2019 | Retires as Professor Emeritus — continues guiding students |
Comparative study of kidney tubules in some vertebrates by micro-dissection histochemical and histological methods
Dr. Keshao Narayan Ingley
MD Physiology (Government Medical College, Nagpur, 1960)

Professor & Head of Physiology · Founding Faculty Member · The Man Who Made Students Feel What They Were Learning
In his final hours, his children placed earphones in his ears. Bhimsen Joshi's voice rose in a soulful abhang — Teertha Vitthala, kshetra Vitthala — and they were certain, as those who have loved someone long and well become certain of such things, that he could still hear it. They brewed his favourite tea and let a warm spoonful rest on his lips. No monitors, no machines. Just the sounds and scents of a life fully lived, brought to a man who had spent ninety-three years paying attention to beauty in all its forms.
He had chosen, at twenty-nine, not to operate on the human body but to explain it. His father was a surgeon of steady hands and calm words, known across Vidarbha. Young Keshao had stood in the corner of that clinic, watching pain soften and dignity restored, and felt something stir. But the scalpel was not his instrument. The chalk was. What called to him was the why behind the how — the hidden logic of the living body, the poetry of a heartbeat, the elegance of a reflex arc. He became a physiologist and a teacher, and for twenty years at MGIMS Sevagram, beginning on the very first day the institution existed, he was both with a completeness rarely seen.
Keshao Narayan Ingley was born on December 9, 1931, in Buldhana, the eldest of five siblings in a joint family that moved with his father's government postings across Vidarbha. New towns, new schools, new neighbours — a childhood of constant relocation that gave him adaptability and a particular attentiveness to people and places.
He entered Government Medical College, Nagpur, in 1953, joining the sixth batch of students. The course was long and demanding — anatomy and physiology, then pathology and pharmacology, then the clinical years. His batch was the first to undergo an eighteen-month internship that included nine months in district hospital wards and nine in primary health centres. Rural India, with its raw demands and limited resources, was built into his training from the beginning.
When the time came to choose a specialty, he followed the counsel of Dr. Shukla, the venerable Professor of Physiology and Biochemistry: if you want to build an academic life, get an MD. He chose Physiology. He began teaching at GMC Nagpur on February 1, 1960.
Then a bureaucrat's pen sent him to an Ayurveda college. The posting made no sense — a trained physiologist in a department where his qualification had no application. He declined, respectfully and firmly. "I'll wait," he said, "even if I must wait long." He waited nine years.
In 1969, the call came from Dr. P.S. Vaishwanar, his mentor, who had been asked to assemble faculty for India's first rural medical college. Dr. Sushila Nayar's MGIMS in Sevagram was still a vision on paper — no buildings, no laboratories, just dust and fields and a stirring idea. Dr. Ingley hesitated. Starting from scratch required more than resolve. But something in the rawness of it called to him. He agreed to go on deputation.
On the morning of Thursday, July 10, 1969, he arrived in Sevagram alongside Dr. B.V. Deshkar, Dr. M.G. Kane, and Dr. G.M. Indurkar. There were no gates to walk through, no lecture halls to enter. They were not stepping into a college. They were building one.
The Physiology department began not in marble halls but in modest rooms where chalk dust mixed with the black soil of Sevagram. There were borrowed benches, second-hand instruments, and a resolve that compensated for everything the place lacked in equipment. Jagdish and Sahebrao, two lab attendants from those early years, remembered how Dr. Ingley stayed behind long after others had left — unpacking crates, arranging instruments, setting up the lab piece by piece. Every pipette, every kymograph, every stimulator found its proper place. By the time students stepped in, the lab was not merely functional. It was waiting for them.
Lectures in those first months were held wherever a blackboard could be propped up — the Gandhi Ashram, the Adhyayan Mandir. Chalk was precious and blackboards makeshift, but the learning was real. The foundation was being laid by hand, day by day, in the heat of Vidarbha.
He stayed. The deputation became a calling. Over twenty years, from 1969 to 1989, he taught Physiology to twenty batches of MGIMS students — the first encounter each of them had with the body's hidden rhythms and rules.
He entered the lecture hall briskly, a paan tucked in his cheek, and went straight to the board — no notes, no slides, only chalk and certainty. His fingers moved with precision, drawing the nervous system stroke by stroke: the brainstem curved into view, spinal tracts unfurled like railway lines, synapses sparked to life in arcs and arrows. Watching him draw was like watching the body being born on a blackboard.
His power lay not only in what he knew but in how he made students feel it. When he taught Parkinson's disease, his face stilled, his limbs trembled, his feet dragged with tragic precision. Stroke: he slumped to one side, arm limp, gait halting. Cerebellar ataxia: he wobbled across the floor, arms outstretched, missteps exaggerated, drawing chuckles that turned into quiet admiration. He did not ask students to remember. He made them feel. They never forgot.
His tools were simple — Samson Wright, Guyton, Ganong, chalk, a pointer — but the experience was unforgettable. To him, Physiology was not a subject but a living force.
The laboratory was his other sanctuary. Every shelf spoke of order: electrodes coiled neatly, kymographs aligned, frogs anaesthetised and handled with respect. First-year students — nervous, tentative — found themselves pithing frogs without trembling, clipping electrodes with exactitude, watching the faint twitch of a muscle dance across a soot-blackened drum. Those inky waves told stories, and under his quiet tutelage, they learned to read them.
In an era when private tuitions flourished and some teachers in Nagpur traded lessons for cash and favours, Dr. Ingley never charged a rupee outside his salary. He never turned away a student who needed help. He believed teaching was a service, not a commodity. By holding that line, he protected the nobility of his craft.
At eleven in the morning and three in the afternoon, the Physiology department paused. Teacups appeared, cardamom scented the air, and Dr. Ingley arrived with his signature paan and a sparkle in his eye. Professors Sharma, Khapre, Patel, and Naik pulled up chairs. The talk ranged freely — examinations, politics, cricket, campus murmurs. Debates flared and dissolved into shared laughter. These tea breaks held no hierarchy and no agenda. They were the heartbeat of the department finding its rhythm.
He established a reproductive biology laboratory, mentoring Dr. Pradeep Sambarey and Dr. K.S. Bhat to investigate the causes of male infertility in Vidarbha — research that earned both men their doctorates. He built pulmonary function and basal metabolic rate laboratories. He guided postgraduate students including Dr. Deshpande and Dr. Ajay Chaudhari, who would later lead Physiology departments at JNMC Sawangi and MGIMS Sevagram respectively.
He helped nurture Sargam — MGIMS's annual cultural celebration — watching from the front row with pride, clapping hardest. He and Mr. Tupkar created the institute's sports department. He attended every football and volleyball match by the Brotherhood Club of Wardha, living each game rather than merely watching it.
Music was the deepest constant. A devotee of Bhimsen Joshi and Jitendra Abhisheki, he never missed a concert and always brought his children, insisting they sit up front. When Bhimsen Joshi sang an abhang, Dr. Ingley would sit upright, eyes closed, fingers tapping gently — not a physiologist, not an administrator, but simply a rasik, a lover of melody. Even in his nineties, each evening he settled into his chair, closed his eyes, and let Marathi classical sangeet wash over him.
On July 11, 1959, he married Sindhu Solao from Amravati district. She later served as warden of the MGIMS girls' hostel from 1981 to 1988. Their three children — Anjali, Sanjay, and Sonali — all graduated from MGIMS, specialising in Anaesthesiology, Orthopaedics, and Pathology respectively. Their daughter-in-law Aradhana and son-in-law Muthu Kumar were also MGIMS alumni. The family's roots in the institution ran four generations deep.
After retiring in December 1989, he joined the nascent medical college at Sawangi as Dean, then Director, building its faculty with the same quiet persuasion he had always used — making calls, paying visits, remembering names, following up with care. He served the university's examination and evaluation department until 2006, concluding his formal career at eighty-six.
In his mid-nineties, he retained a mental sharpness that surprised those who rang him expecting a brief exchange. On June 5, 2023, I called him as part of my efforts to document MGIMS's early teachers. What followed was an hour and a half of effortless, engaged conversation — stories told with precision, memory sharp, affection for the past unmistakable. He painted scenes rather than merely reported them. When the call ended, I found myself quietly moved. He was not recalling the past. He was still teaching.
Each morning in Nagpur, he descended from his sixth-floor apartment and took his place on a worn wooden bench beside the electrician, the auto-rickshaw driver, the plumber, and the shopkeeper. He chuckled at their jokes, passed the kettle without fuss, and never once spoke of the institutions he had built or the positions he had held. To them, he was simply Doctor Saab — a neighbour, a listener, a friend.
In October 2024, he was admitted to hospital after a series of seizures. I visited him there, surrounded by Sanjay, Sonali, Anjali, and his granddaughter Shreya. He looked tired, his voice faint. But when I stepped in, he opened his eyes, recognised me, and smiled. He asked about my health in sentences that came slowly, each word carefully coaxed. We exchanged pleasantries. Then his eyes grew heavy and he drifted into sleep. It was a quiet hour I will always hold dear.
His children brought him home to die. No monitors, no machines. They brewed his tea and placed Bhimsen Joshi's abhang in his ears. He passed on April 13, 2025, as he had lived — surrounded by devotion, dignity, and the music he had loved all his life.
| 1931 | Born, 9 December, Buldhana, Vidarbha |
| 1953 | Entered Government Medical College, Nagpur — sixth batch |
| 1960 | Began teaching Physiology at GMC Nagpur, 1 February |
| 1969 | Arrived Sevagram, 10 July — one of four founding faculty members |
| 1972 | Appointed Professor & Head of Physiology, MGIMS |
| 1981 | Wife Sindhu appointed Warden, MGIMS Girls’ Hostel |
| 1989 | Retired from MGIMS, December — twenty batches taught |
| 1989 | Joined Sawangi Medical College as Dean, then Director |
| 2006 | Concluded formal career at eighty-six |
| 2023 | Gave ninety-minute interview, sharp and engaged, aged ninety-one |
| 2025 | Died, 13 April, Nagpur — aged ninety-three |
A study on taster, non-tester sickling, G6PD deficiency, color blindness, function test based metabolic rate and protein bound iodine in rural population
The study of some physical and biochemical characteristics of semen in normal and infertile men
Investigations and management of male infertility in rural areas
Effect of drugs and other measures on seminogram in humans
Effect of drugs and other measures on seminogram in human
Investigations and management of male infertility in rural area
Dr. Sutikshna Pande
MD Physiology (Shyam Shah Medical College, Rewa) [1975]

Professor & Head of Physiology · Thirty-Five Years at Sevagram · The Teacher Who Believed in Students Before They Believed in Themselves
He drove at twenty kilometres an hour on Sevagram's still streets. Whenever residents heard the unmistakably loud horn of his second-hand Maruti and saw him pull up with his courteous offer — "Can I give you a lift?" — the standard reply, delivered with a smile, was: "No thank you, Sir. I'm in a hurry today."
The joke, gentle and affectionate, captured something true about Dr. Sutikshna Pande. He was unhurried in everything — in speech, in movement, in the measured way he delivered a concept in the lecture hall, waiting for students to catch up before moving forward. In a world that rewarded speed and output — papers published, conferences attended, grants secured — he was a quiet heretic. He published little. He attended few conferences. He taught for thirty-five years with chalk and a blackboard and the conviction that a well-explained idea, delivered simply and patiently, was worth more than any other academic currency.
The students he shaped are now senior doctors across the country. They remember his thick-framed glasses, the striking moustache, the crisp white coat buttoned to the top, the deliberate pauses in his lectures that made them lean forward to catch what came next. They remember that he explained physiology in Hindi when students struggled with English, that he stayed after class with those who were lost, that he treated first-year anxiety as a problem worth solving rather than a weakness to be dismissed. They remember that he believed in them before they believed in themselves.
That was his research output. It did not fit in a publication list.
Sutikshna Pande was born on March 23, 1939, in Singhpur, a small village in Narsinghpur district of Madhya Pradesh. His father was an agricultural officer whose postings moved the family continuously — Narsinghpur, Khandwa, Damoh, Raipur, Jabalpur. Young Sutikshna grew up acquiring the adaptability of someone who must always start again in a new place.
His name came from the Ramayana: Sutikshna was a devoted disciple of the sage Agastya, so dedicated that when he offered Guru Dakshina, his teacher refused it, saying the honour of teaching such a student was reward enough. It was a name that would turn out to be prophetic, though nobody could have guessed it from his early years.
Medicine was not his dream. He entered Netaji Subhash Chandra Bose Medical College in Jabalpur in 1958 to fulfil his mother's wish, not his own. It did not suit him. English was difficult, the subject did not excite him, and before his first MBBS examination he resolved to quit. The cost of withdrawal — ₹5,000, beyond his mother's means — kept him enrolled. He found another way out, taking a position teaching at a military school for boys. He kept his medical past a secret.
He loved it immediately.
He showed his students how to dissect frogs. He explained how the heart beats. They were fascinated. Six months into this work, a conversation with one of his students produced a quiet revelation: this was what he wanted to do. He returned to medical school, this time with a clear purpose. He turned morning tea breaks into impromptu tutorials for his batchmates, making optics and physiology accessible through informal explanation. A senior professor, Dr. N.K. Mishra — who would later head the Medicine department at Gandhi Medical College, Bhopal — noticed this unusual sight of a student teaching students and saw in it the markings of someone exceptional.
He graduated in 1967. The years that followed were uncertain — family planning posts in Damoh and Chandipur, district hospital work that brought ethical difficulties he navigated uncomfortably. It took six years to find his place. At Shyam Shah Medical College in Rewa, under the mentorship of Dr. D.N.S. Chowdhary, a wise anatomy professor who recognised his talent and directed him toward Physiology, he finally arrived. He became a demonstrator, then completed his MD in Physiology in 1975. At thirty-six, he had found his calling. He had known it was teaching since he was in a military school explaining how the heart beats. The road there had simply taken longer than it should have.
He arrived at MGIMS in November 1975. The institution was barely six years old. The Physiology Department had two senior faculty on government deputation — Dr. B.V. Deshkar and Dr. K.N. Ingley — and a recent vacancy left by Dr. I.D. Singh's departure. Dr. Pande joined as Lecturer, beginning the long steady climb that would take him to Professor and Head by 1999.
His classroom style was neither dramatic nor flamboyant, but it held students in a particular kind of attention — the attention produced by clarity rather than performance. He broke complex physiological principles into simple, digestible truths. He made the frog's beating heart a gateway into the mysteries of human physiology. He demanded that students grapple with concepts rather than memorise them, asking them to explain rather than recite. His sharp eyes behind thick-framed glasses swept the room; when a student's attention drifted, a quick "Focus!" followed. He did not shout. He did not need to.
He explained physiology in Hindi for students who struggled with English — a practical accommodation that other faculty rarely made and that students from Hindi-medium backgrounds never forgot. He was strict in the lecture hall and consistently available outside it, in the way that matters most to those who are struggling.
For six years, he served as warden of the boys' hostel, fostering a disciplined but caring atmosphere, helping new students adjust through orientation camps. For more than three decades, he led the Friday evening all-religion prayers at five o'clock — playing the harmonium, drawing on the Bhagavad Gita for guidance. He had led a Geeta Samiti during his Shyam Shah years, hosting annual eloquence competitions and philosophical debates. The Gita was not a performance of piety. It was the animating philosophy of his life.
Dr. Sushila Nayar recognised this. She frequently acknowledged his spiritual leadership at the institution — the contribution of a man who maintained the Gandhian devotional practice of the campus long after many faculty treated it as a formality.
He was a regular on the early-morning walks — out at four in the morning with Professor O.P. Gupta, or taking evening strolls with Professor Narang. He built his friendships through consistency of presence rather than expressiveness of personality. He was quiet among peers, slightly hesitant with seniors, yet deeply trusted by both. He was the professor who listened, the senior who defended his juniors, the mentor who gave without requiring return.
Among the thirteen Physiology MDs who trained at MGIMS between 1969 and 2003, and the many more MBBS graduates whose foundation he built, one name captures what Dr. Pande was to his students with particular vividness.
Devender Sachdeva arrived at MGIMS in 1994, lost and doubting himself. Medical school felt, as he described it, like a mountain he could not climb.
"Dr. Pande saw something in me," Sachdeva recalled. "He took me under his wing. He didn't just teach physiology — he taught me how to believe in myself. He talked to me about the Gita, about finding inner strength. It wasn't just academic advice. It was spiritual guidance, life advice. He never gave up on me, even when I had given up on myself."
Sachdeva completed his MBBS, specialised in Pharmacology, and now heads the department at Tomo Riba Institute in Arunachal Pradesh. He attributes it entirely to Dr. Pande.
There were others like Sachdeva — students who came to MGIMS uncertain and left with direction, whose trajectories changed because one professor had the patience to see them clearly and the commitment to stay alongside them until they found their footing. This was the research Dr. Pande conducted across thirty-five years. Its results walked into hospitals and departments and lives across the country.
In 1999, he stepped down as department head, passing leadership to Dr. Ramji Singh. He continued as Emeritus Professor for another decade before leaving Sevagram in 2010 for Ujjain, where he taught at Ruxmaniben Deepchand Gardi Medical College for fifteen more years.
When I spoke with him on May 19, 2023, his voice carried a sadness he did not try to conceal. "Sevagram lost its light after Behenji's passing," he said. "I felt detached. Students moved on after their Physiology studies. Frustration and disappointment led me to leave." It was the honest admission of a man who had given a place his best years and found that institutions, unlike devoted students, do not always register what they have received.
He continued teaching into his mid-eighties, donating much of his salary to help patients and those in need — a practice consistent with everything else he had ever done with resources that came to him.
In January 2025, he was diagnosed with Parkinson's disease and stepped down from teaching at Ujjain. Tremors came, then a walker. He remained active on Facebook, keeping himself informed about Sevagram, connected to the institution that had been the centre of his life for so long.
He married Anusuya Vyas from Gwalior in 1970. They chose not to have children. His students were his family — the slow accumulation of young doctors he had believed in, argued with, explained things to in two languages, and sent out into the world carrying something of his steadiness.
His story, as he himself seemed to understand, was not one of spectacular triumph. It was the story of a man who found his calling in teaching, who invested more than he extracted, and whose legacy lives in the doctors he shaped rather than the papers he published. It is, in the context of this book, one of the most important stories of all.
| 1939 | Born, 23 March, Singhpur, Narsinghpur district, Madhya Pradesh |
| 1958 | Entered Netaji Subhash Chandra Bose Medical College, Jabalpur |
| 1967 | Graduated MBBS |
| 1975 | Completed MD Physiology, Shyam Shah Medical College, Rewa |
| 1975 | Joined MGIMS as Lecturer, November |
| 1999 | Appointed Professor & Head of Physiology |
| 1999 | Stepped down as Head, passed leadership to Dr. Ramji Singh |
| 2010 | Left Sevagram after thirty-five years |
| 2010 | Joined Ruxmaniben Deepchand Gardi Medical College, Ujjain |
| 2025 | Diagnosed with Parkinson’s disease, January — stepped down from teaching |
Effect of feed on migrating myoelectric complex in rats
The involvement of monoaminergic mechanism to pain responsiveness in conscious rats
Dr. K. Shankar Bhat
PhD Physiology (MGIMS, Sevagram) [1992]

Professor & Head of Physiology · First Physiology PhD at MGIMS · The Man Who Counted His Blessings and Always Found Them More
His father had given him a piece of advice that stayed with him for seventy years: make two columns in life, one for blessings and one for difficulties, and you will find that blessings always outnumber hardships by a wide margin. If you understand this, you will always be content.
Kunhikatta Shankar Bhat understood it. A man who had wanted to be a doctor and could not afford the fees, who became a physiology teacher instead and found it suited him completely, who was made a hostel warden against his nature and found the role genuinely difficult, who retired from a long academic career and then — quietly, without drama — returned to the other inheritance his father had left him, performing Shiva Poojas and Ganapati Havans with the same sincerity he had brought to explaining endocrinology to first-year MBBS students. He counted his blessings. They outnumbered the hardships.
Shankar Bhat was born on September 18, 1946, in Mudipu, a small hamlet in Bantwal Taluka of Dakshina Kannada, Karnataka, the eldest of seven siblings. His father was a farmer and a priest — a lineage of sacred duties passed across generations that young Shankar absorbed without knowing he would one day return to it.
He was a bright student, moving through Sri V.V. High School in Kodlamogaru, PUC at MGM College, Udupi, and a BSc from St. Aloysius College, Mangalore. In the medical qualifying examination, he secured 71% — enough to earn admission to Mysore Medical College for MBBS. It was a genuine achievement. His father could not afford the fees. He let the dream go.
The route that opened instead was not a consolation prize. In the 1960s, India faced an acute shortage of medical teachers, and institutions including AIIMS, PGI, and JIPMER launched MSc programmes in Anatomy and Physiology, offering a stipend of ₹500 a month to attract science graduates. Bhat joined JIPMER's Physiology programme. Practicality brought him in; passion kept him.
The programme had one requirement he found genuinely distressing: students had to kill and dissect dogs, rabbits, guinea pigs, and cats for animal experiments. His upbringing and convictions would not allow it. "That was a very tough period," he recalled. "I don't know how I managed to get through without killing animals for experiments." He managed. He completed his MSc in Medical Physiology in 1973 and began looking for a place to teach.
He found one 2,500 kilometres north.
In 1974, he joined the newly established Guru Gobind Singh Medical College in Faridkot, Punjab — the same institution where Jayaram Anbalagan had arrived the same year, from the same programme, for the same purpose. They worked alongside each other under the same principal, Professor K.S. Sachdeva. The parallel was striking enough even then; it would become more so later.
After a year in Faridkot, he moved to Delhi, taking a post as Scientific Officer at the Defence Institute of Physiology and Allied Sciences — an institute focused on human performance research in extreme and wartime conditions. Pure research did not suit him. "I didn't want to spend my life with a pencil and rubber," he would say, with the directness of someone who had identified exactly what he needed from his working life. He craved a classroom.
Lady Hardinge Medical College provided that. The academic culture appealed to him, the students were engaged, and it felt, for a time, like home. But Lady Hardinge did not offer a PhD programme in Physiology, and his mentor Dr. O.P. Bagga urged him to look elsewhere for doctoral work.
In 1981, he appeared before the MGIMS selection board in Sevagram. Among the panelists was a familiar face: Professor K.S. Sachdeva, now Dean of MGIMS — the same man who had been his principal at Faridkot seven years earlier. Bhat's academic record was recognised with three salary increments at appointment, a gesture that signalled clearly what the institution thought of its new hire.
Settling into Sevagram was an education of its own kind. The Gandhian ethos — vegetarian food, Friday prayers, shramdan, khadi — was unlike anything in his previous experience. "For the first time in my life," he recalled, "I learned that you could survive months without money." He adapted. The simplicity, once unfamiliar, came to feel like the right register for a life he had always intended to live seriously.
He had married Ratna — an MA and MD in Hindi Literature from Andhra University — on February 19, 1977. They were allotted a Type-II quarter at Sevagram, later moving to MLK Quarters No. 10 after his promotion to Reader, where their neighbours included Professors O.P. Gupta, A.P. Jain, Sutikshna Pande, A.C. Tikle, and Dr. M.L. Sharma. It was the kind of residential community that forms naturally when people of similar professional commitment live in close proximity — bound by intellect, shared purpose, and the ordinary daily warmth of neighbours who become friends.
The department he joined was led by Dr. K.N. Ingley, with Dr. Sutikshna Pande as Reader. The three-member teaching faculty divided the subject between them: Ingley taught the nervous system, Pande covered cardiovascular and respiratory physiology, and Bhat took endocrinology and related topics. Together they delivered 180 lectures, 90 practicals, 40 demonstrations, and 40 tutorials to each batch of first-year MBBS students — an intensive commitment that left little ambiguity about where the department's priorities lay.
Bhat understood his students' position precisely. "They weren't seeking deep physiological insights," he said later. "Just a way to survive the first year and pass. The real understanding would come later." He taught accordingly — distilling Guyton and Ganong into clear, retainable notes, simplifying without falsifying, giving students tools they could actually use.
For his PhD, he chose semen analysis in infertile men — the department housed a well-established infertility lab, and the clinical question was genuinely unresolved. Dr. Ingley was his guide and, by Bhat's account, an ideal one: "He never interfered. He let me ask my own questions, design my own pro forma, collect and analyze my data, and write my thesis in my own way."
The research produced a finding that cut against the department's existing assumptions. Analysis of 300 infertile men revealed that the traditional drugs being used to treat infertility showed no impact. Men with very low sperm counts were simply least likely to father children, regardless of treatment. Dr. N.K. Tyagi's statistical work uncovered the pattern. The methodological limitations were real — no randomisation, no control group, ethics committees not yet active — but the finding was honest and the analysis careful. The PhD was awarded without a viva, reviewed by one internal and two external examiners who approved it in absentia. It became the first PhD awarded in Physiology at MGIMS.
In the mid-1980s, the institution appointed him Warden of the Boys' Hostel. His wife Ratna was simultaneously appointed Warden of the Girls' Hostel — an unusual domestic arrangement in which husband and wife each oversaw separate student residences, together responsible for the daily welfare, discipline, and safety of the entire residential student population.
He was a teacher and a researcher. He was not, by instinct or temperament, an administrator or disciplinarian. Boys broke curfew, returned late, tested the institution's rules with the creativity that boredom and youth reliably produce. Dr. Bhat, patient by nature, found the enforcement role genuinely uncomfortable.
Then Dilip Raghavan from the 1985 batch died in a motorcycle crash returning from Shirdi. Further incidents followed. Investigations began, pressure mounted, and the cumulative weight of a role he had never wanted became unbearable. He stepped down.
He did not blame the institution for assigning him the role. He understood that in a small campus with limited faculty, administrative duties were distributed as much by necessity as by aptitude. But the episode confirmed for him that his place was in the classroom and the laboratory — not in the corridors of the hostel at midnight, listening for the particular silence that meant someone had just done something they shouldn't.
He left MGIMS in November 1990, spending a brief period at a private medical college in Latur before joining D.Y. Patil College, Kolhapur, as Professor of Physiology. The private college world was materially better resourced and spiritually thinner. Students lacked the quality of seriousness he had known in Sevagram. He carried Sevagram with him — its students, its rhythms, its simplicity — in the way that those who have lived there always do.
From Kolhapur he moved to Yenepoya Medical College, where he led the Physiology department until sixty, then continued a further decade at the management's request, retiring finally in 2016 at seventy.
Teaching done, he returned to his father's inheritance. He immersed himself in Sanskrit texts, relearned ancient rituals, and began performing Shiva Poojas, Satyanarayan Poojas, Durga Poojas, and Ganapati Havans — not professionally at first but out of the pull of something that had been waiting for him. His sincerity was evident, and people sought him out. "The English education system distanced us from our heritage," he said. "But when you return to your roots, you find both meaning and a decent livelihood."
His son chose differently — an MBA from London, his own business. Every generation makes its own calculation.
The story of Shankar Bhat and Jayaram Anbalagan — the two South Indian MSc physiologists who took the same programme at JIPMER in the same years, traveled independently to the same medical college in Faridkot, worked under the same principal, and then arrived separately at MGIMS Sevagram within two years of each other, both completing PhDs there before returning to medical colleges in South India — is one of the quieter improbabilities of the MGIMS story. Tamil and Kannada, different departments, different years of arrival. The same arc, the same formation, the same Sevagram. Some parallels are too exact to be only coincidence and too incomplete to be called destiny. This one sits comfortably in between.
When Bhat was about to leave Sevagram, he bought a second-hand Luna. Dr. Pande bought one too. The two slow-moving vehicles, driven by two unhurried men who had each found their calling in a village in Vidarbha, navigating the same quiet roads at the same measured pace. It is as good an image as any for what Sevagram was, in those years, for the people who came to it and stayed.
| 1946 | Born, 18 September, Mudipu, Bantwal Taluka, Dakshina Kannada |
| 1973 | Completed MSc Medical Physiology, JIPMER, Pondicherry |
| 1974 | Joined Guru Gobind Singh Medical College, Faridkot — alongside Dr. Jayaram Anbalagan |
| 1975 | Moved to Defence Institute of Physiology and Allied Sciences, Delhi |
| 1977 | Married Ratna, 19 February |
| 1979 | Joined Lady Hardinge Medical College, Delhi |
| 1981 | Joined MGIMS Sevagram — three salary increments at appointment |
| 1985 | Appointed Warden, Boys’ Hostel |
| 1987 | Awarded first PhD in Physiology at MGIMS |
| 1990 | Left MGIMS, November |
| 1990 | Joined D.Y. Patil College, Kolhapur, as Professor of Physiology |
| 2016 | Retired from Yenepoya Medical College, aged seventy |
| 2016 | Returned to Sanskrit studies and priestly rituals — Shiva Poojas, Ganapati Havans |
Dr. Ramji Singh
MD: King George's Medical College, Lucknow (1975)

He meant it literally. During his postgraduate years at King George's Medical College in Lucknow, his research on the central action of Angiotensin II in dogs had begun with disaster — animal after animal dying under anaesthesia, an expensive imported reagent wasted, a supervising professor waiting for results that were not coming. The failure had driven him across the corridor to the Pharmacology department, where he spent long hours learning drug administration techniques, unearthed a buried head holder and mechanical drill from the department's dusty stores, designed specialised cannulas, and rebuilt his entire experimental technique from scratch. When he resumed the experiments, his hands were steady, the animals survived, and the research moved forward. The faculty who had quietly doubted the outsider — he was not a KGMC alumnus — saw what he was made of.
That capacity to fail, analyse the failure, and return with improved hands would become the defining characteristic of a career that took him from a village 100 kilometres west of Gorakhpur to the Executive Directorship of AIIMS Kalyani.
Ramji Singh was born in 1957 in Bansgaon, Gorakhpur district, Uttar Pradesh. His father Keshav Prasad Singh began as an assistant development officer and rose to block development officer, and with each posting the family moved — Maharajganj, Saunghat, Menhdawal, Bhatpar Rani — Ramji adapting to new teachers, unfamiliar accents, and different syllabi with every transfer. The disruption that would have defeated some students sharpened him instead. He learned to find his footing quickly.
His father's plan for him was modest and clear: become a doctor, return to Ballia, run a small private practice. There was nothing wrong with this plan. Ramji followed it without particular resistance, entering Sri Krishna Medical College in Muzaffarpur with the 1974 batch. Bihar's academic calendar was chaotic in those years — class suspensions, exam postponements, the institutional disorder that had worsened in the Emergency's aftermath — and what should have taken five years stretched considerably. He completed his MBBS in 1980.
He remembered one examiner from those years with particular warmth: Dr. S.P. Nigam, a distinguished Professor of Medicine from Sevagram, who tested him on a case of mitral stenosis during the First MBBS examinations. Years later, when Ramji joined MGIMS, he met Dr. Nigam again. The circle had closed quietly, as circles in the MGIMS story tend to do.
In June 1979, a few months before his Second MBBS examinations, he married Lalitaji. Their first son arrived in 1981. He was twenty-two, still in medical school, already a husband and father — the kind of domestic responsibility that concentrates a young man's ambitions.
He had intended private practice. A friend filling out postgraduate applications at King George's Medical College included Ramji's name on the form, ticking boxes for every subject including physiology and community medicine, unaware of the cutoff marks. Ramji was accepted into the Physiology programme. He reasoned that an MD would improve his prospects. He went.
What happened next surprised him. Under Professor S.D. Nishith, head of the Physiology department at KGMC, he found himself genuinely engaged by research for the first time. The Angiotensin II project had high stakes — ₹5,000 of the department's research grant spent on Swiss-imported reagent, a significant sum. When the initial experiments failed and the animals died, Nishith did not rescue him from the consequences. Ramji rescued himself: the corridor visits to Pharmacology, the excavated equipment, the redesigned cannulas, the rebuilt technique. The research recovered. He had learned something about himself that private practice in Ballia could not have taught him.
He did not receive a stipend during his postgraduate years — an unusual hardship for a married man with a child. His second son Ashok was born in October 1984. He worked as a demonstrator from September 1983 onward, the modest salary providing basic stability. He completed his MD in 1985, defended his thesis, and began scanning for lecturer posts.
His department head saw the advertisement for a post at MGIMS before Ramji did. He summoned Ramji, dictated the biodata to his secretary, wrote a recommendation letter in his own hand, and told them to airmail it the same day. It was the kind of mentorship that changes careers by acting before the student has organised himself to act.
The interview was scheduled for August 4, 1986. It was Ramji's first journey outside Uttar Pradesh — a 1,000-kilometre trip over twenty-eight hours. He stepped off at Wardha East station to find every cycle rickshaw taken. A man with two Lucknow students saw his predicament and gestured to a space in his rickshaw: "Come along, young man." Ramji arrived at his hotel opposite the station carried by a stranger's generosity.
The next morning, he walked onto the MGIMS campus — gravel underfoot, neem-scented air, the distant sound of ashram prayers. In the Physiology department, Dr. K.N. Ingley greeted him. Dr. M.D. Khapre nodded. Dr. Sutikshna Pande and Dr. K.S. Bhat welcomed him with warm smiles. The easy camaraderie of a small department that knew itself well settled his nerves before the interview began.
Dr. Sushila Nayar opened the proceedings: "Dr. Singh, if selected, how soon can you join MGIMS?"
"Immediately, ma'am," he said without hesitation.
She outlined the code of conduct: khadi, vegetarian diet, the Gandhian ethos that was not merely institutional decoration but daily practice. He listened and agreed. He had not known, arriving at Wardha station the previous evening, that this was the place he would spend the next twenty-six years. He knew it by the time he walked out of the interview room.
When he joined in September 1986, his life fit into a room at Kabir Niwas. Over the next decade, his footprint in Sevagram grew—first to the Type-2 quarters, then to a larger house in MLK Colony. Finally, in 2003, he moved a mile from the hospital to a home he had built himself. It was no longer just institutional housing; it was a house with his own gate and his own garden. By the time he turned the key in that front door, the village of Sevagram had officially ceased to be a workplace and had become his hometown.
He rose through the department steadily — Lecturer in 1986, Reader in 1991, Associate Professor in 1995, Professor and Head in 1998 — leading it for thirteen years. His teaching earned him the Professor K.P. Puthuraya Best Teacher Award in Physiology in 2008. He did not seek the award; his students and colleagues had made the case for it.
He registered for a PhD under Dr. K.N. Ingley in 1988, intending to continue the department's reproductive physiology research. The subject did not ignite him. He did not complete it. He was honest about this — a man who understood the difference between obligatory academic credential and genuine intellectual engagement, and who chose not to pretend the two were the same. What he did instead was become a PhD guide himself, mentoring Jyoti Jain, Sachin Pawar, Vinod Shende, Amit Kant, and Bharati Mahindrakar through their doctorates. He supervised postgraduate students from 2002 to 2012 — eight in total, from Alka Rawekar to Vikash Udan — and oversaw MD theses in the Surgery department as well, including work by Tapti Saha on post-meal urinary alkaline changes in duodenal ulcer management and by B.S. Bakane on TENS and surgical wound flap survival.
In December 1999, Ramji and Dr. S. John Premendran brought the 45th Annual National Conference of Physiologists and Pharmacologists to Sevagram. The theme was hypertension in the new millennium, but the true test was the terrain. To host 200 delegates in a village, Ramji had to revert to the scrappiness of his Lucknow lab days. He spent months navigating the bureaucracies of the ICMR and the Medical Council of India for grants, eventually bridging the gaps by leaning on family resources to ensure no guest went without a comfortable bed or a hot meal.
The logistics were an exercise in improvisation—transforming rural spaces into academic halls that rivaled urban centers. By the final day, the skepticism of the city delegates had been replaced by the quiet hum of a successful gathering. Dr. Sushila Nayar, then eighty-five, rose to deliver the presidential address. She moved slowly, her frame diminished by age, but as she stood at the podium and looked out at the assembly Ramji had built from nothing, she didn't need a formal commendation. She simply caught his eye, and in that steady, sharp gaze was the silent recognition of a mission fulfilled.
From 1998 to 2003, Ramji lived the double life of a professor and the Warden of the Jawaharlal Nehru Boys' Hostel. While the role was often viewed by faculty as a burdensome detour from academic work, Ramji turned the warden’s office into a space where the door stayed unlatched. He wasn't just checking room assignments; he was a constant presence in the corridors, listening to the anxieties of students far from home.
The "hostel boy" who sat in his office or shared a meal with him during that period eventually became the cardiologist in London, the oncologist in Mumbai, or the neurosurgeon in New York. These men didn't just remember him as an administrator; they continued to call him "Sir" with a tone that suggested family rather than faculty. Decades later, when these specialists reached back to Sevagram, it wasn't out of institutional duty, but because the warden of the Nehru Hostel had once treated their personal struggles with as much gravity as their physiology lessons.
When Dr. Ramji Singh left MGIMS in 2012, he wasn't looking for a quiet exit; he was seeking a larger canvas. He moved into the AIIMS system, first as Professor and Head of Physiology at AIIMS Patna, and eventually as the Executive Director of AIIMS Kalyani—perhaps the furthest point imaginable from the quiet clinic in Gorakhpur his father had once envisioned. Along the way, he held additional charges at AIIMS Deoghar and Guwahati, becoming a pillar of the burgeoning AIIMS network.
Yet, his influence wasn't merely administrative. His move opened doors for nearly two dozen MGIMS faculty members, a quiet testament to an institutional loyalty that followed him across state lines. Over four decades in the classroom and two decades in high-level administration, he balanced the rigors of national-level governance—serving as General Secretary of the APPI and as a Fellow of GSMC-FAIMER—with the patient work of a mentor, guiding Ph.D. students and chairing university boards.
His career has been defined by a refusal to stay static. After years in the Gandhian ecosystem of Sevagram and the structured world of the AIIMS institutions, he took on a new challenge as the Dean of a private medical college in Durg, Chhattisgarh. It was a move driven by a characteristic curiosity: a desire to understand the mechanics of private medical education in India.
He remains quiet about these transitions, carrying the steady confidence of a man whose self-worth doesn't rely on the titles on his door. He had arrived in Sevagram a stranger, shaped by a series of fortunate accidents—a friend’s application form, a timely recommendation, a chance rickshaw ride. He spent twenty-six years turning that stranger into a fixture of the community, proving through consistent work that most obstacles are not matters of destiny, but simply problems of technique.
Read Dr. Sushila Nayar's full profile in Architects of MGIMS
| 1957 | Born, Bansgaon, Gorakhpur district, Uttar Pradesh |
| 1974 | Entered Sri Krishna Medical College, Muzaffarpur |
| 1979 | Married Lalitaji, June |
| 1980 | Completed MBBS |
| 1983 | Joined KGMC Lucknow as Demonstrator — MD Physiology |
| 1985 | Completed MD Physiology, King George’s Medical College, Lucknow |
| 1986 | Joined MGIMS as Lecturer, September |
| 1991 | Promoted Reader |
| 1995 | Promoted Associate Professor |
| 1998 | Appointed Professor & Head of Physiology |
| 1998 | Appointed Warden, Jawaharlal Nehru Boys’ Hostel |
| 1999 | Organised 45th National Conference of Physiologists, MGIMS |
| 2008 | Awarded Professor K.P. Puthuraya Best Teacher Award in Physiology |
| 2012 | Left MGIMS after twenty-six years |
| 2012 | Joined AIIMS Patna as Professor & Head of Physiology |
| 2016 | Appointed Executive Director, AIIMS Kalyani |
The involvement of monoaminergic mechanism to pain responsiveness in conscious rats
A comparative study of free radical antioxidant status of anesthetic agent semen in fertile infertile men
The study of morphological and functional sperm indices in subjects of impaired fertility potential
Cardiac efficiency tests in medical students
Soleus H-Reflex in Chronic Low Back Pain
Nerve Conduction Velocity – A Normative Study
Electrophysiological Evaluation of Carpal Tunnel Syndrome in a Population of Subjects with Diabetes
Study of sperm deformity index (SDI), level of reactive oxygen species (ROS) and sperm function tests in normozoospermic and oligo-asthanoterato-zoospermic males
Effect of Noise Pollution on Hearing in Auto-Rickshaw Drivers – A Baep Study
A Study of Blink Reflex Alteration in Patients of Hypothyroidism and Type-2 Diabetes Mellitus – A Case Control Study.
Autonomic neuropathy, peripheral neuropathy and minimal hepatic encephalopathy in cirrhosis of liver: A clinical and electrophysiological study.
Dr. A.R. Chaudhari
MD Physiology: Mahatma Gandhi Institute of Medical Sciences, Sevagram (1987)

Professor & Head of Physiology · Thirty-Five Years at Sevagram · The Man Who Arrived at Two O'Clock, Every Day, for Thirty-Five Years
At exactly two in the afternoon, he would stride into the Physiology lecture hall, chalk in hand. Not at two minutes past. Not at one fifty-eight. At two. Students who had been in his classes long enough knew to be seated and ready before the hour turned.
His lectures were built the same way — meticulous, structured, delivered with the precision of someone who had thought carefully about what came first and what came next. He drew diagrams on the blackboard rather than projecting them on slides, sketched flowcharts rather than handing out printed notes, and required students to construct their understanding rather than consume his. "The chalk and blackboard force a teacher to think and students to engage," he said. It was not nostalgia for old methods. It was a considered pedagogical conviction, held and practised for thirty-five years.
He was not a showman. Dr. K.N. Ingley had performed Parkinson's disease in the lecture hall, wobbling and trembling to make students feel what they were memorising. Ajay Chaudhari did not perform. He explained — carefully, thoroughly, in a low husky voice — and trusted that clarity was its own form of engagement. For the many students who filled the Physiology lecture hall across three and a half decades, it was.
Ajay Rameshwar Chaudhari was born on July 11, 1959, in Wardha — the fourth of five siblings, with four brothers and a sister. His father Rajeshwar Chaudhari worked as a railway accountant; his mother Kamalabai ran the household with the quiet efficiency that holds a family together without drawing attention to itself.
The formative influence was his elder brother U.R. Chaudhari, a chemistry professor, whose home in Ramnagar was organised around learning. It was his brother who taught Ajay how to study, how to write, how to structure preparation for examinations. The lessons were absorbed early and stayed permanent. By the time Ajay moved through Buniyadi Bal Mandir, New English High School in Wardha, and J.B. Science College, the habits of disciplined academic work were already second nature.
In 1978, he secured admission to Government Medical College, Nagpur — twenty-fourth rank on the state merit list. He earned his MBBS in 1983, completed his internship, and found himself at the familiar crossroads of a newly graduated doctor: which direction now?
The answer came from Dr. C.B. Taori, a biochemistry faculty member at MGIMS and a close friend of his elder brother. "Why chase a clinical career?" Taori said. "Specialisations take years, and there's no certainty of getting your desired branch. Physiology has a vacancy — take it." It was practical advice delivered plainly. Ajay took it. He joined MGIMS as a Demonstrator in Physiology and enrolled in postgraduate studies under Dr. K.N. Ingley.
He had not chosen Physiology out of passion. Passion came later, in the way it often does in academic medicine — through the specific questions a subject opened rather than the subject itself. In Dr. Ingley's infertility laboratory, peering through a simple microscope at Neubauer chamber counts, something caught his attention and held it. Male infertility: its causes, its mechanisms, and the possibility of doing something about it. He completed his MD in 1987 and joined the department as Lecturer in 1988.
He entered a department of seasoned teachers: Dr. Ingley as head, Dr. Sutikshna Pande as Reader, Dr. K.S. Bhat, and Dr. Ramji Singh — a team with strong individual characters and an established culture of twice-daily tea gatherings at eleven and three. Dr. K.S. Sachdeva, who had been Professor of Physiology and Dean, joined those Saturday morning tea sessions and offered a consistent message to young faculty: "You must publish, or you'll remain an assistant professor for life." The nudge — "sometimes a shove," as Chaudhari recalled — pushed him and his colleagues to write and research beyond their lecture notes.
His own research settled on oxidative stress in male infertility — a subject understudied in India at the time. He examined antioxidant impacts on sperm count and motility, blood group antigens, secretor status and their correlation with sperm antibodies. He built a research culture in the department around the infertility theme, directing his postgraduate students into its many subsidiary questions: varicocele as a cause of infertility, immune responses, the edge cases where sperm counts reached near zero. The sperm quality analyser arrived in 2000, replacing the manual Neubauer chamber counts that had characterised the lab's first three decades. Precision improved; the underlying questions remained as pressing as they had always been.
His books entered the reading lives of MBBS students across the country. Viva in Physiology, published in 1988 — the year he joined as Lecturer — and Textbook of Practical Physiology in 2000 went through four editions each. They became staple reads because they did what he did in his lectures: simplified without falsifying, explained without condescending, gave students what they needed to understand rather than merely what they needed to pass. The combination of blackboard teaching and written texts that reinforced each other was characteristic of a man who thought about learning systematically.
He took over as Head of Department in 2012, following Dr. Ramji Singh and Dr. Sutikshna Pande. All three had served exactly eleven years as head — a numerical coincidence that became part of departmental folklore. He would serve eleven years himself.
Dr. Pande had been a strict disciplinarian, precise and demanding. Chaudhari carried that structural rigour forward but applied it with a gentler touch — less military in manner, equally serious in standard. Under his leadership, the department modernised its teaching methodologies and established a sports physiology laboratory, expanding the department's research scope beyond its long focus on reproductive physiology.
He was a fair leader. Residents, colleagues, lab technicians, and nurses found in him someone who did not make them feel their contributions were invisible. He was not given to grand gestures — the small, consistent acknowledgements of a man who noticed what people did and said so — but those around him understood that they were valued. His office, a small paper-filled room, became a place where people came not only for departmental business but for the quiet counsel of someone who listened carefully before speaking.
If he exceeded his lecture slot — spilling occasionally into the Community Medicine hour that followed — Dr. B.S. Garg's disapproving glare from the doorway was enough to wrap things up. He accepted this with the equanimity of a man who knew exactly what he was doing and why, and who also knew that institutional life requires occasional compromise with the clock.
His elder daughter Madura topped the state board examinations in 2007 — repeating, in a different generation, the discipline her father had inherited from his own elder brother. His younger daughter Rasika secured third rank in the Nagpur board, entered MGIMS in 2012, and went on to complete her MD in Radiology at GMC Nagpur. Two daughters, two medical careers, both shaped by the household habits of a family where learning was simply what one did.
He retired on July 31, 2023, passing the department to Dr. Shobha Paj, leaving behind a faculty that included Dr. Sachin Pawar, Dr. Nishant Bansod, Dr. Ruchi Kothari, and Dr. Vinod Shende. The department he handed over was larger, better equipped, and more research-active than the one he had joined as Demonstrator in 1983. The continuity was not accidental — it was the accumulated effect of a man who had spent thirty-five years making small, consistent investments in the department's future rather than his own prominence.
His real legacy was not in the books, though the books were good. It was not in the laboratories, though the laboratories were built with care. It was in the diagrams on the blackboard — drawn at exactly two o'clock, in a low husky voice, with a piece of chalk that forced both teacher and student to think — that would resurface in the memory of MGIMS students decades later, at a moment of clinical difficulty, when the physiology they had learned in Wardha turned out to be exactly what they needed.
| 1959 | Born, 11 July, Wardha |
| 1978 | Admitted to Government Medical College, Nagpur — 24th rank, state merit list |
| 1983 | Completed MBBS — joined MGIMS as Demonstrator in Physiology |
| 1987 | Completed MD Physiology under Dr. K.N. Ingley |
| 1988 | Joined as Lecturer — published Viva in Physiology |
| 2000 | Published Textbook of Practical Physiology — sperm quality analyser acquired |
| 2007 | Daughter Madura topped Maharashtra state board examinations |
| 2012 | Appointed Professor & Head of Physiology |
| 2012 | Daughter Rasika entered MGIMS — later MD Radiology, GMC Nagpur |
| 2023 | Retired, 31 July — passed department to Dr. Shobha Paj |
Dr. B.C. Harinath
MSc Biochemistry, Nagpur University (1961)
PhD Biochemistry, Oklahoma State University (1968)
Postdoctoral Fellow, Washington University School of Medicine, St. Louis (1969

Director-Professor of Biochemistry · Director JBTMRC · Forty-Four Years at Sevagram · The Man Who Named His Diagnostic Test After the Village
His friends teased him in his later years: "You've come full circle — from Bio-chemi-stry to Tree."
He laughed. He knew it was true.
The man who had spent four decades studying the molecular biology of parasites, building diagnostic kits, running immunodiagnostic workshops for medical schools across the country, and mentoring nineteen PhD students in the biochemistry of filariasis and tuberculosis — this man, in the last chapter of his Sevagram years, was planting amla trees on a fifteen-acre farm behind the boys' hostel. He had named the project Arogyadham. The Jain group from Jalgaon had helped him establish it. He tended the saplings himself. The carbon, hydrogen, and oxygen molecules he had studied for decades now appeared in the flowering shrubs and fruit-bearing trees he was cultivating by hand.
The campus was amused and a little fascinated. It was not a contradiction, exactly — it was a completion. A hard-nosed scientist from a small village in Andhra Pradesh had arrived in a small village in Maharashtra in 1970, spent forty-four years building something significant, and then, in the fullness of it, found his way back to the soil.
***
Bhaskar Chenappa Harinath was born on September 4, 1937, in Kallur, a village in the Chittoor district of Andhra Pradesh, sixty kilometres from Tirupati. He completed his BSc at the University of Madras in 1954, his MSc in Biochemistry at Nagpur University in 1961, and then — in the movement that would define the arc of his professional life — went to the United States, completing his PhD at Oklahoma State University and postdoctoral fellowships at Washington University School of Medicine in St. Louis from 1968 to 1969.
He arrived at MGIMS on April 24, 1970, one year after the institution admitted its first students. He came with a PhD from America, postdoctoral training at one of the world's leading medical research institutions, and the particular energy of someone who has been preparing for something important and has finally found the place to do it.
The department he was joining did not yet exist as a separate entity. Biochemistry and Physiology shared a combined department. In 1974, they split — Dr. Harinath taking charge of Biochemistry, Dr. Deshkar leading Physiology. What Dr. Harinath inherited was, in terms of equipment, faculty, and research infrastructure, almost nothing. What he brought was the training to build it from scratch and the temperament to insist that it be built well.
***
The research direction he chose was not obvious. Filariasis — the mosquito-borne parasitic infection that causes lymphatic damage and, in advanced cases, the disfiguring swelling of limbs — was a serious public health problem in rural India but not a prestige research area. It was the kind of disease that afflicts poor communities and receives attention proportional to their political influence, which is to say: insufficient. Harinath saw it as an opportunity precisely because it was underworked.
He built his department's research identity around it. He studied the immunology of filariasis, developed diagnostic methods, and created a diagnostic test he named SEVAFILACHEK — after Sevagram, the village where he had made his home and his laboratory. It was a deliberate act of naming: this diagnostic tool carried the village's identity into the scientific literature.
He recruited Dr. M.V.R. Reddy and Dr. G.B.K.S. Prasad from Sri Venkateswara University in Telangana, and together they published groundbreaking work on filariasis. His PhD students — P. Kaliraj, P. Rama Prasad, Kumud Parkhe, I. Kharat, Ashok Malhotra, V. Chenthamarakshan, K. Cheirmaraj, L. Jena, and others — formed what he explicitly cultivated as a family of filarial biologists. He guided nineteen PhD students between 1980 and 2011. He published over two hundred papers in international journals, operated from a village with no urban research infrastructure, and earned a reputation among immunodiagnostics researchers worldwide that had nothing to do with the prestige of his institution's address.
He ran popular workshops on immunodiagnostics in Biochemistry that drew medical schools across the country to Sevagram. He convinced Dr. Sushila Nayar to invest in equipment the department needed, arguing his case with the persistence of someone who understood that good research requires tools and that tools require institutional will to acquire them.
The Dr. B.C. Roy Award came in December 1993, recognising his contributions to the development of a specialty at MGIMS. He joined the company of Dr. Sushila Nayar, Dr. J.S. Mathur, Dr. P. Nayar, and Dr. Prakash Behere as MGIMS recipients of the Medical Council of India's most prestigious honour for specialty development. He served as President of the Indian Immunology Society from 1990 to 1992 and President of the Association of Clinical Biochemists of India from 1994 to 1995. He later patented the Mycobacterial ES-31 serine protease for tuberculosis diagnostics and established the MycoProtein-DB, a database for mycobacterial proteases.
***
Later in his career, he extended his diagnostic work from filariasis to tuberculosis — developing serological tests he believed would be effective tools for TB diagnosis. He invested significantly in this direction: time, effort, his department's research focus.
The Indian government eventually banned serological tests for TB diagnosis in favour of sputum smear microscopy and molecular tests, which had demonstrated evidence of superiority. His tests were effectively set aside.
It was hard for him. He had spent years on this work, believed in it, built around it. The frustration and disillusionment were real, and those who knew him could see it. Science requires the willingness to be wrong, but that willingness is easier to profess than to embody when a decade of effort is what is being set aside. His filariasis work remained a genuine and lasting contribution. The TB diagnostic work was a lesson in how even gifted and productive scientists can develop biases toward their own methods. He carried both parts of the record honestly.
***
He was outwardly impatient — known for occasional bursts of temper, a strict taskmaster who held his students and himself to high standards and was not gentle when those standards were not met. He spoke English with a distinct Telugu accent and never became fluent in Marathi or Hindi, which in Sevagram's linguistic community was a permanent marker of his outsider origin. He did not compensate for this with social effort — he was a man of few words outside the laboratory, not given to gossip or small talk, often more absorbed in mosquito-borne disease than human conversation.
Yet he earned genuine respect — from colleagues, from staff, from the influential figures in Sevagram's Gandhian world — through the quality of his work and the integrity of his conduct. In a village where simplicity was both an ethic and a daily reality, a biochemist from Andhra Pradesh who had trained in Oklahoma and St. Louis and then chose to spend forty-four years in Sevagram building a research department was understood to be doing something unusual. The choice itself commanded a certain regard.
As a mentor, he was demanding and inspiring in equal measure. His perfectionism was not mere exactingness — it came from a genuine belief that research done carelessly was not worth doing, and that students were capable of more than they typically asked of themselves. The research family he built, and the publication record that emerged from it, vindicated the belief.
***
He retired from MGIMS in 2014 and moved to Tirupati with his wife Vimla. The amla farm — Arogyadham — was behind him, but the impulse it represented followed him: an interest in Yoga, Naturopathy, and herbal medicine that deepened in his final years. He dreamed of creating a holistic health retreat and senior citizen homes in a nature-friendly environment. He donated nine acres of land near IIT Tirupati for the establishment of an orphanage — a late act of generosity from a man whose working life had been organised around building institutions that outlasted him.
His son Ashok, a 1984 MGIMS alumnus who had earned both his MBBS and MD at the institution, married his classmate Renuka Kulkarni, who completed her MD in Pathology at MGIMS. Both eventually settled in the United States. His son Anil, an engineer, also went abroad.
Dr. Harinath died on October 22, 2022, survived by Vimla and his two sons. He had arrived in Sevagram in 1970 as a young man freshly returned from America, full of ambition and research plans. He left in 2014 as someone who had built more than he had planned, in a place that had given him more than he had expected.
The amla trees at Arogyadham are still there. From Bio-chemi-stry to Tree: the journey, in the end, made its own kind of sense.
| 1937 | Born, 4 September, Kallur, Chittoor district, Andhra Pradesh — sixty kilometres from Tirupati |
| 1954 | Completed BSc, University of Madras |
| 1961 | Completed MSc Biochemistry, Nagpur University |
| 1968 | Completed PhD, Oklahoma State University |
| 1969 | Postdoctoral fellowship, Washington University School of Medicine, St. Louis |
| 1970 | Arrived MGIMS, 24 April — joined combined Biochemistry and Physiology department |
| 1974 | Biochemistry separated from Physiology — took charge of department |
| 1980 | Began guiding PhD students — nineteen students between 1980 and 2011 |
| 1990 | President, Indian Immunology Society — until 1992 |
| 1993 | Dr. B.C. Roy Award, December — MCI’s most prestigious honour for specialty development |
| 1994 | President, Association of Clinical Biochemists of India — until 1995 |
| 2011 | Last PhD student guided — thirty-one years of doctoral mentorship |
| 2014 | Retired from MGIMS — established Arogyadham amla farm, fifteen acres, behind boys’ hostel |
| 2014 | Moved to Tirupati with wife Vimla — donated nine acres near IIT Tirupati for orphanage |
| 2022 | Died, 22 October, Tirupati — survived by Vimla, sons Ashok and Anil |
Immunological study in filariasis
Lipid metabolism in pregnancy
Metabolism and mechanism of action of diethylcarbamazine
Immunodiagnosis of human filariasis
In vitro cultivation studies with filarial parasite
Immunodiagnostic studies in filariasis
Immunological Studies in Bancroftian Filariasis
Studies on filarial excretory and secretory antigens
Studies in Filarial excretory and secretory antigens
Detection treatment and immuno-monitoring of filarial patient
Immunochemical approaches for diagnosis of Filariasis
Immunological and Immunoprophylactic Studies in Filarial infections
Diagnostic use of filarial antigen and antibody isolated from hydrocele fluid
Humoral immune response in pulmonary tuberculosis
Filarial antigens of Diagnostic and Prophylactic Importance
Immuno-diagnosis of extra-pulmonary tuberculosis
Studies on in vivo released filarial antigens
Isolation, Purification and Diagnostic use of Mycobacterium tuberculosis excretory secretory antigens in Tuberculosis
Studies in Mycobacterial and nerve antigens in Leprosy
Oxidative stress and effects of antioxidants supplementation in carcinoma of upper digestive tract and oral submucous fibrosis
Studies on in vitro and vivo released mycobacterium tuberculosis antigen in tuberculosis
Utility of ES-31 and ES-41 antigens for immunoscreening of pulmonary and extrapulmonary tuberculosis – hospital case study
Biochemical and immunological studies in tuberculosis
Isolation and characterization of filarial antigens with Diagnostic and prophylactic potential
Studies on circulating antigens in tuberculosis
Isolation, Characterization and; possible function of certain mycobacterial excretory secretory antigens of diagnostic interest
Studies on Mycobacterial Excretory-Secretory protein antigens of diagnostic interest in HIV-TB coinfection
Mr. Chaturbhuj Taori
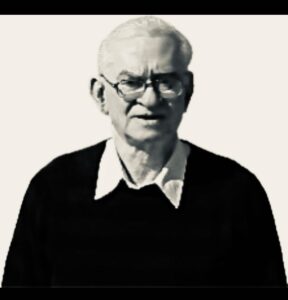
Lecturer & Reader, Biochemistry · Thirty-Six Years at Sevagram · The Man Who Built the Laboratory No One Noticed Until It Was Gone
On November 5, 2009, Gopal Taori handed his parents the keys to a house.
He had bought it in Nagpur — large, beautifully furnished, a real home for their retirement, the kind of gift that takes years of planning and love to give. He also handed his father the keys to a new Maruti Swift Dzire. Mr. Taori wept. His wife Veena wept. Their son had given them everything he wanted to give them, and they knew it, and the afternoon was saturated with that particular happiness that comes when gratitude and love and the passage of time all arrive together at once.
The following afternoon, brimming with joy, Mr. and Mrs. Taori set off for Sevagram. Mr. Taori was behind the wheel. A little ahead of Khadki village, their car collided with a truck. Both of them were gone.
It is rare to journey through life together and depart together. Mr. and Mrs. Chaturbhuj Taori were among those few.
***
Chaturbhuj Taori was born on January 20, 1945, to Kausalya Devi and Bansilalji, the second of five children in a Marwari-speaking family in Pulgaon, Wardha district. His name — Chaturbhuj, meaning one with four arms, an epithet of Lord Vishnu — was auspicious and weighty. He went by C.B. Taori throughout his life, the initials a modest reduction of a name that might otherwise have seemed to promise more than any one person could deliver.
He was a capable student. He matriculated from R.K. High School in 1960, completed his BSc in 1965, and earned his MSc in Biochemistry from Nagpur University in March 1968, securing the second rank on the merit list. Between 1967 and 1970, he worked as a Demonstrator in Biochemistry and Physiology and lectured in Pharmaceutical Chemistry at Nagpur University, under Professor A.K. Dorle. He had built a solid early academic record and found, in teaching, something that suited him genuinely rather than merely adequately.
In September 1972, he joined MGIMS as Lecturer in Biochemistry under Dr. B.C. Harinath. His predecessor Mr. M.G. Nathani had just left. The department at that point consisted of exactly two people: Dr. Harinath, freshly returned from postdoctoral training in the United States, and Taori. The first MBBS batch had been admitted that year, and Biochemistry was still folded into Physiology. Taori took charge of teaching all the Biochemistry classes — with chalk and blackboard, because that was what Sevagram had in 1972 — explaining the Krebs cycle, protein metabolism, vitamins, minerals, the intricate chemistry of the living body, to students who were encountering it for the first time.
He had not expected to discover, on arriving, that his salary at MGIMS was ₹495 per month — lower than the ₹725 he had earned at Nagpur University. He asked for fair pay. His requests were ignored. He stayed anyway, and kept teaching.
***
The division that developed between C.B. Taori and Dr. B.C. Harinath was not one of hostility so much as irreconcilable professional temperament. Harinath was a researcher — single-minded, driven by the immunology of filariasis, building his department's identity around laboratory discovery and publication. Taori was a teacher — his satisfaction came from the classroom, from making biochemistry accessible to first-year MBBS students, from running the clinical laboratory with meticulous precision and ensuring that the results it produced were reliable.
Neither calling was inferior to the other. But in a department where the head's priorities were research-centred, a man whose deepest satisfaction came from teaching occupied a structurally frustrating position. The intricacies of microfilarial immunology never captured Taori's imagination. The department's identity — which became increasingly synonymous with Harinath's research programme — left him peripheral to the work that defined it.
He tried to find a research path of his own. His interest lay in diabetes, not filariasis. He sought training, explored registration for a PhD through a former university professor. Dr. Sushila Nayar, who noticed his frustration and wanted to address it, contacted Dr. V. Ramalingaswamy at AIIMS in March 1975 to arrange a training programme in parasite immunology for him, then followed up two months later with the Director General of Health Sciences. Despite her efforts, Taori was denied access to the workshop.
The PhD never materialised. He could not register within MGIMS without working on filariasis. External routes fell through. Mr. Taori would never become Dr. Taori. He carried this with a specific kind of professional sadness — not bitterness exactly, but the settled awareness of a door that had closed and would not reopen.
In 1980, he completed a six-week endocrinology training programme at the National Institute of Nutrition, which sharpened his clinical biochemistry work and enabled him to mentor postgraduate students — guiding Chakrabarti through an MD on diabetes in 1994 and Pati through another in 1997. These were the research contributions available to him within his constraints, and he made them carefully.
***
What he built, and maintained for thirty-six years, was the clinical biochemistry laboratory at MGIMS — a service that generated blood chemistry results for the hospital's patients, on whose accuracy clinical decisions depended. He took ownership of it from his first year and never relinquished it. He standardised techniques, enforced quality controls, and ran it with an exactingness that had nothing to do with ambition or recognition. "Quality," he told his team, "is doing it right even when no one's watching."
This is the work that disappears from institutional memory most quickly — not because it was unimportant but because it produced no papers, no awards, and no visible monuments. Accurate laboratory results are experienced only in their absence: when they are wrong, when a treatment decision goes awry, when a patient is harmed. When they are right, they are invisible, absorbed into the ordinary functioning of a hospital as though they required no effort. Taori made them right, every day, for three and a half decades. The patients whose diagnoses were accurate because the biochemistry results were accurate will not know his name.
He also led the development of a paramedical course for eleventh and twelfth standard students at J.B. Science College, Wardha — a collaborative programme involving Biochemistry, Pathology, and Microbiology, funded by the Government of Maharashtra's Vocational Department. He understood that the laboratory sciences needed trained technicians as much as they needed professors, and he invested in the pipeline accordingly.
He retired as Reader in January 2005, having never reached the rank of Professor — the PhD requirement for promotion remained an obstacle he had never been able to clear. He remained in the classroom for three more years, teaching through November 2008 because the work itself still gave him something that retirement could not easily replace.
***
Nearly 2,300 medical students passed through his Biochemistry classes between 1972 and 2008. They learned the Krebs cycle and protein metabolism from a man with chalk on his hands and an MSc rather than a PhD, who had been denied the training he sought and had made peace, not entirely cheerfully, with the career he had rather than the one he had imagined. He taught them well regardless.
His son Gopal entered MGIMS with the class of 1990, earned his MD in Medicine from GMC Nagpur, specialised in critical care, and eventually settled in Australia. His daughter Anuradha followed in 1992, earning her DGO and MD in Obstetrics and Gynaecology. Both children had watched their father teach in the same institution for the entirety of their childhood, and both had chosen medicine.
After retirement, Mr. and Mrs. Taori divided their time between India and Australia, present for the grandchildren that their children were raising on the far side of the world. Their modest house in Dhanwantary Colony — built in the early 1990s, as MGIMS faculty of that generation typically did when they decided to stay permanently — was the home they had made. Gopal's gift was a different kind of home: the one that said, in the language of houses and car keys and a son's tears, that the sacrifice had been seen and the sacrifice had mattered.
They did not live in it. They drove toward Sevagram the next afternoon, full of joy, and the road took everything.
| 1945 | Born, 20 January, Pulgaon, Wardha district |
| 1960 | Matriculated, R.K. High School |
| 1965 | Completed BSc |
| 1968 | MSc Biochemistry, Nagpur University — second rank on merit list |
| 1967 | Demonstrator in Biochemistry and Physiology, Nagpur University |
| 1972 | Joined MGIMS as Lecturer in Biochemistry, 1 September |
| 1975 | Dr. Sushila Nayar attempts to arrange immunology training — denied |
| 1980 | Six-week endocrinology training, National Institute of Nutrition |
| 1994 | Guided Chakrabarti — MD thesis on diabetes |
| 1997 | Guided Pati — MD thesis on diabetes |
| 2005 | Retired as Reader, January |
| 2008 | Last day of teaching, November — thirty-six years after first class |
| 2009 | Died, 6 November, near Khadki village — with wife Veena |
Dr. M.V.R. Reddy
PhD (Nagpur University) [1987]

Professor & Head of Biochemistry · Thirty-Seven Years at Sevagram · The Gentlest Man Three Hundred Students Ever Met
The night before he died, he shared warmth and laughter with his family. By morning, he had slipped away — without struggle, without burdening anyone. He was fifty-nine years old, and he had not been ill. Death arrived quietly, as if it knew that any other manner of arriving would have been wrong for this particular man.
Three hundred students wrote tributes. Nearly every one of them used the same word: gentle.
***
Maryada Venkata Rama Reddy was born on July 1, 1957, in Karivemula, a village in Andhra Pradesh sixty-two kilometres west of Kurnool. His father Narsimha Reddy and mother Narsamma were the quiet strong foundation of a family in which he was the eldest of four children. He completed his schooling at IPH School in Kodumur in 1972, his intermediate studies at Osmania College, Kurnool, and his BSc and MSc from Sri Venkateswara University by 1980.
He arrived at MGIMS in November 1980 as a Junior Research Fellow, twenty-three years old, stepping into a world that was foreign in almost every dimension. Hindi and Marathi were unknown to him. English had entered his life only after childhood. He had never set foot in a medical school. The department around him was full of physicians and surgeons. He had an MSc in Biochemistry. The question that formed quietly inside him — did he belong here? — was one he did not answer by leaving. He answered it by staying, and working, and slowly becoming indispensable.
Dr. B.C. Harinath, a fellow Telugu-speaking academic from Tirupati, had brought him to MGIMS. The department at that time was a crucible of early research energy — Harinath at its centre, supported by Mr. C.B. Taori, J.N. Naidu, and doctoral scholars including Dr. A.K. Malhotra, I. Kharat, and G.B.K.S. Prasad. For Reddy, Prasad's presence offered particular comfort — a familiar face in an unfamiliar place. Together they navigated the biochemistry laboratory and the research culture Harinath was building around filariasis. The lab became his refuge. From Patel Hostel to Kabir Colony, and eventually to MLK Colony, he moved through different quarters, each a witness to his growing confidence.
In December 1980, just a month after joining, he married Lakshmi Reddy, who came from Nagarur in the Kurnool district. She was also an MSc graduate, would later earn a BEd, and would eventually become Principal of Kasturba Vidya Mandir — a professional life built entirely in Sevagram. She joined him in 1982. They spent the next thirty-five years in this village together, raising two sons who would both study medicine at MGIMS and marry classmates who would also study medicine at MGIMS. The institution ran through their family like a thread.
***
He had not imagined, arriving in Sevagram, that he would one day sit in a laboratory at Harvard. But in August 1983, he secured a place in a WHO training programme at Harvard University's Department of Tropical Public Health, working with Dr. W.F. Piessens on hybridoma techniques — a vital tool in biomedical research that was then at the frontier of immunological investigation.
Four months in Massachusetts. The contrast with Sevagram could not have been more complete — the scale of the institution, the resources available, the density of expertise in every corridor. He immersed himself, learned what he had come to learn, and took careful note of the standard against which his own work would need to be measured.
He returned to Sevagram in December 1983 noticeably different — more assured, more focused, carrying the specific confidence of someone who has seen the wider world of their discipline and found that they can hold their own in it. The question of whether he belonged had been answered, definitively, somewhere between Cambridge and the Wardha plains. He never asked it again.
He completed his PhD in immunodiagnostics — filariasis — from Nagpur University in 1987. He rose from Lecturer to Reader in 1989, Associate Professor in 1996, Additional Professor in 1999. When Dr. Harinath retired in 2000, Reddy took charge of the department — and of responsibilities that extended well beyond it, including oversight of the library and the central store, management of research grants, and the full range of administrative work that a department head in a rural medical college absorbs without the institutional support available in larger universities. He handled it with what everyone who worked with him described as quiet efficiency — never appearing burdened, never seeking recognition for the load he was carrying.
***
The question he was sometimes asked — how could he win major research grants from international agencies while working from a small village like Sevagram? — had a straightforward answer: he had chosen to work on filariasis, an area that was critically important for public health in rural India and almost entirely neglected by biochemistry researchers in medical schools. The combination of genuine need, minimal competition, and serious scientific work produced exactly the recognition that those conditions reliably produce.
His research expanded from filariasis diagnostics into applied immunology and molecular biology, autoimmune diseases, and potential vaccine candidates — developing diagnostic tools and identifying targets that earned recognition from agencies operating far beyond Wardha district. He published more than 150 papers in indexed journals and mentored over a dozen PhD and MD students. He received further research training at Johns Hopkins School of Medicine and the University of Illinois College of Medicine in Rockford, accumulating expertise across hybridoma techniques, IRMS, and molecular biology.
He served as General Secretary of the Association of Clinical Biochemists of India from 2003 to 2009 and as Executive Council member of the Asian Pacific Federation of Clinical Biochemists from 2004 to 2010. He represented ACBI at the International Federation of Clinical Chemistry, served as Managing Editor of the Indian Journal of Clinical Biochemistry, and chaired the board of studies at Maharashtra University of Health Sciences. In 2011, MUHS awarded him its Best Teacher Award — making him the third MGIMS faculty member to receive the honour. He deflected the recognition with characteristic ease, crediting mentors, colleagues, and chance. Those who knew him understood that this was not false modesty. He genuinely did not experience his achievements as primarily his own.
His annual two-week workshops on immunodiagnostics drew thirty participants from across India, providing intensive hands-on training in diagnostic techniques for infectious diseases. They became nationally recognised, attracting more applicants than they could accommodate. He also brought third-year MBBS students into the research process through the ICMR Short-Term Studentship Programme — teaching them to collect data, analyse results, and write manuscripts — because he believed that early exposure to research changed how doctors thought about evidence for the rest of their careers. Many of those students found themselves drawn deeper into academic medicine because of those months in his laboratory.
***
"Don't guess," he would say, eyebrows slightly raised, when a student reached for a shortcut. "Think. Then answer."
He had no patience for memorisation without understanding, but he expressed this impatience without creating fear. His classroom manner was of a piece with everything else about him: precise in expectation, warm in delivery, genuinely interested in whether the person in front of him understood. Science, to him, was not about rote learning but about inquiry — the courage to question, the discipline to test, and the humility to accept when one was wrong.
First-year MBBS students — often overwhelmed, sometimes in genuine danger of failing — found in him someone who noticed their difficulty and addressed it without making them feel ashamed of it. He had a particular attentiveness to students from disadvantaged backgrounds, those who carried extra uncertainty about whether they belonged. He had known that uncertainty himself, arriving in Sevagram in 1980, and he had never forgotten what it felt like. He believed perseverance mattered as much as knowledge, and he communicated this belief in the specific way that is most persuasive: by behaving consistently as if it were true.
Many who came to him at the edge of failing found their footing because of him. He opened doors that he held open with one hand while continuing his other work with the other, because that is how generous people do it — without making the door-opening the main event. Ashalata Srinivasan, from the MGIMS class of 1989, put it simply: "A teacher takes a hand, opens a mind, and touches a heart." He lived by this without ever having articulated it.
The word his colleagues used for him was Ajatshatru — one who has no enemies. He bore no grudges, held no envy, sought no power. There was a childlike quality to his affection — free from malice, free from calculation. In a department where the research culture could be competitive and the administrative pressures were substantial, this quality was rarer than it sounds.
***
A photograph taken months before his death — set against the Bali sea — shows him serene and composed, modest and unassuming, radiating the particular grace of someone at peace with how they have spent their time. He had been to Bali with his family. He had come home to Sevagram. The following night, he was with his family in warmth and laughter. By morning, he was gone.
Dr. Manu Kothari once wrote that those who cannot live well cannot die well — that a good death is the crowning glory of a good, happy life. When Dr. Reddy's time came, he was spared the torment of prolonged illness, the indignity of slow decline, the suffering of toxic treatment. He departed as he had lived: without fuss, without burden, with quiet dignity.
His wife Lakshmi, Principal of Kasturba Vidya Mandir, was the steady partner of thirty-six years. Their sons Srikanth — MGIMS 2001, MD in Psychiatry — and Sridhar — MGIMS 2008, MS in Orthopaedics — both married classmates from the same institution: Pooja, MD in Pharmacology, and Sakshi, MD in Radiology. Both couples were formed at the institution their father had given his working life to. After his death, the family relocated to Indore.
He was fifty-nine. It was not enough years. But the years he had were used with such care, and such consistent generosity, that three generations of students mourned him simultaneously. Dr. Anshu, Professor of Pathology, wrote: "You would not have known a gentler soul. You would not have encountered a more meticulous, silent, and hardworking person."
Three hundred students said something similar, each in their own words, unprompted.
| 1957 | Born, 1 July, Karivemula, Andhra Pradesh |
| 1980 | MSc, Sri Venkateswara University |
| 1980 | Arrived MGIMS as Junior Research Fellow, November |
| 1980 | Married Lakshmi Reddy, December |
| 1983 | WHO training programme, Harvard University — hybridoma techniques |
| 1987 | PhD in immunodiagnostics, Nagpur University |
| 1989 | Promoted Reader |
| 1996 | Promoted Associate Professor |
| 1999 | Promoted Additional Professor |
| 2000 | Took charge of department on Dr. Harinath’s retirement |
| 2003 | General Secretary, Association of Clinical Biochemists of India — until 2009 |
| 2011 | Maharashtra University of Health Sciences Best Teacher Award |
| 2017 | Died, 9 April, Sevagram — aged fifty-nine |
Development of immunoassays for diagnosis and monitoring of W.bancrofti infected cases
Immunodiagnostic and Immunoprophylactic evaluation of Brugia malayi filarial antigens
Evaluation of oxidative stress : antioxidant status immunological determinants in different clinical groups of lymphatic filariasis in an endemic area
Isolation, Purification and evaluation of mycobacterium tuberculosis excretory secretory antigens in Diagnosis of Extra-pulmonary tuberculosis
In vivo and in vitro maintenance of Brugia malayi filarial parasites and diagnostic evaluation of its purified antigens
Analysis of blood glucose, lipid profile and other biochemical parameters as risk factors for acute myocardial infarction in a rural population
Lymphatic filarial parasites: studies on morphological features, seroreactivity and enzymes character
Detection and follow up of children with occult filarial infection in an endemic area
Lymphatic filarial parasites: Studies on morphological figures, seroreactivity and enzymes character
Analysis of seroreactivity of filarial endemic population against antigens of different stages of filarial parasites
Production and evaluation of recombinant filarial antigens in Immunodiagnosis of filariasis
Protective Immunity in lymphatic filariasis : Role of B.malayi antigens as protective immunogens
Analysis of different immunological factors across the clinical spectrum of filariasis in an endemic area
Analysis of different immunological factors across the clinical spectrum of filariasis in endemic area
Comparative Evaluation of recombinant Sxp-1 antigen and B.malayi microfilarial antigens in detection and management of Bancroftian filariasis
Generation of Monospecific Polyclonal Antibodies to Recombinant Filarial Antigens Wb Gst and Wbl 2 and Comparative Evaluation of their Diagnostic Utility in Filariasis
Protective Immunity in Lymphatic filariasis : Identification and evaluation of vaccine candidates
Development and Evaluation of rapid formate tests for filariasis using rWbL1 and other recombinant filarial antigens and antibodies raised against them
Identification, characterization and evaluation of recombinant antigens as prophylactic tools in Lymphatic filariasis
A Study for detection of potential antimalarial therapeutics with possible proposition of oxidative rationale
Evaluation of Filarial Recombinant Enzyme Glutathione – S- Transferases (GST) and Ral Family Protein Wbl2 As A Combination Vaccine in Filariasis.
Evaluation of Recombinant Filarial Troponin and Paramyosin as Diagnostic Tools in Lymphatic Filariasis
Evaluation of Immunomodulatory Effect and therapeutic Role of Filarial Antigens on the Development of Type 1 Diabetes.
Assessment of Anti-inflammatory Activity and therapeutic Potential of Filarial Proteins in inflammatory Arthritis Using Rat Model.
Protective immunity in lymphatic filariasis: Identification, characterization and evaluation of recombinant filarial antigens
Anti-inflammatory potential of Cystatin and other novel Filarial derived Immunomodulators
Evaluation of the effect of filarial cystatin and other proteins in attenuating immune activation in experimental colitis
Exploration of a novel therapeutic approach targeting type 1 diabetes using the filarial derived WbL 2 and other immunomodulatory proteins
Study for exploration of effective formulation or lead molecule using herbal Extract and synthetic agents against Brugia malayi by in vitro as well as in vivo model and validation of therapeutic rationale
Study of Biochemical risk factors in Urolithiasis patients of an urban region in Central India
Dr. Ramvishal Agrawal
MD Pathology & Bacteriology (Government Medical College, Nagpur) [1963]
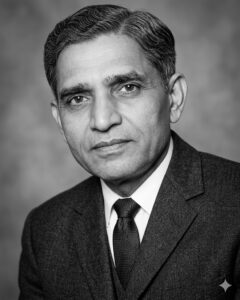
Professor & Head of Pathology · Founding Faculty · The Man Who Built a Department with Determination and Sweat
One Sunday morning, Dr. Satish Sharma received his weekly assignment: travel to GMC Nagpur, collect pathology specimens and slides from Mrs. Shobha Grover, and bring them back to Sevagram. The specimens came packed in two heavy cotton sacks, their seams straining under the weight of preserved tissues and glass slides. When no transport was available from Wardha East station, Sharma would sling the sacks over his shoulders and walk back through the dry dust.
This is how Dr. Ramvishal Agrawal built a pathology department. Specimen by specimen, Sunday by Sunday, carried on a postgraduate student's back from Nagpur because Sevagram's cupboards were bare and its shelves needed filling. He was building something in a place that had nothing to build with except determination and sweat — and he made determination and sweat sufficient.
Ramvishal Agrawal was born on March 15, 1934, in Raipur, and completed his schooling and premedical studies there before joining Government Medical College, Nagpur, in 1952. He earned his MBBS in 1957 and completed his MD in Pathology and Bacteriology in 1963, trained under Dr. J.B. Srivastava — who would later become India's Director General of Health Services — and worked alongside Dr. B.K. Aikat at PGIMER Chandigarh, Dr. K.D. Sharma at Haffkine Institute, and Dr. Shobha Grover in ICMR's cytopathology programme. He also led forensic medicine services, developing postmortem and autopsy protocols that sharpened a diagnostic precision he would later carry into a teaching role.
In December 1970, he arrived in Sevagram to establish the Department of Pathology at MGIMS. His wife Dr. Padma Agrawal joined as Reader in Anatomy the same day. They came from GMC Nagpur, deputed by the Government of Maharashtra, stepping into an institution that was barely a year old and still solving the most basic problems of existence — what rooms to use, what equipment to acquire, how to make a medical school function in a village with rural simplicity and no urban infrastructure.
He was, for the first period, the entire department.
The pathology museum he created was characteristic of his approach: meticulous, purposeful, and made from whatever was available. He collected mounted specimens, photographs, and illustrations framed between X-ray plates — using X-ray film as mounting material because that is what was to hand. He introduced side-room laboratories — small diagnostic units within hospital wards where house officers could perform essential tests: white cell counts, haemoglobin measurements, malaria detection, urine glucose analysis — bringing the diagnostic function closer to the patient and reducing the delay between clinical suspicion and laboratory confirmation. By the time he left MGIMS in 1976, ten such side-room laboratories were operational.
He pioneered mobile diagnostic services, taking pathology to outreach camps in Deoli and Pulgaon — rural patients receiving accurate diagnoses at locations accessible to them, integrating pathology with public health in exactly the way the Gandhian ethos of the institution demanded.
He developed histopathology services specifically calibrated to the diseases that defined rural India in that era: leprosy, tuberculosis, and filariasis. Working closely with Dr. K.V. Desikan on leprosy and Dr. A.R. Shukla on ophthalmology, he refined diagnostic techniques for leprosy ocular involvement — work that helped preserve the eyesight of leprosy patients who might otherwise have gone blind. Pathology, to him, was not confined to the laboratory. It was a clinical tool, and its purpose was the patient.
Faculty joined him gradually: Dr. G.S. Gehlot in 1973, then Dr. Narang, Dr. Lele, Dr. Nasiruddin Khan, and Dr. S.M. Sharma — several of them MBBS graduates who later obtained their MDs and returned to lead the department they had first entered as junior faculty. The succession he created was as much about the people he formed as the systems he established.
When the Pathology department relocated to the new college building in 1973, the move happened on a Sunday, organised entirely by Dr. Agrawal and the 1970 batch — microscopes, slides, specimen jars, microtomes, staining equipment, records, and furniture, packed and transported by students and their professor together. By evening, he had brought the entire batch to his home and fed them. It was the kind of day that a batch remembers fifty years later.
The MGIMS library in 1969 was a small room beside the Biochemistry and Pathology laboratories: a table, two chairs, an almirah, and thirty-five books. Dr. Agrawal looked at it and saw what it could become.
He persuaded Dr. Sushila Nayar to allocate larger space and funds. He brought books from his own collection. He reached out to colleagues and encouraged donations. Dr. I.D. Singh, the first principal, donated his personal collection. The shelves filled. At one point, half the books on display were donated. The small room became two large halls.
He called it his child. This was not rhetorical. When the monsoon rains came through open windows and books began to soak, he rushed home, returned with old clothes — including one of his own shirts — and mopped the floor himself until the last puddle had dried. A pathologist in old clothes, mopping a library floor in the rain, because the books mattered.
Dr. Santosh Gupta, from the 1970 batch, remembered what it was like to be Dr. Agrawal's postgraduate student approaching their qualifying examinations. Knowing that Sevagram's limited patient volume could not provide the exposure needed, Agrawal sent his students to BJ Medical College, Pune, for intensive immersion in haematology and histopathology months before the exams. Pune offered a flood of slides and specimens and seasoned pathologists. When they returned to Sevagram, Gupta said, they no longer hesitated. When an examiner placed a slide under the microscope, they diagnosed with confidence. "Dr. Agrawal hadn't just trained us," Gupta recalled. "He had prepared us for the real world."
This habit of mind — thinking not about what was convenient for the institution but about what his students needed — extended beyond Sevagram. When Dr. Agrawal moved to BJ Medical College in Pune as Dean after leaving MGIMS in 1976, he used his position to open the door for MGIMS students who needed postgraduate places that Sevagram, which did not yet offer postgraduate courses, could not provide. Students from the 1969 through 1972 batches found their way to Pune through his deliberate intervention: Rajendra Deodhar and Bhakti Dastane from 1969; Pramod Gupta, Rajiv Hivre, Anilkumar Jain, and others from 1970; Govind Bang, Surinder Bajwa, Dilip Gode, and others from 1971; Krishan Dutt Bharadwaj and others from 1972. He had left Sevagram. He had not left his students.
At BJ Medical College, he introduced what became known as his "ting-ting" seminars — named for the sound of the slide box — requiring postgraduate students to make real-time diagnoses from unknown slides. The department he led there conducted over a thousand clinical post-mortems. He subsequently served as Dean at GMC Aurangabad and VMGMC Solapur before returning to BJMC Pune, and spent a decade after retirement shaping the pathology department at Bharati Vidyapeeth, Pune, building another museum. He published fifty research papers and led national pathology conferences. His students called him Bhishmacharya — the elder teacher whose guidance shaped their careers and instilled in them a sense of purpose that outlasted the curriculum.
His wife Padma, Professor of Anatomy, died before him. Their daughter Naina, who had grown up watching her parents build a medical institution in a Gandhian village, died a year before her father after a courageous struggle with breast cancer. Dr. Agrawal died on March 25, 2022, aged eighty-eight. Their son Neeraj, an oncologist at Duke Raleigh, and daughter Nita, a radiologist, both practice in the United States.
He had built a pathology department in a place that had nothing. He had built a library from thirty-five books. He had sent his students, on his own initiative, to Nagpur and Pune to get what Sevagram could not yet give them. He had built a museum in his retirement. He was always building something — spaces, systems, futures, the careers of people who would carry forward what he had started in the dry dust of Sevagram in 1970.
"His dedication was infectious," Satish Sharma said. "In a place with few resources, he built a department with sheer willpower and sweat."
The sacks came from Nagpur every Sunday. The shelves filled. The library survived the monsoon.
| 1934 | Born, 15 March, Raipur |
| 1952 | Entered Government Medical College, Nagpur |
| 1957 | Completed MBBS |
| 1963 | Completed MD Pathology and Bacteriology, GMC Nagpur |
| 1970 | Arrived MGIMS, 14 December — established Department of Pathology |
| 1970 | Wife Dr. Padma Agrawal joined as Reader in Anatomy — same day |
| 1973 | Pathology department relocated to new college building — moved by students on a Sunday |
| 1976 | Left MGIMS, 1 August — joined BJ Medical College, Pune as Dean |
| 1976 | Continued opening doors for MGIMS students at BJ Medical College |
| 1976 | Subsequently Dean, GMC Aurangabad and VMGMC Solapur |
| 2012 | Built pathology department and museum at Bharati Vidyapeeth, Pune — in retirement |
| 2022 | Died, 25 March, aged eighty-eight |
Dr. K.V. Moghe
MD Pathology: Government Medical College, Nagpur (1963)
Professor & Head of Pathology · Five Years of Steady Service · The Sthitpragya of the Pathology Corridor
The word for him, those who worked alongside him agreed, was Sthitpragya — the Gita's term for one who possesses wisdom beyond knowledge, serenity beyond success. It was not a metaphor applied after the fact. It described, with unusual precision, how he actually was.
He moved through the Pathology corridors in his crisp white shirt and khadi trousers, unhurried, saying little. His hair had gone grey and he had not troubled to dye it — an indifference to vanity that seemed consistent with everything else about him. His thick spectacles framed eyes that observed more than they revealed. When he did speak, it was in Marathi, measured and calm, and it was sufficient. He had nothing to prove. He had ceased, long before arriving in Sevagram, to be surprised by life's arrangements.
K.V. Moghe was born in 1931, the same year as the third batch of Government Medical College, Nagpur — which he would later join in 1949, alongside Dr. M.L. Sharma, who would go on to become GMC's principal. He earned his MBBS in 1954 and his MD in Pathology in 1963, both from the institution where he had trained and where he would spend most of his career. He began as a Lecturer in Pathology in 1956, rising steadily to Reader and then Professor by April 1969.
There was, whispered about with a trace of irony by those who knew him, a brief posting to an Ayurvedic college — an episode he absorbed with the same equanimity he brought to everything else, filing it under life's occasionally absurd arrangements and moving on.
In 1976, the Government of Maharashtra sent five professors from Nagpur to Sevagram in one consignment, a deliberate effort to fortify the still-young MGIMS. Dr. Moghe was among them. He took charge of the Pathology department, inheriting it from Dr. G.S. Gehlot, who had held it briefly after Dr. Agrawal's departure. His salary was ₹2,344 per month — modest, unpretentious, entirely sufficient, much like himself.
The Pathology department of that era was a particular kind of place: the sharp smell of formalin, the quiet hum of microscopes, mounted specimens and hand-drawn charts crafted by Sitaram, the department's resident artist, who produced visual teaching aids with a devotion that made the walls a kind of illustrated textbook. Students pored over slides in rooms lit by laboratory lamps, deciphering the architecture of cells and tissues under the patient guidance of a department head who carried his knowledge without display.
Dr. Moghe's teaching was an extension of his personality — direct, uncluttered, practical. He had no patience for academic posturing. What mattered was whether students understood the essentials. As pathology's canonical texts evolved — Anderson, then Robbins coming into wider use — he remained focused on the fundamentals, distilling rather than embellishing, ensuring clarity rather than exhaustiveness. He taught mostly through practical sessions rather than large lectures, and mostly in Marathi, because that was the language in which the concepts would settle most securely in his students' minds.
He had a deep fondness for Clinical Pathological Conferences — the monthly sessions where a case was presented and the assembled clinicians and pathologists worked through it together like a medical detective story. He presided over these with quiet authority and a particular kind of intellectual pleasure: the enjoyment of a man who genuinely likes puzzles and has spent a career developing the tools to solve them. He led students through the maze of symptoms and findings without flamboyance, nudging rather than directing, leaving them with the satisfaction of having found the answer rather than been given it.
He supervised four MD theses: Santosh Gupta on G6PD deficiency, S.M. Sharma on blood groups and breast cancer, V.R. Bhongade on the epidemiology and pathology of laryngeal cancer, and N.S. Ingole on frozen section analysis. These were the research projects available in an era when formal methodology training was scarce even for supervisors, when research questions were broad rather than sharp, and when the MD thesis was more often a passport to graduation than a genuine contribution to knowledge. Dr. Moghe supervised conscientiously within those constraints, as did his contemporaries across the country. The limitations were systemic; the effort was real.
The department's reach extended well beyond the college walls. Pathology technicians and residents traveled to villages for social service camps, collecting blood samples in the night for filariasis and malaria screening — torches in hand, moving through fields and alleys, doing the work that rural public health required of people willing to do it.
The camp at Sirpur Kagaznagar — a town so far south that its people spoke Telugu — was particularly memorable. The response was large enough and the need evident enough that the hospital had to produce signage in Telugu, a quiet testament to how far MGIMS's reach had extended and how seriously the department took its public health function. No grand announcements followed. The work was done and the camp moved on.
Dr. Moghe presided over this department with the same steady efficiency he brought to his microscope work: not spectacular, but reliable in the way that matters most in medicine, where the consequences of unreliability fall on patients.
Two things gave him particular solace outside the laboratory. One was Marathi classical music, which filled his solitary hours and which he returned to with the consistency of someone who finds in a beloved art form a register of experience that work cannot provide. The other was the Bhagavad Gita — not as performance or ideology but as a philosophical companion, a text whose concept of the steadily wise person he seemed, without apparent effort, to embody.
He never lost his temper. He never sought recognition. He functioned without aggression and without the jostle for institutional position that marks less settled personalities. He was, as one assessment of him put it, a gentleman to the core — the rare kind of department head untouched by ambition. In a world where success often inflates the ego in proportion to its arrival, he had arrived at a settled place decades earlier and stayed there.
In February 1981, Dr. M.M. Arora joined the department, and a fortnight later Dr. Moghe relinquished his position and returned to GMC Nagpur, where he led the Pathology department until retirement in May 1985, handing the post to Dr. Shobha Grover. He had spent five years in Sevagram, arriving from Nagpur as a quietly authoritative figure and departing the same way, having given the department and its students exactly what he had to give — which was, in each case, more than it looked like at the time.
His tenure was one of basic haematology and histopathology, formalin and microscopes, monthly CPCs and midnight blood collection camps. It was not a period of dramatic institutional transformation. It was a period of steady, competent service in a department that served patients who had no other option. That is its own form of distinction.
| 1931 | Born, Nagpur |
| 1949 | Entered Government Medical College, Nagpur |
| 1954 | Completed MBBS |
| 1956 | Joined GMC Nagpur as Lecturer in Pathology |
| 1963 | Completed MD Pathology, GMC Nagpur |
| 1969 | Promoted Professor of Pathology, GMC Nagpur, April |
| 1976 | Arrived MGIMS, 16 June — one of five professors deputed from Nagpur |
| 1976 | Took charge of Pathology department from Dr. G.S. Gehlot |
| 1981 | Relinquished position, March — returned to GMC Nagpur |
| 1985 | Retired from GMC Nagpur, May — handed department to Dr. Shobha Grover |
HTML Code
Glucose-6-phosphate dehydrogenase deficiency in diseases
Histological study of breast tumors and its relation with blood groups isoantigens and sex chromatin
Study of carcinoma larynx with reference to histomorphological features and epidemiological factors
Frozen section examination in surgical Pathology materials with ancillary studies
Dr. G.S. Gehlot
MD Pathology (MGM Medical College, Indore) [1972]

Professor & Head of Pathology · Six and a Half Years at Sevagram · The Man Who Found a Discovery on a Bicycle and Taught Medicine Where It Lived
During a practical examination, Dr. Gehlot noticed a student from the 1976 batch who had come from flood-stricken Allahabad. "Where from?" he asked. "Allahabad," the student replied. Without further preamble, Dr. Gehlot proceeded to question him entirely on the epidemiology and microbiology of diarrhoeal disease — transforming a routine examination into a lesson directly relevant to what the student had just lived through.
This was his pedagogy in miniature: no patience for performance, no interest in jargon, complete insistence that medicine remain connected to the world it existed to serve. He had little regard for students who dazzled with terminology but lacked depth. What mattered was whether the knowledge could be applied — in a flood, in a village, in the specific situation in front of you.
Gopal Sharan Nainaji Gehlot was born on June 15, 1939, in Talwada, a village in Nalchha Tehsil in Dhar district, Madhya Pradesh. He completed his schooling there and moved thirty kilometres to Badwani for his intermediate education, finishing in 1956. Medicine drew him early. He entered Gandhi Medical College, Bhopal, in 1959 and earned his MBBS in July 1964.
Between his MBBS and the MD he would complete in 1972, he spent years in general practice — establishing a thriving clinic that gave him a clinical breadth unusual in a future pathologist, a grounding in the full spectrum of patient presentation that would later inform how he taught and examined.
His MD thesis at MGM Medical College, Indore, took him into the Adivasi heartland of Madhya Pradesh to study leucocyte variations among tribal communities. Research, for him, meant long journeys on foot and bicycle to villages where modern medicine rarely arrived — the same mode of fieldwork that had characterised the Gandhian leprosy workers in the region and that MGIMS would later build into its institutional DNA. From this work, he identified what would later be recognised as the Pelger-Huët anomaly — a morphological abnormality in neutrophil nuclei that carries diagnostic significance. It was a genuine discovery, made in the field rather than in a well-equipped laboratory, and it earned him lasting recognition in the discipline.
He spent seven and a half years as resident pathologist at MGM Medical College, building expertise across clinical and chemical pathology, bacteriology, serology, morbid anatomy, histopathology, and blood banking. Dr. J.N. Monga, the formidable Professor and Head of Pathology, validated his abilities — a stamp of approval that carried weight in academic circles.
By the early 1970s, MGIMS had a Reader in Pathology post that had sat vacant for over two and a half years. Dr. R.V. Agrawal, then Head of Pathology, spotted Gehlot's potential and personally recommended him to Dr. Sushila Nayar. The interview was a quiet affair. Dr. I.D. Singh, the Principal, found in Gehlot a man of few words and firm resolve, and offered him the position.
On June 14, 1973 — one day before his thirty-fourth birthday — Dr. Gehlot arrived in Sevagram. His salary was ₹1,042 per month. The department he joined was still in its early years, shaped by Dr. Agrawal's founding energy but still thin on staff and infrastructure. He worked with quiet diligence, building his expertise in the specific disease profile of rural Vidarbha — leprosy, tuberculosis, filariasis, the parasitic and infectious conditions that defined the pathology workload of a hospital serving an underserved population.
When Dr. Agrawal left in 1976, Gehlot took over as Head of Pathology on January 11, adding responsibility for Forensic Medicine — a discipline Dr. Agrawal had previously managed — to his existing portfolio. He was not the most conspicuous figure on the MGIMS campus. He did not seek limelight. He ran a department, taught students, supervised postgraduate work, and came back the next day and did it again.
At 8 MLK Colony, Dr. Gehlot lived alone for most of his Sevagram years. His wife Jaswant — whom he had married on May 25, 1963 — ran a nursing home in Indore, delivering babies and treating patients with her RMP qualification and diploma in Homeopathy. Their three children, two daughters and a son, stayed in Indore for school. For four years, Sevagram was his home in name; his family was elsewhere.
His kitchen was a kerosene stove and a few pots. Vidarbha summers were merciless — the heat clinging through the nights, the air barely moving. His son Sunil, who visited during summer holidays, remembered the only solution available: soak the mosquito nets in water, stretch them over the beds, and hope the night breeze dried them slowly enough to cool the air beneath. Such were the material conditions in which a senior pathologist and department head lived while building an institution that would eventually serve hundreds of thousands of patients.
The isolation accumulated. In July 1977, he submitted a resignation. He later withdrew it. In September 1979, he applied through UPSC for a post at Goa Medical College. This time the departure was final. On January 15, 1980, he was relieved of his duties. His Sevagram chapter had lasted six and a half years.
He returned to Indore and set up general practice in Tilak Nagar. The pathologist became, by incremental community demand, a trusted neighbourhood doctor — mornings spent in a bustling clinic diagnosing fevers, anaemias, and infections, two hours in the pathology laboratory, and the rest of the day available to the steady stream of villagers who had learned to trust him. For nearly two decades, until 2011, he worked in both modes simultaneously, the clinical and the diagnostic.
He subsequently taught at Aurobindo Medical College in Indore, then at a medical college in Ujjain, and finally at a dental college in Indore — teaching until his final years with the consistency of someone for whom the activity itself remained worthwhile independent of institutional affiliation or professional status.
His son Dr. Sunil Gehlot, who had entered MGIMS with the class of 1988 — fifteen years after his father arrived in Sevagram — runs a private surgical practice in Indore. The father had come to build a department; the son had come to be educated in it. Between the two arrivals, MGIMS had become something worth choosing rather than merely something that needed people willing to go.
Dr. Gehlot died on November 18, 2016, aged seventy-seven, of cardiac arrest after a long struggle with colon and prostate cancer. He had found the Pelger-Huët anomaly in an Adivasi village on a bicycle, built a pathology department in a Gandhian medical college on a kerosene stove, and spent the rest of his working life in the service of patients who came to him because they trusted him.
The flood student from Allahabad, questioned on diarrhoeal disease in a Sevagram examination hall, would have carried that lesson for a long time. The best teaching tends to find the student where the student actually is
| 1939 | Born, 15 June, Talwada, Nalchha Tehsil, Dhar district, Madhya Pradesh |
| 1959 | Entered Gandhi Medical College, Bhopal |
| 1963 | Married Jaswant, 25 May |
| 1964 | Completed MBBS, July |
| 1972 | Completed MD Pathology, MGM Medical College, Indore — identified Pelger-Huët anomaly in Adivasi communities |
| 1973 | Arrived MGIMS, 14 June — one day before his 34th birthday |
| 1976 | Took charge as Head of Pathology, 11 January — on Dr. Agrawal’s departure |
| 1977 | Submitted resignation, July — later withdrew it |
| 1979 | Applied for Goa Medical College post through UPSC |
| 1980 | Relieved of duties, 15 January — left Sevagram after six and a half years |
| 1980 | Returned to Indore — general practice and pathology laboratory, Tilak Nagar |
| 2003 | Taught at Aurobindo Medical College, then colleges in Ujjain and Indore |
| 2016 | Died, 18 November, Indore — aged seventy-seven |
Dr. K.V. Desikan
MD Pathology (Christian Medical College, Vellore) [1966]

Leprologist · Chairman, LEPRA India · The Man Who Examined Thirty Thousand People in Thirty-Five Villages and Took Notes at the Journal Club Until His Eighties
On Friday mornings, a slight elderly man would appear at the Department of Medicine's journal club. He was not on the faculty list for the session. He had not been invited as a discussant. He came because he wanted to learn, and because he saw no reason why a man of his age and standing should stop wanting to learn.
He was the only one who took notes.
When the presenting resident finished, questions would come from the floor — the usual ones, testing knowledge, probing gaps. Then Dr. K.V. Desikan would raise his hand. His questions were the kind that leave a presenter momentarily speechless: precise, unexpectedly deep, emerging from a lifetime of accumulated knowledge that the twenty-eight-year-old at the front of the room could not have anticipated. The mischievous smile that followed was legendary. He knew exactly what he was doing.
He was in his seventies and eighties during those Friday mornings. He had received the Damien-Dutton Award — the highest international recognition in leprosy work. He had over 150 publications. He had designed and implemented the world's first Survey, Education and Treatment programme for leprosy, a method the Government of India adopted nationally in 1955 and the WHO subsequently endorsed globally. He took notes at the journal club.
***
Krishnaswami Venkataraman Desikan was born in 1926 as the eleventh of twelve children in a poor family. He entered Mysore Medical College with the MBBS batch of 1944 and distinguished himself by reaching his third year without failing a single subject in any year — a genuine outlier by the standards of an era when medical school attrition was high. He qualified as a doctor in 1949, already shaped by Gandhian ideals that would govern every subsequent decision he made about where to work and why.
Before he reached his final year, he had been diagnosed with leprosy himself.
This is not a minor biographical detail. To be a medical student in the 1940s and contract the disease that most frightened and stigmatised patients — to experience from inside what the diagnosis meant, what it did to the person who received it, how doctors and society responded — was the crucible of his entire career. His treatment brought him into contact with Dr. Cochrane and Dr. Paul Brand at the Christian Medical College, Vellore. Their influence planted the interest. Dr. Ramanujam, a leprologist in Madras, nurtured it. Professor Jagadeeshan of the Hind Kusht Nivaran Sangh connected him to Dr. Sushila Nayar.
The connection to Sevagram had been made. It would take decades to complete.
***
In the early 1950s, Dr. Sushila Nayar was secretary of the Gandhi Smarak Nidhi Kushtha Nivaran Samiti at Wardha, working to integrate leprosy control into Gandhi's constructive work programme. She directed Desikan to undergo formal training at the Ackworth Leprosy Hospital in Wadala, Bombay, before joining her. By the time he completed the training, she had left Wardha to become Health Minister of Delhi State.
Dr. Wardekar, a pathologist who had taken over the Samiti, welcomed him instead. The organisation became the Gandhi Memorial Leprosy Foundation, and Desikan joined it in 1952. Wardekar had identified thirty-five villages around Sevagram for a leprosy control initiative. What followed was the work that would define Desikan's reputation and, through him, the management of leprosy across India and the world.
He visited all thirty-five villages — on foot, by bicycle, by bullock cart, on horseback, wading across rivulets. He went door to door, examining every man, woman, and child for signs of leprosy. Over five years, he and his team repeatedly examined more than 30,000 individuals and diagnosed 550 with leprosy. He established clinics in three villages and began treating patients with Dapsone. He generated awareness, conducted epidemiological surveys, and motivated patients to seek treatment — changing the relationship between the disease and the community from one of concealment and fear to one of engagement with healthcare.
This was the world's first Survey, Education and Treatment programme for leprosy diagnosis and management. The Government of India used it as the model for the National Leprosy Control Programme in 1955. The WHO endorsed and globalised it. The strategic logic — systematic survey, community education, accessible treatment — has shaped leprosy control worldwide for seventy years. It was designed and tested in thirty-five villages around Sevagram by a man in his mid-twenties who walked to reach them.
***
In 1957, he was transferred to the GMLF's Leprosy Control Unit at Chilakalapalli in Srikakulam district, Andhra Pradesh — a semi-tribal area where he was treating nearly 15,000 leprosy patients. He extended his services beyond the unit's mandated boundaries into tribal villages where no other doctor was present, providing emergency medical care for any condition that presented itself.
In 1962, at thirty-six, he enrolled at Christian Medical College, Vellore — the institution where he had been treated as a student — for a postgraduate degree in Pathology. His MD thesis involved autopsy studies on leprosy patients. He completed it in 1966. It was the beginning of the histopathological work for which he would become internationally recognised.
From Chingleput, where he served as Senior Research Officer at the Central Leprosy Teaching and Research Centre, he conducted a WHO fellowship year at institutions in the United Kingdom, the United States, and Japan — training in mouse footpad experiments and other advances in leprosy research. Back in India, he pioneered studies that used mouse footpad techniques to understand the pathogenesis of the disease.
In 1976, Union Health Minister Karan Singh asked him to take charge as Director of JALMA — the Japanese Leprosy Mission for Asia institute in Agra, recently taken over by ICMR. Within a year, JALMA had established itself as a centre of both outstanding clinical work and serious publication. National and international workshops, symposia, and conferences followed. His co-authorships with colleagues Ramu and Girdhar produced a sustained body of leprosy research across its entire clinical, histopathological, and immunological spectrum. He published over 150 papers in his career, covering descriptive epidemiology, diagnostics, histology, immunology, physiology, therapy, and clinical observation. His bibliography was the map of a discipline he had helped create.
***
He retired from JALMA in 1987 and came back to Sevagram — full circle, thirty-five years after Gandhi's constructive work programme had first drawn him to this village and its surrounding district. With support from LEPRA, the British Leprosy Relief Association, he established a leprosy histopathology laboratory at MGIMS and took charge as the first Chairman of LEPRA India, a position he held until 2003. From Secunderabad, LEPRA India conducted leprosy control activities in Andhra Pradesh and the tribal areas of Koraput, Orissa.
He continued research from a small office, writing notes on the backs of envelopes, because that was what was at hand and because the idea mattered more than the medium. He attended the Friday journal club in the Medicine department because he wanted to know what was current and because he saw no reason to stop learning. He asked questions that left residents speechless because he had been thinking about infectious disease for forty years and the depth of that thinking was not something that retirement could diminish.
In 2001, he received the Damien-Dutton Award — the highest international recognition in leprosy. The director of the Damien-Dutton Society spoke of his untiring efforts to bring treatment to the poorest of the poor, to restore self-worth to people whose disease had stripped it from them. His response was characteristically precise: "I feel honoured, but I have to remind myself that I am no greater than several others who have worked, struggled, sacrificed, and remained unknown."
He meant it. Authorship questions can damage the best professional relationships; Desikan never agreed to put his name to a paper he had not worked on, and never gifted authorship. He gave his juniors the first-author position routinely. He co-authored exactly one paper with his daughter, Dr. Prabha Desikan — a microbiologist, later at MGIMS — who had grown up watching her father walk to villages and examine tens of thousands of people for a disease that others feared to approach. The single shared paper between them is its own kind of testament.
***
He lived to ninety-six. In his final years, the maladies of old age kept indoors a man whose nature was to be in motion — in villages, in laboratories, in conference halls, in the journal clubs of departments where he was not on the roster. The body stilled. The mind, by all accounts, did not.
His daughter Dr. Prabha Desikan compiled his biography — K.V. Desikan: An Extraordinary Life — launched at the International Leprosy Congress in Hyderabad in early November 2022, days after his death on October 23. The congress was a gathering of the international leprosy research community. His biography was launched among the people who understood best what his work had meant.
He had been diagnosed with the disease as a medical student and spent sixty years trying to understand it, treat it, and remove the fear and stigma that made it worse than its pathology required. He examined 30,000 people in thirty-five villages near Sevagram in the early 1950s. He returned to Sevagram in 1987. He attended the Friday journal club and took notes.
"I have to remind myself that I am no greater than several others who have worked, struggled, sacrificed, and remained unknown."
He said this. He did not believe it was false modesty. He believed it was true. It was also, by the evidence of everything else, not entirely accurate.
| 1926 | Born, eleventh of twelve children, Mysore |
| 1944 | Entered Mysore Medical College — MBBS batch |
| 1944 | Diagnosed with leprosy as a medical student — treated at CMC Vellore |
| 1949 | Qualified MBBS |
| 1952 | Joined Gandhi Memorial Leprosy Foundation, Wardha |
| 1952 | Began door-to-door survey of thirty-five villages around Sevagram |
| 1955 | Government of India adopted his SET programme as national model |
| 1957 | Transferred to Leprosy Control Unit, Chilakalapalli, Andhra Pradesh |
| 1962 | Enrolled for MD Pathology, CMC Vellore |
| 1966 | Completed MD — began histopathological leprosy research |
| 1976 | Appointed Director, JALMA Institute, Agra — under ICMR |
| 1987 | Retired from JALMA — returned to Sevagram |
| 1987 | Established leprosy histopathology laboratory, MGIMS |
| 1987 | Appointed first Chairman, LEPRA India |
| 2001 | Received Damien-Dutton Award — highest international honour in leprosy |
| 2003 | Stepped down as Chairman, LEPRA India |
| 2022 | Died, 23 October — biography launched at International Leprosy Congress, Hyderabad |
Dr. Narendra Samal
MD Pathology (MGIMS, Sevagram) [1981]

Professor & Head of Pathology · Twenty Years at Sevagram · The Rarest Kind of Life
Three months after Dr. Narendra Samal died, on February 26, 2024, Swarnlata died too — at home, as if she could not bear to leave him alone on his final journey.
They had spent fifty years proving, in the specific language of action rather than declaration, that love was a practice and not a sentiment. He had waited years to pursue his own postgraduate degree so that she could complete hers first. He had resigned as Professor and Head of Pathology — a position of genuine standing, built over two decades — so that she could accept a department headship at a new institution. He had converted from Islam to Hinduism and changed his name, officially documented in the Maharashtra Gazette in February 1985, so that there would be no ambiguity about where he stood. When she suffered a severe brain injury in a scooter accident in the early 1990s, he became her doctor, her nurse, and her steady presence until her recovery. When a stroke left him profoundly disabled in his final years, she became his caregiver, tending to him without complaint until his death. Then she followed him, three months later.
Some bonds are too strong to be broken even by time. Theirs was one of them.
Naziruddin Khan was born on April 2, 1947, in Charinangala, a village in Badchana tehsil of Odisha, just months before Indian independence. He was orphaned early. Poverty was a constant companion through his childhood and education — through Bhadrak College, through Utkal University, through Sriram Chandra Bhanj Medical College in Cuttack, where he completed his MBBS in 1970. Each institution he passed through was a step taken with the single-mindedness of someone who understood that education was the only available path.
What brought him to MGIMS was a Gandhian freedom-struggle veteran named Bihari Lal, who had a keen eye for potential and wrote a letter to Dr. Sushila Nayar recommending the young Dr. Khan. When he arrived at MGIMS in the summer of 1972, the only available position was house officer in Medicine. He took it without hesitation.
In August 1972, he transitioned to Pathology as a Lecturer — the department where he would spend the next two decades building both his career and the field itself. The following year he married Swarnlata Samal, an Odia woman from a Hindu family, and together they committed to a life in Sevagram — one thousand kilometres from Odisha, in a place whose language, culture, and rhythms were entirely unfamiliar. They were both without postgraduate degrees when they arrived. Neither had the resources to enrol in a three-year programme away from MGIMS. They would have to be patient, and they were patient — but he was patient for her first.
Students from the 1975 to 1992 batches called him Khan Chacha. They said this with a particular warmth that coexisted, uneasily to outsiders but naturally to those who had been taught by him, with the memory of flying chalk and flying dusters.
"He used to strike terror in the hearts of students," recalled Monika Ahuja of the 1982 batch. Abhay Kelkar from 1987 put it differently: "Despite the occasional turbulence, we were blessed to have been taught, scolded, and rebuked by this teacher in his inimitable style."
His intensity was not cruelty. It was the particular severity of a man who believed pathology was serious, that medical students were capable of mastering it seriously, and that anything less than full engagement was a failure of respect — toward the subject, toward the patients who needed doctors to understand it, and toward the students themselves. He was easily recognisable in the corridors: white khadi trousers, an off-white silk shirt, paan almost always in his mouth, a distinct Odia accent that gave his presence a quality unlike anyone else on campus. He supervised seventeen postgraduate students through their MD theses, including V.C. Gupta, Aruna Mutha, Kiran Swarup, Milind Jagtap, Nitin Gangane, Girish Muzumdar, and Renuka Kulkarni. Dr. Nitin Gangane went on to become Dean of MGIMS and later Vice-Chancellor of KLE Academy of Higher Education and Research, Belagavi.
Beyond teaching, he took on the editorship of the MGIMS Annual Reports in the mid-1980s, working with Dr. S. John Premendran, Mr. Shankar Bhat, Dr. Pradeep Joel, and Mr. C.D. Gokulachandran. In September 1988, Dr. Sushila Nayar appointed him Warden of the Boys' Hostel alongside Dr. A.P. Jain — tasked with improving discipline and conditions in a hostel that had become difficult to manage. He approached it with the same rigour he brought to the classroom. Dr. Nayar wrote him a personal letter of commendation, acknowledging his conscientiousness and the trust he had justified through his service.
The conversion and the name change — from Naziruddin Khan to Narendra Samal — happened in February 1985 and were officially recorded in the Maharashtra Gazette. He had already been Swarnlata's husband for twelve years. The conversion was not a precondition she had set. It was a statement he chose to make, about belonging, about commitment, about the kind of man he intended to be.
Their home in Sevagram became a tradition for students during Saraswati Puja — the Muslim-turned-Hindu professor and his Hindu wife welcoming students with sweets and warmth, across whatever religious boundaries the calendar recognised. Dr. V.K. Gupta, a pathologist from the 1976 batch who remembered both of them well, spoke of the love they shared as something that transcended the narrow categories the world tried to impose on it.
In May 1992, he resigned as Professor and Head of Pathology at MGIMS.
The reason was straightforward: Swarnlata had been offered the position of Head of the Department at the newly established JN Medical College in Sawangi, Wardha. She had been a Lecturer at MGIMS since 1976, had risen through Reader and Associate Professor, and had reached Professor in 1990. But the path to department head at MGIMS was blocked by the existing structure. Dr. Nayar, who valued them both, had created an additional professorship specifically to ensure Swarnlata's promotion could proceed. It was not enough.
He resigned from the position he had built over twenty years. He walked away from it so that she could walk toward something she deserved.
Dr. Nayar wrote him a personal note expressing her disappointment — not anger, but the sadness of someone who had invested in a person and wished the conversation had happened earlier. She respected his decision. She wished him well.
At Sawangi, he developed clinical laboratories and continued teaching pathology. In November 2017, he suffered a severe stroke that required intensive care and mechanical ventilation for three weeks. He survived but was left profoundly disabled — dependent, confined, the active and forceful figure of the classroom reduced to the stillness of a man who could no longer do for himself. For six years, Swarnlata cared for him at home, without complaint, with the matter-of-fact devotion that had characterised everything she had done in their life together.
He died on December 3, 2023. She died on February 26, 2024.
Their elder son Nitin is an MGIMS alumnus from the class of 1995 who completed his MS in Orthopaedics at his father's institution. Their younger son is a physiotherapist. The boys grew up in the house where Saraswati Puja was celebrated and paan was always present and students came for sweets, where their father wore white khadi and spoke with an Odia accent and threw chalk when he needed to and loved their mother in a manner that left no room for ambiguity.
The seventeen pathologists he trained are practising across the country. The institution he helped build across two decades in Sevagram, and the one he helped launch in Wardha, carry the imprint of a man who understood that rigour and love were not opposites — that both demanded the same quality of commitment, the same refusal to do things halfway.
He gave everything to his work and everything to his wife, and somehow both were given fully, not divided. This is the rarest kind of life.
| 1947 | Born, 2 April, Charinangala, Badchana tehsil, Odisha |
| 1970 | Completed MBBS, Sriram Chandra Bhanj Medical College, Cuttack |
| 1972 | Arrived MGIMS — house officer in Medicine, then Lecturer in Pathology, August |
| 1973 | Married Swarnlata Samal |
| 1976 | Swarnlata joined MGIMS as Lecturer in Pathology |
| 1985 | Converted to Hinduism, changed name to Narendra Samal — recorded in Maharashtra Gazette, February |
| 1988 | Appointed Warden, Boys’ Hostel — alongside Dr. A.P. Jain, September |
| 1990 | Swarnlata promoted to Professor of Pathology |
| 1992 | Resigned as Professor & Head of Pathology, May — so Swarnlata could accept department headship at JN Medical College, Sawangi |
| 2017 | Suffered severe stroke, November — left profoundly disabled |
| 2023 | Died, 3 December |
| 2024 | Swarnlata died, 26 February — three months after him |
Comparative histopathological study of the skin, oral mucosa and lymph node in leprosy
Clinico-pathological study of endometrium in dysfunctional uterine bleeding
Study of Hepatitis B surface antigen ( HBsAg) and alpha fetoprotein (AFP) in various liver diseases
Fibrinogen levels in sickle cell disease
Study of Hepatitis B surface antigen (HBsAg) immunostatus in cases of leprosy
Study of Hepatitis B surface antigen immunostatus in case of lymphoproliferative disorders
Study of malignant soft tissue tumors with special reference to histomorphology at Mahatma Gandhi Institute of Medical sciences: A review of 10 years
Detection of Hepatitis B surface antigen (HBsAg) and antibody (anti-HBs) from filter paper blood samples
A correlative study of filarial antigen and antibody in blood and hydrocele fluid of hydrocele cases with histomorphology of tunica vaginalis
Epidemiological study of dysplasia of uterine cervix in married women around Sevagram: retrospective analysis
Alloxan-induced diabetes mellitus in albino rats with special reference to histomorphology of pancreas
Histological study of early skin lesions in leprosy
The prevalence of human immunodeficiency virus infection among blood donors and patients with leprosy and tuberculosis in rural population around Sevagram
Cytological study of leukoplakic lesions in oral cavity
Cytomorphological study of palpable thyroid diseases by fine needle aspiration cytology
Immunodiagnosis of tuberculosis
Dr. Satish Sharma
MD Pathology (MGIMS, Sevagram) [1980]

Professor & Head of Pathology · Forty-One Years at Sevagram · The Legacy That Is Quiet, Unresolved, and Real
His father, Dr. M.L. Sharma, was one of the most commanding figures in MGIMS history — charismatic, dynamic, deeply admired, the kind of person around whom institutional memory organises itself. Satish Sharma arrived in Sevagram on July 18, 1974, his father's forty-fifth birthday, and spent the next four decades working in the same institution, in the department just down the corridor.
He was not his father. He knew it. He did not try to be.
He was a reserved man, almost a loner — soft-spoken, rarely socialising, often seen pacing the corridors in the particular manner of someone whose thinking is done in motion. He was approachable, kind, a good listener. He was not a leader in the way the word usually implies: someone who asserts, directs, and commands. Administration was not his calling. Conflict avoidance was his default. The department, at times, ran itself. Yet he taught pathology at MGIMS for nearly forty years, guided twenty-one postgraduate theses, and understood what a blood smear could tell you better than most people in the country.
His legacy at MGIMS is quiet and unresolved, as his own institution's assessment of him acknowledged. It is also real.
Satish Sharma was born on December 5, 1949, in Barwaha, a town on the Narmada River in West Nimar district of Madhya Pradesh, named for the twelve ghats that once lined its banks. His father was twenty years older than him — still a medical student at Government Medical College, Nagpur, when Satish was born. The family lived in a medical colony opposite Ajni railway station, surrounded by doctors and medical teachers. Medicine was not a career Satish chose so much as a world he had always inhabited.
He attended St. Antony's High School in Ajni, then Patwardhan High School in Sitabuldi, then Mohota Science College. He entered Indira Gandhi Medical College, Nagpur, in the second batch — admitted with 59.8% in his BSc Part I, at a time when 60% was the standard threshold. The margin was thin. In his second MBBS, he found his subject. Pathology — its precision, its detective logic, the way a microscope revealed what the naked eye could not — was what he wanted to spend his life doing.
His father had moved to Sevagram in December 1970, deputed by the Government of Maharashtra to help build MGIMS. On July 18, 1974 — his father's birthday — Satish arrived to join him. The Pathology department was then under Dr. R.V. Agrawal, who had known the Sharma family since their Nagpur colony days. Agrawal recognised Satish's interest and took him on. Alongside Dr. Santosh Gupta from the 1971 batch, he threw himself into histopathology in a department that had few patients, fewer specimens, and faculty who sketched microscopic findings on blackboards because teaching slides were scarce.
His MD thesis under Dr. K.V. Moghe examined breast tumours — their histology, blood group isoantigens, and sex chromatin — precise work requiring patience and careful eyes. Patient load in Sevagram was low in those years, and Dr. Agrawal solved the exposure problem the same way he had solved it for others: he sent Satish and Santosh to B.J. Medical College, Pune, for intensive immersion in slides and specimens before the final examination.
He described the pathology of his training years with the clarity of someone who had thought carefully about what that era demanded: no auto-analysers, haematology relying entirely on morphology, haemoglobin estimated by Sahli's method, cells counted manually with a haemocytometer. Histopathology was labour-intensive — tissues processed by hand, microtomy manual, staining basic haematoxylin and eosin. Frozen sections were rare. Immunohistochemistry was unheard of. Complex cases were sent to Nagpur or Bombay. But both Dr. Agrawal and Dr. Moghe had taught him that a well-trained pathologist could do more with a microscope than any machine.
He took that lesson permanently. Through the decades when electronic cell counters became standard and automation reshaped laboratory medicine, he continued to trust the blood smear. RBC morphology fascinated him throughout his career — the way each red cell's shape and size and colour told a story about what was happening inside a patient's body. He could classify anaemia from a smear with the confidence of someone who had been doing it for thirty years, because he had been.
He became Reader in 1982 and led the department from 1995 to 2004, later continuing as Professor. A technicality in the promotion structure kept him from reaching Director-Professor — a small irony that those who knew him noted without drama.
Between 1987 and 2009, he supervised twenty-one postgraduate theses covering fine needle aspiration cytology, sickle cell anaemia, leukemia, breast cancer, Helicobacter pylori in gastric lesions, placental histology in adverse pregnancy outcomes, mast cell distribution in leprosy, and frozen section diagnostics. It was a substantial body of mentorship across a broad range of the discipline.
His students remembered him pacing the classroom with chalk, sketching histological details with effortless ease, filling lectures with real-world examples rather than abstract descriptions. He made pathology concrete. He revealed the essence of disease rather than merely cataloguing its appearances.
What he could not do — or would not — was the administrative work of leadership. He avoided enforcing decisions, let things run their course, and withdrew from the institutional confrontations that department heads inevitably face. His junior colleagues absorbed the guidance role in thesis supervision when he stepped back from it. The department, at times, continued without his direction because he did not provide direction. These are the facts, and they sit alongside the other facts without cancelling them.
His father's shadow was long. Dr. M.L. Sharma had commanded and people had followed. Satish Sharma had the intellect, the experience, the years — and a temperament that made the commanding mode unavailable to him. He lived in the institution, and in the shadow, and left his mark on both in a register quieter than his father's but not less real.
He retired as Professor and Head at the end of 2015, then remained at MGIMS on annual extensions for another six years before moving to Bhopal. He taught at Mahavir Institute of Medical Sciences and later at Shankaracharya Medical College, Bhilai — stepping away finally on October 1, 2023, after forty-nine years in medical education. He was seventy-three.
For nearly a decade, he had managed the Nagpur PMT Centre alongside his departmental responsibilities, ensuring examination logistics ran cleanly. He had captained his school football team for three consecutive years and retained a genuine love for sports — when Dr. O.P. Gupta needed someone to lead the institute's sports department in the mid-1990s, the choice was immediate.
His sons Pawan and Vijay are both MGIMS alumni — Community Medicine and Anaesthesiology, one settled in Dubai, the other in Hyderabad. He now lives in Dhanvantary Colony, a mile and a half from the medical college where he arrived on his father's birthday in 1974.
Dr. R.V. Agrawal's instruction to his students was to focus on a cell and try to understand what it does in health and disease. Satish Sharma heard this and carried it. Over forty years, he pressed his eye to the microscope and did exactly that — reading cells, finding stories, trusting the preparation of the eye more than the output of the machine. Whatever his limitations as an administrator, as a pathologist he was serious and skilled, and in the end a serious and skilled pathologist who teaches for four decades shapes a great many doctors who will carry what they learned into wards and clinics and operating rooms for the rest of their working lives.
That is its own form of legacy. Quiet, unresolved, and real.
| 1949 | Born, 5 December, Barwaha, West Nimar district, Madhya Pradesh |
| 1968 | Entered Indira Gandhi Medical College, Nagpur — second batch |
| 1974 | Arrived MGIMS, 18 July — his father Dr. M.L. Sharma’s 45th birthday |
| 1977 | Joined Pathology department formally, 1 August |
| 1982 | Promoted Reader in Pathology |
| 1987 | Began supervising MD theses — continued until 2009 |
| 1995 | Led department as Head of Pathology |
| 2004 | Stepped down as Head — continued as Professor |
| 2015 | Retired as Professor & Head, 31 December |
| 2021 | Left MGIMS after annual extensions — moved to Bhopal |
| 2021 | Taught at Mahavir Institute of Medical Sciences, then Shankaracharya Medical College, Bhilai |
| 2023 | Stepped away from teaching, 1 October — aged seventy-three, after forty-nine years |
Study of Hepatitis B Surface antigen and immunological profile in blood donors
An evaluation of accuracy of fine needle aspiration cytology in the diagnosis of lymphadenopathy with histomorphological correlation
Cytological study of effect of chewing tobacco and betel nut on the character of epithelial cells of oral cavity
Study of sputum cytology in male chronic smokers
Clinicopathological retrospective and prospective study of leukemia in a rural community
Frozen section examination in surgical Pathology material: A study of 205 cases
Comparative study of different reporting systems used for reporting cervical / vaginal cytological diagnosis
Evaluation of high resolution USG in diagnosis and management of scrotal disorders
Clinico-epidemiological and histomorphological study of breast tumors in a rural community: a retrospective and prospective study
Hematological profile in patients of sickle cell anemia and sickle cell trait in relation to blood gas analysis
Study of non-neoplastic gastric lesions with special reference to Helicobacter pylori infection
Correlative study of cytological features with histological grading and axillary lymph node status in breast carcinoma
A correlative study of Haemoglobin S percentage and haematological parameters in patients of sickle cell trait
Correlative study of cytological, biochemical and microbiological parameters in benign body cavity effusions
Microwave processed cell block preparation as a diagnostic technique complementary to cervico-vaginal specimens
Placental histology and its correlation with adverse pregnancy outcome and use in estimation of time since fetal death in cases of stillbirth
Erythrocyte sedimentation rate in health and disease
Significance of mast cell density and distribution in various histopathological lesions of leprosy
Role of fine needle aspiration cytology in bone lesions
Study of clinico-pathologic characteristics of infiltrating duct carcinoma of breast with micropapillary carcinoma component
A 9-Year Study of Cytological Profile of Breast Carcinoma with Micropapillary Component
An Audit of Blood Bank Services.
Dr. Santosh Gupta
MD Pathology (MGIMS, Sevagram) [1980]

Reader, Pathology · Nine Years at Sevagram · The Man Who Knew Viswanath's Debut Scores
The interview panel included Dr. Sushila Nayar and, to Santosh Gupta's surprise, Pratibha Patil — then Maharashtra's state public health minister, later India's first woman President.
Patil leaned forward. "Are you interested in sports?"
"Yes, Madam. Cricket."
"Do you know how many runs Gundappa Viswanath scored on his debut?"
Without hesitation: "0 and 137. The Kanpur Test against Australia last year."
A newspaper was fetched. The score was verified. Pratibha Patil smiled. "You may go."
He had secured his place at MGIMS.
Santosh Gupta was born on December 5, 1950, in Gondia, the eldest of six siblings in a joint family of modest means. His father Gokul Prasad taught at a middle school; his mother Shyama Devi ran the household. Her atrial fibrillation shaped his childhood more than anything else — her heart racing unpredictably, confining her to the house, requiring Santosh to balance school, household chores, and her care simultaneously. His grandmother had bronchial asthma. Medicine was not an abstract ambition for him. It was a response to specific suffering he had watched from close range and felt powerless to address.
In 1968, he missed admission to Indira Gandhi Government Medical College, Nagpur, by three marks. He completed a BSc at Dhote Bandhu Science College, Gondia, and waited. In 1970, when BHU conducted the PMT for MGIMS, he appeared. The interview with Dr. Nayar and Pratibha Patil followed. He knew Viswanath's debut scores. He was in.
MGIMS in 1970 was bare and unfinished — buildings scattered across dry land, no orientation camp, no Gandhi Ashram stay, the old hospital housing wards, OPDs, lecture halls, seminar rooms, dissection hall, and operating theatres all together. He was not there for comfort. He was there for a purpose he had clarified beside his mother's bed years earlier.
During his final MBBS viva in November 1975, he was questioned for thirty minutes on a paraparesis patient from Chhattisgarh — neuroanatomy, neuropathology, clinical neurology. He had long abandoned Davidson's Medicine for Cecil's and Rustom Jal Vakil's Clinical Medicine. He held his ground. He loved Medicine and expected to practise it.
Sevagram had no postgraduate programmes in 1975. Further education meant Pune or Bombay, and most courses were unpaid. Santosh's father was in debt. His family depended on him. Earning while studying was not a preference — it was a constraint.
Pathology offered something Medicine did not: a salaried lecturer's post for MBBS graduates, without the usual progression through house officer and registrar roles. His heart was in Medicine. His situation was in Pathology. Survival came first.
He joined MGIMS as Lecturer in Pathology on January 14, 1977, under Dr. K.V. Moghe, on a basic pay of ₹325 plus allowances. Six months later, Dr. Narayan Ingole — a batch junior — became the second MGIMS alumnus to join as faculty. When the MD Pathology programme began in 1978, Santosh and Dr. Satish Sharma were its first two candidates.
His thesis on G6PD deficiency was not proceeding well. A faculty member from Jhansi named Dr. Saxena offered him advice he would remember for the rest of his life: don't take the thesis too seriously — it is a passport for the exam, not a masterpiece. Hundreds have researched the same topic. Get it done. A completed thesis, even if imperfect, is always better than an unfinished one.
He refocused. He completed it. He earned his MD in Pathology in April 1980 — a decade after arriving at MGIMS as a first-year student.
He was appointed Reader in Blood Bank and Haematology in February 1984. The nine years between his arrival in 1977 and his departure in 1986 were not what he had expected academic life to be. Research papers were published without his name. Permission to attend conferences he had contributed to was denied. For the entirety of his time at MGIMS, he was never permitted to guide postgraduate students — while Dr. Moghe mentored four, Dr. Arora one, and Dr. Samal seventeen. Between 1976 and 1986, the department produced thirty-five papers, mostly case reports, typically listing only the department head as author.
He managed to publish three papers of his own: on glycogen's role in endometrial infertility, on alpha-1-antitrypsin and hepatitis B in chronic liver disease, and on blood groups, sickle cell haemoglobin, and G6PD deficiency in the Mahar community of rural Maharashtra. The sickle cell work had genuine promise. Administrative obstacles prevented it from progressing.
He was not a difficult personality. He maintained close relationships with the department's technicians — Gyaneshwar Thackeray, Bhoyar, Mahajan, B.M. Patil, and Babu Dhole — the people who made the laboratory actually function, whose contributions rarely appeared in any record. He understood that departments ran on more than faculty.
But the experience of watching his work appropriated, his mentorship opportunities blocked, and his research impeded accumulated into a growing certainty that Sevagram was not the place where he was going to build the career he had imagined. On April 1, 1986, he resigned. Six weeks later — on May 10, his wedding anniversary — he opened a private practice in Wardha.
For two decades, the practice ran. It was good work, reliable work, necessary work. It was also, eventually, monotonous. The pull of teaching proved stronger than he had anticipated.
In 2006, he closed the practice and returned to academia, teaching across four institutions over fourteen years: Jawaharlal Nehru Medical College, Wardha; People's Medical College, Bhopal; LN Medical College, Bhopal; KD Medical College, Mathura. He retired at seventy, returned to Wardha, and quietly reopened his practice. The loop that had begun in Gondia, passed through Sevagram, detoured through Wardha and Bhopal and Mathura, had brought him back to the same town — carrying the accumulated experience of five institutions and four decades.
He had married Uma Devi from Jhansi. Their son Sandeep is an oral and maxillofacial surgeon; their daughter Neeta moved from fashion designing to homemaking.
At seventy-five, he looks back without bitterness — which is itself a kind of achievement, given what the MGIMS years contained. The institution had not given him everything it might have. He had found other ways forward. He had taught, practiced, moved, returned, and kept going.
The interview with Pratibha Patil was in 1970. Gundappa Viswanath's debut scores were 0 and 137. He knew them without hesitation. He has always known things carefully, precisely, and in full — including, in the end, how to make peace with a career that did not unfold as planned and was worth having anyway.
| 1950 | Born, 5 December, Gondia, Maharashtra |
| 1970 | Entered MGIMS — interview with Dr. Sushila Nayar and Pratibha Patil |
| 1975 | Completed MBBS, November |
| 1977 | Joined MGIMS as Lecturer in Pathology, 14 January |
| 1978 | Enrolled in MD Pathology — one of first two candidates in the programme |
| 1980 | Completed MD Pathology, April |
| 1984 | Appointed Reader in Blood Bank and Haematology, February |
| 1986 | Resigned, 1 April |
| 1986 | Opened private practice in Wardha, 10 May — his wedding anniversary |
| 2006 | Closed practice — returned to academic medicine |
| 2006 | Taught at JNMC Wardha · People’s Medical College Bhopal · LN Medical College Bhopal · KD Medical College Mathura |
| 2020 | Retired at seventy — returned to Wardha, reopened practice |
Dr. Narayan Ingole
MD Pathology (MGIMS, Sevagram) [1981]

In June 2016, visiting his sister in Nagpur, he sat on a swing. It broke. He fell, injuring his neck. Paralysis followed — arms and legs refusing to obey. Four years of physiotherapy. His wife Jyotsna's care, constant and patient. Gradual, partial return.
He never asked why.
"Life unfolds as predestined," he would say. Lord Vishnu, Vitthal, and Rukmini were central to his prayers. He had been a regular visitor to Pandharpur. He carried no regrets and harboured no bitterness — qualities that, after a career which included failing his MD on the first attempt, serving for nearly a decade under a man who had once been his student, and spending thirty-four years building a department in conditions of chronic resource scarcity, had been genuinely earned rather than merely professed.
Narayan Shyam Rao Ingole was born on October 11, 1953, in Nagpur, the second of six children. His father brokered deals in the paan market by day and prepared Ayurvedic herbal remedies by evening. His mother Shashikala Bai managed the household without formal schooling. He walked to primary school in Itwari and attended New English High School in Mahal, harbouring ambitions of chemical engineering.
The turning point came when he saw his grandfather — weak, frail, in Indira Gandhi Medical College — sigh and say: "There should be a doctor in the family." The statement settled in him. He traded his mathematics textbooks for biology and enrolled in a BSc at the Institute of Science, Nagpur.
In 1971, MGIMS called for an interview. The panel included Dr. Sushila Nayar presiding, Maharashtra Health Minister Pratibha Patil among a dozen panellists, and a clerical mix-up that had already approved another candidate using Narayan's selection papers by mistake. Dr. Nayar was furious — at the staff, at the confusion, at the situation — and delegated the interview to the remaining panellists while she recovered her composure.
Mr. Kakade, a lawyer on the panel, asked: "Have you ever smoked?"
"No, sir."
"Your friends must be smoking."
"No, sir. I don't have friends who smoke."
A professor: "Do you know the harms of smoking?"
"Sir, I know it can cause lung cancer."
"What else?"
"I don't know, sir. But if you give me a chance to study medicine, I will find out."
He left uncertain. He enrolled in a B.Tech. course at Laxminarayan Institute of Technology. A week into engineering, a telegram arrived: he had been accepted at MGIMS.
At the admission office, a stranger approached him. "I'll give you ₹5,000. Just let my son take your place." A fortune in those days. He paid his own fees instead, becoming Roll No. 22 of the MGIMS Class of 1971.
The first month was orientation at Gandhi's ashram — prayers at four in the morning, voluntary labour, khadi spinning, shared campus cleaning. His batch was the first to undergo the full month; the following year, faculty complaints about lost classroom time shortened it to two weeks for all subsequent batches.
He lived in Patel Hostel, then Dharmanand Hostel, then C Block of the new boys' hostel. Surgery fascinated him. In his final MBBS examinations, he failed it. Six months later, he passed. He completed house jobs in surgery under Dr. Narang and orthopaedics under Dr. Ahuja, intending to pursue postgraduate surgery.
MGIMS offered no postgraduate seats in surgery. BJ Medical College in Pune had places, but they were unpaid. Three years without income was not possible for him. He stayed at MGIMS and enrolled in Pathology — not by passion, initially, but by circumstance. The circumstance eventually became a calling.
In 1978, he joined the Pathology department as Demonstrator. The department then had six lecturers, all MBBS graduates doing their postgraduations simultaneously: Lele, Narang, Khan, S.M. Sharma, Santosh Gupta, and Bhongade. Small rooms, flickering lights, manual blood smears, histopathology slides stained in glass trays, no automated equipment. Teaching slides were scarce because patients were scarce. Faculty sketched microscopic findings on blackboards and reconstructed classic cases from memory.
For his MD thesis, he needed a hundred photographs. Dr. Ahuja lent him his personal Nikon camera. Dr. Moghe insisted on professional photographs from Retina Studio in Nagpur — an expense exceeding a professor's monthly salary. He found the money.
In April 1981, he sat his MD examination. The external examiner Dr. Shridhar Agrawal from Raipur was a legend for severity — it was said he believed first-attempt passes were not possible, and he proved it across three medical colleges simultaneously, passing only two candidates. Ingole was not one of them.
He returned in October 1981. This time, with different examiners at GMC Nagpur, he passed. His career at MGIMS had begun in earnest.
He rose through the standard academic ladder — Lecturer, Reader, Associate Professor, Professor — over more than two decades of steady, methodical work. Along the way, an unusual institutional arrangement shaped a significant part of his middle career.
When the university advertised a single professorship, Dr. S.M. Sharma — the department head — chose not to apply. Out of deference to his senior, Ingole also refrained. This left Dr. Nitin Gangane, seven years his junior, as the sole candidate. Gangane was appointed Professor. For nearly a decade, Ingole served in a department formally headed below him by his own former student.
He did not allow it to strain either relationship. Dr. Sushila Nayar, recognising the awkwardness immediately, created an independent professorship in haematology for Ingole — preserving his seniority and insulating him from the institutional fallout. His camaraderie with both Sharma and Gangane remained intact before and after his retirement. This was not a small achievement.
He mentored twenty-five postgraduate students across his career. He led histopathology and haematology, modernised diagnostic techniques, replaced slow haemoglobin electrophoresis methods with faster alternatives, and introduced automated cell counters that transformed blood analysis. As head of the blood bank, he built a year-round blood donation calendar that grew the bank's annual collection from a handful of donations to 4,000 bottles by the time he retired.
His working method was the method of his era: patience, scrutiny, methodical cross-checking. Hours over slides, books consulted, Dr. Khedikar at IGMC Nagpur telephoned when a case remained uncertain. No flamboyance, no innovation for its own sake. Accuracy achieved through repetition, judgement sharpened through experience.
He retired in October 2015. Then came the swing in his sister's home in Nagpur, the sudden snap, the fall, the paralysis. Four years of physiotherapy. Jyotsna's care. Gradual, partial recovery — enough to walk with support.
He never once asked why. He is a devout man who believes life unfolds as it is meant to, and this belief, held not as performance but as genuine orientation, carried him through the slow work of recovery with a grace that struck those who knew him as entirely characteristic.
He married Jyotsna Pokale of Wardha on January 12, 1983 — after completing his MD, in keeping with the personal rule he had set himself. Their son Abhishek, an MGIMS alumnus from the class of 1998, completed his MD in Community Medicine at the same institution. The family pattern of MGIMS, continued across generations.
He lives now in his own house on the Wardha-Sevagram road, three minutes from the hospital. His days are peaceful. He carries no regrets. The department he helped build over thirty-four years has automated cell counters, immunohistochemistry, molecular diagnostics, liquid-based cytology, AI-assisted screening — a transformation so complete that the department of the 1980s, with its glass staining trays and borrowed Nikon camera and blackboard drawings, seems like another world.
It was another world. He built the bridge between them, slide by slide, donation by donation, student by student, in the quiet methodical way that was always entirely his.
| 1953 | Born, 11 October, Nagpur |
| 1971 | Accepted at MGIMS — refused ₹5,000 bribe, became Roll No. 22, Class of 1971 |
| 1971 | First batch to complete full month orientation at Gandhi’s ashram |
| 1978 | Joined Pathology department as Demonstrator |
| 1981 | Failed MD examination, April — Dr. Shridhar Agrawal, external examiner |
| 1981 | Passed MD examination, October — GMC Nagpur |
| 1983 | Married Jyotsna Pokale of Wardha, 12 January |
| 1981 | Joined MGIMS faculty formally, 1 March |
| 1990 | Dr. Nitin Gangane — former student — appointed Professor above him; Dr. Nayar created independent haematology professorship for Ingole |
| 2015 | Retired, 31 October — after thirty-four years |
| 2016 | Accident at sister’s home, Nagpur — fell from swing, paralysis followed |
| 2020 | Gradual partial recovery after four years of physiotherapy and Jyotsna’s care |
Pancytopenia : A clinicopathologic analysis of 219 cases
Platelet volume parameters in health and disease
Prevalence and co-infection of infectious disease markers in blood donors in a rural hospital in Central India
Leucocyte alkaline phosphatase activity in non-hematological malignancies and its utility as a probable predictor of metastasis with emphasis on breast and colon cancer
Haemostatic Alterations in Sickle Cell Haemoglobinopathies
Thrombocytosis: Age Dependant Etiology and Utility of Platelet Volume indices in Differential Diagnosis
Hemostatic Alteration in Liver Diseases
An Audit of the Fresh Plasma Usage and Study of the Effect of Fresh Frozen Plasma Transfusion on international Normalized Ratio (inr).
A study of ethylene diamine tetraacetic acid (EDTA)- dependent pseudothrombocytopenia
Study of haemostatic profile in patients of type 2 Diabetes Mellitus and Relationship of fibrinogen level to glycemic status (HbA1C) and duration of disease
Dr. Nitin Gangane
MD Pathology (MGIMS, Sevagram) [1987]
PhD (Umeå University, Sweden) [2009]
Sixty years after his birth at Kasturba Hospital, he left Sevagram as Vice-Chancellor of KLE Academy of Higher Education and Research in Belagavi — having served along the way as the first MGIMS alumnus to become Dean of the institution, having earned a PhD from Umeå University in Sweden, having published over 180 papers from a rural teaching hospital in a village, and having built the Population-Based Cancer Registry of Wardha district into a nationally recognised public health instrument.
His colleague Dr. Anshu, who worked alongside him for years in the Pathology department, said when he left: "The shock and tears that flowed were genuine."
Nitin Gangane's father Mrigrajendra came from Gulbarga, had been a freedom fighter in the Hyderabad Liberation Movement, had gone underground at sixteen to escape persecution under the Nizam, had worked alongside Vinoba Bhave and Baba Amte, and had moved to Sevagram in 1960 inspired by Annasaheb Sahastrabuddhe. His mother Prabha, orphaned young and raised by an aunt in Mumbai, worked in MGIMS's Medical Records section until her retirement.
The family lived in Sevagram. The boy attended the government school, then Yeshwant High School, then Swavalambi Vidyalaya in Wardha. These were Marathi-medium institutions, rooted in the ordinary life of a small village. What they gave him, alongside his education, was a fearlessness about confronting systems that behaved badly — a quality his father had modelled at sixteen and that Nitin would find repeatedly necessary in his own career.
On June 26, 1976, the first anniversary of Indira Gandhi's Emergency, he attended a resistance meeting in Wardha with his brother Bipin. Police raided. Nitin and Ashish Wele were arrested. Being minors, they were placed in a remand home under the Juvenile Act, where they remained — completing their schooling by attending college during the day and returning to the facility each night — until October 1977, seven months after the Emergency was revoked and the Janata Party had already taken power. The wheels of justice grind slowly. The experience forged something permanent in him.
He entered MGIMS in 1978 with Roll No. 24, one of the last batches to face essay-style papers on Biology, Physics, Chemistry, and Gandhian thought in the entrance examination. He earned his MBBS in 1983.
After internship, he took house jobs in radiology and anaesthesiology and worked briefly as a research officer on a WHO filariasis project. He believed the house job admission process had been unfair to some classmates and took legal action over it — straining his relationship with the MGIMS administrative officer. When the postgraduate radiology course was not offered that year, he turned to Pathology. The turn was pragmatic. Under Dr. S.M. Sharma's mentorship, he studied the histomorphology of malignant soft tissue tumours. He earned his MD in Pathology in December 1987 and his DNB two years later.
Promotion was slow in coming. In December 1991, he left MGIMS for Jawaharlal Nehru Medical College, Sawangi, where a newly established institution offered swift advancement. He completed a six-month oncology fellowship at Tata Memorial Hospital under Dr. Anita Borges and Dr. Kikkeri N. Naresh, and built his expertise in cancer pathology.
At JNMC, he uncovered gross irregularities in the examination revaluation process and reported them to the Vice-Chancellor. The friction with administration followed immediately. When MGIMS advertised a professorship in 1996, he applied. Dr. Sushila Nayar intervened to secure his appointment. He returned to his alma mater.
Dr. Anshu's assessment of his leadership as a teacher is precise enough to quote directly: "It is very difficult to teach diagnostic reasoning in Pathology, as it is both an art and a science. He is one of the very few teachers who could slowly lead a student from a wrong diagnosis to the right one, step by step, carefully demolishing one differential after another, until the student felt as if she had made the correct diagnosis herself."
Beyond the seminar room, his pathology reports were models of clinical utility — concise, focused entirely on what the treating physician needed to begin treatment and determine prognosis, nothing more. His questions in teaching sessions were sharp, basic, and logical. He read continuously, regardless of how busy he was. These were not separate qualities but expressions of the same discipline: a mind that had learned to cut to what mattered and stay there.
The second source of respect was his fairness. He treated every person with respect regardless of their position in the hierarchy. He was present in good times and bad. He did not expect everyone to excel; he understood each person's strengths and worked with those. If someone needed help — a university document, a last-minute recommendation, an introduction to a colleague — it was a phone call away. The department's teaching and non-teaching staff were always willing to give more than they had to, because he had earned that willingness.
He kept a low profile. He rarely raised his voice. He spoke little. None of this prevented him from being the person everyone confided in, the person whose departure produced genuine shock and tears.
He led the department from 2004 to 2018, acquiring equipment and technology against persistent administrative resistance. He mentored eleven MD theses on cancers in Central India. He served as Principal Investigator on seven research projects and co-investigator on twelve, funded by IARC, UICC, NIH, ICMR, UGC, and DST. The Yamagiwa-Yoshida Memorial International Cancer Study Grant took him to IARC in Lyon and NIDCR/NIH in Bethesda. He served as President of the Maharashtra chapter of the Indian Association of Pathologists and Microbiologists from 2006 to 2009. And from a village in Vidarbha, without the institutional infrastructure available at urban research centres, he published over 180 papers in high-impact journals.
In September 2011, Dr. Miguel San Sebastian and Dr. Bhoomikumar Jegannathan from Umeå University visited MGIMS. Their meeting with Nitin sparked an interest in the epidemiology of breast cancer that complemented the regional cancer data he was already assembling. Over the next five years, he made several trips to Sweden. He was awarded his PhD from Umeå University in 2018 — adding European doctoral training to a career built entirely in rural India.
Since 2010, he had led the Population-Based Cancer Registry of Wardha district — a systematic tracking of cancer patterns and trends across a rural population that would otherwise go unrecorded. The registry became a nationally recognised instrument for understanding cancer epidemiology in Central India.
In 2018, he became Dean of MGIMS — the first alumnus of the institution to hold the position. He had been born at Kasturba Hospital. He was now responsible for the institution that hospital anchored.
In 2021, he was appointed Vice-Chancellor of KLE Academy of Higher Education and Research in Belagavi. His PhD, his research record, his deanship, his engagement with MUHS governance, his national and international fellowships — all of it had prepared him for an appointment that was the culmination of a career built with consistent purpose across four decades.
In November 2025, he left KLE to become Executive Director of AIIMS Deoghar in Jharkhand. One does not walk away from a Vice-Chancellorship — a position of comfort and authority — without deliberate intention. Gangane is a man who knows his own mind. Having seen his work through in Belagavi, he chose a new frontier.
He has left Sevagram, even parted with his house there. The village shaped him. He did not need to stay in it to carry what it gave him.
| 1961 | Born, 11 June, Kasturba Hospital, Sevagram — delivered by Manimala Chaudhary |
| 1976 | Arrested during Emergency, 26 June — attended resistance meeting in Wardha with brother Bipin |
| 1976 | Placed in remand home under Juvenile Act — completed schooling while under detention |
| 1977 | Released October — seven months after Emergency revoked |
| 1978 | Entered MGIMS — Roll No. 24, Class of 1978 |
| 1983 | Completed MBBS |
| 1987 | Completed MD Pathology, December — joined MGIMS faculty |
| 1989 | Completed DNB |
| 1991 | Left MGIMS for JNMC Sawangi, December |
| 1995 | Oncology fellowship, Tata Memorial Hospital — under Dr. Anita Borges and Dr. Kikkeri N. Naresh |
| 1996 | Returned to MGIMS — Dr. Sushila Nayar intervened to secure appointment |
| 2006 | President, Maharashtra chapter, Indian Association of Pathologists and Microbiologists — until 2009 |
| 2010 | Led Population-Based Cancer Registry of Wardha district |
| 2018 | Awarded PhD, Umeå University, Sweden |
| 2018 | Became Dean of MGIMS — first alumnus to hold the position |
| 2021 | Appointed Vice-Chancellor, KLE Academy of Higher Education and Research, Belagavi |
| 2025 | Left KLE — appointed Executive Director, AIIMS Deoghar, Jharkhand, November |
Immunophenotyping of primary malignant nodal and extranodal lymphoid neoplasms: a prospective and retrospective study
Utility of cell block technique by microwave processing for rapid diagnosis in fluids and fine needle aspirates
Study of epidemiological factors in oral cancer
Population based cancer registry of Wardha district
Cytohistological discrepancies in carcinoma cervix
Study of epidemiological factors in esophageal cancer
Study of oxidant and antioxidant status in tubercular, reactive and metastatic lymphadenopathy
Association of Epstein Barr Virus (Ebv) infection with Non-Familial Breast Cancer in Women in Central india: An Immunohistochemical and Serological Study
Study of histologic profile of psoriasis
Expression of CD34, PCNA and VEGF in in-situ and invasive squamous cell carcinoma of cervix
Estrogen receptors, progesterone receptors and p53 expression in complex and/or atypical endometrial hyperplasia and endometrial adenocarcinoma
Expression of Her2/neu receptor in epithelial ovarian malignancies.
E-cadherin as a prognostic biomarker in oral squamous cell carcinoma
Role of P53 and her 2 neu as a prognostic biomarker in breast carcinoma
Comparison between automated and manual method of reticulocyte count
Role of p53 and Her-2/neu as a prognostic biomarker in breast carcinoma
Role of Caspase-3 as a prognostic biomarker in breast carcinoma
Role of Caspase-8 as a prognostic biomarker in breast carcinoma
Estrogen receptors, progesterone receptors, and p53 expression in complex and/or atypical endometrial hyperplasia and endometrial adenocarcinoma
To evalaute the diagnostic accuracy of CBNAAT in comparison to FNAC in suspected cases of tubercular lymphadmitis
Dr. Arvind Bhake
MD Pathology (Indira Gandhi Government Medical College, Nagpur) [1987]

Professor of Pathology · Fourteen Years at Sevagram · The Pathologist Who Wrote About Cells the Way a Naturalist Writes About Birds
Before computers arrived at MGIMS, Dr. Arvind Bhake wrote his cytology reports by hand.
Each one was meticulous — the cell described, its cytoplasm detailed, its nucleus examined, the structure and any deformity rendered in prose that was both scientifically precise and, by the account of those who read it, almost lyrical. Old-timers at MGIMS still recall those reports. They remember them with the particular fondness reserved for things that have been lost — noting, without sentimentality but with genuine regret, that the reports generated today with the speed of a WhatsApp message have shed something that his carried.
He was a pathologist who wrote about cells the way a good naturalist writes about birds: with exactness, yes, but also with an evident pleasure in the thing being described. Cytopathology was, to him, the heartbeat of the discipline — the ability to distinguish health from disease in minutes, from a microscopic glance, which he thought was nothing short of magic. He had chosen pathology after watching anxious surgeons pace outside the laboratory waiting for biopsy reports. It struck him that before a single incision was made, it was the pathologist's eye that determined the course of treatment. The power to diagnose, to unravel the unseen — this was the thing.
Arvind Bhake was born on January 12, 1961, in Wardha, the youngest of six children in a household shaped by his father Sridhar Madhav Bhake, principal of the local Government College of Education, and his mother Shalini, who managed the family with warmth and quiet efficiency. He passed through Government Practicing School and then the red-bricked corridors of Craddock High School in Wardha, completing his schooling in 1976, followed by two years at Jankidevi Bajaj College of Science.
Medicine announced itself, as it sometimes does, through a school skit. He played a doctor. His classmates called him "Doctor Saheb" afterward, and the name stuck long enough to become a direction. In 1978, he entered Indira Gandhi Government Medical College, Nagpur. He earned his MBBS in 1983, completed internship and house jobs in medicine and surgery, and then chose pathology — drawn there by the logic of the waiting surgeons and the microscope's revelatory power.
His mentors were Dr. Khedikar and Dr. Anil Pendsey. Dr. Khedikar — a woman of remarkable simplicity — had a quality rare in teachers: the ability to distil the most complex diagnoses into perfect clarity. His MD thesis examined imprint cytology of lymph nodes, taking him deep into microscopic analysis. During that period, he formed an unlikely camaraderie with Mr. Srivastava, the photographer at Retina Studio in Nagpur — one a doctor, the other an artist, both committed to precision.
He earned his MD in Pathology in 1987 and spent a year sharpening his skills in histochemistry, molecular diagnostics, and haematology techniques. In 1988, MGIMS advertised a vacancy.
MGIMS was not, to Arvind Bhake, merely a job opportunity. It was a place he had heard about since childhood — his brothers had spoken of Dr. Ulhas Jajoo with reverence, and the institution's reputation as one that rivalled AIIMS, JIPMER, and PGI was part of the family's understanding of what serious medicine looked like. He arrived for the interview with ambition and genuine respect for the place.
The selection committee was formidable: Dr. Sushila Nayar, Kamala Desikan, Dean K.S. Sachdeva, Dr. K.V. Desikan, Dr. Shobha Grover, and Dr. Narendra Samal. They examined him on histopathology, cytology, haematology, and staining techniques. He was selected.
He joined on a quiet November morning in 1988, entering a department led by Professor Narendra Samal, with Dr. Satish Sharma, Dr. Narayan Ingole, Dr. Kiran Swarup, Dr. Nitin Gangane, and Dr. Subir Mitra as colleagues. Dr. K.V. Desikan held an Emeritus Professorship. It was a department with depth and character, shaped by over a decade and a half of steady institution-building.
Sevagram became his home for fourteen years. He read widely and seriously — Anderson, Robbins, Wintrobe, Williams, Tietz, Walter, Bancroft, DeVita on molecular pathology, Dacie and Lewis, Christopher Fletcher, Ackerman, Allen Gibbs, Armed Forces Institute of Pathology updates. The MGIMS library was his second home. His cytopathology practice deepened. His reports grew in quality and in the particular quality of attention — precise and almost literary — that made them memorable to the clinicians who received them.
One episode captures the range of what pathology demanded in those years. Dr. Samal asked him to introduce coagulation tests in the department. There was no ready source of thromboplastin. He sourced a dead rabbit from the animal farm, worked with the Microbiology department to extract the rabbit's brain, and obtained the thromboplastin he needed. The prothrombin time and INR tests followed — the department's first step toward advanced coagulation diagnostics, improvised entirely from available materials. This is what building a department in a rural medical college required: not just knowledge, but the willingness to solve problems with whatever was to hand.
He diagnosed a case of pseudomyxoma peritonei alongside Dr. Kalantri in 1997 — a rare finding, published in Indian Practitioner — one of the small triumphs he remembers with particular pleasure.
He mentored MD residents in cytology-based research that advanced the department's diagnostic capabilities: Rajiv Tangri on fine needle aspiration cytology in focal liver lesions, Nitin Shende on nucleolar organizer regions in breast cytology, Gupta on endoscopic brush cytology in upper gastrointestinal abnormalities, Naresh Gurbani on FNAC in prostate lesions, Ranbeer Singh on FNAC in soft tissue tumours, and Suniti Pathak on endometrial aspiration cytology. The common thread was cytology — the tool he loved — applied across the body's systems with clinical questions driving each study.
He rose to Reader by 1992 and Professor by 1998. His teaching reflected his own formation: close attention to the specimen, insistence on the pathologist's eye as the primary instrument, pleasure in the complexity of what cells could reveal. He believed that immortality in medicine lay not in titles or tenure but in publications and shared knowledge — a belief reflected in his consistent research output and editorial work.
He is drawn to Marathi drama and classical music with the same genuine engagement he brings to pathology. He played table tennis and football in his younger years, serving as a steadfast centre-back. He sings — Marathi and Hindi songs — and has considered, with the slightly amused self-awareness of someone who knows his own enthusiasms, starting a YouTube channel. He speaks of writing a book on lymph nodes for fellow "lymphomaniacs" — the self-coined term that captures how he feels about his specialty's corner of the body.
He married Anita Savargaonkar, a physiotherapist from Pune, in 1997. Their son Adhokshaj is pursuing his MD in Medicine at Jawaharlal Nehru Medical College, Sawangi — the institution Arvind joined in November 2003 after fourteen years at MGIMS, where he continues to teach and lead and investigate.
About Sevagram, he says with the wry precision of someone who has earned the right to be both affectionate and funny about a place: "Sevagram will always have a special place in my memory — at least until old age brings some neurodegenerative disease and makes me forget it all."
The reports he wrote by hand, detailing cells in prose that read like something worth reading, have not been forgotten by those who received them. In the era of automated outputs and rapid turnaround, they are remembered as a different mode of attention — slower, more thorough, more fully inhabited. He was a pathologist who looked carefully and wrote well about what he saw — a combination rarer than it should be, and more valuable than it is usually credited to be.
| 1961 | Born, 12 January, Wardha |
| 1978 | Entered Indira Gandhi Government Medical College, Nagpur |
| 1983 | Completed MBBS |
| 1987 | Completed MD Pathology — thesis on imprint cytology of lymph nodes |
| 1988 | Joined MGIMS, November |
| 1992 | Promoted Reader in Pathology |
| 1997 | Married Anita Savargaonkar, physiotherapist, Pune |
| 1997 | Diagnosed pseudomyxoma peritonei alongside Dr. Kalantri — published Indian Practitioner |
| 1998 | Promoted Professor of Pathology |
| 2003 | Left MGIMS, November — joined Jawaharlal Nehru Medical College, Sawangi |
Fine needle aspiration cytology in diagnosis of focal liver lesions
Study of argyrophilic nucleolar organizer regions in breast cytology
Endoscopic brush cytology in diagnosis of upper gastrointestinal tract lesions
Fine needle aspiration cytology in diagnosis of lesions of prostate
Fine needle aspiration cytology in diagnosis of soft tissue tumors
Endometrial aspiration cytology in diagnosis of normal and abnormal endometrium
Dr. Pratibha Narang
MD Microbiology (Lady Hardinge Medical College, New Delhi) [1971]

Microbiology lectures at MGIMS were scheduled after lunch. Post-lunch drowsiness was a known hazard. Dr. Pratibha Narang's sharp eyes and, as Dr. Prabha Desikan recalled, her impeccable aim were the corrective: a piece of chalk flying through the air with precision, waking the unfortunate student before she had registered what had happened. The chalk landed. The student woke. The lecture continued.
This detail is offered not as an anecdote about discipline but as an introduction to a woman whose entire career was organised around the refusal to accept less than full engagement — from her students, from her institution, from herself. She taught Microbiology for over fifty years at MGIMS, founded its department from nothing, built it into a laboratory of national repute, led the institute as Dean, served as Secretary of the Kasturba Health Society, published 145 scientific papers including 105 original articles on tuberculosis, supervised 34 MD theses and two PhD students, won the Senior Commonwealth Fellowship and the first Dr. P.R. Gangadharam International Travel Award given by the American Lung Association, and — when her institution did not yet offer postgraduate courses — packed up her two daughters, aged two and four, and moved to Delhi to complete her MD herself.
She retired in March 2025. She had been at MGIMS for fifty-one years.
Pratibha Narang was born on September 9, 1947, in Srinagar. Her father was a mathematics teacher of considerable distinction — a gold medallist from Punjab University who taught at DAV College, Hoshiarpur, and then at the Doon School in Dehradun, where he eventually retired as Vice Headmaster. He wrote twenty-five mathematics textbooks, contributed articles on Einstein's theory of relativity to the Times of India and Hindustan Times, was published in the Illustrated London News, and was invited by the BBC to speak on public schools. The household she grew up in was one in which intellectual seriousness was the ambient condition.
At ten, she joined the Doon School as a day student. Her classmates included Sanjay Gandhi, Kamal Nath, Naveen Patnaik, Mani Shankar Iyer, and Karan Thapar. She completed her intermediate at the Allahabad Board and entered Lady Hardinge Medical College in Delhi in 1965. She earned her MBBS, served as the college's cultural president, and won the Annie McKenzie Prize for being the best all-rounder.
After graduating, she completed two house jobs in Obstetrics and Gynaecology at AIIMS from 1971 to 1972. On January 16, 1971, she married Dr. Ravinder Narang, a surgeon completing his MS in General Surgery from PGI Chandigarh. Gynaecology had been her intended speciality. The pivot to Microbiology was practical and deliberate. Her husband was seeking a faculty position at a teaching hospital; a clinical speciality and the demands of a young family were not, she judged, compatible with the life they were building. Microbiology offered a different rhythm.
Her mentor at Lady Hardinge, Dr. K.B. Sharma, gave her the counsel she would remember for the rest of her career: "Virgin soil yields the best harvest, provided one tills it."
On August 10, 1973, she joined MGIMS as Lecturer in Microbiology — the first Microbiology teacher the institution had appointed. Microbiology was then still part of the Pathology department. MGIMS had no postgraduate programme. In 1976, she took study leave, moved to Delhi with her two daughters aged two and four, completed her MD in Microbiology at Lady Hardinge, and returned to Sevagram in May 1978 as Reader. The soil was virgin. She began to till.
Microbiology became a separate department on August 15, 1980. It had two technicians, no postgraduate students, and Dr. Narang. She became Professor and Head in 1982 and led the department for twenty years.
The intellectual centre of her work was tuberculosis. This was not an abstract speciality choice. Dr. Sushila Nayar had founded the Badshah Khan Hospital in Faridabad as a TB sanatorium in the early 1950s, had watched children and young adults die there, and had never released that specific grief. Her commitment to TB control was personal. When Dr. M.D. Gupte, a professor of Community Medicine at MGIMS, secured ICMR funding for a field trial on TB but left before completing the project, Dr. Nayar turned to Dr. Narang — the co-investigator, without prior field experience — and asked her to lead. She led. The result was the first ICMR field trial on intermittent Short Term Chemotherapy for pulmonary tuberculosis patients in the Wardha district, examining TB prevalence in both tribal and non-tribal populations through smear and culture-positive cases.
This was the work that shaped the rest of her research career. TB became her subject in its full complexity — latent and active infection, drug-sensitive and drug-resistant strains, pulmonary and extrapulmonary disease, typical and atypical presentations. Her Microbiology lectures built Robert Koch's world for students who had never imagined microorganisms could be made vivid and consequential. In the seminar hall, in the laboratory, at the blackboard, she crafted a narrative around Mycobacterium tuberculosis that made the discipline feel like the most important subject in medicine — which, in terms of global burden of disease, it arguably was.
She established the postgraduate programme in Microbiology in the 1980s, and TB research became its central axis. The students she produced — Rajni Gaind, Manjusha Dudhe, Prabha Desikan, Rahul Narang, Ujwala Raut — became leading microbiologists across India. She supervised thirty-four MD theses and two PhD students. She collaborated with TB researcher Madhukar Pai in a study of latent tuberculosis among healthcare workers — research that placed MGIMS on the international TB research map. She published 145 papers between 1974 and 2022, 105 of them original articles on tuberculosis, and received seventeen extramural research grants from national and international agencies.
In 1992, she received the Senior Commonwealth Fellowship to the United Kingdom. In 2000, she became the first recipient of the Dr. P.R. Gangadharam International Travel Award, given by the American Lung Association under the IUATLD. In 2006, the Tuberculosis Association of India gave her the Lupin-TAI Award. In 2012, she became President of the Indian Association of Medical Microbiologists. In 2018, the Vidarbha Association of Medical Microbiologists created the "Dr. Pratibha Narang VAMM Professional Achievement Oration Award" in her honour — given annually to a senior microbiologist from the region for outstanding contributions.
She became Dean of MGIMS in 2002 — the first woman to hold the position — and served until 2007. In October 2007, she became Secretary of the Kasturba Health Society, a role she held until 2014. Those who worked with her in administrative roles described the same qualities that characterised her teaching: calm, attentive, thorough, firm where necessary, never indifferent to the person in front of her.
Dr. Prabha Desikan — who chose Microbiology for her postgraduate training despite being third on the merit list, specifically because of Dr. Narang's example, and who went on to become Director of ICMR-BMHRC, Bhopal — described her as a diagnostician whose approach to clinical samples was exemplary, a researcher whose clarity about hypotheses was remarkable, and a mentor who was deeply invested in each of her students. The firmness, the practical advice, the wealth of knowledge and experience — and behind all of it, a kindness and warmth that Desikan called rare and invaluable.
About her own mentor, Dr. Narang said: "Dr. Sushila Nayar's perfection and attention to detail were evident everywhere — in fieldwork, conference presentations, publications, and grant applications. She seemed to read every word before it went to print." The quality she most admired in her teacher was the quality she spent fifty years embodying in her own practice.
Her family became a small medical school in itself: Dr. Ravinder Narang in surgery, daughter Ritambhara in gynaecology, daughter Dipti in paediatrics, son Udit in internal medicine, sons-in-law and daughter-in-law all in medicine. A household in which medicine was not a profession but an inheritance.
She continued as Emeritus Director-Professor after stepping down from departmental leadership, remaining available to faculty and students with the consistency of someone who does not know how to be otherwise. The chalk, presumably, still had its uses.
"Virgin soil yields the best harvest, provided one tills it."
She tilled it for fifty-one years.
| 1947 | Born, 9 September, Srinagar |
| 1957 | Joined Doon School, Dehradun, as day student — classmates included Sanjay Gandhi, Naveen Patnaik, Kamal Nath, Mani Shankar Iyer, Karan Thapar |
| 1965 | Entered Lady Hardinge Medical College, Delhi |
| 1971 | Married Dr. Ravinder Narang, 16 January |
| 1971 | House jobs in Obstetrics & Gynaecology, AIIMS |
| 1972 | Daughter Ritambhara born, 4 March — began Demonstratorship in Microbiology, Lady Hardinge |
| 1973 | Joined MGIMS, 10 August — first Microbiology teacher appointed |
| 1976 | Took study leave — moved to Delhi with daughters aged two and four |
| 1978 | Completed MD Microbiology, Lady Hardinge — returned to MGIMS as Reader, May |
| 1980 | Microbiology became separate department, 15 August |
| 1982 | Appointed Professor and Head of Microbiology |
| 1992 | Senior Commonwealth Fellowship — visited public health and reference laboratories, United Kingdom |
| 2000 | First recipient, Dr. P.R. Gangadharam International Travel Award — American Lung Association, IUATLD |
| 2002 | Became Dean of MGIMS — first woman to hold the position |
| 2006 | Lupin-TAI Award — Tuberculosis Association of India |
| 2007 | Became Secretary, Kasturba Health Society — until 2014 |
| 2012 | President, Indian Association of Medical Microbiologists |
| 2018 | Vidarbha Association of Medical Microbiologists created “Dr. Pratibha Narang VAMM Professional Achievement Oration Award” in her honour |
| 2025 | Retired, 31 March — after fifty-one years at MGIMS |
Diagnostic importance of stick ELISA in smear negative cases of pulmonary tuberculosis
Prevalence and characterization of non tuberculosis mycobacteria (NTM) among symptomatics screened for pulmonary tuberculosis in community.
Study of Klebsiella pneumoniae in hospital patients and hospital environment.
A study of Trichomonas vaginalis infection with evaluation of different diagnostic techniques
A comparative study of Campylobacter jejuni in childhood diarrheas among the hospital and community subjects.
Evaluation of growth of Mycobacterium tuberculosis on different culture media
Detection of circulating tubercular antigens with Ayoama – B using stick ELISA technique
Microbiological and epidemiological study of fungal isolates in sputum of symptomatics for pulmonary tuberculosis
Microbial flora in cases of cervicitis vaginitis in reproductive group with reference to some epidemiological parameters
Role of anti neural antibodies in nerve damage in leprosy patients.
Epidemiological characterization of salmonella typhi strains using serotyping, phage typing, biotyping antibiogram and plasmid transfer as marker
A study of staphylococcal bacteraemias in hospitalized patients.
Epidemiological typing of clinical isolates of proteus species.
Study of mycobacterial isolates from clinical samples with sub division of Mycobacterium tuberculosis into its variants.
Evaluation of investigative techniques and clinical parameters in the diagnosis of childhood tubercular lymphadenitis- a field study.
Evaluation of diagnostic potential of Mycobacterium tuberculosis excretory-secretory antigen (ESAS-DEI) by stick ELISA in tuberculosis
Standardization and evaluation of direct sensitivity test for M. tuberculosis in pulmonary tuberculosis.
Detection of extended spectrum beta lactamases producing strains of Klebsiella pneumoniae and oxytoca in rural hospital
A study of vancomycin resistance amongst the methicillin resistant strains of staphylococcus aureus isolated in a rural hospital.
Evaluation of different screening procedures for the detection of extended spectrum beta lactamases (ESBLs).
Paraffin slide culture technique for isolation of nontuberculous mycobacteria from stool and sputum samples
Evaluation of BACTEC 460 TB system and serodiagnostic kits in pulmonary and extrapulmonary tuberculosis.
Blood culture positivity rate for mycobacteria of HIV seropositive and seronegative cases suspected of tuberculosis.
Evaluation of rapid multi-tube method for detection of susceptibility of Mycobacterium tuberculosis to rifampicin and isoniazid
Comparison of a whole blood interferon gamma release assay with tuberculin skin testing to detect latent tuberculosis infection in children.
Isolation and characterization of mycobacterial species from AIDS patients attending a rural hospital in central India
Comparison of MTT Tube method with conventional method and real time PCR for detection of Rifampicin resistance in Mycobacterium tuberculosis
Characterization of Non tuberculous Mycobacterial isolates from HIV seropositive patients attending a rural hospital and their correlation with environmental isolates
Detection of Amp-C Beta lactamases producing bacteria from various clinical specimens in a rural hospital
Detection of Extensively Drug Resistant (Xdr) Strains Amongst the Multidrug Resistant (Mdr) Mycobacterium Tuberculosis Isolates Processed in Tertiary Care Hospital in Central india.
Evaluation of Direct MTT Colorimetric Method For AFB Positive Sputum in order to Detect Rifampin Resistant Mycobacterium Tuberculosis.
Speciation and Drug Susceptibility of Non-Tuberculous Mycobacteria Isolated From Symptomatics For Pulmonary Tuberculosis.
Epidemiology of Nontuberculous Mycobacteria (NTM) from the environmental samples in Wardha district in Central India
Isolation,identification and characterization of Candida isolates from oral lesions
Study of high risk human papillomavirus genotypes and epidemiological factors in cervical cancer patients and normal women
Evaluation of newer in situ cold staining methods against conventional Ziehl-Neelsen for the detection of acid fast bacilli in sputum.
Dr. Deepak Kumar Mendiratta
MD Microbiology (Government Medical College, Patiala) 1984

He had spent four years as a medical officer at a primary health centre in Sauja — a village of under a thousand people, seventy-eight kilometres from Chandigarh, poor road connectivity, unreliable electricity, the nearest bus stop reachable only by scooter. Five kilometres of bicycle riding at the far end. This was his daily commute to work. By the time he arrived in Sevagram in November 1986, rural life held no surprises for him. He adapted to village life, as one account put it, as naturally as a duck takes to water.
This is worth establishing early, because it explains something about why he stayed. Many faculty members came to Sevagram from cities and experienced the simplicity as a sacrifice to be endured. Mendiratta arrived already formed by the rural Punjab experience — the 1984 riots following Indira Gandhi's assassination had eventually driven him to seek something new, but what he was looking for was not urban comfort. He wanted to do better microbiology. Sevagram, under Dr. Pratibha Narang, offered exactly that.
Deepak Kumar Mendiratta was born on October 30, 1952, in Agra, the son of Shri Prem Nath Mendiratta, an aeronautical engineer in the Indian Air Force, and Rita Rani Mendiratta. The family moved with his father's postings — Agra, Tambaram, Bangalore, where he attended St. Joseph's High School — and he completed his matriculation in 1969 at Baroda High School after five years there. He earned his BSc at Government Mohindra College, Patiala, in 1973, and his MBBS at Government Medical College, Patiala, in 1977.
Between 1977 and 1982, he served in the Punjab Civil Medical Services, which included four years at the Sauja primary health centre — the bicycle and the scooter and the quiet difficulty of medicine practiced far from backup. In December 1982, he moved to a Demonstrator post in the Microbiology department at his alma mater in Patiala, completing his MD in December 1984.
After his MD, he returned to village practice for two years. Punjab in 1984 was convulsed by the riots following the assassination. Fear and uncertainty accumulated. A trip to Delhi brought him to Dr. Shrinivas, Head of Microbiology at AIIMS, who listened to his career ambitions and suggested Sevagram immediately — the Microbiology department under Dr. Pratibha Narang was exactly the environment he was describing. Mendiratta wrote to Dr. Narang. Her reply was warm and elegant. He packed his belongings and took the next train south.
He arrived on November 17, 1986.
He began in two-room accommodation in Kabir Colony. His parents, who had retired to Lucknow in 1979, moved to Sevagram in 1999 and remained there until their deaths. In 2002, he built his own house in Sushila Nagar Colony, a kilometre from the college, with Dr. Ramji Singh and Dr. B.S. Garg as neighbours.
The department he joined had Dr. Narang, postgraduate students Dr. Tripathi and Dr. Ramani, and two technicians. He had come from general practice and a demonstrator post — not from a research-intensive academic background. The initial hesitation was honest: he was uncertain whether he was equipped for faculty life. Dr. Narang's manner dissolved the uncertainty quickly. They worked side by side, sharing slides, discussing cases, refining diagnoses. The department had the atmosphere of a family rather than a hierarchy. Outside working hours, the young faculty community gathered for badminton, carrom, birthday celebrations, and staff club events — the social texture of a campus where people genuinely liked each other.
Two years after joining, drawn by the prospect of higher earnings, he applied for a faculty position in Saudi Arabia. Dr. Narang gave him a two-year leave of absence. He worked at Naib Hospital, Gazi, from February 1989 to February 1991. Dr. Sushila Nayar was keen for his return. When his Saudi term ended, he came back to Sevagram.
He was promoted to Associate Professor in August 1995, Professor in August 2002, and Director-Professor shortly before his departure. When Dr. Narang became Dean in 2002, she handed the Microbiology department to him. He led it for twelve years.
The research direction he inherited from Dr. Narang was tuberculosis, and he continued it with full commitment. Among his most significant contributions was a field trial on short-course chemotherapy for tuberculosis — work that helped establish the evidence base for the DOTS regimen adopted nationally. He conducted important research on tuberculous lymphadenitis and leptospirosis. In 2003, the department collaborated with the University of California, Berkeley, on a diagnostic study using gamma interferon to detect latent TB — the partnership with Madhukar Pai that Dr. Narang had initiated, continued and developed under his leadership.
Across his tenure, he undertook twenty-three national, international, and regional research projects, published nearly eighty papers, and guided eleven postgraduate students from Ravneeth Kaur in 2002 to Somnath Bhunia in 2013. Their theses ranged across the infectious disease spectrum of rural Central India — leptospirosis in acute febrile illness, Candida in preterm neonates, enterococcal resistance patterns, non-viral microbial keratitis, metallo-beta-lactamase production in Pseudomonas and Acinetobacter, PCR for neonatal sepsis diagnosis. The breadth reflected a department whose interests extended well beyond any single pathogen.
Teaching was a significant part of what he was — a fact that became sharply visible after he left Sevagram. At Chirayu Medical College in Bhopal, where he became Dean in May 2019, microbiology attendance among students stood at ten percent when he arrived. Within a few months, it reached ninety percent. This required no particular magic: it required the consistent application of the clarity, approachability, and high expectation that his postgraduate students at MGIMS had valued and that he brought unchanged to a new institution.
He described Dr. Narang with the precise warmth of someone who has chosen their words carefully: "It's rare to find and work with such a wonderful head of department. She was not only a philosopher and guide but also showered affection like an elder sister."
He married Mala, originally from Bareilly, on October 8, 1981. She had been teaching school in Patiala. In 1991, she joined MGIMS as a computer operator and rose through the institution's administrative structure to become Administrative Officer — a position she held until 2014, when she resigned coinciding with her husband's departure. Their careers at MGIMS ran in parallel for twenty-three years. Both left together when the chapter closed.
Their son Sidharth — MGIMS 2004, MS Surgery, MCh Plastic Surgery from CMC Vellore — practises privately in Nagpur. Their daughter Surabhi, an engineer, lives in the United States.
He left MGIMS on August 7, 2014, for Chirayu Medical College in Bhopal. The private, for-profit college environment was not congenial — the structured restrictions, the intellectual atmosphere thinner than what he had known, the loss of the autonomy Sevagram had given him. On October 31, 2022, he retired from academic medicine. He spends his time now in Nagpur with his grandchildren.
The years in Sauja on a bicycle, the years in Sevagram working through slides with Dr. Narang, the twelve years leading the department, the field trial that contributed to DOTS, the eighty papers, the eleven postgraduates — these are the constituents of a career built in village settings, by a man who was formed by rural life early enough that it never felt like sacrifice.
| 1952 | Born, 30 October, Agra |
| 1973 | Completed BSc, Government Mohindra College, Patiala |
| 1977 | Completed MBBS, Government Medical College, Patiala |
| 1977 | Joined Punjab Civil Medical Services — four years at Sauja PHC |
| 1981 | Married Mala, 8 October, Bareilly |
| 1982 | Demonstrator, Microbiology, GMC Patiala |
| 1984 | Completed MD Microbiology, December |
| 1986 | Arrived MGIMS, 17 November |
| 1989 | Two-year leave — Naib Hospital, Gazi, Saudi Arabia |
| 1991 | Returned to MGIMS, February — Mala joined as computer operator |
| 1995 | Promoted Associate Professor, August |
| 1999 | Parents moved from Lucknow to Sevagram — lived with him until their deaths |
| 2002 | Promoted Professor, August — took charge of Microbiology department when Dr. Narang became Dean |
| 2003 | Collaborated with University of California, Berkeley — gamma interferon study for latent TB detection |
| 2014 | Left MGIMS, 7 August — Mala resigned same day after 23 years |
| 2019 | Dean, Chirayu Medical College, Bhopal — May to November 2020 |
| 2022 | Retired from academic medicine, 31 October |
A study of seropositivity for leptospirosis in cases of acute fever attending out patient department of a rural hospital in Wardha district
Study of colonization by yeast in the preterm neonates admitted in the NICU of a rural hospital with special reference to Candida species
Speciation and characterization of enterococci isolated from patients in a rural hospital with special reference to high level aminoglycoside resistance (HLAR)
Study of non viral microbial keratitis in patients attending Kasturba hospital, Sevagram in central India.
Clinical and bacteriological correlates of whole blood interferon gamma (IFN- ?) in newly detected cases of pulmonary TB.
Study of SXT element in Vibrio cholerae in a rural hospital of Central India
Comparison of Microscopy, Culture on LJ and Bactec 460 TB System and Detection of insertion Sequence 6110 in Sputum For the Diagnosis of Tuberculosis Pulmonary Symptomatics
Detection of Metallo-Beta-Lactamase Producing P.Aeruginosa Isolated From Patients Attending A Rural Hospital in Central india Using Phenotypic and Genotypic Methods
Prevalence of Metallo-B-Lactamases in Clinical Isolates of Acinetobacter Baumannii From a Tertiary Care Rural Hospital in Central india.
Prevalence of ?-Lactamases and their Co-Expression in Gram Negative Bacilli Isolated From invasive Sites of Patients Admitted in Tertiary Care Hospital of Central india.
Utility of Clinical Parameters, Septic Screen and Pcr For Rapid Diagnosis of Bacterial Neonatal Sepsis in Culture Positive Cases.
Detection and characterization of Ampc β lactamase in Escherichia coli and Klebsiella pneumoniae isolated from sterile fluids of patients attending a tertiary care rural hospital by phenotypic and genotypic method.
Dr. Radheshyam Naik
MD Medicine (Government Medical College, Nagpur) [1970]
LLB (Nagpur) [1981]

The day before he died, Dr. Bipin Tirpude drove out to Bahera — the ancestral village in Raipur district where Radheshyam Naik had chosen to spend the final chapter of his life. The Parkinson's had slowed him, and the dementia had loosened some memories, but that afternoon, sitting with his oldest student — now the head of the very department he had built — Naik talked about Sevagram. He remembered the classrooms, the hostel, the boys and their parties. He asked, quietly, whether it might be possible to go back and visit.
Tirpude said yes. He began making arrangements — a lunch, a gathering of the old department staff, a small reunion in the place that had occupied Naik for more than two decades. On April 1, 2018, a Sunday, before any of it could happen, Naik died at home. He went the way he had lived: without fuss, without spectacle, without the bustle he had spent his whole career carefully avoiding.
Radheshyam Naik was born on November 2, 1938, in Bahera, a village eighty kilometres north of Durg in what is now Chhattisgarh. He arrived on Krishna Janmashtami, so his parents named him accordingly. His father, Shri Man Rakhan Lal, was a zamindar who would later give a substantial portion of his land to Vinobaji's Bhoodan movement. The son inherited something of that willingness to hold things loosely.
He went to Government Medical College, Nagpur, earned his MBBS in 1962, and stayed for an MD in Medicine, completing it in 1970 under Dr. J.N. Berry — the legendary physician who ran the Department of Medicine with the quiet authority of someone who had seen everything and forgotten nothing. Three years under Berry left a mark. Naik emerged from them precise, unhurried, and constitutionally incapable of panic.
But medicine was not where he ended up. In those years, medical schools routinely pulled faculty from general medicine to staff their forensic departments — Forensic Medicine being the specialty nobody volunteered for. When Naik was asked to make the move, he made it without argument. He set about learning a new field with the same methodical thoroughness he had brought to the one he was leaving.
What followed was one of the stranger academic CVs in Indian medicine. To the MD in Medicine he added a Diploma in TB and Chest Diseases, then an LLB, then a Diploma in Business Management, then an MA in Public Administration, then an MA in Political Science. He studied law partly because a forensic physician who understands courts is worth more than one who does not, and partly because Naik simply liked to learn things. When he sat for his LLB finals, he topped the examination at Nagpur University. His first MD student, Dr. S.K. Singhal, topped the first year. Teacher and student attended law classes together in the early 1980s, sitting in the same lecture hall, taking the same notes. Neither seemed to find this arrangement unusual.
Forensic Medicine has a structural disadvantage as a teaching subject: its patients are dead. Students who have spent their early clinical years learning to read a living body find themselves asked to redirect that attentiveness toward a corpse. Most resist. The subject had acquired a reputation as dull, mandatory, and to be survived rather than studied.
Naik understood this, and he met it head-on. His lectures were scheduled every Tuesday and Saturday, and they had a hundred percent attendance — not because he demanded it, but because students wanted to be there.
He used Bollywood. His two favourite films for the purpose were Waqt (1965) and Ittefaq (1969) — both crime films, both built around mysteries of identity and evidence — and he used scenes from them to anchor legal medicine concepts in images his students already carried. He owned two licensed 12-bore guns, and when the curriculum reached firearms injuries, he brought them out. The students examined them. The mechanism of injury was no longer abstract.
"Forensic Medicine is traditionally perceived as a dry subject," said Dr. Ashok Mehendale, from the 1976 batch, "but Dr. Naik knew the art of injecting humour, spicing the tedious topics with humour and enlivening his classes. To the class he was a stress buster — jokes, witty metaphors, humorous similes, puns, sarcasm, or a funny story. He was an entertainer as well as an educator."
The one-liners circulated long after graduation. His Chhattisgarhi-inflected Hindi mixed into English mid-sentence — not as an apology for imperfect language but as a genuine expression of someone thinking in several registers at once. Dr. Bipin Tirpude, who spent fifteen years working alongside him, remembered the lectures as improvised performances: the man knew his subject, trusted his audience, and rarely needed notes.
He also had the instinct of an institution-builder. In the early 1980s, before most medical schools in Maharashtra had moved in this direction, Naik started postgraduate training in Forensic Medicine at MGIMS. Over the next two decades, he guided fifteen MD students while simultaneously pushing to separate forensic autopsies from the general pathology workflow, establishing forensic medicine as a discipline with its own rigour and its own institutional territory.
He also, almost incidentally, ran the cine club. Sevagram in the late 1970s had no television. The campus was a long way from anything resembling entertainment. Naik — by then also warden of the boys' hostel — began screening a film every weekend. The cine club ran for years, a weekly punctuation in the quiet of a village campus where evenings would otherwise have offered nothing but study.
He lived in Nagpur. He came to Sevagram on a scooter — one strategically stationed at each end of the commute, so that a scooter waited for him at Wardha station when he arrived by train, and another waited at Nagpur when he returned. The arrangement was purely practical, and he maintained it for years without complaint.
Dr. V.K. Gupta, from the 1976 batch, remembered him this way: "Cool in the classroom and well-versed with the subject matter, he was running the forensic department as a solo player. He never punished any hooligans. He was liberal with attendance and in the examination too."
As hostel warden, his philosophy was similar. The boys made noise, threw parties, tested rules in the ways that boys always do. He watched with the expression of someone who had long since made peace with human nature. He was not lax so much as realistic — understanding that the energy that makes a student difficult to manage at twenty-two is often the same energy that makes him capable at forty.
His own son, Tarun, was in the MGIMS class of 1987 — Naik's students were also his son's classmates. Dr. Abhay Kelkar, from the same batch, remembered this without ambiguity: "I remember him for his impartial attitude towards his own son. No undue favours were ever granted to him." The son had to sit the same examinations, answer the same questions, and earn the same passing marks as everyone else in the room.
Dr. S.P. Kalantri was Naik's neighbour for several years and also his physician. He wrote later: "Introverted, unassuming, and self-effacing, Dr. Naik was polite to a fault. Although he was armed with an MD in Medicine, he made light of his degree and played a perfect patient — listening to advice carefully and adhering to the treatment to the T."
There is a particular kind of doctor — and Naik was one — who, having spent decades telling patients what to do, cannot bring himself to exercise any authority over his own care. He followed instructions. He did not bargain. He did not deploy his degree as a reason to second-guess. He simply listened, and complied, with the patience he had brought to everything else in his life.
After retirement he went to Nepal — Pokhara — and taught for several years at a medical school there, because the alternative was to stop teaching and that was not a serious option. He came back in 2014 and went to Bahera, the village where he had started.
On the morning he died, the lunch in Sevagram was still being planned. His student was on the telephone. The tables had not yet been set.
He is survived by his wife; by Tarun, who operates at Chandulal Chandrakar Memorial Hospital in Bhilai; by Vishal, an engineer in Pune; and by Harsha, his daughter from the MGIMS batch of 1998, who is now in Manchester.
Three generations of students passed through his classrooms — from the 1975 batch to the 2004 batch. Somewhere in that span is almost every doctor currently practising forensic medicine in this part of India. They learned the subject from a man who had not chosen it, who had not trained for it in the conventional sense, who had simply been told to do it and had decided, without bitterness, to do it properly.
The Bollywood clips, the shotguns, the law classes with his own student, the weekend film screenings, the hundred-percent attendance on Tuesdays and Saturdays — these were the instruments of a teacher who had understood early that the subject was not the obstacle. The obstacle was indifference. And against indifference, he had a well-tested arsenal.
| 1938 | Born, 2 November, Bahera, Raipur district, Chhattisgarh — on Krishna Janmashtami |
| 1962 | Completed MBBS, Government Medical College, Nagpur |
| 1970 | Completed MD Medicine, GMC Nagpur — under Dr. J.N. Berry |
| 1977 | Joined MGIMS, 1 March — Professor & Head of Forensic Medicine |
| 1980 | Completed LLB — topped Nagpur University finals |
| 1980 | Started postgraduate training in Forensic Medicine at MGIMS — among first in Maharashtra |
| 1980 | Attended law classes alongside first MD student Dr. S.K. Singhal — same lecture hall, same notes |
| 1987 | Son Tarun in MGIMS class of 1987 — examined without favour alongside his own students |
| 2002 | Guided final MD student Dr. Pushpendra Singh |
| 2003 | Retired, 9 August |
| 2003 | Taught at medical school in Pokhara, Nepal — several years |
| 2014 | Returned to Bahera — the village where he had started |
| 2018 | Died, 1 April, at home in Bahera |
Criminals a descriptive analysis of 1048 subjects studied in Wardha Nagpur jails
Effect of environmental factor on detection of spermatozoa in seminal stains on different types of cloth
Detection of chlorine by thin layer chromatography in seminal stains on different types of cloth in different environments
Effect of environmental factors in different climates on detection of spermatozoa and choline on seminal stains on different fabrics
Confirmation of diagnosis of septicemia by postmortem culture of surface swab, peritoneal swab, liver spleen kidney and heart blood in cases of burns
Effect of the total serum cholesterol concentration on suicidal behavior
Co-ordinated approach towards the establishment of cause of death in case of burns
Determination of blood group in dried blood stains by absorption evaluation methods on various types of cloth in different environments
Clinico radiological study of third molar as an indicator of chronological age
Detection of soot particles in respiratory passage in cases of in cases of death due to burn
Study of medico-legal epidemiological aspects of burns cases
Role relevance of toxicology laboratory in department of forensic medicine toxicology
Trends of poisoning cases in Kasturba hospital of MGIMS Sevagram Wardha
Role of toxicology laboratory in estimation of poison diagnosis of admitted cases in Kasturba hospital of MGIMS Sevagram Wardha
Dr. Madhav Datatraya Khapre
MD Pharmacology: Government Medical College, Nagpur (1967)

Professor & Head of Pharmacology · Sixteen Years at Sevagram · The Doctor Who Was Also a Celestial Singer
"Anybody with a bit of hard work and rote-learning could become an engineer or doctor," Dr. M.D. Khapre said, "but music and singing could not be learnt this way. It required exceptional imagination, passion, and talent. I wanted to be a devoted Hindustani Classical vocalist in my adolescence but ended up being a doctor instead."
He said this without bitterness. He had made peace with the compromise decades earlier, and the compromise had not been complete — music had remained present throughout his life in Sevagram, filling his home with mehfil sessions and bhajans, carrying him onto the stage of Dhanwate Rang Mandir in Nagpur in the early 1980s, resonating through cultural evenings at MGIMS where his baritone stopped whatever else was happening in a room. He was a doctor who taught pharmacology as though it were a performance art, and a musician who had chosen medicine as his profession, and over time the two vocations became so intertwined that those who knew him could not easily say which was the larger part of him.
Gajanan Ambulkar, who knew him for decades, remembered him simply: "His heart belonged to music, and we often wondered if he was a doctor or a celestial singer."
Madhav Dattatraya Khapre was born on February 4, 1937, in Nagpur, into a family of some standing — his father was a lawyer and landlord, their home a mansion called Khapre Wada on Pataleshwar Road in Badkas Chowk. He attended New English High School, a kilometre from home, and entered Government Medical College, Nagpur, in 1955.
The path to pharmacology came through proximity and character. Dr. Dashputre, the Head of Pharmacology at GMC, lived near the Khapre family. His influence drew Madhav toward the department for his MD. Under Dashputre, and alongside Dr. M.L. Sharma, Dr. V.R. Deshpande, and Dr. P.R. Kherdikar, he learned the discipline as both science and craft — understanding not just mechanism and dosage but the pedagogical challenge of making a subject that students feared into one they could inhabit with confidence.
He began his career as an assistant medical officer at Mayo Hospital, Nagpur, then joined the GMC Pharmacology department as Lecturer in July 1967. In 1970, the Government of Maharashtra deputed him to MGIMS as Reader in Pharmacology. He arrived on February 21, 1971, joining Dr. M.L. Sharma, who had come the previous December. They were the entire department. Sharma was forty-one. Khapre was thirty-three. They had sixty first-year students before them and a great deal to build.
Dr. Sharma and Dr. Khapre were, by every account, complementary rather than interchangeable. Sharma was the senior figure — the Professor, the Principal, the institutional presence. Khapre brought a different register: lighter, more playful in manner, the music always visible beneath the surface, a warmth in the classroom that students felt immediately.
Together they established the culture of the Pharmacology department. Their lectures wove in humour without sacrificing rigour. They used jokes not as decoration but as delivery mechanisms — making a drug's mechanism memorable by embedding it in a story, making an adverse effect stick by attaching it to something funny. Notes taken in their classes were passed down through successive batches as treasured documents, used long after the teachers themselves had moved on. During the 1980s, when textbooks by Satoskar from KEM Mumbai and K.D. Tripathy from MAMC Delhi became the standard references, Khapre's classroom notes circulated alongside them as a parallel curriculum that students trusted more completely.
He understood the linguistic challenge his classroom presented — Marathi, Hindi, and Punjabi speakers, many with limited English fluency, confronting pharmacological terminology for the first time. He moved between English and Marathi during lectures with natural ease, not as a concession but as a genuine teaching decision, understanding that concepts needed to land in the language where the student actually thought. Students felt seen rather than accommodated.
"Pharmacology is like a puzzle," he would say. "Each drug is a piece, and it's our job to fit them together to create effective treatment plans for patients."
He was promoted to Professor in 1977. He returned briefly to GMC Nagpur before resuming his MGIMS professorship in April 1980, teaching seven batches between 1978 and 1985. In 1988, after leaving Sevagram, he mentored Dr. S. John Premendran through a PhD thesis examining the impact of calcium, strontium, and barium on various muscle tissues and their interactions with calcium antagonists — pure pharmacological science that reflected how seriously he took the research dimension of his discipline.
While completing his final MBBS years, he had explored Indian classical music under the tutelage of Pandit Annaji Kshirsagar, immersing himself in the teachings of the two legendary Vishnus — Pandit Vishnu Narayan Bhatkhande and Pandit Vishnu Digambar Paluskar. He did not confine himself to any single Gharana. He was devoted to Ustad Amir Khan's style, and held deep reverence for Sant Gyaneshwar and Gulabrao Maharaj of Madhan, Vidarbha — a devotion that eventually produced an audio cassette of Maharaj's bhajans that he pressed and distributed among friends and colleagues at his own cost, asking nothing in return.
His home in Sevagram became a gathering place. For college events and the Ganpati festival, he organised musical mehfil sessions where his baritone resonated through the air — bhajans from the Ashram Bhajanavali alongside classical compositions. Sudam Ambulkar sang; Hari strummed the tanpura; talented medical students including Avinash Wagh played the tabla; Shyam Babhulkar and others joined. The sessions ran late. There was tobacco, paan supari, tasty chivda, and music until the night was well advanced. On those evenings, the distinction between the pharmacology teacher and the classical vocalist had entirely dissolved.
As Chairman of Sargam — MGIMS's musical society — and cultural in-charge for the college's annual day, he was the animating force behind the institution's cultural life. He performed songs from iconic Hindi films of the 1950s, transported listeners into nostalgia with the ease of someone who understood that music's function was to carry people somewhere they needed to go. He taught acting to MGIMS staff members. When Sujata, the school-going daughter of hospital cashier Mr. D.R. Bele, had performances lined up in Wardha and Nagpur, he accompanied her to the venues personally. The music teacher in him could not distinguish between his students in medicine and anyone else around him who was trying to learn something difficult.
In the early 1980s, he performed in a Marathi drama titled Pankh Labhale Aaj Suranna at Dhanwate Rang Mandir, Nagpur, alongside established actors including Pandit Prabhakar Deshkar. The doctor from Khapre Wada had made it, after all, to the stage he had imagined in adolescence — not as a full-time musician, but fully present, on his own terms.
Gajanan Ambulkar, eighty-two years old when he shared his memories, offered an image that said more than any professional assessment could. Dr. Khapre appeared at his father's funeral in the rain — not light rain, but the kind that turns Vidarbha streets to ankle-deep mud. He came anyway. He shouldered the arthi. He marched forward in the mud without comment, because the family needed him there and he had come to be there.
"I will forever cherish the memory of his presence at my father's funeral," Ambulkar said. "Rain pouring relentlessly. Undeterred by ankle-deep mud, he marched forward, shouldering my father's arthi — a symbol of profound respect."
This is the man the pharmacology lectures came from, and the mehfil sessions, and the quiet presence at performance venues. The kindness was not a separate quality from the teaching or the music. It was the source of all of it.
He left MGIMS in August 1987, taught briefly at GMC Aurangabad, took voluntary retirement in June 1988, then taught at Dr. Punjabrao Deshmukh Memorial Medical College, Amravati, and subsequently at Jawaharlal Nehru Medical College, Sawangi, until 2005. Each institution received the same quality of attention he had given Sevagram.
When I spoke with him by telephone on May 30, 2023, he was eighty-six years old. His voice carried nostalgia and warmth in equal measure. "The two decades I spent in Sevagram during the 1970s and 1980s were the golden days of my life," he said. The bond he had formed with the people, the joy in the work, the shared love of classical music, the sense of belonging — these had woven themselves into the fabric of his soul in a way that age had not loosened.
In the last years of his life, his health declined. A renal tumour required a nephrectomy. In January 2026, he developed bilateral femoral artery occlusions. Sepsis and multiorgan failure followed. His family, not wishing to prolong his suffering, asked the intensivists to withhold further life support. He died at Viveka Hospital in Nagpur on January 18, 2026 — a fortnight before what would have been his eighty-ninth birthday.
He had wanted to be a Hindustani Classical vocalist. He became a pharmacologist who taught like a performer, organised the cultural life of an institution, shouldered the arthi in the rain, and made his home a place where the music never stopped. He did not choose between the two lives. He lived both.
| 1937 | Born, 4 February, Nagpur — Khapre Wada, Pataleshwar Road |
| 1955 | Entered Government Medical College, Nagpur |
| 1967 | Joined GMC Nagpur as Lecturer in Pharmacology, July |
| 1971 | Arrived MGIMS, 21 February — Reader in Pharmacology |
| 1977 | Promoted Professor of Pharmacology |
| 1980 | Resumed MGIMS professorship, April — after brief return to GMC Nagpur |
| 1982 | Performed in Marathi drama “Pankh Labhale Aaj Suranna” — Dhanwate Rang Mandir, Nagpur |
| 1987 | Left MGIMS, August — after sixteen years |
| 1988 | Took voluntary retirement from GMC Aurangabad, June |
| 1988 | Mentored Dr. S. John Premendran through PhD thesis on calcium antagonists |
| 1988 | Taught at Dr. Punjabrao Deshmukh Memorial Medical College, Amravati — three years |
| 1991 | Taught at Jawaharlal Nehru Medical College, Sawangi — until 2005 |
| 2026 | Died, 18 January, Viveka Hospital, Nagpur — aged eighty-eight |
A comparative study of pharmacological actions of calcium, strontium barium and their interactions with calcium antagonists on different muscle tissues
Dr. S. John Premendran
MSc Pharmacology: Christian Medical College (CMC), Vellore
The train from Chennai had been running for twenty-two hours when it pulled into Wardha East on the morning of February 28, 1975. The platform was nearly empty. John Premendran, twenty-seven years old, a freshly minted MSc from CMC Vellore, stepped down with a single bag and looked around. A cycle rickshaw was the only transport on offer. He climbed in and asked for the medical college.
The road ahead was flat and featureless — no shops, no landmarks, no reassuring sign that a college lay anywhere in this landscape. By his own later admission, a dark thought crossed his mind: what if the rickshaw puller simply disappeared with his luggage? He said nothing, held his bag closer, and watched the road unspool into the distance.
The man delivered him safely to the college gate, helped carry his bag to the Physiology department, and refused to make a fuss about it. John gave him five rupees — a sum that felt both inadequate and right — and stood at the entrance of what would become his home for the next thirty-four years.
John Samuel Premendran was born on September 5, 1947, in Vellore, Tamil Nadu, the son of Dr. M. James Sudarsanam — a historian, a teacher, and the Vice Principal of Voorhees College. It was a household in which books mattered and precision was expected. Young John grew up wanting to be a doctor.
He came close. He sat the entrance examination for CMC Vellore's MBBS programme and missed the cutoff by a margin narrow enough to sting. What followed was not defeat but redirection. He completed a BSc at Voorhees College — botany, zoology, chemistry — and then returned to CMC, this time for an MSc in Pharmacology. He was, it turned out, exceptionally good at it.
After a brief stint as a lecturer at CMC, he began looking for what came next. A classmate, Mrs. Nambiar, who had taken a position in the Physiology department at a new medical college in a village called Sevagram, mentioned that Pharmacology had a vacancy. John applied. An interview was called. He boarded the GT Express north, and arrived — as described — at an almost empty station on the edge of Vidarbha's cotton country.
The village life felt, unexpectedly, familiar. He had grown up near Katpadi, a small town outside Vellore, and Sevagram's pace did not alarm him. That Marathi was unknown to him mattered less than the fact that written Hindi was not. He settled.
On March 1, 1975, John Premendran walked into the Pharmacology department for the first time as a member of staff. His salary was ₹530, paid in cash. He was housed in the boys' hostel. His teaching tools were a blackboard and chalk.
He never asked for more.
For thirty-four years, through every wave of educational technology — overhead projectors, slide carousels, the eventual arrival of PowerPoint — Premendran taught pharmacology with chalk. His lectures on the autonomic nervous system, on chemotherapy, on central nervous system pharmacology were constructed, line by line, on a blackboard, in handwriting his students recognised as his own form of calligraphy. The same precision appeared in everything he wrote outside the classroom: his letters, his research notes, his correspondence with students after they had graduated and moved on. He wrote it all in green ink.
The green ink was not an affectation. It was simply his — a marker of a sensibility that valued the particular over the generic, the handmade over the mass-produced. Students who received letters from him decades later knew, before they opened the envelope, who had written it.
His other signature contribution was practical. Premendran had trained in experimental pharmacology at CMC Vellore, where dog dissection was conducted with rigour. He brought that expertise to MGIMS and passed it on. A department attendant named Wankhede built a piston-and-lever apparatus to measure ureteric peristalsis in dogs, and the graphs it produced were exceptional. Research followed: plant extracts and snake venom, the behaviour of calcium and strontium and barium on muscle tissue. In 1989, this work became a PhD from Nagpur University.
When the Prevention of Cruelty to Animals Act ended animal experimentation in 1998, Premendran did not mourn the old methods for long. His first MD student, Dr. V. Bonde, was assigned a project on community-acquired pneumonia instead — a pivot made possible by his relationships across departments, with colleagues in Medicine and Paediatrics who welcomed a pharmacologist's student into their wards without hesitation.
"His discipline and punctuality were clear in everything he did," Bonde recalled. "And he made sure others followed his example."
There was something Sevagram did to people who stayed long enough. The absence of distraction — no cinema, no metropolitan restlessness — turned inward energy outward, toward students, toward music, toward community. Premendran felt this.
Every December, he spent a month training nursing and medical students in Christmas carols. On the evening of the 24th, the group would walk to Dr. Sushila Nayar's residence and sing for her. Dr. Nayar made a point of requesting him personally: "John, when will you bring your carol team?" After the singing, there were cakes and biscuits, and the kind of memory that a life accumulates without knowing it is accumulating anything at all.
On other evenings, he played the violin. He had begun learning Carnatic classical violin at twelve, under a teacher who charged ten rupees a month for lessons in both violin and harmonium. At MGIMS, he found a musical companion in Dr. Vivek Pophali, a faculty member in Medicine who played guitar. They performed together at college concerts — Pophali on guitar, Premendran on violin — while colleagues Dr. R.K. Gupta and Dr. M.D. Khapre contributed their voices.
He guided eleven MD students across three decades. One of the stranger dynamics of his career was that his first postgraduate student, Dr. V. Bonde, was fifty years old when he enrolled — five years older than his guide. The potential awkwardness was absorbed without comment. Premendran's view of teaching had no room for hierarchy based on age. Learning was what mattered; the rest was arrangement.
Premendran was, by temperament, an introvert. He did not fill rooms with noise. Students who knew him only from the corridor might have found him reserved, perhaps even distant. Those who knew him longer discovered the warmth underneath the quietness — a man of strong religious conviction, soft speech, and a precise ethical sense that he applied as rigorously to small decisions as to large ones.
Dr. Swanand Pathak, from the 1993 MBBS batch, remembered one image above all others: Premendran arriving at the railway station to receive him when he came to Sevagram for the first time. "He was not only a remarkable mentor," Pathak said, "but a man of great stature." The gesture — a senior professor, turning up at a station to meet a student he had not yet taught — said something that no formal tribute could have said more clearly.
His wife Sheila, who came from Chennai and initially found village life an adjustment, became a fixture of Kasturba Vidya Mandir, where she taught mathematics and English to the children of MGIMS faculty — some of whom later became doctors themselves. She eventually became the school's principal. On evenings and weekends, she tutored students at home. Decades later, her students — and their parents — still spoke of her with specific, undiminished gratitude.
John Premendran retired from MGIMS on August 18, 2009, after thirty-four years. He was not done teaching: he joined Mamata Medical College in Khammam, spent eight more years in a Pharmacology department, and served briefly as its head.
His son Ben, admitted to MGIMS in 1995, completed both his MBBS and his MD in Anaesthesiology at the same institution where his father had taught. In 2020, Ben moved to Abu Dhabi, and in 2022 his parents followed.
Sheila Premendran died on January 31, 2024, at their home in Sevagram, after a long illness. She had returned to the place that had, against early expectations, become hers.
John Premendran now lives with his son in Abu Dhabi. He is in his late seventies. Whether he still plays the violin is not recorded. Whether he still writes in green ink, one suspects, is not really in question.
| 1947 | Born, 5 September, Vellore, Tamil Nadu |
| 1947 | Father Dr. M. James Sudarsanam — historian, Vice Principal, Voorhees College, Vellore |
| 1967 | Completed BSc — Botany, Zoology, Chemistry — Voorhees College |
| 1972 | Completed MSc Pharmacology, CMC Vellore |
| 1975 | Arrived Wardha East station, 28 February — by cycle rickshaw to MGIMS |
| 1975 | Joined Pharmacology department, 1 March — salary ₹530 |
| 1989 | Awarded PhD, Nagpur University — research on calcium, strontium, barium on muscle tissue |
| 1998 | Pivoted from animal experimentation to clinical pharmacology research — Prevention of Cruelty to Animals Act |
| 2009 | Retired from MGIMS, 18 August — after thirty-four years |
| 2009 | Joined Mamata Medical College, Khammam — eight more years teaching pharmacology |
| 2022 | Moved to Abu Dhabi with son Ben |
| 2024 | Wife Sheila died, 31 January — at their Sevagram home, after long illness |
Effect of calcium, strontium barium on different types of muscle- tissue their interaction with calcium antagonist
Effect of calcium,strontium,barium on different type of mammalian muscle tissue their interaction with diltiazem
Pharmacological basis of use of certain activities of Ricinus communis, linn solanum, surattense burm extracts
Use of antimicrobials for the treatment of pneumonia in medicine and pediatric indoor patients
Study of the pharmacological action of the extracts of certain phanerogam plants.
A pattern of drug utilization in a village in central India : a prospective study
Effect of hydroalcoholic leaf extract of Kalanchoe pinnata pers in ethylene glycol induced nephrolithiasis, paracetamol induced hepatotoxicity and the peristalsis of goat ureter
Drug utilization study of selected population of antenatal mothers in rural India
Study of antimalarial potential of Calotropis gigantea extracts in mice
Anti Snake Venom Activity of Plant andrographis Peniculata
Dr. B. K. Mahajan
Diploma in Public Health (DPH): United Kingdom (1962)
Medical & Hospital Administration: London School of Hygiene and Tropical Medicine
On the morning of July 17, 1973, a train from Delhi pulled into Wardha station carrying a fifty-eight-year-old doctor with a neatly packed suitcase and, by all accounts, no intention of slowing down. Dr. B.K. Mahajan had just finished fourteen years as head of the Department of Preventive and Social Medicine at M.P. Shah Medical College in Jamnagar. He had also spent thirteen years before that in the Bombay State Health Services — as epidemic medical officer, plague control officer, district health officer, deputy director of public health — battling the diseases that moved through poor populations like water through cracked ground. He could, at fifty-eight, have stopped.
Instead, he had accepted Dr. Sushila Nayar's invitation to come to Sevagram and build a department. He stepped onto the dusty platform at Wardha and hired a conveyance to the campus. What awaited him was a medical college that had been running for four years, a community medicine department in early formation, and a founding director who had already decided that her students would learn medicine from villages, not only from wards.
Mahajan had been preparing for this, without knowing it, his entire career.
He was born on July 15, 1915, in Chuhar Munda, in the Sialkot district of what was then West Punjab — a landscape that no longer exists as he knew it, erased by Partition thirty-two years before he arrived in Maharashtra. His MBBS from Punjab in 1940 placed him fifth in the university. Prizes and scholarships followed.
His formation was unusually wide. Thirteen years in the Bombay State Health Services gave him the epidemiologist's habit of mind — the capacity to read a district rather than a patient, to see a disease not as an individual misfortune but as a consequence of water, housing, nutrition, and neglect. In 1961 and 1962, under the Colombo Plan, he trained in preventive and social medicine in the United Kingdom, then studied medical and hospital administration at the London School of Hygiene and Tropical Medicine. By the time he arrived in Jamnagar for his first professorship, he had accumulated the kind of experience that no examination could confer.
The twenty-two research papers he published at Jamnagar covered filariasis, leprosy, smallpox, nutrition, water supply, and primary healthcare — a map of the public health problems that rural India faced and that urban medicine, trained in tertiary hospitals, was not designed to address. When Nayar was looking for someone to run community medicine at MGIMS, Mahajan's record made him the obvious choice. The question was whether he would come.
He came.
The programme that Mahajan inherited and built was, by the standards of Indian medical education in the 1970s, radical. First-year students — fresh from their school-leaving examinations, barely adults — were sent into villages. Not for a day trip. For ten to twelve days at a time, sleeping on charpoys, eating jowar bhakri, drawing water from wells, living as the people they were being trained to serve actually lived.
Dr. Ashok Mehendale, from the 1973 batch, remembered the geography of those early camps: Sevagram and Warud for the first batch in 1969, then Panar, Kharangana, Kutki, Karanji Bhoge, Barbadi, Mhasala in successive years, each village receiving a batch of students who arrived with their medical bags and left, a fortnight later, with something that no pharmacology lecture could provide: an unambiguous understanding of what poverty looked like from the inside.
"It was a life they had never known — simple yet harsh. And it changed them forever."
The National Medical Commission made comparable programmes mandatory for Indian medical colleges in 2023. MGIMS had been running them for more than fifty years.
The General Outpatient Department was the other instrument. Conceived with Nayar and executed by Mahajan, the GOPD was designed to function as a primary health centre nested inside a teaching hospital — a place where students saw the common ailments of a rural population before they were routed upward to specialties, where antenatal care sat alongside anti-rabies vaccines and tuberculosis follow-up, where triage was not a bureaucratic function but a clinical education. Students who passed through the GOPD early in their training understood, before they ever entered a specialty ward, that most of what a doctor encounters in practice is neither dramatic nor specialised.
In the classroom, his method was Socratic and unforgiving of passivity. "Tell me," he asked a student in the middle of a lecture, "if you were to start a malaria control programme in this very village, where would you begin?" There was no rote answer. He wanted them to think like practitioners, not like examination candidates. Dr. V.K. Gupta, from the 1976 batch, remembered that Mahajan kept his lectures anchored to the epidemiological triad of agent, host, and environment — and trusted students to read the rest. "The rest," he would say, "you can easily find in your textbooks." What they could not find in textbooks was the thing he gave them in the field.
He went to the villages himself. He walked when he had to, mapping disease patterns, running health camps, taking notes that his students remembered long afterward — not for their length but for what they noticed. He saw the subtle shifts in disease trends, the gaps between what government reports recorded and what was actually happening in a household. His students learned, by watching him, that the most important skill in public health was attention.
In June 1977, Nagpur University recognised MGIMS for postgraduate studies in Community Medicine — the first such recognition in the region. The first four MD students were Dr. Anand Tatte, Dr. G. Subrahmanyam, Dr. M.C. Mathew, and Dr. Luis A.V. Barreto. Nayar and Mahajan guided them together.
Sevagram was unlike anywhere Mahajan had worked before. The pace was slow. The campus was small. He lived at 14 MLK Colony with his wife Aruna, and the house became, in the way that certain houses on small campuses do, a place people gravitated toward — a space where ideas were exchanged and the warmth of the couple inside made the address familiar to everyone on campus.
His closest companion at MGIMS was Dr. M.L. Sharma of the Pharmacology department. Their friendship was a feature of campus life — two senior men of a certain seriousness, and between them an ease and humour that those around them found reassuring. Mahajan's Punjabi — pure, lilting, carrying the cadences of a Punjab he had left decades before — would emerge in moments of pleasure or teasing. He had a fondness for catching medical students off-guard, leaving them both confused and smiling.
His colleagues found in him a particular quality of fairness. He listened to residents rather than merely instructing them. He sought the views of nurses. He treated the laboratory technicians with a patience and precision that made them trust him. Even the administration softened around him, because he never bullied and never raised his voice, and yet, somehow, always got what he needed.
On January 24, 1966 — the day Indira Gandhi was sworn in as Prime Minister — an Air India Boeing 707 crashed near Mont Blanc. Among the 117 people killed were the physicist Homi Bhabha and Lalit Mahajan, B.K. Mahajan's twenty-two-year-old son, who was on his way to the United States to study engineering.
Mahajan did not speak of this often. Those who knew him in Sevagram knew it as background — a sorrow that had been carried for years before he arrived, that had not broken him but had altered him in ways that a man of his reticence would not have named. To keep his son's memory present in a form that had meaning, he established the Lalit Mahajan Award, given each year to the best student in Preventive and Social Medicine. A father's loss, redirected toward the subject to which he had given his working life.
He left Sevagram in August 1982, after nine years. Col. S.K. Chatterjee left the same month. Two founding figures gone simultaneously, a gap that the department would take years to close.
He went to AIIMS, New Delhi, as a senior consultant for the Integrated Child Development Services, working on child health policy at a national level until 1988, then advised the Delhi Council of Child Welfare until 1997. The work continued to move outward, as it always had with him — from the individual patient to the community, from the community to the district, from the district to the country.
What he left at MGIMS was structural. The village immersion programme, the GOPD as a model of integrated primary care, the postgraduate curriculum in community medicine, the cohort of doctors who understood — in their bodies as well as their minds, because they had slept on charpoys and eaten jowar bhakri — that public health was not a specialty practised in hospitals. It was a way of seeing that either developed early or not at all.
Dr. Suneela Garg, from the 1974 batch, remembered his rare capacity to bring together people who did not naturally cooperate — bureaucrats, policymakers, villagers, students — and hold them in the same room long enough to accomplish something. He visited the villages himself, she said, and addressed problems directly rather than delegating them downward.
The Lalit Mahajan Award is given every year. The villages are still visited. The GOPD still runs. The man who sent doctors to sleep on charpoys in Vidarbha's villages is gone, but the habit he instilled — of looking past the patient to the conditions that produced the patient — is still, fifty years later, part of what MGIMS does.
| 1915 | Born, 15 July, Chuhar Munda, Sialkot district, West Punjab |
| 1940 | Completed MBBS, Punjab — fifth in university |
| 1940 | Joined Bombay State Health Services — epidemic medical officer, plague control officer, district health officer, deputy director of public health |
| 1953 | Joined M.P. Shah Medical College, Jamnagar — Professor & Head of Preventive and Social Medicine |
| 1961 | Training in Preventive and Social Medicine, United Kingdom — under Colombo Plan |
| 1962 | Medical and Hospital Administration, London School of Hygiene and Tropical Medicine |
| 1966 | Son Lalit Mahajan killed — Air India Boeing 707 crash near Mont Blanc, 24 January — 117 killed including Homi Bhabha |
| 1973 | Arrived MGIMS, 17 July — aged fifty-eight |
| 1977 | Nagpur University recognised MGIMS for postgraduate studies in Community Medicine, June — first in region |
| 1982 | Left MGIMS, August — joined AIIMS New Delhi as senior consultant, ICDS |
| 1988 | Advised Delhi Council of Child Welfare — until 1997 |
Assessment of Nutritional Status of Preschool children in a rural community around sewagram with special reference to impact of state supplementary feed program
A Study of Perinatal Mortality
Anemia in school children in the age group of 6-14 years
Dr. Mohan Digambar Gupte
Diploma in Public Health (1973)
MD Preventive and Social Medicine, BJ Medical College Pune (1975)

In February 2018, Dr. Mohan Gupte walked back through the gates of MGIMS for the first time in thirty-five years. The campus had swelled—new architecture casting longer shadows, a sprawling hospital, corridors thick with a new generation of students—but he still knew its bones. These were the rooms where he had taught; these were the offices where he had argued over leprosy data before leaving in 1983. That departure had launched a career spanning the Indian Council of Medical Research (ICMR), the World Health Organization (WHO), and the chair of the first WHO Technical Advisory Group for Leprosy Elimination.
He had returned to receive the International Gandhi Award for Leprosy from the Vice President of India. The honor had been instituted by the Gandhi Memorial Leprosy Foundation in Wardha, the very organization where he had labored in the 1970s before finding his academic home at MGIMS. To stand on this specific soil, receiving an award for work that had pivoted exactly here, possessed the kind of quiet symmetry an epidemiologist might describe as statistically improbable.
He accepted the honor, quietly redirected the entirety of the prize money to mental health research, elderly services, and a struggling student, and then he went home.
The Sanctuary in Pune
Born in Pune on February 10, 1948, his earliest education was not in a classroom, but in his own living room. His father, Digambar, was a headmaster who viewed education as the only honest lever to lift the impoverished. His mother, Venutai, took that philosophy a step further. She brought struggling students and ostracized women directly into their home, offering them shelter before guiding them toward Annasaheb Karve's Hingne Institute. For the Guptes, a house was never merely a residence; it was a sanctuary.
In 1966, a tragic fall at school claimed Venutai’s life. Mohan was eighteen. Already a brilliant scholar—holding a national scholarship and ranking in the top thirty of the Maharashtra SSC examinations—the sudden grief reoriented his compass. Rather than chasing the lucrative avenues his academic brilliance afforded, he sought out the margins. He harbored no interest in wealth; he possessed a singular need to be fundamentally useful.
This drive led him to B.J. Medical College in Pune, culminating in an MBBS in 1970, followed by a Diploma in Public Health and an MD in Preventive and Social Medicine. Two mentors profoundly shaped his hands and his mind. Dr. N.S. Deodhar, a surgeon retrained at Harvard, taught him to view populations, rather than just individuals, as his patients—treating statistical evidence as a vital clinical instrument. Dr. P.V. Sathe taught him the delicate balance of holding clinical medicine in one hand and community health in the other. Under Sathe’s guidance, Gupte investigated ergot poisoning—a toxic grain fungus devastating the poor. Mastering the intricate machinery of high-performance liquid chromatography, he forged habits of meticulous precision that would anchor him for a lifetime.
The Inconvenient Observation
Before he arrived in Sevagram, there was the smallpox campaign, and before that, the quiet, heavy wards of leprosy hospitals. In 1976, Dr. Deodhar sent him to interview for the Deputy Director post at the Gandhi Memorial Leprosy Foundation. The panel was formidable, featuring Baba Amte, R.R. Diwakar, and Devendra Kumar. Diwakar looked at the young doctor and asked a piercing question: Had he ever seen poverty up close?
Gupte answered without academic abstraction. He spoke with the heavy, unadorned truth of what his own eyes had witnessed. He was hired immediately.
Rising to Acting Director, Gupte began to notice fractures in the established medical gospel. Textbooks unequivocally stated that regular dapsone therapy prevented deformities in leprosy. Yet, as Gupte tracked his clinical records, the data refused to comply. He watched patients faithfully take their medication, only to see their deformities advance. He published his findings. The medical establishment met him with harsh skepticism. But he stood firmly beside his data, willing to say in print what others whispered, until time and science proved him right.
When internal politics at the Foundation became a barrier to his work, he walked directly into Dr. Sushila Nayar’s office at MGIMS in November 1979. He explained his reality. Recognizing his rare caliber, she offered him a readership in Preventive and Social Medicine before he left the room. By December, the thirty-one-year-old was living in Sevagram.
The Architecture of Illness
His three-and-a-half years at MGIMS were a whirlwind of quiet revolution. Promoted to Professor and Head, he mentored postgraduates, treated patients, and even taught statistics to the faculty—with Dr. Nayar herself sitting in the audience, absorbing his lectures.
It was here that his unparalleled observational skills flourished. When an unusual number of nursing students from Kerala began falling ill with tuberculosis, he did not simply treat the cases as unfortunate statistics. He looked at the architecture of the Birla-donated building—Community Medicine occupying the floor directly above the Medicine wards—and traced the invisible paths of contagion that others had walked past without a second glance.
He was a man deeply embedded in the realities of his patients. He examined them with bare hands and, in a detail his own biography records without a hint of self-pity, he personally contracted leprosy during this period. Treated by Dr. K.V. Desikan, he made a full recovery, his empathy for the afflicted now etched into his own immune system.
Building the National Stage
In June 1983, with Dr. Nayar’s blessing, he departed for Chennai to lead a massive ICMR leprosy vaccine trial. MGIMS had been the vital connective tissue between his early fieldwork and his future on the global stage.
What followed was a masterclass in institution-building. He led tuberculosis epidemiology at the Tuberculosis Research Centre and oversaw biostatistical monitoring across India. In 1999, he became the Director of the National Institute of Epidemiology, building India's capacity for outbreak investigation from the ground up. He helped shape the multidrug therapy (MDT) program that revolutionized global leprosy treatment, established India's first Field Epidemiology Training Centre, and spent a decade lobbying to create the ICMR One Health Institute in Nagpur.
Today, the young reader who arrived in Sevagram with a resignation letter in his pocket is an elder statesman of global public health. The dapsone observation that was once dismissed is now standard medical doctrine. He began in a headmaster's home where the struggling were welcomed off the street, and he spent his entire life doing a grander version of the exact same thing: finding the problems the world refused to name, and naming them anyway.
| 1948 | Born, 10 February, Pune — father Digambar Gupte, headmaster; mother Venutai, teacher; house always open to struggling students |
| 1966 | Mother Venutai died — fell at her school; Mohan was eighteen; national scholarship, top thirty in Maharashtra SSC |
| 1970 | Completed MBBS, BJ Medical College, Pune |
| 1973 | Diploma in Public Health |
| 1975 | MD Preventive and Social Medicine — thesis on ergot poisoning under Dr. P.V. Sathe; mastered HPLC and electrophoresis |
| 1976 | Appointed Deputy Director, Gandhi Memorial Leprosy Foundation, Wardha — interview panel included Baba Amte and R.R. Diwakar |
| 1978 | Published findings on dapsone and deformity progression — contradicted established view; met with scepticism; eventually proved right |
| 1979 | Went directly to Dr. Nayar — offered readership on the spot; joined MGIMS December as Reader, Community Medicine |
| 1981 | Promoted Professor and Head, Community Medicine |
| 1982 | Contracted leprosy while at MGIMS — treated by Dr. K.V. Desikan; full recovery |
| 1983 | Left MGIMS, June — ICMR leprosy vaccine trial, Chennai; WHO interest |
| 1999 | Director, National Institute of Epidemiology, Chennai, and ICMR School of Public Health |
| 2000s | Chaired first WHO Technical Advisory Group for Leprosy Elimination; established India’s first Field Epidemiology Training Centre |
| 2018 | Returned to MGIMS — received International Gandhi Award for Leprosy from Vice President of India; donated entire prize money |
Observation on clinical response of leprosy patients to multidrug regimen operational aspect in Wardha dist.
Monitoring of severe malnourished children in ICDS block-Dharani
Lt. Col. S.K. Chatterjee
Diploma in Public Health Administration: All India Institute of Hygiene, Kolkata (1949)
MD Preventive & Social Medicine: Armed Forces Medical College (AFMC), Pune (1975)
Professor & Head of Community Medicine · Six Years at Sevagram · The Only Man in Sevagram
When Lt. Col. Sudhir Kumar Chatterjee retired from the Indian Army Medical Corps on February 29, 1976, after twenty-five years of service, five medical colleges offered him a position. He had just completed his MD in Preventive and Social Medicine at the Armed Forces Medical College in Pune, at the age of fifty-four. He was experienced, qualified, and entirely employable. Four of those colleges were in cities. The fifth was MGIMS, Sevagram — a rural campus on the edge of a cotton-farming village in Vidarbha, built on Gandhian principles, run by a woman whom he would later describe, without irony, as the only man in Sevagram.
He chose Sevagram. He arrived on March 9, 1976. His monthly salary was ₹1,531 — the same as his army pay. He did not consider this a sacrifice worth mentioning. What mattered, as those who knew him understood, was not the salary but the work. And the work at Sevagram, he had decided, was the kind that mattered.
He was born on February 3, 1921, in Baidya Para, Jamalpur, Bihar — the fifth of nine children in a household shaped by the rhythms of the Indian Railways, where his father worked. The family ethos was not complicated: discipline, education, duty. He attended Hari Sabha Bengali Medium School, then Eastern Railway Boys' High School, then Haji Mohsin College in Hooghly. He entered Calcutta National Medical College in 1939 and graduated in 1945.
The army followed. He joined the Indian Army Medical Corps in 1949, the same year he completed his Diploma in Public Health Administration at the All India Institute of Hygiene. Field postings took him to Siliguri, Srinagar, Gaya, and across the subcontinent — the life of a military doctor in newly independent India, making quick decisions in difficult places, learning that medicine practised under constraint was still medicine, and often the most consequential kind.
His daughter Gopa, who was nine years old when India went to war with Pakistan, remembered what those years felt like from the other side of the uniform: "How dreadful were the days when war broke out with Pakistan. Communication was scarce, and the uncertainty was agonizing. We would wait anxiously, hearts heavy with worry, longing for any news of his safety."
He survived the wars. He moved through postings in Agra, Shillong, Delhi, Bombay, and finally Pune, where his role shifted from field medicine to teaching. At the Armed Forces Medical College, he spent four years as Reader and then Associate Professor in Preventive and Social Medicine. He was fifty-three when he enrolled for his MD. He obtained it in 1975. Then the army released him, and Sevagram called.
He arrived at MGIMS as an Associate Professor and was promoted to Professor in November 1980. He headed the Department of Community Medicine through years in which the department was finding its shape — absorbing the legacy of Dr. B.K. Mahajan, who had left the previous month after building the village immersion programme and the GOPD from nothing, and pressing forward into the postgraduate training in community medicine that Mahajan had begun.
Colleagues remembered two things about him immediately. The first was his bearing. A quarter-century in the army had produced a particular quality of presence — erect, precise, economical with words, the kind of man who said "meet me in the department office" when he had something serious to discuss, and who meant it. His instructions were crisp. His expectations were clear.
The second thing they remembered was the hat. In Sevagram, where the Gandhian ethos meant khadi was standard dress for those who took the institution's founding principles seriously, Chatterjee wore khadi — and paired it with a British-style hat. The combination was entirely his own: the military man who had absorbed the village, the retired officer who had chosen rural service, the Bengali from Bihar who had come to Maharashtra and put on its cotton while keeping something of his own formation visible on his head.
He had a particular phrase he returned to when describing Dr. Sushila Nayar. "The only man in Sevagram is Dr. Sushila Nayar," he would tell colleagues — not as a comment on gender, he would explain, but as the most precise description of authority he could offer. Then he would tell the story. In April 1966, when Prime Minister Indira Gandhi was preparing to visit the United States, her ambassador B.K. Nehru was asked how President Johnson should address her. She answered without hesitation: "You can tell him that my cabinet ministers call me 'Sir.'" Chatterjee told this story to explain Nayar. The parallel was clear to anyone who had encountered both women.
His daughter Gopa was in his classroom. She had secured admission to MGIMS in the same year he joined — 1976 — so that father and daughter arrived on campus together, one to teach, one to learn. His son Rajib graduated three years later, in 1979. The campus was, for those years, also home.
The transition from military to civilian institutional life is rarely seamless, and Sevagram's particular character — its Gandhian quietness, its deliberate simplicity, its ethos of service that asked for no salute — offered the army's structures and habits nowhere to rest. Chatterjee absorbed this without apparent difficulty. He wore the khadi. He attended the department. He did the work.
What Sevagram gave him in return was duration — time in one place, with one community, long enough to see the students he had taught go on to practice and teach themselves. Dr. Ashok Mehendale, who graduated from MGIMS in 1976 and would eventually head the same department three decades later, was among those who passed through his classroom. The continuity mattered. The army had moved him constantly; Sevagram held him still long enough to accumulate something more than competence.
He officially retired in February 1981, then continued on contract until July 1982. When he finally left, the department he and Mahajan had built was a functioning entity — a postgraduate programme, a community medicine curriculum grounded in fieldwork rather than lecture halls, and a generation of doctors who had spent ten days sleeping on charpoys in Vidarbha villages and understood, in their bodies, what the epidemiological textbooks meant.
He did not stop. In 1983 he joined Charutar Arogya Mandal — now Pramukhswami Medical College. In January 1986 he moved to Pravara Rural Medical College in Loni, teaching until December 1988. He was sixty-seven. The Royal Institute of Health and Hygiene, London, made him a Fellow in 1986. He was deputed to Nairobi and Tanzania under the Aga Khan Project. The career continued to expand outward, as it had throughout his life.
In his final years in Pune, he led a community tuberculosis surveillance team. On Sundays — not weekdays, Sundays — he conducted home visits, screening patients, counselling them, checking that they were taking their medication. He was, by that point, well into his eighties. The habit of going to where the patient was, rather than waiting for the patient to come, had been built at MGIMS and had never left him.
He lost his wife Gita in May 2017, after sixty-six years of marriage. The family had begun planning a centenary celebration for his hundredth birthday — February 3, 2021, the same date on which, a century earlier, he had been born in a railway town in Bihar. He died in November 2020, three months before the party.
There is something fitting, though not consoling, in the near-miss. He had spent his life just ahead of schedule — obtaining his MD at fifty-four, joining a new institution at fifty-five, still doing home visits in his eighties. That the hundredth birthday arrived without him is the kind of irony that a man of his precision would have noted, filed, and declined to make a fuss about.
His two children both graduated from the campus where he taught. His students went on to build the discipline he had helped establish. The khadi and the British hat are gone. The department remains.
| 1921 | Born, 3 February, Baidya Para, Jamalpur, Bihar |
| 1939 | Entered Calcutta National Medical College |
| 1945 | Completed MBBS |
| 1949 | Joined Indian Army Medical Corps · completed Diploma in Public Health Administration, All India Institute of Hygiene |
| 1949 | Field postings — Siliguri, Srinagar, Gaya, Agra, Shillong, Delhi, Bombay, Pune |
| 1954 | Enrolled MD Preventive and Social Medicine, Armed Forces Medical College, Pune — aged 53 |
| 1975 | Completed MD — aged fifty-four |
| 1976 | Retired from Army Medical Corps, 29 February — five colleges offered positions |
| 1976 | Arrived MGIMS, 9 March — daughter Gopa admitted same year |
| 1979 | Son Rajib graduated from MGIMS |
| 1980 | Promoted Professor, November |
| 1981 | Officially retired, February — continued on contract |
| 1982 | Left MGIMS, July |
| 1983 | Joined Charutar Arogya Mandal, Pramukhswami Medical College |
| 1986 | Joined Pravara Rural Medical College, Loni — Fellow, Royal Institute of Health and Hygiene, London |
| 1986 | Deputed to Nairobi and Tanzania — Aga Khan Project |
| 2017 | Wife Gita died, May — after sixty-six years of marriage |
| 2020 | Died, 3 November, Pune — three months before his planned centenary celebration |
Dr. K.K. Ghuliani
MD Preventive and Social Medicine, AIIMS Delhi (1967)

The Scrabble Game
On most evenings in Vivekanand Colony, if you knocked on the Ghulianis' door at the wrong moment, you would find a Scrabble board mid-game and two people quietly annoyed at the interruption—who would wave you warmly inside anyway.
By day, Dr. K.K. Ghuliani moved through the Department of Community Medicine with the unhurried precision of a man who had spent decades learning that urgency and panic were not the same thing. But in those evenings, he transformed into an animated storyteller and a fierce cricket enthusiast. His laughter, when it finally broke, was rich and entirely unguarded. Mrs. Mohini Ghuliani would place something hot on the table, effortlessly making the guest feel that their intrusion had, in fact, been the point of the evening all along.
This was the Ghuliani the department only saw obliquely. In the classroom and the office, he was someone else entirely: short in stature, invariably dressed in crisp khadi, economical with his words, and possessed of a deep, steady calm that no one dared confuse with weakness.
Mianwali, and the Border Crossed
He was born on September 16, 1926, in Mianwali, in the North-West Punjab that is now Pakistan. When Partition fractured the subcontinent in 1947, it took his geography from him. He crossed the border carrying only what he could hold, eventually securing his MBBS at Punjab University in 1950. At the time, Government Medical College in Amritsar—the single functioning medical college in northern India—was buckling under the overflow of a newly divided nation's desperate need for doctors.
He joined the Army Medical Corps in 1951, serving as a Regimental Medical Officer through postings in Amritsar, Jubbulpore, Kirkee, and Jhansi. The military forged the architecture of his professional life. It instilled a permanent belief that rigorous preparation was the only reliable shield against chaos; that discipline was not a personality trait, but a clinical tool; and that a doctor who lost his composure under pressure was a doctor of limited use.
He chased the advancing frontier of science throughout his career, studying hygiene, preventive medicine, malariology, and statistical quality control whenever the army permitted, eventually earning his MD in Preventive and Social Medicine from AIIMS in 1967.
By the early 1980s, the Community Medicine department at MGIMS was in a precarious state. Dr. Mohan Gupte had left for Chennai, leaving Dr. S. Nagesh as a solitary lecturer carrying a weight no single academic should bear. A department of that size desperately needed a head. Dr. Ghuliani—recently retired from the Armed Forces Medical College in Pune and fresh from a WHO malaria evaluation team in northeastern India—was available.
He arrived on October 28, 1983, at a salary of Rs. 2,520 a month. He took the helm of the department and made absolutely no fuss about the condition in which he found it.
The Weight of Quiet Authority
The Department of Community Medicine had been built by men of considerable, affectionate noise. Dr. B.K. Mahajan was a classic Punjabi presence—broad, warm, and booming. Lt. Col. Chatterjee commanded rooms with the clipped, polished register of colonial-era military precision. Dr. Mohan Gupte was effortlessly magnetic, accumulating friends simply by existing.
Dr. Ghuliani was none of these things, nor did he try to be. His authority was never a performance. It resided entirely in his absolute consistency. What you saw on his first day was exactly what you saw on his last. His standards did not fluctuate with his mood, and he never raised his voice because he simply never needed to. Students and junior staff calibrated themselves to his quiet frequency quickly. They learned that his silence was not coldness; it was a profound form of respect. He assumed your competence until you proved otherwise, and he withheld both judgment and praise until they had been thoroughly earned.
Under his eight-year watch, his MD students systematically mapped the public health geography of Wardha district. They investigated maternal health, hypertension in business communities, occupational hazards in ginning mills, and trachoma in slums. This was not an eclectic list of academic curiosities; it was a deliberate, utilitarian index of the exact afflictions plaguing Vidarbha, designed to make the department useful to the people rather than just productive for journals.
He spoke Punjabi, Pashto, Urdu, and Hindi fluently. Marathi, however, remained beyond his grasp. He never pretended otherwise. This linguistic gap was the quiet hallmark of his generation—men who had crossed borders they had not chosen to cross, who rebuilt their lives in places that were not quite home, and who dutifully made those places home anyway.
The Letters from Pune
While Dr. Ghuliani anchored the department, Mohini Ghuliani anchored the campus. She played the sitar, she knitted, and she taught flower arrangement to the women of Sevagram with a patience that turned her into a neighborhood institution. Their home became a place of reliable, magnetic warmth—the kind of house people gravitated toward without planning to, and always left much later than they intended.
In July 1991, he handed the department over to Dr. G.V.S. Murthy and moved to Pune to support his daughter through her Paediatrics MD. He worked as a WHO consultant for the National Leprosy Eradication Programme, quietly following the institutional footsteps of Dr. Mohan Gupte once again.
After leaving Sevagram, he never returned to the campus. By his own quiet admission, he was too introverted for the managed emotions of a grand reunion or the self-consciousness of being perceived after a long absence. Instead, he kept his bonds alive in the way introverts often do: through the written word. Long, meticulous letters would arrive in Sevagram, the handwriting as precise as his military training, the sentiments as unguarded and warm as a Friday night Scrabble game.
He died on March 13, 2015, at the age of eighty-eight, survived by his wife.
The MD theses his students produced still sit on the department's shelves, serving as a patient, quiet record of Wardha's history. But his true legacy does not exist in institutional files. It lives in the memory of a steady man who stepped into a fractured department, offered eight years of undemonstrative brilliance, and asked for nothing in return except that the work be taken seriously. In Sevagram, that was always enough.
| 1926 | Born, 16 September, Mianwali, North-West Punjab (now Pakistan) |
| 1947 | Partition — crossed the border with what he could carry |
| 1950 | Completed MBBS, Government Medical College, Amritsar (Punjab University) |
| 1951 | Joined Army Medical Corps — Regimental Medical Officer; postings in Amritsar, Jubbulpore, Kirkee, and Jhansi |
| 1967 | Completed MD Preventive and Social Medicine, AIIMS Delhi |
| 1980s | Retired from Armed Forces Medical College, Pune — WHO team evaluating falciparum malaria control, northeastern India |
| 1983 | Arrived MGIMS, 28 October — took over Community Medicine without fuss; salary ₹2,520 a month |
| 1991 | Handed department to Dr. G.V.S. Murthy, 1 July — moved to Pune to support daughter’s MD in Paediatrics |
| 1991 | WHO consultant, National Leprosy Eradication Programme, Maharashtra |
| 2015 | Died, 13 March, aged eighty-eight — wife Mohini survived him |
A study of child bearing and rearing practice in Anji village of Wardha district
An epidemiological study of trachoma in rural slum area of Wardha district
An epidemiological study of hypertension in business community of Wardha
An epidemiological survey among the employees of ginning mills in Wardha
An epidemiological study of morbidity of female breast in rural community in Wardha dist.
Study of the impact of health educational intervention on knowledge attitude practice of 7th class students regarding nutrition immunization general hygiene
Study of drinking water quality in rural area impact of health practice on the health of consumer
Dr. Naresh Kumar Tyagi
MPhil, International Institute for Population Sciences Mumbai (1988)
PhD Statistics, Meerut University (1990)

The complaint remained identical across three decades. A researcher would appear at Dr. Naresh Tyagi's door—sometimes an anxious postgraduate student, sometimes a senior faculty member clutching a sheaf of handwritten data—and explain that they had conducted a study and now required his help with the analysis.
Tyagi would adjust his glasses and look at the numbers. He would ask when the study had been designed. Inevitably, he would learn that the design had been finalized months or even years earlier, entirely without his involvement.
"One of the problems I encountered all my life was that people didn't ask me to help them design the study. They would do the study, come along with the data, and then ask for my help."
He said this not with bitterness, but with the mild, enduring exasperation of a man who had spent his entire life explaining a fundamental truth of science: a statistician consulted after an experiment is like a doctor called after the patient has died. He could sometimes salvage the analysis; he could perform a brilliant statistical autopsy. But he could never salvage a flawed design. Yet, knowing this, he kept coming to work anyway, chasing the numbers in the hope of catching them early.
Born on January 6, 1951, in Saharanpur, Uttar Pradesh, Tyagi lost his mother when he was still a child. After the fifth grade, he left home, drifting from hostel to hostel, staying ahead of his studies through the kind of fierce, quiet self-sufficiency that early loss either shatters or cements. He completed his matriculation in Muzaffarnagar, earned a BSc from Vardhaman College in Bijnor, and finished an MSc in Statistics at DAV College in 1974.
He moved to Delhi for a difficult year, surviving a job at a private college that routinely failed to pay its staff. He abandoned a half-started MA in Economics only when a Government of India fellowship came through for the International Institute for Population Sciences (IIPS) in Mumbai. Population studies—the sweeping mathematics of human existence—became the specialization that would eventually lead him to Sevagram.
Between 1977 and 1980, he worked as a Junior Scientific Officer at K.E.M. Hospital in Mumbai, mapping the statistical effects of environmental pollution on human health. A WHO fellowship then took him to Indonesia and Thailand. Upon submitting his findings, the universe presented him with a rare, binary choice. On a single morning in 1980, two envelopes arrived simultaneously: one offering a position in the Indian Police Service, the other offering a post at a rural medical college in a Gandhian village.
He looked at the two divergent paths. He chose Sevagram.
He joined MGIMS on September 10, 1980, as a Lecturer in Statistics and Demography. It was a deeply unusual position: a non-medical statistician embedded inside a medical institution. His value was entirely dependent on the quality of the questions the clinicians around him were willing to ask—and on how early in their research they thought to ask them.
His closest intellectual partnership was forged with Dr. B.D. Bhatia, an Associate Professor of Paediatrics. Crucially, Dr. Bhatia did not bring Tyagi dead data; he brought him questions before the data existed. Together, they designed and published a groundbreaking series of papers on the relationship between low birth weight and maternal measurements. This work informed Tyagi's own MPhil thesis and his 1990 PhD in Statistics. The central question—why some babies are born underweight while others are not—was investigated through rigorous multivariate analysis across Wardha district. It was exactly how Tyagi believed all clinical research should function: a doctor and a mathematician, arriving at the truth together.
In 1982, when MGIMS acquired a computer from the ICMR, Tyagi sat down and wrote original programs in BASIC and FORTRAN to handle salary calculations and student admissions. Before the machine arrived, he had run the entire biostatistics operation on fiercely systematic paper-based methods, designed to impose rigid consistency on data that would otherwise arrive in chaotic, incompatible forms from different wards. His wife, Sudesh, joined MGIMS as a computer operator, working alongside him in the Medical Records Department to collect, enter, and clean the hospital's data. The institute's records from that era carry the unmistakable, reliable hallmark of two people who took numbers seriously enough to treat them with reverence.
Numbers governed his professional life, but they also dictated his personal rhythms. Every morning, Tyagi walked the Sevagram-Wardha road carrying a walking stick. It was not a social stroll; it was the kind of solitary, kinetic movement that a highly analytical mind requires to process complex probability. Those who passed him on those mornings knew better than to interrupt unless they had an equation worth solving.
In the evenings, the rhythm changed. Chess was his particular arena. The campus provided a rotating cast of formidable opponents—Dr. S.C. Varshney, Dr. R.M. Raizada, Dr. U.S. Jajoo, Dr. S.P. Kalantri, and Dr. G.V.S. Murthy. The chess games were fiercely strategic; the conversation around them was wonderfully light.
He was known for speaking his mind with mathematical precision. In an institutional setting, where diplomacy often dilutes the truth, his directness was legendary. He refused to soften assessments he knew to be accurate, and he never inflated praise for sloppy research. In a discipline where the integrity of a study depends entirely on an honest critique at the design stage, his bluntness was professionally essential, even if occasionally unwelcome.
His other great passion, entirely removed from medicine, was the Bombay Stock Exchange. Beginning in 1976 with the purchase of Tata Motors shares, Tyagi applied the exact same analytical rigor to the market that he brought to epidemiology: tracking trends, calculating moving averages, and making his own assessments rather than following the herd. Whether this obsession made him wealthy is unrecorded. That it engaged his brilliant, number-hungry mind is absolute fact.
He retired from MGIMS in January 2011, packing up thirty years of data. But men who chase numbers rarely stop counting. He immediately joined KLE University in Belagavi, Karnataka, as Professor and Head of Epidemiology and Biostatistics. In a sense, he was simply founding the same department he had built at MGIMS in 1982 all over again. Over the next decade, he developed curricula, expanded a PhD program, and was made a Fellow of the Indian Society for Medical Statistics.
His legacy at MGIMS, however, remained profoundly personal. His son, Vishal, completed his MS in Otolaryngology at MGIMS and now practices in Mumbai. His daughter, Swati, completed her MBBS at MGIMS and practices Obstetrics and Gynaecology in Haryana. Both were trained by the very colleagues their father had sparred with over chessboards and datasets for three decades.
Biostatistics is the subject medical students dread and researchers routinely abuse. They dread it because its logic is alien—the cold language of probability rather than the warm art of diagnosis. They abuse it by consulting its practitioner too late, asking a statistician to bless a badly designed experiment.
Dr. Tyagi spent thirty years at MGIMS fighting to be present at the beginning of the story rather than the end. He succeeded often enough to accumulate a monumental body of work: the birth weight studies, a hundred published papers, the original BASIC programs, and a generation of students who finally understood that a statistician is not a calculator, but a collaborator.
The core problem he described—that people came to him too late—was never fully solved. But the people who did sit across from his desk learned what it looked like to do science correctly. And that is exactly what a master teacher leaves behind: not a perfectly solved equation, but a much clearer understanding of the math.
| 1951 | Born, 6 January, Saharanpur, Uttar Pradesh — lost his mother in childhood; left home after fifth grade |
| 1974 | Completed MSc Statistics, DAV College, Muzaffarnagar |
| 1975 | Fellowship, International Institute for Population Sciences, Mumbai — Government of India / UN programme |
| 1976 | Purchased Tata Motors shares — began lifelong engagement with the Bombay Stock Exchange |
| 1977 | Junior Scientific Officer, KEM Hospital and GS Medical College, Mumbai — environmental pollution and health |
| 1979 | WHO fellowship — Indonesia and Thailand; health delivery systems |
| 1980 | Two offers on one morning: Indian Police Service and MGIMS — chose Sevagram |
| 1980 | Joined MGIMS, 10 September — Lecturer in Statistics and Demography, Community Medicine |
| 1982 | MGIMS acquired ICMR computer — wrote salary and admissions programmes in BASIC and FORTRAN |
| 1988 | Completed MPhil, IIPS Mumbai — low birth weight in Wardha district |
| 1990 | Completed PhD in Statistics, Meerut University |
| 1994 | Organising Secretary, 12th Annual Conference of Indian Society of Medical Statistics, Sevagram — 110 delegates; torrential rains |
| 2011 | Retired from MGIMS, 31 January — 11,100 days |
| 2011 | Professor and Head, Epidemiology and Biostatistics, KLE University, Belagavi |
| 2012 | Fellow, Indian Society for Medical Statistics |
Dr. G.V.S. Murthy
MD Preventive & Social Medicine: All India Institute of Medical Sciences, Delhi (1985)

In his final MBBS examination at Guntur Medical College, a young G.V.S. Murthy sat down for the Preventive and Social Medicine (PSM) paper. He scored 75 out of 200. He failed. Six months later, he reappeared, scored 119, and quietly scraped through. The subject had beaten him once, and then, seemingly, released him.
Two decades later, that same young man was a full professor at the London School of Hygiene and Tropical Medicine. He was one of India's foremost public health researchers, the man who built the country's first Community Ophthalmology Department in the public sector, and the architect of a diabetic retinopathy screening program that would eventually safeguard the vision of 25,000 patients in Wardha district alone. The subject he had once failed had become the absolute cornerstone of his life.
An epidemiologist might describe this kind of irony as a confounding variable. Dr. Murthy preferred not to dwell on it. There was always the next project to build.
His full name—Gudlavalleti Venkateswara Satyanarayana Rao Murthy—carries his village inside it. Gudlavalleru, a town fifty kilometers southeast of Vijayawada, anchors the front of his name, a traditional Telugu marker tying identity permanently to geography. Born on New Year's Day in 1956, he was schooled in New Delhi before returning south to Guntur Medical College in 1974.
When he graduated with competent, though unexceptional, marks in 1979, he did not follow the familiar, ambitious trajectory of a young Indian doctor. Instead, he went to the mountains of Bhutan. Serving as a Medical Officer at the Chukha Hydroelectric Project from 1981 to 1982, he learned something a classroom cannot teach: how to practice medicine when the supply chain is broken, the infrastructure is minimal, and the textbook answer is simply unavailable.
By the time he completed his MD in Preventive and Social Medicine at AIIMS in 1985—spending his residency moving between tribal villages, urban slums, and rural settlements—he had accumulated a depth of fieldwork rarely seen in purely institutional careers. He had seen the vast, painful gap between what public health promised on paper and what it delivered in practice, and he began to think seriously about how to close it.
In October 1988, an elegant arrangement was proposed. Murthy's wife, Vishala, a brilliant microbiologist, wanted to pursue her MD. MGIMS had a vacancy in Microbiology under Dr. P. Narang. Meanwhile, the Community Medicine department needed a researcher. The geometry was perfect: Sevagram would gain a brilliant mind, and the Murthys would gain an academic base.
He arrived on January 2, 1989, taking a Reader position at Rs. 1,200 a month. By December 1990, he was an Associate Professor. By 1991, Vishala had completed her MD thesis on Mycobacterium tuberculosis. The plan had worked precisely as designed.
What had not been part of the design was how deeply Sevagram would embed itself in him.
Short, stocky, with large expressive eyes, Murthy possessed an immediate, magnetic ease in the classroom. He could pivot seamlessly between polished English and fluent Hindi mid-sentence. His true genius lay in his ability to shatter a complex epidemiological concept into its simplest components, reassembling it in front of his students so the logic glowed visibly at every step. Students who had found public health statistics utterly opaque suddenly discovered that, under Murthy's hands, the subject had a beautiful shape.
Beyond the lecture hall, he became the rare kind of academic that an institution quietly relies on to survive. He could hold a department head's absolute confidence without ever seeming obsequious, and defend a junior colleague's interests without appearing confrontational. He understood Sevagram’s Gandhian ethos not as a dusty historical footnote, but as the actual, living framework for practicing medicine. Whether navigating the unpaved village lanes of Anji or the academic corridors of the hospital, he was entirely at home.
On May 2, 1992, after three and a half years, he resigned. Vishala’s MD was complete, his aging parents in Delhi needed him, and AIIMS had offered him a position at the Dr. R.P. Centre for Ophthalmic Sciences.
It was a narrow door, but it opened into a massive room. Because Murthy arrived at community ophthalmology through the lens of public health, he began asking questions no one else was asking. While India’s eye care system in the 1990s was laser-focused on adult cataracts, Murthy looked at the devastating, unaddressed gap of childhood blindness.
He built India's first Community Ophthalmology Department in the public sector. He established a model pediatric eye care program that shifted national policy—a model later replicated in Indonesia and Nepal. From 2005 to 2015, as a full professor at the London School of Hygiene and Tropical Medicine (LSHTM), he worked with the WHO in Geneva, advised UNAIDS, and helped build the national monitoring system for India's HIV/AIDS control program.
His friends in Sevagram had always insisted that when Murthy left in 1992, the departure hadn't quite taken. He returned too often; he slipped back into old conversations too easily.
They were right. Decades later, a conversation with a former MGIMS colleague evolved into a massive public health intervention targeting diabetic retinopathy—an epidemic quietly blinding rural India. On October 20, 2016, MGIMS launched the Diabetic Care Initiative for Wardha district, funded by the Queen Elizabeth Diamond Jubilee Trust and supported by LSHTM. Mobile screening units drove into communities that had never seen an eye specialist.
Twenty-five years after leaving the campus, the man who had once failed his PSM exam was back in Wardha, serving as the architect of a program that identified 25,000 diabetic patients to safeguard their vision. The subject had claimed him completely.
Murthy is still active today, splitting his time between Hyderabad and London, still generating the crucial evidence that health policy in low-income settings requires but rarely receives. His elder son, Anirudha, a dentist with a master's in social entrepreneurship, works at the intersection of disability and health systems, walking the same territory his father pioneered.
In March 2024, the family suffered the kind of loss that disrupts every accounting of a life. Their younger son, Aashrai, a neurologist practicing in the United States, died young. In his memory, the Gudlavalleti family established the Dr. Aashrai Sai Venkat Gudlavalleti Memorial Award in Neurological Sciences, turning their grief into a lasting mechanism for medical excellence.
Dr. Murthy still carries his village's name at the front of his own, and it has traveled with him to Geneva, London, Lagos, and Kathmandu. He came to Sevagram for a brief three and a half years, failed to stay, and spent the next thirty years returning. His friends were right all along: he never really left.
Effect of supplementary nutrition in malnourished preschool (1-5 yrs) rural children of Dist. Wardha
Evaluation of conjunctival impression cytology in detection of vitamin A deficiency
Dr. Ashok Mehendale
MD Community Medicine, MGIMS (1986)
MPH, IIHMR Jaipur / University of North Carolina Chapel Hill (1996)

The cricket bat was not merely decorative. Three years later, in the inter-college tournament of 1979, MGIMS faced an engineering college from Nagpur. The opposing team boasted two fast bowlers who had played in the Ranji Trophy, and MGIMS was floundering. Mehendale walked to the crease at number six. He faced a searing delivery and, in one fluid, seemingly effortless motion, flicked his wrists. The ball soared over long-off, cleared the boundary fence, and landed permanently in institutional memory.
Those present that afternoon still recall the collective intake of breath from the crowd, the stunned expression on the bowler's face, and the quiet, almost imperceptible smile that crossed Mehendale's lips as he watched it land. He would spend the next five decades in Sevagram teaching community medicine with that exact same quality—the rare capacity, at the precise moment it mattered, to make the impossible look effortless.
He was born in Wardha on March 22, 1956, though his family possessed no settled geography. They had roots in Madhya Pradesh, Karnataka, Gujarat, and Maharashtra, passing through Vadodara and Navsari before arriving in Pune. His father, Dr. Madhukar Anant Mehendale, was a Sanskrit scholar of towering international standing—the mind behind the Dictionary of Sanskrit on Historical Principles, a researcher of rock inscriptions, and a lecturer at Göttingen and Yale. His mother was a librarian. At home, Ashok was called "Gamya," a name his parents elegantly constructed from the third and fourth notes of the Indian classical music scale.
As a child, his handwriting was flawless. In the fourth standard, his boru (reed pen) glided across the page with such precision in an inter-school competition that relatives later joked it predicted his fate as a doctor. (Naturally, once ballpoint pens replaced fountain pens, his handwriting deteriorated comprehensively, cementing his medical destiny).
When he sat for the B.J. Medical College entrance in Pune, he tied for the final available seat. The seat was awarded to a female student. His mother, who had once held admission to three medical colleges without attending any, refused to accept this as the end of the road. She pointed him toward the entrance examination for MGIMS. Soon after, a telegram arrived from Dean Dr. I.D. Singh, summoning the young man to Sevagram.
On July 27, 1976, he stood before a formidable ten-member interview panel. Decades later, he would remember only one face clearly: Dr. Sushila Nayar, who had designed the examination herself and insisted on questioning each candidate personally.
"Why do you want to become a doctor?" she asked him.
Mehendale knew the expected answers: to serve the poor, to help the suffering, to give back to society. He chose to say something true instead.
"This is the only profession where one can blend swarth—self-interest—and parmarth—altruism."
Badi Behenji smiled. She then tested him on Gandhian history. He named the Aga Khan Palace and Yerawada Jail without hesitation, recalled Gandhi's appendectomy at Sassoon Hospital, and spelled out "BCG" in full when challenged. At six o'clock that evening, the results were posted. He had topped the entrance examination.
From that first interview until her death in January 2001, Ashok Mehendale remained firmly within Sushila Nayar's trusted inner circle. He shared meals at her table, drove her to the hospital, accompanied her on remote field visits, and traveled with her across the country. In a railway compartment in Delhi, she casually introduced him to Atal Bihari Vajpayee. Though she always struggled to pronounce his Marathi surname—there being no equivalent for the hard 'L' sound in Hindi—she considered him family.
Her influence on his career was absolute, direct, and entirely unconventional. When he completed his MBBS and wanted to specialize in pediatrics, she simply told him the seat was taken. When he asked to pursue a Diploma in Child Health, she refused. When he drifted into Pathology as a demonstrator, she promptly summoned him back and placed him in Community Medicine. There, the General OPD offered him exactly what he had actually been searching for: children to treat, immunization programs to run, and mother-and-child welfare at the absolute center of his daily life.
Dr. Sushila Nayar personally selected his MD thesis topic, despite not being his official guide, signing off on it at the Nagpur airport before buying him a cup of coffee. In April 1986, when he sat for his MD practical examination, she was in Delhi undergoing surgery and could not be present. He passed the examination without her in the room. He later reflected that perhaps this was the entire point—she had spent a decade preparing him to stand without her.
The rural programs that defined his teaching life at MGIMS were originally conceived by Dr. Sushila Nayar and Dr. B.K. Mahajan, but they became Mehendale’s to run, his to inhabit, and eventually his to transmit to a generation of students who had never met the founders.
He oversaw the grueling Social Service Camps for decades, sending first-year students into villages for a two-week immersion where they ate the same food and drank from the same wells as their assigned families. Because he had been one of those terrified students himself in 1976, he knew exactly what the experience required and precisely the kind of doctor it was capable of producing.
The Reorientation of Medical Education (ROME) camp at the Kasturba Rural Health Training Centre in Anji was his personal domain from 1988 to 1990. Students arrived stripped of their tertiary hospital assumptions. They worked alongside village health workers and conducted surveys that forced them to view a community as a living organism rather than a collection of hospital beds.
Dr. Amol Dongre, who was posted at Anji under him, remembered Mehendale braving floods during fieldwork, collecting jowar for the Health Assurance Scheme, and sleeping on rough gunny sacks when the work ran late into the night. It is a precise memory, because a senior doctor sleeping on a gunny sack in a flooded village is the kind of image a medical student never forgets.
In 1990, Dr. Sushila Nayar informed him he was to become the Warden of the Boys' Hostel. Her logic was unassailable: "You've been a student here since 1976 and know hostel life inside out. Now it's time to sit on the other side of the table." He dutifully packed his belongings, left his comfortable quarters, and moved into the Warden's Apartment in A Block for five years.
He had lived in those exact rooms himself. He knew instantly when midnight noise was genuinely dangerous and when it was simply the kinetic energy of twenty-two-year-olds with nowhere else to put it. He rarely raised his voice; a single, calibrated look was usually sufficient. He was not positioned "above" the students in the traditional, antagonistic manner of wardens. He was, in some essential sense, continuous with them—he was simply the boy who had arrived at Wardha station with a cricket bat, just a little further down the line.
In 1995, Mehendale applied for a Master's in Public Health through a United Nations Development Fellowships program, backed by a fierce personal recommendation from Dr. Sushila Nayar. The selection committee quickly informed him that the program was exclusively for women from developing countries. He was entirely ineligible.
Dr. Sushila Nayar pressed his case anyway. The committee bowed to the pressure, creating an unprecedented "thirteenth" fellowship position—an exception made specifically for him, making him the only male recipient that year. He completed the program between Jaipur and the University of North Carolina, returning to Sevagram in 1996 with an MPH and immediately resuming the heavy work that had been waiting for him.
Among those who knew him, what stayed with you was not just the reach of his memory, but its warmth. It did not feel stored; it felt inhabited. Years later, an alumnus would return quietly, unsure if he would be recognised, and before he could introduce himself, Mehendale would look up, say his name, ask after his parents, recall the town he came from, and trace, in a few unhurried sentences, the arc his life had taken. Nothing announced, nothing displayed—just a mind in which people did not fade.
That same instinct shaped the MGIMS Alumni Association he helped found in 1993 and tended for decades. When visitors arrived—researchers, donors, old students finding their way back—the institute turned to him almost by reflex. He would begin without preamble, his voice settling into its natural register, moving between Hindi, Marathi, and English as the moment demanded. What followed was never a formal account. It was a walk—through the Ashram, across the wards, into the spaces where the institution had slowly taken form.
And somewhere along the way, the years would begin to gather. A name would open into a face, a face into a family, a family into a place you could almost see. He would pause at the library, linger in the Adhyayan Mandir, and then, as if she had only just stepped out for a moment, Dr. Sushila Nayar would enter the telling—present, immediate, unmistakably alive. You might begin by listening. But before you knew it, you were no longer outside the story. You were walking through it.
He was promoted to Additional Professor in December 2000. Just ten days into the new year, on January 3, 2001, Sushila Nayar died. The Silver Jubilee reunion of his 1976 batch had been held just days prior on Christmas. The profound loss that followed was the kind that never truly resolves; it simply becomes part of the permanent architecture of a life.
He led the department from October 2010 to March 2020, guiding twenty-three postgraduates and authoring fifty research papers. In May 1995, he married Anuradha. Their children, Ajita and Shivansh, were both born in Sevagram and naturally gravitated toward the healing arts—Ajita pursuing her postgraduation in dental surgery, and Shivansh in orthopedics. Even after his official retirement from MGIMS, the compulsion to teach remained unbroken. He took a final guard at Jawaharlal Nehru Medical College until late 2024. Only then did he finally declare his long innings closed and walk back to the pavilion—gloves off, pads unbuckled, his bat resting quietly after half a century at the crease.
He arrived in 1976 with a tin trunk and a cricket bat. He never quite left. The terrified young students who passed through his village camps are now the senior doctors and department heads shaping the future of Indian medicine. They still remember the man who slept on a gunny sack in a flooded village, and who could still, half a century later, tell them their own names without ever needing to be reminded.
| 1956 | Born, 22 March, Wardha — father Dr. Madhukar Anant Mehendale, Sanskrit scholar; lecturer at Göttingen and Yale |
| 1976 | Topped MGIMS entrance examination, 27 July — answered Dr. Nayar’s question about swarth and parmarth |
| 1976 | Arrived Wardha station — trunk in one hand, cricket bat in the other |
| 1979 | Six over long-off — inter-college cricket tournament against Ranji Trophy bowlers; MGIMS 1975 batch reunion |
| 1982 | Completed MBBS — placed in Community Medicine by Dr. Nayar after Pathology demonstratorship |
| 1986 | Completed MD Community Medicine — examination in April; Nayar in Delhi for surgery, could not attend |
| 1986 | Joined MGIMS faculty, June — Lecturer in Community Medicine |
| 1988 | Oversaw ROME camp, Anji — slept on gunny sacks during floods; stayed because the work was not finished |
| 1990 | Appointed Warden, Boys’ Hostel A Block — by Dr. Nayar; stayed five years |
| 1993 | Co-founded MGIMS Alumni Association — with Dr. A.P. Jain |
| 1995 | UNFPA / UN Development Fellowship — only male recipient; MPH at IIHMR Jaipur and UNC Chapel Hill |
| 1995 | Married Anuradha, May |
| 2000 | Promoted Additional Professor, December |
| 2001 | Dr. Sushila Nayar died, 3 January — twenty-five years after the entrance examination |
| 2010 | Head of Department of Community Medicine — until March 2020 |
| 2020 | Retired from MGIMS, March — continued teaching at JNMC Sawangi until late 2024 |
Fertility trends in rural Wardha
Epidemiology of reproductive tract infection in rural Wardha
An epidemiological study of nutritional anemia amongst adolescent girls in village around MGIMS Sevagram
Study of coronary heart disease at Kasturba hospital MGIMS Sevagram
Process documentation of activities at Kasturba rural health training centre, Anji
Assessing the role of integrated management of childhood illness (IMCI) at household level in rural area : an intervention study
Epidemiological study of reproductive tract infections in rural area of Wardha district
A study to find out reasons of partial/ no immunization in rural area of Wardha
A study of chest symptomatic with cough more than two weeks vs. three weeks for diagnosis of pulmonary tuberculosis
An epidemiological study of neonatal morbidity in rural Wardha
An Epidemiological Study of Ocular Morbidity Among Population of Age 50 Years and Above in Five Currently Adopted Villages of MGIMS
Epidemiological Study of Morbidity Amongst the Elderly Population in Rural Wardha.
A Study on Health Profile of Youth in Rural Wardha.
An Epidemiological Study of Maternal Morbidity in the Area of PHC, Kharangana (Gode)
Assessment of effect of Early Childhood Development interventions on child feeding practices including responsive feeding and nutrition status of 6 to 23
Effect of Probiotics on nutritional status of children based on the follow up study of a cohort.
Epidemiological study of Common Mental Disorders in women of reproductive age group in Central India
Assessment of readiness to quit tobacco use by using “stage of change” model among high school attendees: A cross sectional study
Health literacy about antenatal, intranatal, postnatal and child health care among mothers having children of age 6 to 24 months: A cross sectional study from tribal region in central India
Magnitude and determinants of gestational diabetes: A cross sectional study from field practice area of a medical college
Health literacy about antenatal, intranatal, postnatal and child health care among women of reproductive age group (15 to 45 years), the cross sectional study in tribal region of Central India
Dr. A.P. Jain
MD General Medicine, KGMC Lucknow
PhD, Nagpur University (1990)

Four days before he fell, Dr. A.P. Jain walked into Dr. Kalantri's office and sat down. They spoke for an hour—about the past, the present, and what he hoped for in the days ahead. His hands trembled, and his steps were heavily unsteady, but there was absolutely no fear in his voice.
He said, simply: "I take life as it comes." Then, with shaking hands, he pushed back his chair and walked away.
On February 6, 2025, he fell in his bathroom, suffering a devastating brain hemorrhage. He spent four weeks navigating critical care units in Nagpur and Sevagram. He died on March 15, 2025, inside the very ICU where he had taught, treated, and mentored for nearly fifty years—connected, in the end, to the dialysis machines he himself had introduced to the hospital two decades before.
His name, Ajeet, meant unconquerable. Those who knew him found the name astonishingly precise.
Born on May 1, 1945, in Sikandrabad, western Uttar Pradesh, he was the sixth of nine children. He completed his MBBS and MD at King George's Medical College in Lucknow. After briefly exploring psychiatry, he found his permanent, unyielding territory in internal medicine.
He married Sushila in Mumbai in 1972 and returned to Sikandrabad to establish a private practice. The practice did not survive. It failed because his patients expected treatment without payment, and he found himself expected to be a physician without sleep. After a brief, frustrating stint at the Durgapur Steel Plant Hospital—where trade unions attempted to dictate his medical prescriptions—he found a vacancy at MGIMS.
He arrived in June 1974. Sevagram in that monsoon season was a two-trains-a-day village, accessible only by horse-drawn tonga, entirely devoid of hotels or English-medium schools. For a couple raised in Lucknow and Bombay, the adjustment was sharp and unforgiving. But Sevagram had a way of making itself necessary to certain people before they quite understood how it had happened. He intended to stay briefly. He stayed for forty-nine years.
He kept a specific, pointed phrase for medical residents who relied too quickly on laboratory tests: The area between the two ears—the brain—is a physician's first and most powerful instrument. He meant this literally. He had trained in an era where clinical diagnosis was meticulously built from history, physical examination, and a basic X-ray. He brought that fierce discipline to Sevagram and maintained it across five decades, even as the technology around him exploded. He was not a Luddite—he introduced echocardiography to the department alongside Dr. O.P. Gupta, and he procured the hospital's first hemodialysis unit. He simply insisted that technology must confirm what the physician’s examination had already suggested, never substitute for it.
At the bedside, he physically crouched down to the patient's level. He listened not only to their symptoms but to their pauses, their hesitations, the things they started to say and abruptly stopped. He took the pulse. He asked a perfectly timed question. He could trace the invisible arc of an illness through history and bare hands alone. His residents watched this method not as a theatrical performance, but as a masterclass demonstrated repeatedly, available to anyone willing to pay attention.
His postgraduate sessions began at 8:00 a.m. Punctuality was not a preference; it was the baseline condition under which teaching was even possible. The structure was beautifully rigid so the learning inside it could be fluid: Mondays were journal clubs, Tuesdays and Thursdays were bedside cases, Wednesdays were mortality reviews, Fridays were X-ray discussions.
In his early years, he was strict in a way that many residents experienced as sheer severity. He routinely dismissed people from the ward for mistakes. He had absolutely no patience for sloppy clinical thinking, careless documentation, or informal English. He corrected their grammar. He corrected their handwriting. For those who survived the crucible, he was modeling a standard of precision that medicine desperately requires but rarely enforces. Looking back across their careers, his students realized the strictness and the brilliance were inseparable.
He guided thirty-four MD students. He established the DNB Family Medicine program and the PG Geriatric Medicine course, both achieving national recognition. In a beautiful piece of institutional irony, the man who had personally failed the DNB examination in 1983 was awarded the National Board’s "Best Teacher Award" in 2018.
In 1995, Dr. Sushila Nayar suffered a heart attack. As the powerful founder-president, she could have demanded treatment at AIIMS. She could have flown abroad.
Instead, she chose Dr. Jain as her physician, keeping him in that role until her death six years later. He was not merely her cardiologist; he was the one person she trusted to understand what she needed and to tell her the unvarnished truth about it. To be trusted completely by a woman who had spent decades ruthlessly assessing the trustworthiness of everyone around her was not a medical credential. It was a measure of absolute character.
In 2018, he was diagnosed with a rare, progressive genetic ataxia. There is no cure. Suddenly, every physical step became a conscious, dangerous calculation. His hands, which had held a stethoscope with the relaxed authority of half a century of practice, began to tremble violently when he wrote. Vertigo constantly threatened his balance. He was forced to grip the podium during presentations. Yet, he fiercely resisted assistance.
He did not ask why. He simply continued. He led rounds, attended seminars, and participated in journal clubs until his contract ended in August 2023.
But his greatest lesson was not taught in a lecture hall. When his wife, Sushila, suffered a catastrophic cardiac crisis in 2022, and later severe sepsis in 2024, she required life support at Sevagram. On both occasions, Dr. Jain stepped back entirely. The physician who had spent his entire life fiercely insisting on his own clinical judgment chose, when it mattered most, to exercise none of it. He placed his wife's life in the hands of the treating team without a single question, without interference, and without demanding a second opinion. That breathtaking act of restraint told his colleagues more about his profound trust in the institution than fifty years of ward rounds ever could.
He survived long enough to see his legacy multiply. His sons, Pramod and Manish, became professors in Orthopaedics and Paediatrics at MGIMS. Their wives, Sonia and Shuchi, rose to head the departments of Dermatology and Obstetrics & Gynaecology. Today, five distinct clinical disciplines are anchored by a single family at the college where he spent his life.
He died in the ICU he had built, on the machines he had procured, inside the hospital he had served for forty-nine years. In his last recorded conversation, he said he took life exactly as it came. He pushed back his chair with shaking hands. And he walked away, unconquered.
| 1945 | Born, 1 May, Sikandrabad, Bulandshahr district, Uttar Pradesh — sixth of nine children |
| 1972 | Completed MBBS and MD, King George’s Medical College, Lucknow |
| 1972 | Married Sushila Mittal, 26 January, Mumbai |
| 1972 | Private practice, Sikandrabad — patients expected treatment without payment; practice did not survive |
| 1974 | Joined Durgapur Steel Plant Hospital — trade unions attempted to direct prescriptions; left within a year |
| 1974 | Arrived MGIMS, 21 June — Sevagram accessible by tonga, no hotels, no English-medium schools |
| 1982 | Began guiding MD students — 34 students over three decades |
| 1983 | Failed DNB examination — the same National Board gave him its Best Teacher Award in 2018 |
| 1990 | Completed PhD, Nagpur University — under Drs. Choubey and Harinath |
| 1995 | Became Dr. Sushila Nayar’s personal physician — held that role until her death in 2001 |
| 2007 | Established DNB Family Medicine programme — national recognition; ran until 2018 |
| 2008 | Established PG Geriatric Medicine course — national recognition; ran until 2021 |
| 2018 | Diagnosed with rare genetic ataxia — continued teaching, rounds, and seminars |
| 2018 | National Board of Examinations Best Teacher Award |
| 2023 | Retired, 31 July — 17,937 days after joining |
| 2025 | Died, 15 March, Sevagram — brain haemorrhage; connected in the end to the dialysis machines he had introduced |
A study of clinical profile pulmonary functions, radiological and electrocardiographic features and filarial immunoglobulins in tropical pulmonary eosinophilia
A study of humoral immuno regulatory mechanisms in lepromatous spectrum of leprosy with special reference to its reactions
A study of humoral immunological profile in certain hereditary ( sickle cell haemoglobinopathy ) and acquired ( iron deficiency ) anemias
Study of effects of zinc sulphate and levamisole on immune functions in sickle cell hemoglobinopathy
A multidimensional Clinico etiological approach effect of anxiolytic antidepressant drugs in the irritable bowel syndrome
A clinico-etiological study of moderate severe anemia and bone marrow biopsy as a diagnostic technique
Clinico-Echocardiographic correlation of left ventricular function in acute myocardial infarction
Multidimensional study of the clinical profile of acute myocardial infarction
Evaluation of prognostic factors and recovery profile in stroke
Study of lifestyles and effect of sprouting cereals and legumes on blood glucose in diabetes mellitus
Study of glycemic index of some common foods in diabetics and non diabetics
Comprehensive evaluation of the elderly
Study of risk factors for chronic vascular complications in diabetes mellitus with special reference to Microalbuminuria
Profile of cirrhosis of liver amongst hospitalized patients in rural central India
Study of oxygen free radicals and antioxidants in certain disease states involving endothelial injury ( diabetes mellitus, acute myocardial infarction ) and effect of short term vitamin e supplementation
An endoscopic study of dyspepsia with special reference to helicobacter pylori in rural central India
Hospital based study of medical psychological impact of alcoholism
Observational study of polyarthritis in a rural referral hospital in Vidarbha region
Sociodemographic and clinical profile of headache : A rural hospital based study
Profile of heart failure in rural central India: A hospital based observational study
Evaluation of diagnostic tests in pleural effusions
Correlative study of symptoms and spirometry in adult bronchial asthma
Role of carvedilol as add on therapy in heart failure in Central India: A Randomized Controlled Trial
The study of prevalence of sleep apnea syndrome in COPD patients
Role of lifestyle associated risk-factors in the development of hypertension prevalence of target organ damage in the hypertensive population
Clinical and psychological study of attempted suicide in rural teaching hospital
Study of Aetiology, Clinical Profile, Role of Psychiatric Comorbidity and Effect of Treatment of Dyspepsia
Study of prevalence of peripheral neuropathy in asymptomatic and symptomatic diabetic patients by nerve conduction study and the variables affecting its development
To study the effect of Physiotherapy in Patients of Fibromyalgia in a 6- months follow-up period using Fibromyalgia Impact Questionnaire
Risk factors for chronic obstructive airway disease and predictors of acute exacerbation : A prospective study in rural central India
Study of Prevalence of Pulmonary Hypertension in Adults with Cirrhosis of Liver in Rural Hospital in Central India
Correlation of Health Related Quality of Life and 6 minute walk test with Severity of Chronic Obstructive Pulmonary Disease in Rural India
Screening strategies for identification of COPD in the geriatric population of rural central India: A population based study
Detection of chronic kidney disease in high risk groups
Dr. Hari Narayan Khattri
MRCP, Edinburgh Clinical training, Hammersmith Hospital London
Before echocardiograms and digital monitors entered the wards, cardiology depended almost entirely on the raw acuity of a physician’s senses. Dr. H. N. Khattri belonged to that fading, masterful era.
In a rural hospital where technology was exceptionally scarce, his trained eyes, highly sensitive hands, and attentive stethoscope more than filled the gap. He practiced and taught medicine at a time when diagnosing a patient meant studying the living, breathing person in front of you, not merely scanning a printed sheet of investigations.
In his hands, the basic physical examination—inspection, palpation, percussion, and auscultation—was elevated to an exact science. He seemed to literally read the heart through the chest wall. Long before humming machines traced cardiac images onto glowing screens, Dr. Khattri could reliably anticipate exactly what those images would eventually show.
Among the students at MGIMS, he acquired a quiet, awed reputation: he was the physician who could "see" the heart without ever opening the chest.
Dr. Khattri came to Sevagram carrying formidable academic credentials. Born in November 1937, he graduated with his MBBS from King George Medical College, Lucknow, in 1959. Like many ambitious, elite physicians of his generation, he traveled to the United Kingdom for advanced training, earning his MRCP from Edinburgh.
In the early 1970s, he trained at London’s prestigious Hammersmith Hospital, working directly alongside renowned cardiologists such as Professor Goodwin and Professor Shillingford. It was there that he refined his deep understanding of coronary artery disease and the then-emerging techniques of cardiac angiography.
When he returned to India, he joined the Postgraduate Institute of Medical Education and Research (PGI) in Chandigarh. Yet, by the late 1970s, his academic promotions had stalled within the institutional bureaucracy.
At that very moment, MGIMS found itself in a crisis. Its Professor of Medicine had suddenly left for a lucrative post in Libya, and the department was left adrift. Dr. Sushila Nayar moved quickly. In September 1978, she wrote to the Director of PGI in words that were at once candid and urgent: “We are badly in need of a substitute… I understand that you have with you Dr. Khattri and Dr. Deodhar, and that their promotions are blocked. I also understand that Dr. Khattri is keen to come. I would be grateful if you could depute him to us for a year.”
The solution benefited both institutions perfectly. MGIMS secured a highly capable physician to stabilize its teaching program; Dr. Khattri secured a department where his elite skills could be fully utilized. In November 1978, the London-trained cardiologist arrived in Sevagram on deputation.
It is deeply tempting to imagine Sevagram’s early faculty as purely self-sacrificing, uncompromising idealists. Dr. Khattri, however, was also a highly practical father.
His son, Sanjeev, was an excellent student and an accomplished swimmer in Chandigarh. A sudden move to a remote, dusty village could have severely disrupted the boy’s academic and sporting development. Before fully settling into Sevagram, Dr. Khattri made careful, calculated arrangements. He ensured that Sanjeev secured admission to the Central School in Nagpur, allowing the child to continue his education and athletic training without interruption.
It was a brilliant, pragmatic compromise: the father would serve the rural hospital, while the son’s future remained entirely secure in the city.
Dr. Khattri stayed at MGIMS for barely two years, yet the mark he left on the institution far outlasted his brief tenure. A cardiologist and professor of medicine in the 1970s, he was remembered above all as a master of bedside teaching.
He lived in the MLK colony near the hospital and ran his clinical service with daunting discipline. Ward rounds began at 7:00 a.m. sharp. A student who arrived even a minute late risked being shut out of the entire day’s teaching, sometimes in full view of others. He inspired admiration, but he also kept his students in a state of constant alertness. In his presence, one came prepared or not at all.
Because formal postgraduate programmes had not yet begun at MGIMS during his tenure, he devoted the greater part of his formidable energy to undergraduate MBBS students. His bedside clinics became legendary. They were long, exacting, and often exhausting, but they opened a world that no textbook could fully capture.
These were the years when rheumatic heart disease crowded the wards of rural India. Patients came with scarred valves, enlarged hearts, raised neck veins, and breathlessness that had already worn down the body. Standing beside the iron hospital beds, Dr. Khattri taught students how to read these signs with their eyes, their fingers, and their ears. He showed them how to detect a distended jugular venous pulse, how to feel a displaced cardiac apex, and how to separate one murmur from another in the noisy uncertainty of a crowded ward.
He began with first principles and moved steadily through anatomy, physiology, and physical signs, explaining not only what to look for, but why it mattered, how it arose, and when it could be trusted. He was never theatrical. He did not mimic murmurs or turn the clinic into a performance. In a calm, measured voice, he made the heart intelligible.
He trained his students patiently and relentlessly. He taught them to listen before they reached for machines, to trust the hand on the chest wall, the eye on the neck veins, and the ear at the precordium. By the end of their clinical postings, they could interpret complex ECGs and diagnose serious cardiac disease with striking confidence, often without relying on sophisticated equipment. In a resource-poor setting, such disciplined clinical skill was not merely admirable. It was indispensable.
His classroom lectures did not quite carry the same life as his bedside sessions. He would arrive with a set of small cards—his own modest version of slides—and build the lecture carefully, point by point. If the wards revealed his brilliance, the lecture hall showed his method.
He also cut a distinctive figure. For a cardiologist, he seemed an unlikely one: heavily built, clad in khadi, walking regularly along the Sevagram-Wardha road, yet never losing his stout frame. But what students remembered in the end was not his appearance. They remembered the presence—a thick-glassed, khadi-clad cardiologist with a formidable command of clinical cardiology, and the rare gift of making generations of students hear the language of the heart.
Like many exceptionally strong personalities, Dr. Khattri had his limitations. He formed opinions about his students very quickly, and once those impressions were formed, they were cast in iron.
Members of the 1975 batch later recalled that, months before the university examinations even took place, he could confidently predict who would pass and who would fail. His predictions were often uncannily accurate—partly because of his razor-sharp clinical judgment, and partly because of the self-fulfilling biases that accompanied his favoritism.
He ruled the medical wards with an iron hand. Winning his approval was notoriously difficult; provoking his displeasure was dangerously easy.
Yet, his academic contributions to the institution were undeniable. He introduced rigorous journal clubs, unflinching mortality meetings, and systematic case discussions. He mentored brilliant younger faculty members like Dr. O.P. Gupta, Dr. A.P. Jain, and Dr. U.N. Jajoo. His teaching left such a profound impression that several of his students—including Dr. Krishan Agarwal—subsequently chose cardiology as their own life’s work.
Many students from the MGIMS batches of 1973 through 1977—among them Mohammad Jusab Khan, Hari Oam, Ashok Birbal Jain, and Kapil Gupta—still remember his bedside cardiology clinics almost word for word. Each of these clinical innings would often stretch for three unbroken hours, with the master diagnostician holding the young men and women in rapt attention.
In early 1980, Dr. Khattri requested to return to his parent institution at PGI Chandigarh. He left Sevagram in April of that year.
Three decades later came a tragic irony that medicine often delivers with quiet cruelty. The master physician who had spent an entire lifetime meticulously diagnosing diseases of the heart died from one himself.
Dr. Khattri succumbed to a massive pulmonary embolism that went entirely undetected until it was far too late. The brilliant doctor who could detect the faintest, most subtle murmur in a crowded, noisy ward was ultimately claimed by a silent clot within his own body.
His tenure in Sevagram was incredibly brief, but its influence deeply endured. Generations of MGIMS alumni still clearly recall the lessons he taught at the bedside—the lost art of observing carefully, touching thoughtfully, and listening deeply. Through them, the legacy of the physician who mastered the language of the human heart continues to live.
| 1937 | Born, November |
| 1959 | Completed MBBS, King George Medical College, Lucknow |
| 1960s | Earned MRCP, Edinburgh |
| 1970s | Trained at Hammersmith Hospital, London — under Professor Goodwin and Professor Shillingford; coronary artery disease and cardiac angiography |
| 1970s | Joined PGI Chandigarh — promotions subsequently blocked |
| 1978 | Dr. Sushila Nayar wrote to Director, PGI — “we are badly in need of a substitute” |
| 1978 | Arrived MGIMS on deputation, November — ensured son Sanjeev’s admission to Central School, Nagpur |
| 1978 | Introduced journal clubs, mortality meetings, systematic case discussions at MGIMS |
| 1980 | Left Sevagram, April — returned to PGI Chandigarh |
| c.2015 | Died — massive pulmonary embolism; undetected until too late |
Dr. Omprakash Gupta
MD General Medicine, Gajra Raja Medical College Gwalior (1969)
In July 2022, at the age of eighty, Dr. O.P. Gupta began volunteering at MGIMS. He had already retired from the headship of the Department of Medicine, from the medical superintendency of Kasturba Hospital, and from a decade as Dean. He had his chest opened for a bypass in 1995 and an angioplasty in 2020. By any reasonable measure, he had done enough.
Yet, at the postgraduate sessions he attended as a volunteer, he was always the first to arrive. He walked briskly. He stood straight. When a presentation contained a subtle clinical error, he found it. When a resident needed encouragement, he offered it. He did not invoke his staggering fifty-one-year institutional history as a reason for anyone to listen to him. He simply sat down and began to teach.
He would stay another year, finally retiring in August 2023. His fifty-two-year tenure is the longest in the history of MGIMS, a span that encompasses the institution’s entire existence from its chaotic third year through its modern sixth decade. Between 1969 and 2022, he taught every single medical student admitted to the college—3,680 future doctors. Today, his students practice medicine across the globe. On February 14th each year, they celebrate his birthday with the warm, grateful reverence reserved for people who were formed by someone whose discipline was absolute, but whose kindness was deeper.
Om Prakash Gupta was born on July 2, 1942, in Chirgaon, Jhansi. The youngest of four children, he completed his BSc in Gwalior and entered Gajra Raja Medical College in 1961. He had initially wanted to be an orthopaedic surgeon, but he found his true calling in internal medicine, completing his MD in 1969.
After a mandatory two-year government service requirement, he arrived at MGIMS on September 20, 1971. He did not apply through a formal advertisement, nor did he leverage a powerful connection. (Dr. Sushila Nayar, the formidable founder-president of MGIMS, hailed from his exact hometown, but he deliberately chose never to mention it. He wanted the position on its merits, or not at all).
He was twenty-nine years old when he joined as a Demonstrator. He would not leave for fifty-two years. His professors had practically demanded he enter lucrative private practice, but he found Sevagram’s serene simplicity and the prospect of a lifetime of teaching far more compelling. "For me," he later reflected, "the decision was as simple and straightforward as that."
When he arrived, the Department of Medicine had exactly three faculty members. Within weeks, one left. Dr. Gupta and the department head, Dr. S.P. Nigam, were left to shoulder the entire clinical, teaching, and administrative load of the nascent institution between the two of them.
For nearly fifteen years, Gupta admitted and treated patients in a decaying two-story building originally constructed by G.D. Birla as a guest house for visitors to Gandhi’s ashram. The general wards resembled dormitories, dimly lit by flickering tube lights. There were no mechanical ventilators, no multipara monitors, no infusion pumps, and no central oxygen. The most advanced piece of equipment in the entire building was a single ECG machine.
Every morning at 8:00 a.m., Dr. Gupta met with Dr. A.P. Jain and Dr. Ulhas Jajoo to painstakingly review the ECG interpretations made by residents overnight. This was not a formal protocol; it was the daily discipline required to maintain clinical excellence in a place with virtually no resources. Living a short walk from the wards in MLK Colony—in an era without television or mobile phones—he visited the wards unannounced in the evenings. He did not come to inspect or intimidate; he came to ensure his patients were safe.
He became the Head of Medicine in May 1980. Trained in the classic bedside tradition, he taught residents that while machines can confirm a diagnosis, a careful physical examination reveals it. Yet, he was never trapped in the past; he personally introduced echocardiography to the department in 1990, demonstrating that the preservation of clinical skills and the embrace of new technology were entirely complementary.
He did not delegate teaching. He guided thirty-four MD students to completion, listening to every family and every resident with absolute patience, even when the wards were overflowing.
"Dr. Gupta mastered the rare skill of bringing joy and engagement to every task," recalled Dr. Tejal Lathia. Dr. S.P. Kalantri, who joined his unit in 1983, remembered something quieter: a lunch invitation shortly after Kalantri’s marriage. Gupta and his wife, Geeta, received the young newlyweds as though they were the most honored guests the house had ever seen. The warmth was not reserved for formal occasions; it was simply the daily temperature of the man.
Dr. Gupta served as Medical Superintendent from 1985 to 1990, and then as Dean from 1994 to 2002. His leadership was defined by what he did not do: he did not project authority, he did not raise his voice, and he fiercely kept the institution clear of the nepotism and favoritism that routinely plague medical administration.
His most profound administrative legacy was introducing multiple-choice questions to the pre-medical entrance test, replacing the vulnerable long-essay format. It was a structural reform that made the selection process fairer, more objective, and impossible to improperly influence.
His quiet administrative grace extended to his relationship with Dr. Sushila Nayar. In her later years, when profound hearing loss caused her visible anguish during administrative meetings, Gupta began sitting beside her. Without being asked, he wrote out the ongoing conversations in longhand so the aging founder could still follow the proceedings of the institution she had built. It was the simple, practical, deeply human response of a physician to a patient in need.
In August 1990, at just forty-eight years old, the man who had spent his life treating heart attacks suffered an acute inferior myocardial infarction. It shocked the campus. He was thin, walked briskly, ate sparingly, never smoked, and had pristine blood sugar.
He recovered, eventually undergoing a bypass in 1995 and an angioplasty in 2020. He applied the same rigorous, proactive discipline to his own secondary prevention as he demanded of his residents. The man who had managed heart failure in a Birla guest house with nothing but an ECG machine lived to experience the full, miraculous progression of modern cardiac medicine as a patient—and he returned to work, always the first to arrive.
He retired from administration, but his mind never stopped moving. He edited the Journal of MGIMS for eighteen meticulous years. In his later life, encouraged by Mrs. Kamala Desikan, he took up sketching and painting.
Most remarkably, he cultivated a deep passion for poetry. His collection, Roshani ki Anant Talash, reflected the philosophical depth he had always brought to medicine. In a beautiful act of intellectual playfulness, he translated the Mandukya Upanishad—the shortest of the ancient texts—into haiku-style Hindi verse.
Today, at eighty-three, he types with the blistering speed of a professional and posts his chaste Hindi poetry on Facebook, where former students across the globe share it widely. Dr. Kalantri frequently spotted him through the wooden partition of their offices, hunched over his computer screen, deeply engrossed in learning something entirely new from the internet.
His wife, Geeta, retired as the Principal of Kasturba Vidya Mandir and continues to serve the women of Wardha. Together, they raised three highly successful children: their son Dilip, now the Head of Surgery at MGIMS; their son Sanjeev, a Vice President at Capgemini; and their daughter Deepti, a Senior Health Service Officer in Mumbai.
When Dr. Gupta finally retired in August 2023 alongside his lifelong colleague Dr. A.P. Jain, their combined departure stripped the department of over a century of clinical wisdom. The atmosphere in the hospital felt noticeably, permanently quieter.
He arrived at twenty-nine, when the institution was barely three years old. He left at eighty-one, having taught every student it had ever admitted. Across those fifty-two years, he turned up early, stayed late, and treated the people in the rural wards as though their care was the absolute center of the medical universe. In Sevagram, it was always supposed to be. And because of Dr. O.P. Gupta, it actually was.
| 1942 | Born, 2 July, Chirgaon, Jhansi district, Uttar Pradesh |
| 1961 | Entered Gajra Raja Medical College, Gwalior |
| 1966 | Completed MBBS |
| 1969 | Completed MD General Medicine — under Professor Ajay Shankar |
| 1971 | Joined MGIMS, 20 September — Lecturer in Medicine; chose not to mention that Dr. Nayar was from his hometown |
| 1973 | Promoted Reader |
| 1980 | Head of Department of Medicine, May — Associate Professor |
| 1983 | Full Professor, June |
| 1985 | Medical Superintendent, Kasturba Hospital — until 1990 |
| 1990 | Introduced echocardiography to MGIMS Medicine department |
| 1990 | Acute inferior myocardial infarction, August — thin, non-smoker, normal blood sugar; profuse sweating the presenting sign |
| 1994 | Dean, MGIMS — until 2002; introduced MCQ to pre-medical entrance examination |
| 1995 | Coronary artery bypass surgery |
| 2002 | Editor, Journal of MGIMS — until 2020; eighteen years |
| 2020 | Angioplasty |
| 2022 | Began volunteering at MGIMS postgraduate sessions, July — aged eighty; always first to arrive |
| 2023 | Retired, 31 July — 18,942 days; the longest tenure in this book |
Study of alpha-1 antitrypsin deficiency in chronic adult liver diseases
A study of Cor pulmonale in pulmonary tuberculosis
A comparative study of efficacy of anti-reactive drugs in therapy of type II lepra reaction utilizing immunological parameters of acute phase reactors and circulating immune complexes
A study of cardiac autonomic dysfunction in diabetes mellitus
Clinico- immunological correlative study of pulmonary and meningeal tuberculosis with special reference to cell mediated and humoral immunity
A study of latent ischemic heart disease asymptomatic diabetes using treadmill exercise test
Exercise electrocardiography in the evaluation of coronary artery disease in asymptomatic hypertensive individuals
Immunodiagnosis in tuberculosis meningitis
Treadmill exercise testing in bronchial asthma
Mycobacterial antigen detection for Immunodiagnosis of tuberculosis
Left ventricular muscle mass by echocardiography
Primary derived M-mode Echocardiographic parameters for diagnosis of left ventricular hypertrophy
Left ventricular mass in normal individuals with abnormal pressor response to physical and mental stress.
Comparative study of left ventricular function measurement of various parameters in normotensive pregnancy induced hypertensive women
Study of serum fructosamine levels in obese, non-obese, normal individuals and diabetes adults: correlations with glucose tolerance test and serum lipids
A comparative study of noninvasive methods for determination
A study of cardiovascular status in the elderly patient
A study of outcome of critically ill patient requiring intensive care at rural hospital Sevagram ( by modified Apache iii scoring )
A study of cases of myocardial infarction with special reference to risk factors prognostic indications
The study of prevalence of HIV infection in Patients with tuberculosis
Prevalence of rheumatic heart disease among school children a rural area in Vidarbha
A study of hyperinsulinemia in hypertension
Infections atherosclerosis : focus on chlamydia pneumoniae helicobacter pylori
The association of the ankle brachial index with coronary artery diseases
Role of C-reactive protein and cardiac troponin-T as prognostic marker in acute myocardial infarction
The Association of The Ankle Brachial index with coronary artery diseases : A cross sectional study
Study of carotid intimal medial thickness and apolipoproteins in patient of stroke
Prevalence of Left Ventricular Systolic and Diastolic dysfunction in normotensive and Asymptomatic Diabetic Patients
Prevalence of Pulmonary Hypertension in Sickle Cell Anaemia in a Rural Hospital of Central India
A comparative study of C-Reactive Protein and ST score (ECG) as prognostic indicators in a case of acute myocardial infarction in a rural hospital of central India
Dr. S.P. Kalantri
MD Internal Medicine. (Government Medical College, Nagpur, 1982)
MPH (Epidemiology) (University of California, Berkeley, USA, 2005)

He was born on Independence Day—August 15, 1957—the youngest of six siblings in a Marwadi family that had produced, across generations, not a single doctor. His father, Gokuldas Kalantri, managed cotton factories owned by the Bajaj group. His mother, Parvati Devi, had been educated only to the fourth grade. There was no medical tradition in the family, and no particular reason to expect that the youngest child would spend his entire life in a Gandhian hospital five miles from home. There was, in fact, no reason to expect much of anything, except that the youngest child always had to find his own way.
He found it, as he would find most things, through a combination of accident, instinct, and the quiet stubbornness of someone who knows what he does not want, even when he cannot yet name what he does.
His schooling moved through Wardha’s institutions, shaped by circumstance rather than a grand plan. He attended Balmandir, then Craddock High School—where a classmate named Suhas Jajoo sat nearby, sparking a friendship that would later determine his entire professional trajectory. At Swavalambi Vidyalaya, English arrived with the Biology curriculum, and Mathematics was quietly dropped. He opted out of Mathematics entirely out of fear. In retrospect, that fear was the most consequential academic decision he ever made: it permanently closed the door to engineering, leaving medicine as the only viable path forward.
When he enrolled at Jankidevi Bajaj Science College, he scored 73% in his BSc Part 1 examination—precisely the margin required for admission to medical college. Medicine had entered his life not through a burning vocation, but through the back door of habit and proximity. He was not marching toward a white coat with purpose; he was simply moving forward.
He entered Government Medical College (GMC), Nagpur, in 1973. Out of a batch of two hundred students, he would eventually emerge ranked fourth in his final MBBS examination. For much of his time at GMC, from undergraduate through postgraduate, he lived in Room No. 99—a number that became a private landmark. During his second year, his childhood friend Suhas Jajoo moved in with him. The Wardha connection had followed him to Nagpur.
During his 1978 internship, the rural posting in Bhadrawati planted something durable in his mind: an unvarnished understanding of what healthcare in rural India actually required, a lesson no lecture hall had ever conveyed with equivalent force. When he began his house jobs, he gravitated immediately toward Internal Medicine. It was not an accidental choice; all of his role models—the sharpest clinical minds at GMC—were in Medicine. He wanted to emulate them, without a single second thought.
His MD program began in 1980 under the formidable Dr. B.S. Chaubey. In a highly unusual move, Chaubey transferred the young doctor into his own unit and took him personally under his wing—a first in GMC Nagpur’s history. Kalantri completed his MD in 1982. He was twenty-four years old, sitting in Room No. 99, with absolutely no map for what came next.
He knew only one thing with uncomfortable certainty: he did not want to sit alone in a private clinic. He craved the noise and rigorous discipline of a teaching hospital—the ward rounds, the fierce arguments over a diagnosis, the quiet pride of watching a terrified student grow into a doctor.
In early May 1982, he went to visit Suhas at his home in Jajoo Wadi, Wardha. By sheer luck, he ran into Suhas’s elder brother, Dr. Ulhas Jajoo, who was already a Reader in Medicine at MGIMS Sevagram. Ulhas looked at him for a moment—long enough to sense exactly what the young man wasn’t saying—and asked casually: "Why don’t you join us at Sevagram?"
There was no grand speech. No persuasion. Ulhas simply acted. A brief word to the Medical Superintendent, Dr. Karunakar Trivedi. A quick meeting. A nod. The post of Senior Registrar was his, for ₹650 a month.
His father had already drawn a very different map. He had built a modest structure in Wardha with windows facing Indira Market. It was meant to be his son’s clinic, the steady income practically within reach. When told of the change in plans, disappointment slipped visibly through his father's eyes. But with a grace his son would only fully understand later in life, he said nothing, and quietly stepped aside.
On a scorching afternoon—May 4, 1982—Shriprakash Kalantri rode his Bajaj Priya scooter through the gates of MGIMS. After the imposing stone architecture of GMC Nagpur, Sevagram felt like another country. The hospital still partly occupied the old Birla guest house; the wooden floors creaked, and the walls peeled in tired layers. There were no ventilators, no monitors, no infusion pumps. Medicine here was practiced the old way: with a stethoscope, a remarkably steady hand, and whatever clinical judgment could be gathered at the bedside.
He joined Dr. A.P. Jain’s unit. The morning ECG correction sessions, led by Dr. O.P. Gupta, Dr. Jain, and Dr. Ulhas Jajoo, possessed the disciplined, terrifying quality of a court hearing. Residents lined up with the night’s ECGs clutched like confession letters, where every missed P-wave was a matter of grave consequence.
He was exactly where he needed to be.
His ascent was steady, each step earned through the slow accumulation of correct decisions at the bedside. He became a Lecturer in 1983, a Reader in 1987, a Professor in 1997, and a Director Professor in 2012.
In February 1984, he married Bhavana Laddha, a science graduate from Indore. Their son, Ashwini, and daughter, Amrita, were both born in Sevagram, delivered by Dr. Shakuntala Chhabra. Ashwini would go on to become a Professor of Community Medicine at MGIMS, marrying Shaily Jain, an administrative officer at Kasturba Hospital. Amrita completed her DNB in Radiology and married Dr. Sahaj Rathi, a hepatologist. The family that the institution had helped begin in 1982 had, by the next generation, grown into the institution itself.
When a lucrative offer to become Professor and Head at a privately owned medical college arrived in 1993, he swiftly declined. Sevagram had given him his professional ethics, his work culture, and an unbreakable connection to his students and patients. He never wanted to leave.
Acquiring an independent unit in 1992, he eventually guided thirty MD students. Many of their theses were published in international journals with the student listed as the first author and SP Kalantri as the last—a deliberate inversion of the academic hierarchy that distinguishes a teacher building careers from one simply harvesting credit.
A week-long workshop on Evidence-Based Medicine (EBM) in Toronto in 2001 permanently altered the register of his clinical thinking. The analytical tools he had been blindly reaching for finally had a name and a rigorous method. He returned with absolute clarity: the pharmaceutical industry’s deep, pervasive presence in the hospital was scientifically and ethically indefensible.
In 2001, he successfully persuaded the President of the Kasturba Health Society, Dhirubhai Mehta, to ban pharmaceutical and device companies from sponsoring medical conferences at MGIMS. It was the beginning of a massive structural earthquake.
In 2004, a Fogarty Scholarship took him to the University of California, Berkeley, where he completed an MPH in Epidemiology. When he returned, equipped with formal epidemiological weaponry, his stance was unambiguous: the industry had to go entirely. When he became Medical Superintendent in 2009, he banned medical representatives from the campus and launched a low-cost generic drug initiative. The cost of a hospital admission at Kasturba plummeted, fundamentally redefining what affordable healthcare meant in Vidarbha.
For decades, Kasturba Hospital’s information lived on fragile paper—registers, slips, and carbon copies covered in handwriting that oscillated between elegant and illegible. It worked, but with immense friction.
When the Hospital Information System (HIS) finally arrived in Sevagram in 2004, it required a decade and a half of agonizing, unglamorous labor. There were 3:00 a.m. trains to Nagpur, blue screens of FoxPro, and servers that crawled. Bhavana stepped in as the system’s database administrator. It was not a supporting role; she became the absolute spine of the project, holding the data architecture together whenever the institution’s enthusiasm for change collided with its appetite for familiar routine.
Today, the HIS that runs Kasturba Hospital is one of the few fully functional systems in India. It carries, invisibly, the legacy of two people with the same surname who spent fifteen years simply refusing to let it fail.
Nothing in Sevagram’s collective memory prepared it for March 2020. For MGIMS—an institution built on the Gandhian promise of open doors—the COVID-19 pandemic posed a cruel paradox: How do you serve the highly contagious without becoming victims yourselves?
As Medical Superintendent, Kalantri found himself in a war room without a map. The old administrative tools of negotiation and consensus-building were instantly obsolete, replaced by oxygen flow rates, tanker GPS coordinates, and the cold, terrifying arithmetic of mortality.
The hospital admitted nearly 6,000 COVID-19 patients. He secured massive donations to install permanent oxygen systems. Crucially, he demanded that only strictly evidence-based therapies govern clinical management, fiercely eliminating the irrational, politically promoted drug regimens sweeping the rest of the country. On Twitter, and across national media, he publicly argued for science. While much of Indian medicine temporarily capitulated to panic and pressure, in Sevagram, rational medicine held the line.
On February 15, 2023, he voluntarily stepped down as Medical Superintendent. His reasoning was characteristically sharp: "It is time to step down when people ask why, not why not."
Over the years, he gathered lives outside the hospital. Obsessed with books since the age of five, he also allowed cricket to shape his imagination. In 2015, he discovered cycling, completing grueling 300-kilometer non-stop brevets alongside his daughter Ashwini, sparking a cycling culture across the campus.
He writes relentlessly in Hindi, Marathi, and English. He documented all 204 classmates of his 1973 batch. He blogs on Matter-of-Fact. And eventually, he compiled ninety-three definitive portraits of the medical teachers who built MGIMS across four decades.
This book is the completion of that massive project. He arrived on a Bajaj Priya, trading his father’s carefully imagined clinic for ₹650 a month and a hospital with creaking floors. He found what he did not even know to ask for: a place where medicine became not merely a job, but the very structure around which his entire life would beautifully organize itself.
He is still here.
<strong>1973 — The Accidental Entry</strong></p>
<p>Joined GMC Nagpur for MBBS, having “inadvertently shut the engineering door” by choosing biology in Class 9.</p>
<strong>1981 — The Credentials</strong></p>
<p>Obtained MD in General Medicine from Government Medical College, Nagpur.</p>
<strong>1982 — The Summer of Arrival</strong></p>
<p>Arrived in Sevagram as a Senior Resident in the Department of Medicine, beginning a “brief posting” that has lasted over four decades.</p>
<strong>1983 — The Staff Register</strong></p>
<p>Appointed Lecturer in Medicine after an interview with the “titan” Dr. B.S. Chaubey.</p>
<strong>2004 — The Berkeley Pivot</strong></p>
<p>Awarded the Fogarty AIDS International Research Scholarship; obtained an MPH in Epidemiology from UC Berkeley, returning with a new focus on evidence and asking better questions.</p>
<strong>2007 — The Superintendent’s Chair</strong></p>
<p>Appointed Medical Superintendent of Kasturba Hospital, focusing on low-cost drug initiatives and the “grammar” of hospital systems.</p>
<strong>2020 — The Pandemic Years</strong></p>
<p>Led the hospital’s COVID-19 response, showcasing that desperate times do not require desperate measures—and that in medicine, restraint is often the best intervention.</p>
<strong>2026 — The Chronicler</strong></p>
<p>Returned to the wards and the classroom, while undertaking the “quiet urgency” of documenting the institutional history of MGIMS.</p>
Prognostic significance of pre discharge six week symptom limited treadmill test after acute myocardial infarction
Efficacy of fiberoptic bronchoscopy in smear negative pulmonary tuberculosis
Diagnostic utility of palpation and percussion in clinic assessment of cardiomegaly
Efficacy of clinical signs in the diagnosis of splenomegaly and ascites
Clinical profile of Snakebite in Sevagram : An observational study
A clinical profile of pesticide poisoning in Sevagram : an observational study
Blood pressure measurement by sphygmomanometer : knowledge, practice and instrument audit
The validity of physical examination in diagnosis of pneumonia
Validity of perception and palpation to screen fever
Validity of Siriraj and Guy’s hospital stroke scores for differentiating hemorrhage from ischemic strokes
Predicting outcome after stroke: Prospective evaluation of three stroke scores
Validity of history and physical examination in the diagnosis of hypothyroidism
Risk factors for acute myocardial infarction : A hospital based case-control study from a rural tertiary hospital in central India
Simple clinical predictors of brain lesions in patients with impaired consciousness: a cross sectional study from a rural, tertiary hospital in central India.
Predictors of in Hospital Mortality in Snake Bite : A hospital based Retrospective Chart Review
Accuracy of History and Physical Signs in Pleural Effusion
Is alcohol consumption associated with increased risk of intracranial hemorrhage? – a hospital based case control study in rural population in central India
Acute undifferentiated fever: A clinico-epidemiological correlation in a rural hospital
Accuracy of physical signs in the diagnosis of meningitis and the diagnostic accuracy of low CSF glucose in the diagnosis of bacterial meningitis
Diagnostic Accuracy of Rapid Diagnostic Test for Leptospirosis
Pattern and Problem of Pesticide Poisoning in a Teaching Rural Hospital – Retrospective Analysis of Hospital based Data
Accuracy of History and Physical Examination for Diagnosis of Acute Myocardial infarction: A Hospital Based Diagnostic Accuracy Study.
Predicting Mortality in Acute Intracerebral Haemorrhage by ICH Score.
Predictors of mortality in patient hospitalized with pesticide poisoning
Predictors of 30-day mortality and disability in patients hospitalized with acute incident stroke
Hyponatremia: Causes, Characteristics and Outcome in Critically ill Medical inpatients
Comparison of Acute Physiology and Chronic Health evaluation (APACHE 2) Score with organ failure score (SOFA) to predict hospital mortality in Medicine Intensive Care inpatients.
Incidence and Risk factors for Ventilator associated Pneumonia
Intermediate syndrome and respiratory failure in acute organophosphorus pesticide self-poisoning
Acute undifferentiated febrile illness in patients presenting to a tertiary care teaching Hospital in central India : Etiology, clinical spectrum and outcome
Clinical Predictors of In House Mortality in pateints with snakebite
Diagnostic accuracy of 20-minute whole blood clotting test (WBCT20) to detect coagulopathy in snake envenomation
Anion Gap and Serum Lactate Levels in Acutre Insecticide Poisoning
Perceptions of Palliative Care Among Patients with Head and Neck Cancer: A Hospital Based Mixed Methods Study
Burden Among Caregivers of Head and Neck Cancer Patients A Hospital-Based Mixed Method Study
Dr. Sanjay Diwan
MD General Medicine, Gandhi Medical College Bhopal (1988)

After completing his MD in August 1988, Sanjay Diwan noticed a job advertisement for MGIMS Sevagram circulating through the Department of Medicine at Gandhi Medical College in Bhopal. He was intrigued, but uncertain. Before acting, he sought the counsel of Shri Banwarilal Choudhary—a man deeply rooted in the Gandhian tradition, his father's trusted mentor, and someone who had spent considerable time at the Gandhi Ashram.
Choudhary did not offer a lecture. He did not weigh the strategic advantages of MGIMS against its alternatives. Instead, he simply gave the young doctor two names: Shri Kanakmalji Gandhi of Sevagram, and Dr. Ulhas Jajoo. That was all.
The names were enough. Diwan applied. While his friends anxiously urged him to take a secure, highly predictable Public Service Commission placement he had already been offered, he waited out the MGIMS interview period in a temporary post. He officially joined the institution on November 3, 1989. Looking back across the decades, he calls ignoring the safe path the best decision of his life.
Born on November 11, 1962, in Megha, a small town in Madhya Pradesh, he was the fourth of six children. His father, Vinay Kumar Diwan, was a Joint Director of Agriculture, a government post that kept the family moving regularly across the state. Diwan attended modest but sufficient schools in Dhar and Itarsi before arriving at Gandhi Medical College in Bhopal with the 1979 batch.
He completed his MBBS in 1984 and his MD in Medicine in 1988. He wrote his thesis on the comparative clinical efficacy of Flurbiprofen and Naproxen in rheumatoid arthritis. The subject was highly specific—not the kind of sweeping public health question that makes global headlines, but the kind of careful, granular comparative work that teaches a young doctor exactly how to weigh evidence. It was a habit of precision he would carry directly into the hospital wards.
At MGIMS, he was assigned to Dr. A.P. Jain's Unit II. The education that followed was entirely different from what he had encountered in Bhopal. In Sevagram, medicine meant thinking a problem through to its absolute end before reaching for an investigation. It meant meticulously organizing the history, working the physical examination, carefully constructing a differential, and arriving at a diagnosis through strict logic rather than clinical reflex.
The bedside was the arena where the teaching happened, and Dr. Jain ran it with a sharp precision that left absolutely no room for the comfortable vagueness that busy wards sometimes permit.
The residents who rotated through during those years—Ashwini Kumar, Kalpana, Chandra, Sanjeev Sharma, Ashish Bhalla, Firoz Sogiawala, Manisha Tanjea, Renuka Lamba, Prabhat Goel, Skand Trivedi—remained permanently etched in Diwan’s memory. In a small irony typical of the medical world, Dr. Trivedi is now his colleague at Bansal Hospital in Bhopal. Sevagram's alumni have a beautiful habit of reappearing in each other's lives at unexpected intervals.
During his tenure, he was promoted to Reader in November 1993. Six months before ultimately leaving Sevagram, he married Niharika, a dietician at Kasturba Hospital from Nagpur. Their lives and careers had been shaped by the exact same institution before they had ever spoken to one another—perhaps the most Sevagram kind of beginning possible.
He spent sixteen years at Jawaharlal Nehru Medical College in Sawangi, rising to Professor of Medicine by November 1999. What he encountered there, however, and what eventually made the institution untenable for him, was the familiar, suffocating pressure of a for-profit medical school. He found himself surrounded by wealthy students and administrators whose primary priority was keeping those students' families satisfied, rather than ensuring they had actually learned medicine.
The mechanism was straightforward and, tragically, not unusual in Indian private medical education: students who had not performed adequately were passed anyway. Teachers who objected were deemed inconvenient. Dr. Diwan had not entered medicine to sign off on failures. After sixteen years of trying to teach properly within a structure that fundamentally did not want him to, he walked away in 2016.
A second attempt at the Mahaveer Institute of Medical Sciences in Bhopal—owned by a childhood friend who had promised a different kind of ethos—revealed the exact same pattern: unfinished buildings, inadequate supplies, and a management far more interested in extracting fees than educating students. He did not stay long. By 2019, he had moved to Bansal Hospital, where the work was purely clinical and consultative, and where the heavy pressures of institutional compromise were finally replaced by the straightforward, honest demands of patient care.
At Sevagram, he had always been a man of few words. This did not stem from reticence or cold distance, but from a profound disposition that preferred deep attention over unnecessary speech. In the wards during the long, anxious nights before examinations, or in the frantic corridors between medical crises, he was the kind of presence that residents actively sought out. He was steady, unhurried, and always prepared to listen without rushing the speaker toward a conclusion.
Those who trained under him in Sevagram speak of what he offered not merely as instruction, but as atmosphere. He had a way of approaching a clinical problem that communicated, without a single announcement, that there was absolutely no need to panic—that the patient in front of them had not fundamentally changed since yesterday, and that a clear head was still the most useful instrument in the room. This is not a quality that can be quantified on a curriculum vitae. But for a terrified resident standing in the ward at two in the morning, it was the only quality that mattered.
His son Amartya, born in 1998, studied computer science. His daughter Tanvi, born in 2000, completed her MBBS and interned in Ujjain. They were born into the institutional life that Sevagram had started, even if Sawangi was where they physically arrived.
Dr. Diwan was at Sevagram for just over two thousand days—five and a half years, a brief tenure by the standards of a department whose other pillars stayed for decades. He came because a wise man gave him two names and no further explanation, because the two names were sufficient, and because something about the campus, once seen, proved far more compelling than the safe, stable salary his well-wishers had urged him to take.
He eventually left because the next stage of his career required it, not because Sevagram had given him any reason to go. He has always been clear about the difference. The sixteen years that followed, and the two painful departures from institutions that refused to meet his ethical standards, were the long consequence of having started his career in a place that showed him what medical education could actually be. He had simply found, thereafter, that most other institutions were not it.
| 1962 | Born, 11 November, Megha, Raipur district, Madhya Pradesh — fourth of six children |
| 1979 | Entered Gandhi Medical College, Bhopal |
| 1984 | Completed MBBS, Gandhi Medical College Bhopal |
| 1988 | Completed MD General Medicine — thesis on Flurbiprofen vs Naproxen in rheumatoid arthritis |
| 1989 | Sought counsel of Shri Banwarilal Choudhary — received two names: Kanakmalji Gandhi and Dr. Ulhas Jajoo |
| 1989 | Joined MGIMS, 3 November — Dr. A.P. Jain’s Unit II |
| 1993 | Promoted Reader in Medicine, November |
| 1995 | Married Niharika, 21 January — dietician, Kasturba Hospital, Nagpur; met at MGIMS |
| 1995 | Left MGIMS, 30 June — joined JNMC Sawangi as Professor of Medicine |
| 1998 | Son Amartya born, Sawangi — computer science |
| 1999 | Professor of Medicine, JNMC Sawangi, November |
| 2000 | Daughter Tanvi born — completed MBBS, Ujjain |
| 2016 | Left JNMC Sawangi — sixteen years; institutional compromise untenable |
| 2019 | Joined Bansal Hospital, Bhopal — clinical and consultative work |
Dr. Satya Prakash Nigam
MD General Medicine, Maulana Azad Medical College (1967)

On a bitterly cold December morning in 1970, Dr. Satya Prakash Nigam (known to generations of MGIMS students as Dr. S.P. Nigam) sat down in Solapur to write a letter. He was writing to Dr. Sushila Nayar to accept her offer of a faculty position at MGIMS. He formally stated that he was pleased to accept. But then, almost in passing, he added a tiny detail: he mentioned that he had already purchased khadi fabric to have new clothes stitched for his arrival.
This was not an accidental inclusion. Nigam knew that Sevagram had strict rules, and that wearing khadi was one of them. He also knew that Dr. Nayar, who had worked closely alongside Gandhi and carried the unbending ethos of those years into everything she built, would instantly notice a man who understood the cultural significance of the cloth before he had even set foot on campus. The mention of the khadi was a small act—a sentence, perhaps two—but it was the calculated, respectful act of someone who had read the place perfectly and wanted its founder to know it.
He arrived at MGIMS on January 22, 1971. He was thirty-four years old, carrying an MD from Maulana Azad Medical College and a paper already published in the British Medical Journal. Crucially, from the moment he began teaching, he became the very first faculty member in Medicine that the inaugural MBBS batch of MGIMS would ever encounter.
Born on October 22, 1936, he enrolled at Government Medical College, Nagpur, in 1957. During his college years, he was a debater—a serious one, not merely a casual participant. He won inter-college competitions, earned the prestigious college color for debating, and served as the secretary of the debating society. The skills this crucible produced—clarity of argument, the rare ability to hold an audience’s attention, and absolute confidence at the front of a room—would serve him brilliantly in hospital wards and lecture halls for the next four decades.
He earned his MBBS in 1961. What followed was a long, deliberately varied apprenticeship: a research fellowship in Medicine at Jabalpur, a senior residency at Irfan Hospital in New Delhi, and a lectureship at Miraj Medical College. The geographic range was intentional. He was assembling a vast command of clinical medicine from multiple settings that no single institution could have provided on its own.
His MD, completed at Maulana Azad Medical College in January 1967 under Dr. Chuttani, produced a thesis on ulcerative colitis. The resulting paper was published in the British Medical Journal in October 1967 and was described, in the parlance of the time, as trendsetting. He was just thirty years old and had been practicing medicine for nine years. By 1971, he was in Sevagram, wearing his new khadi.
When Nigam walked into the MGIMS wards in January 1971, the Department of Medicine was not yet a department in any formal sense—it was simply a man, a nascent teaching program, and a cohort of students who had never been taught clinical medicine by anyone else.
He carried the immense weight of that beginning, and his success was visible in what those inaugural students went on to accomplish. Dr. Balkrishna Maheshwari, from that first batch, topped Nagpur University in the Final MBBS. Dr. Govinda Pillai excelled in General Medicine. The department Nigam built from the ground up produced the academic results that justified the Medical Council of India's eventual recognition of MGIMS—a recognition for which his early, foundational work had been absolutely essential.
He was promoted to Associate Professor in July 1973—a role that briefly required him to also lead the Paediatrics Department when the need arose—and to Professor of Medicine in September 1976. The rapid pace of these promotions reflected the reality of a young, ambitious institution: seniority was accumulated quickly simply because there was a massive amount of work to do, and very few people qualified to do it. His starting salary was Rs. 750 a month. By July 1972, he had secured a scooter allowance of Rs. 40 per month—a rare badge of practicality in the social grammar of a Gandhian campus.
The 1970s at MGIMS belonged to a completely different diagnostic world. Investigations were severely limited, imaging was basic, and the laboratory's capabilities were restricted to those of a young rural hospital. In this bare-bones environment, raw clinical judgment—the trained capacity to read a patient's illness purely through observation, history, and physical examination—was not merely a traditional virtue; it was a daily survival necessity.
Nigam was, by all historical accounts, exceptionally gifted at it. He took immense pride in the diagnostic precision he could achieve with minimal technological investigation. His method at the bedside was characterized by a highly specific quality of attention: he was unhurried, obsessively thorough, and spoke in a tone that frightened patients found instantly reassuring. He was soft-spoken. His language was chosen carefully. Patients often felt that his presence itself was a form of treatment—that the simple act of being seen clearly and spoken to gently by a master physician who was plainly not in a rush was a powerful medicine all its own.
Outside the college, he served as the personal physician to Acharya Vinoba Bhave and the Bajaj family in Wardha. He ran medical camps in the surrounding villages, offering top-tier clinical skills to rural populations who would never otherwise have had access to a physician of his caliber.
In July 1978, he resigned, citing domestic and financial circumstances that he did not specify in detail, and which his colleagues respectfully accepted without pressing him. He was officially relieved of his duties on September 14, 1978, exactly seven and a half years after his arrival. He was forty-one years old.
He moved to Katni, a small town northeast of Jabalpur, and built a private practice from scratch. The transition from pure academic medicine to private practice is notoriously difficult—the skills overlap, but they are not identical. The social intelligence required to establish a thriving practice in an unfamiliar town is not taught in any medical curriculum. Yet, Nigam made the transition seamlessly. He understood that private practice required the ability to connect with patients as individuals, to factor their social circumstances into clinical decisions, and to cultivate relationships with other consultants grounded in mutual respect rather than cutthroat competition. Within a few short years, he became one of the most trusted physicians in Katni.
He practiced there for twenty years, bringing the exact same unhurried quality of attention to his private clinic that he had brought to the rural wards of MGIMS. Tragically, on August 5, 1998, he was killed in a road accident. He was sixty-one years old.
He had married Shashi in Lucknow in 1967, the same year his landmark paper appeared in the BMJ. Together, they raised three daughters. When he left MGIMS in 1978, none of them were old enough for medical college. But years later, two of them came back.
Jyotsna, from the 1985 MBBS batch, completed her MD in Medicine at MGIMS—studying in the very department her father had built from nothing. Namita, from the 1989 batch, completed her MD in Obstetrics and Gynaecology at the same institution. Their third sister, Divya, studied medicine in Odessa.
The two daughters who returned to Sevagram walked the exact same corridors where their father had once taught the inaugural batch of students. They learned from physicians he had personally trained, participating in an invisible, multi-generational chain of medical transmission that institutions sustain without always being consciously aware of it.
In December 1970, their father had written a letter stating he had bought the khadi. It was a small thing to say. It was also, as history proved, exactly the right thing to say—the quiet act of a man who understood that truly arriving somewhere requires far more than formally accepting a job offer. It requires the absolute willingness to become part of the place.
| 1936 | Born, 22 October |
| 1957 | Entered Government Medical College, Nagpur — debater, college colour, secretary of debating society |
| 1961 | Completed MBBS, GMC Nagpur |
| 1964 | Research fellowship in Medicine, Medical College and Hospital, Jabalpur |
| 1967 | Completed MD General Medicine, Maulana Azad Medical College — thesis on ulcerative colitis |
| 1967 | Published in British Medical Journal, 28 October — “trendsetting”; he was thirty years old |
| 1967 | Married Shashi, 6 March, Lucknow |
| 1968 | Lecturer in Medicine, Dr. V.M. Medical College, Solapur |
| 1970 | Wrote to Dr. Nayar accepting the MGIMS offer — mentioned he had already purchased khadi |
| 1971 | Arrived MGIMS, 22 January — first faculty member in Medicine; first to teach the inaugural MBBS batch |
| 1973 | Promoted Associate Professor, July — also led Paediatrics when needed |
| 1976 | Promoted Professor of Medicine, September |
| 1978 | Resigned, July — relieved of duties 14 September; aged forty-one |
| 1978 | Established private practice, Katni, Madhya Pradesh — one of the most trusted physicians in the town within years |
| 1998 | Killed in a road accident, 5 August, Katni — aged sixty-one; twenty years of practice there |
Dr. Ulhas Jajoo
MD General Medicine, GMC Nagpur

During his first year at Government Medical College in Nagpur, a seventeen-year-old Ulhas Jajoo was mercilessly ragged for wearing khadi. It was 1968. The fabric was crumpled, the cut was old-fashioned, and teenagers are rarely generous toward anything that marks a classmate as different. He endured the mockery for as long as he could bear it. Finally, defeated, he went to a shop and bought a white shirt and trousers in terrycot—synthetic, unremarkable, perfectly invisible.
He went home and told his father what he had done. His father listened quietly. Then he asked a single question: "How long will you allow fear to guide your path in life?"
Ulhas returned the terrycot clothes. He put the khadi back on. The ragging eventually stopped, as these things usually do. For the next fifty-eight years—through medical college, through his MD, and through a half-century career at MGIMS—he wore khadi every single day. He drove a simple scooter. He wore locally made chappals. He never owned a car. These choices were never a performance; they were simply the outward expression of a man who had decided, at seventeen, exactly who he was going to be.
Born on February 14, 1951, in Wardha, Ulhas was a brilliant student who placed tenth in the state matriculation examination. He was admitted to the Laxminarayan Institute of Technology (LIT) in Nagpur to study mathematics and engineering. He had found his subject. He was ready to begin.
Then, Dr. Ramchandra Wardekar, founder of the Gandhi Memorial Leprosy Foundation and a close family friend, came to visit. When Ulhas mentioned his engineering plans, Wardekar went quiet. He then revealed that his own path into medicine had been entirely shaped by Ulhas's grandfather, Shrikrishnadas Jajoo. The family possessed a deep history of healing that Ulhas had not inherited. Wardekar gently suggested that he should.
Ulhas confessed he was terrified of frogs and dissections. Wardekar assured him the fear would pass. Trusting the older man, Ulhas withdrew his admission from LIT, spent a year studying earthworms and cockroaches at JB Science College to conquer his squeamishness, and entered medical college in 1968. The fear of frogs did, in fact, pass.
He completed his MBBS in 1972 and his MD in general medicine shortly after. He chose internal medicine specifically because it could be practiced without heavy infrastructure, relying on nothing that was unavailable to the poor. Before joining any institution, he spent a month traveling across India to meet doctors who had chosen unconventional paths—Dr. Rajnikant Arole in Jamkhed, Harivallabh Parikh, and Narayan Desai. He needed to understand what a life in rural medicine actually looked like before he committed to it.
On April 26, 1977, he joined MGIMS as a Lecturer in Medicine.
Within a year of arriving, the twenty-seven-year-old Jajoo wrote a bold, four-page letter to Dr. Sushila Nayar. It outlined a radical vision for village healthcare, developed not in a library, but by riding a rented bicycle through monsoon rains to reach remote communities. Sitting in their homes, he had realized a fundamental truth: a villager's priority is their daughter's marriage, bank loans, and subsidized seeds—not their blood pressure.
He proposed a three-tier system: village health workers, a mobile health team, and the hospital. He advocated for community kitchens, people's courts, and cost-price medication. His central argument was revolutionary for a clinician: charity is insufficient; a community must be actively involved in its own health.
Dr. Nayar recognized something incredibly rare in the young man: a physician with the brilliant diagnostic instincts of a clinician, but the deep systemic convictions of a public health worker. She repeatedly tried to persuade him to take over the Department of Community Medicine. He politely declined. He believed that a strong foundation in curative internal medicine was essential to any credible public health work. He refused to leave the wards. Instead, he did both, holding curative medicine and village outreach in the same hand without ever finding the combination unusual.
He called his medical residents sherus—lions. And he meant it.
He taught at the bedside with the ease of a man for whom the ward, not the seminar room, was the natural location of truth. He physically crouched to the patient's level. He listened to the pauses in a patient's history just as closely as the words. He employed Socratic questioning—refusing to hand a student the answer before they had worked through the reasoning themselves. He visibly delighted in being proven wrong by a resident who had looked more carefully than he had.
Between 1984 and 2013, he guided thirty-eight MD students, researching the exact diseases ravaging rural Wardha: heart attacks, strokes, hypertension, and diabetes. His lectures drew students who had no obligation to attend, holding them spellbound for hours.
Year after year, on his February 14th birthday, tributes pour in from across the globe. What is striking about these accounts is what they omit. They rarely dwell on his diagnoses or publications. Instead, they consistently return to his professional ethics, his unbreakable character, and his profound way of simply being present with a suffering person. With Dr. Jajoo, the medicine was always inseparable from the man.
He resisted email for years. He avoided Twitter, Facebook, and WhatsApp. He preferred to write letters by hand on simple postcards. The scooter he rode was not a loud political statement against cars; it was simply what he had always used, and he saw no logical reason to replace it.
He spoke Hindi, Marathi, English, and Marwari, moving between the languages in a crowded room the way one moves between rooms in a beloved house. For more than two decades, he organized the Tapodhan Shree Krishndas Jajoo Smriti Karyakram, an annual gathering honoring unpublicized social service. Standing at the microphone in his white khadi, translating stories for the villagers, he was frequently moved to tears. He never tried to hide them.
When his parents entered their late eighties, he moved them into the familiar walls of their century-old family home. Alongside his brother Suhas, a plastic surgeon, he provided total care. Because he had never separated his role as a son from his role as a physician, the care was simultaneously filial and medical.
Having deeply absorbed the writings of Dr. Manu Kothari and Atul Gawande on mortality, he understood that how a person dies is as profound a medical question as any other. He arranged for his father, and later his mother, to die with absolute dignity at home, surrounded by family. They were not rushed to ICUs. They were not subjected to tubes and interventions that would have prolonged their dying rather than their living. As a master physician, he knew exactly what those interventions would entail. He consciously chose otherwise.
His legacy at MGIMS is deeply embedded. His wife, Kiran, taught school in Wardha, while his daughter, Namita, and son, Sumedh, both studied medicine at MGIMS and now work in the very department where their father spent his life.
On February 28, 2026, shortly after turning seventy-five, Dr. Ulhas Jajoo finally retired.
The students who passed through his unit are now the senior physicians shaping the next generation of Indian medicine. When they look back, they do not remember a specific paper or a complex technique. They remember a man in a crumpled khadi shirt, crouching at a villager's bedside, listening to the silence after a sentence ended, and asking the exact question that made them look again.
At seventeen, his father asked him how long he would allow fear to guide his path. He returned the terrycot clothes that day. And for the next fifty-eight years, he never stopped answering the question.
| 1951 | Born, 14 February, Wardha — grandfather Shrikrishnadas Jajoo, Gandhian, declined Chief Ministership of CP and Berar |
| 1967 | Placed tenth in state matriculation — Craddock High School, Wardha |
| 1967 | Admitted Laxminarayan Institute of Technology, Nagpur — mathematics |
| 1968 | Withdrew from LIT — Dr. Ramchandra Wardekar redirected him to medicine; entered GMC Nagpur |
| 1968 | Ragged for wearing khadi — bought terrycot clothes; father asked the question; returned them |
| 1972 | Completed MBBS, GMC Nagpur |
| 1976 | Completed MD General Medicine — chose internal medicine for its proximity to the poor |
| 1976 | Travelled India before joining any institution — met Dr. Rajnikant Arole, Harivallabh Parikh, Narayan Desai |
| 1977 | Joined MGIMS, 26 April — Lecturer in Medicine |
| 1978 | Four-page letter to Dr. Sushila Nayar, 16 September — vision for village healthcare; three-tier system proposed |
| 1984 | Began guiding MD students — 38 students over three decades |
| 2003 | Founded Tapodhan Shree Krishndas Jajoo Smriti Karyakram — annual gathering of people in unpublicised service |
| 2026 | Retired, 28 February — 17,840 days after joining; still in khadi, still on the scooter, until the last day |
A Clinico-epidemiological study of hypertension and coronary heart diseases in a rural community around Sevagram Vidarbha
Urine sugar as a tool for diagnosis and control of non insulin dependent diabetes mellitus ( NIDDM)
A clinical evaluation of prognostic factors of anti-tetanus Sclerotherapy in management of adult tetanus
Efficacy of clinical evaluation and role of radiography in the diagnosis of lower respiratory tract diseases
Clinical evaluation utility of fine needle aspiration biopsy as a diagnostic technique
The risk of cardiovascular. complication in patients under going major survey and its correlation with preoperative medical examination
Treadmill testing in asymptomatic subject with abnormal resting electrocardiogram
Correlations of bedside physical signs echocardiography in heart disease
Clinical profile of typhoid fever
An approach to patient of unexplained fever
Efficacy of clinical evaluation and role of chest radiography, ultrasonography in diagnosis and management of pleuritis
Clinical profile of complicated malaria in Kasturba hospital, Sevagram
Bed side prognostic factors in non traumatic adult patients admitted
Organizational aspects of medical intensive care unit at MGIMS Sevagram (an observational study )
Diagnostic approach for the patients of severe anemia in Kasturba Hospital Sevagram
Role of peripheral smear examination as a diagnostic tool, in the hands of medical residents ,in bedside evaluation of severe anemia
Bone – marrow examination in diagnosis of severe anemia
Detection of iron deficiency in cases of severe anemia
Study of indices indicating response to therapy in severe iron deficiency anemia
Evaluation of peripheral smear and culture indices in response to potential vitamin B12 and folic acid therapy in macrocytic anemia
Study of coulter indices in response to oral iron replacement and its comparison with parenteral iron therapy in severe iron deficiency
Evolving Bedside Diagnostic Approach to patients of Acute Onset Intracranial Neurodeficit, Stroke in particular
Study of profile of patients of megaloblastic anemia in rural population of central India
Clinical Profile of Complicated Malaria in Kasturba Hospital Sevagram
Utility of chest x- rays in the bedside diagnosis of acute pulmonary tuberculosis
Efficacy of Bedside Diagnostic Approach in Patients of Acute onset Intracranial Neurodeficit, particularly stroke: A prospective study
Correlation of Elevated ST Segment resolution and relief of Coronary Pain after Streptokinase in ST elevated Maiden Myocardial Infarction as a marker of Morbidity and Mortality
Drug Resistance Pattern in Bacillary and Bacillary (Radiologically diagnosed sputum-negative but culture-positive) Pulmonary Tuberculosis
Revisiting and Evolving Different Criteria to Differentiate between Transudative and Exudative effusions
Risk factor of Chronic Kidney Disease in Central Rural India
Prevalence of Hypertension in a Rural Community of Central india.
Prevalence of Diabetes Mellitus Type 2 in a Rural Population of Central india.
Total cholesterol, Triglycerides, Low density lipoprotein cholesterol and High density lipoprotein cholesterol as risk factor in Coronary Artery Disease in individuals above 60 years of age, in rural community of central India – A case control study
Prevalence of coronary artery disease in individuals above 60 years in rural community of Central India
Diagnostic accuracy of ADA in serous effusions.
Diagnostic accuracy of a drop hydrogen peroxide test to differentiate exudative and transudative pleural effusion
Prevalence of Nephropathy among adults in Central Rural India screened by proteinuria
Prevalence of metabolic syndrome and its risk factors among rural adult population (Age > 35 years) in central India
Dr. Vivek Wamanrao Poflee
MD General Medicine, IGMC Nagpur (1983)

In 1978, a twenty-four-year-old Vivek Poflee had topped Medicine in his final MBBS examinations. He had successfully secured a highly coveted seat in the MD program at IGMC Nagpur, placing himself within reasonable distance of the secure, prestigious career his family expected and he had worked relentlessly toward.
Then, he took a hard look at the man running his department. He saw a Head of Department who spent his energy cultivating political connections, who remained entirely indifferent to patients, and who valued self-promotion above teaching—making genuine learning the absolute last priority in a place where it should have been the first.
Poflee watched this for as long as his conscience allowed. And then, he walked out.
"Madness," said some. "Reckless," said others. But he resigned anyway. This pattern—of deliberately leaving a situation that was working adequately on paper because the conditions for integrity had been compromised in practice—would recur in his career. It defined him far more precisely than any medical credential ever could.
He was born on August 1, 1954, in Nagpur. His father, Dr. Wamanrao Poflee, was a medical officer in the State Medical Services. His mother, Sumati, had been a brilliant student who chose instead to raise children deeply curious about how the world functioned. The household naturally produced scientists, engineers, economists, and doctors.
Young Vivek absorbed an early and permanent obsession with the mechanics of the physical world. He spent hours in his bedroom and at Somalwar High School building call bells, buzzers, and wireless transmitters, much to the amusement—and occasional alarm—of his family. His instinct was always for tinkering, for taking a system completely apart to understand it, and then reassembling it better than it had been before.
Medicine entered his life as the natural next step from a household where healing was present and his own aptitude for science was undeniably clear. He entered IGMC Nagpur in 1971, topped his MBBS in 1975, and secured his MD seat in 1978. Then came the resignation.
What followed was a masterclass in self-sufficiency. Rather than navigating the politics of the Indian academic system, he went to Baghdad in January 1979. He spent two years in Iraq—moving through Quadhmia Republic Hospital, Balad Republic Hospital, and Mahmood Hospital—practicing medicine in a foreign landscape, far from the institutional support that makes clinical work comfortable. When he returned to India, he bought a friend's dispensary, set up a private practice, and quietly rebuilt a life that worked.
Three years after walking away, with merit finally restored to the department, he reapplied to the MD program. This time, he trained under Dr. P.Y. Deshmukh—a man of genuine intellectual seriousness, precisely the thing his previous supervisor had not been. He completed his MD in 1983. In September 1984, he joined MGIMS in Sevagram.
He arrived at a Department of Medicine already in formidable formation. The unit in the mid-1980s stood, as he later described it, on four massive pillars: Dr. O.P. Gupta, Dr. A.P. Jain, Dr. Ulhas Jajoo, and Dr. S.P. Kalantri. Each was a complete physician in the manner the institution demanded—holding clinical, teaching, and research commitments simultaneously without apparent strain. Poflee found his place within this structure not by replicating what the others were doing, but by bringing exactly what they lacked.
He gravitated toward clinical neurophysiology—EEGs, EMG, and nerve conduction studies. It was a field resting at the precise intersection of neurology and physics, requiring the kind of patient, systematic attention to electromechanical data that suited his engineering temperament perfectly. After training at NIMHANS in Bangalore and CIIMS in Nagpur, he returned to MGIMS and established the neurophysiology clinic—a facility that had not existed before his arrival.
His most widely noticed contribution, however, was the Hand Mill Test. It began with a straightforward clinical roadblock: some patients requiring coronary evaluation could not walk on a treadmill due to severe knee arthritis or muscular conditions. The standard stress test was therefore impossible.
Poflee, channeling the boy who built wireless transmitters, took a stationary exercise bicycle, modified one of its pedals, and bolted the entire metal frame to a concrete platform so patients could crank the machine with their hands instead of their legs. He tested it with a cardiologist in Nagpur, then replicated it at MGIMS. A Medicine resident, Dr. Sanjeev Batra, wrote his thesis on the comparative results. Soon, engineering students from nearby institutions began seeking out the MGIMS doctor who physically built his own diagnostic equipment. He welcomed them all.
He had played the guitar for years, though the brutal demands of medicine had gradually displaced the music. At MGIMS, Gajanan Ambulkar—an artist by temperament and training—persuaded him to pick it up again.
A small, beautiful ensemble formed: Poflee on guitar, Dr. S. John Premendran on violin, and Dr. R.K. Gupta from Pharmacology on flute. When Mrs. Kamala Desikan invited them to perform at the college's Silver Jubilee, they played a patriotic musical program to an audience of faculty and students. It was the kind of magical occasion that small institutions, when they are functioning well, generate entirely without effort—people with separate, hidden skills discovering that they could produce something beautiful together.
He left MGIMS in April 1992. He was not unhappy; he was simply honest. The four pillars of the Medicine department were firmly rooted where they had always been, and there was absolutely no upward movement available for a fifth person of his seniority. He named this reality clearly, rather than constructing a more flattering, diplomatic account of his departure.
In 1992, he joined Jawaharlal Nehru Medical College in Sawangi as Professor and Head of Medicine. The college was only two years old and desperately needed someone to build it from nothing. He did exactly that, eventually extending his reach into the roles of Medical Superintendent and Dean.
And then, he resigned again.
Administration was not the work he had come into medicine to do. The endless files, the bureaucratic meetings, the institutional politics—they were pulling him away from the patients and the teaching. In 1994, he returned to Nagpur, resumed private practice, and continued clinical neurophysiology at SureTech Hospital, deliberately ensuring his services remained available to patients who could not pay.
In 2005, a profound tragedy struck. An autoimmune vasculitis rapidly took his hearing in both ears. But the tinkerer simply adapted. He did not retire. He continued his work as a neurophysiologist in total silence.
He and his wife, Sandhya, were among the very first doctors in Nagpur to drive an electric car—first the Reva, then the Comet. The choice was deeply consistent with a sensibility that had always been drawn to how complex systems worked, and what those systems cost the world they operated within.
He delivered health talks on All India Radio. He conducted workshops on the cybernetic principles of business management. In 2021, he published a book of devotional songs he had composed and set to music himself. His interests were too vast to be reduced to mere hobbies; they were the natural expression of a mind that simply refused to observe the usual, artificial partition between the scientific and the spiritual.
His son Hrishikesh, born in Sevagram in 1986, studied computer science, moved to the United States, joined the US Army as a cybersecurity specialist, and married Dr. Teja Mehendale, a family physician from Pune. The invisible connections between what MGIMS produced and the wider world run, in his case, across a generation and an ocean.
Vivek Poflee walked away from his first MD when a supervisor made integrity impossible. He walked away from a Deanship when administration made medicine impossible. Both decisions required him to actively discard something highly valuable—time, position, the path of least resistance—in order to preserve something he valued far more. Neither departure was made in anger. Both were made with wide-open eyes.
The Hand Mill he built is still used. The neurophysiology clinic he established at MGIMS continued to serve patients long after he left. At seventy, he remains a working neurophysiologist in Nagpur, completely at peace with the knowledge that he has fulfilled his calling.
The tinkerer who built wireless transmitters in his childhood bedroom never actually became a different person. He simply found a field large enough to contain him.
| 1954 | Born, 1 August, Nagpur — father Dr. Wamanrao Poflee, State Medical Services |
| 1971 | Entered IGMC Nagpur |
| 1975 | Completed MBBS — topped in Medicine |
| 1978 | Resigned from MD programme, IGMC — supervisor indifferent to patients and to teaching |
| 1979 | Baghdad — Quadhmia Republic Hospital, Balad Republic Hospital, Mahmood Hospital |
| 1981 | Returned India — private practice; reapplied to MD under Dr. P.Y. Deshmukh |
| 1983 | Completed MD General Medicine, IGMC Nagpur |
| 1984 | Joined MGIMS, 19 September — Associate Professor of Medicine |
| 1986 | Son Hrishikesh born, Sevagram |
| 1987 | ICMR fellowship — NIMHANS Bangalore under Dr. M. Gourie Devi; Bombay Hospital; CIIMS Nagpur |
| 1987 | Established neurophysiology clinic at MGIMS — first in Sevagram |
| 1989 | Invented Hand Mill Test — modified stationary bicycle for patients unable to use treadmill |
| 1992 | Left MGIMS, 12 April — joined JNMC Sawangi as Professor, Head, Medical Superintendent, Dean |
| 1994 | Resigned from JNMC — administration displacing patients and teaching; returned to Nagpur |
| 2005 | Autoimmune vasculitis — lost hearing in both ears; continued as neurophysiologist |
| 2021 | Published book of devotional songs — composed and set to music |
Comparative study of treadmill hand mill in the evaluation of patient of ischemic heart disease
Dr. Karunakar Trivedi
MS Surgery, MGM Medical College Indore (1963)
It did. Karunakar Trivedi became a surgeon, a Department Head, a Medical Superintendent, and an elite cardiac surgeon trained in Cleveland and New York. He became a man who performed highly complex mitral valve surgeries in a bare-bones rural teaching hospital in Vidarbha, relying on a nurse named Alice and a technician named Rama Rao Ugale to help hold the operation together.
His mother offered her prayers to the Narmada. The vow was kept.
The inheritance that shaped him was far more profound than just a nickname.
His father, Kashinath, had met Mahatma Gandhi in 1925, immediately left his teaching career, became the joint editor of Navjivan, and dedicated himself entirely to the Nai Talim (Basic Education) movement in Sevagram. His mother, Kalavati, had faced brutal lathi charges in protest, led fierce agitations against liquor shops, and answered Gandhi's call for personal satyagraha in Ajmer. She was sentenced to three months in prison—while pregnant with her first child.
The Trivedi family had lived in the Sabarmati and Sevagram ashrams alongside Gandhi, Kasturba, Sardar Patel, Vinoba Bhave, and Jayaprakash Narayan. Kalavati had taken Sanskrit lessons inside the ashram and learned how to ride a bicycle—taught personally by Bapu himself.
Into this extraordinary family, and in this highly specific place, Karunakar was born on April 29, 1938.
He was educated in Indore and entered MGM Medical College in 1955, completing his MS in Surgery in 1963. During his clinical rotations, cardiothoracic surgery captured his imagination completely: the meticulous craftsmanship required in the operating room, and the terrifying, unforgiving precision demanded by the human heart and its chambers.
He longed for advanced training in the United States. In a time before the internet flattened distances, he relied on instinct and persistence—poring over thick hospital directories, sending applications into the unknown, and preparing for the demanding ECFMG examinations. One acceptance led to another: a surgical residency at Norwalk Hospital, followed by advanced cardiac training at the Lahey Clinic in Boston between 1967 and 1968. Each step widened his horizon and sharpened his craft.
When he returned to India, the country itself seemed to be in the midst of building anew. He joined the newly established medical college in Raipur, but his journey was already being quietly redirected.
A few months earlier, in March 1970, Dr. Sushila Nayar had written to Shri Shyama Charan Shukla, then Chief Minister of Madhya Pradesh, requesting that Dr. Trivedi be deputed to the fledgling medical college in Sevagram. As a Member of Parliament who knew Shukla well, her word carried weight. The request was accepted.
Once she realised that she could use her influence to write directly to chief ministers and senior officials, she began to do so with purpose and regularity. It became one of her most effective ways of building the institution—one letter at a time. Through such interventions, Dr. Prabhat Kumar Acharya was deputed as a dermatologist to MGIMS in July 1972, following a letter from Shri Prakash Chandra Sethi, then Chief Minister of Madhya Pradesh. Years later, in 1978, Dr. H. N. Khattri was similarly deputed from PGI Chandigarh.
And so, in August 1970, he arrived at MGIMS as a Reader in Surgery—among its very first clinical teachers, at a time when even the inaugural batch of students had yet to set foot on campus. The institution was still an idea taking shape; he would help give it form.
The invitation to Sevagram had come after Karunakar visited the campus, walked the empty wards, observed what was there (and what was missing), and confided his deep doubts to Dr. Wardekar. Dr. Wardekar asked a simple, piercing question: "You're thirty-seven—don't you want to explore, take on new challenges, and truly live?" By morning, Karunakar and his wife had decided. Sevagram would be their home.
He had married Dr. Mrudula Naik on May 26, 1969. She was a gifted obstetrician. Their fathers had arranged the union, they had worked in the same hospital as interns and registrars, and now they would build their careers in the exact same rural institution—she heading Obstetrics and Gynaecology, he Surgery. A Gandhian family twice over, joined in both marriage and service.
Dr. and Mrs. Trivedi were among the very first clinical teachers at MGIMS. Kasturba Hospital was then a deeply modest fifteen-bed facility, run by compounders holding training certificates personally signed by Gandhi.
Dr. Trivedi was promoted to Associate Professor in July 1971. As the hospital began to expand, he took on the additional responsibility of Medical Superintendent and plunged into the demanding task of building a department of surgery from the ground up.
There was nothing to inherit—only space, need, and resolve. He helped set up operating theatres, equipped wards, and trained students who often had to assist in surgeries simply because there were no house officers yet. Learning and service unfolded side by side, each necessity shaping the other.
Beyond the hospital, he led large rural surgical camps where, over a few intense days, more than a hundred procedures were performed. Even now, after more than five decades, those days return to him with striking clarity. He recalls working alongside Dr. Anant Damodar Ranade—an Ayurvedic physician by training, not an ophthalmologist—who performed cataract surgeries in villages around Sevagram. Together, they operated tirelessly, sharing skills, improvising when needed, and responding to an overwhelming burden of untreated disease
Then, completely without warning or consultation, the management appointed Dr. Raj Kumar—an impeccably credentialed double FRCS—as Head of the Department, abruptly replacing him.
There was no discussion. There was no explanation. It was a brutal decision made entirely behind closed doors. It was not that Dr. Raj Kumar was unqualified; he was superbly qualified. What stung was the sheer manner of the act—a dedicated captain replaced mid-series without being told, without even the chance to respond. Dr. Trivedi wrestled with the humiliation for days. In June 1972, with a heavy heart, he left Sevagram and returned to Madhya Pradesh.
He returned to thoracic surgery at MGM Medical College in Indore. He successfully performed closed-heart procedures, including mitral valve surgery. But he knew, with the harsh self-assessment of a master craftsman, that he needed more formal training to perform the work at the elite level he demanded of himself.
He was accepted for a highly coveted cardiac surgery residency at St. Vincent Charity Hospital in Cleveland, Ohio, under Dr. Earl B. Kay—a legendary pioneer who had developed the Kay-Suzuki valve prosthesis. He then moved to St. Francis Hospital in New York for pediatric cardiac surgery. When he finally returned to India, he was an entirely different surgeon—not just technically, but in his absolute confidence and clarity of purpose.
In 1976, Dr. Sushila Nayar was visiting her niece in Long Island, New York. One quiet evening, reflecting on the past, she asked a question: Would Dr. Trivedi and his wife ever consider returning to Sevagram?
Time had softened the old, bitter wounds. The Emergency had upended lives across India; several Trivedi family members had been imprisoned, and their government positions revoked. The future was terrifyingly uncertain. Dr. Nayar's offer felt like both an opportunity and a deeply needed homecoming. The Trivedis agreed.
In September 1977, Dr. Trivedi returned to MGIMS as Professor and Head of Surgery, and Medical Superintendent—his simultaneous reinstatement serving as a clear, institutional signal that his initial departure had been a massive mistake. He returned older, and considerably more skilled. Cleveland and New York had armed him with cardiac surgery capabilities at a level that Sevagram had never previously seen.
He rebuilt what needed rebuilding. Equipment was relentlessly procured until the operating theatres could actually support his ambitions. He performed closed mitral valve surgeries, pericardiectomies, and hydatid cyst removals. Alice, the first staff nurse to assist in Sevagram's cardiac surgery, and Ram Rao Ugale, the OT technician with preternaturally steady hands, became the human infrastructure of something genuinely pioneering.
His leadership was soon tested. A resident who had won his postgraduate seat through a bitter court order returned to Sevagram hoping to begin afresh. The hospital management, deeply stung by their legal defeat, spitefully denied him married accommodation and assigned him a room in the boys' hostel instead. The grievance was undeniably real, and it caught fire.
Residents organized. Demands rapidly accumulated. And then, in an act that shocked many who intimately knew the man, an effigy of Dr. Trivedi—the Medical Superintendent—was burned on campus.
He remained completely calm. He absolutely refused to retaliate. He simply kept the hospital running and ensured the patients were cared for. Weeks passed. Tempers finally cooled. And then, one by one, handwritten letters of profound apology began arriving on his desk—acknowledging his integrity, expressing deep remorse, and recognizing the ugliness of what had been done. The strike ended not in a triumphant crushing of the residents, but in genuine reconciliation. They had found their way back through the sheer clarity of his restraint.
But leadership always extracts a heavy price. As Medical Superintendent, he had upheld discipline in ways that inevitably created distance. Colleagues who had once shared easy camaraderie became cautious; conversations grew measured.
By early 1984, a new administrative order abruptly downgraded the Medical Superintendent's position without consultation, eroding the autonomy he had painstakingly built and trusted. His famous candor, once deeply valued by the institution, had begun to discomfort those newly in power. Whispers replaced the respect that had once been genuine.
He requested to be relieved in 1983. The resignation was not accepted. He stayed until he simply could not remain without compromising his own self-respect. On June 15, 1984, wearing simple khadi, he walked away from Sevagram for the last time.
Returning to Indore, he joined a charitable trust hospital and spent the next four decades performing surgeries that far exceeded in number what Sevagram had ever required. He stepped down from administration in 2008 but continues as an honorary consultant to this day, operating three days a week at an age when most surgeons have long since put down the scalpel.
In 1998, Dr. Sushila Nayar appointed him as a trustee of the Kasturba Gandhi National Memorial Trust in Indore. By 2016, he became its Chairperson.
His children flourished globally: Rajshree as a pediatric intensive care specialist in Australia; Anita with a master's in design building a career at Thomson Reuters; and Apoorv, an IIM graduate managing portfolios in Singapore.
The family that had carried its son through a Gandhian ashram childhood—through nights sitting with Gandhi, Patel, and Vinoba; through his mother's prison sentence and his father's dedication to Basic Education—had produced a master surgeon. He performed cardiac operations in a rural teaching hospital, endured displacement, returned in triumph, endured displacement again, and continued operating into his eighties.
His mother had offered her prayers to the Narmada. She had been absolutely right to do so.
| 1938 | Born, 29 April, Wardha — father Kashinath joint editor of Navjivan; mother Kalavati imprisoned while pregnant with first child |
| 1955 | Entered MGM Medical College, Indore |
| 1963 | Completed MS Surgery |
| 1967 | Surgical residency, Norwalk Hospital, USA |
| 1967 | Advanced cardiac training, Lahey Clinic, Boston — until 1968 |
| 1969 | Married Dr. Mrudula Naik, 26 May — obstetrician; would head OBG at MGIMS |
| 1970 | Joined MGIMS, August — Reader in Surgery; among first clinical teachers |
| 1971 | Promoted Associate Professor, July — Medical Superintendent |
| 1972 | Left MGIMS — replaced as Head of Surgery without consultation; returned to Madhya Pradesh |
| 1973 | Cardiac surgery residency, St. Vincent Charity Hospital, Cleveland — under Dr. Earl B. Kay |
| 1975 | Paediatric cardiac surgery, St. Francis Hospital, New York |
| 1977 | Returned MGIMS, September — Professor and Head of Surgery; Medical Superintendent |
| 1984 | Left MGIMS, 15 June — walked away in khadi after administrative autonomy was eroded |
| 1984 | Joined charitable trust hospital, Indore — four decades of surgery |
| 1998 | Appointed trustee, Kasturba Gandhi National Memorial Trust, Indore — by Dr. Sushila Nayar |
| 2008 | Stepped down from administration — continued as honorary consultant |
| 2016 | Chairperson, Kasturba Gandhi National Memorial Trust |
A clinical study of surgical manifestation of filariasis
A clinical study of post operative wounds
To study the prevalence of surgical diseases in rural population around Sevagram
A Clinicopathological study of the effect of hydrocele on spermatogenesis
Dr. Raj Kumar
FRCS Edinburgh (1959) · FRCS London (1959)
In 1947, a young Raj Kumar was diligently preparing for his twelfth-grade Zoology examination in Lahore when the brutal reality of Partition arrived. His family had anticipated the violence and managed to move ahead to Ambala.
Then came a specifically cruel addition to the general catastrophe: his college principal, who had bravely returned to Lahore to collect the students' examination papers, was killed in the raging riots. The documents were entirely destroyed. Raj Kumar, instead of sitting his examination and moving forward, was forced to retake the entire grueling year.
He did not lose hope. He emerged as a top student, secured admission to the inaugural class of the newly established Amritsar Medical College in 1947, and spent the next decade building a surgical career that would take him across the globe. By the time he arrived in Sevagram in June 1972 to build a surgery department from absolute nothing, he was forty-one years old, possessed a double FRCS, and had already survived far more disruption than most careers encompass in a lifetime.
The story of the Partition examination is told at the beginning because it establishes something essential about his character: this was a man who treated devastating setbacks merely as the next problem to be solved, rather than the end of the road. He would need that exact quality in Sevagram, though for very different reasons.
Raj Kumar was born on December 12, 1930, in Gujranwala, an hour's drive from Lahore, where his father served in the British Army. He deliberately dropped his surname—Chopra—as an Arya Samaji practice that he maintained fiercely throughout his entire life.
At Amritsar Medical College, his classmates included Dr. Jagdev Singh Guleria (later a renowned cardiologist) and Dr. Panangipalli Venugopal (the eminent cardiac surgeon). He obtained his MBBS in September 1953. During this period, he played football and aggressively boxed, representing the medical college in state tournaments. That physical confidence and competitiveness would remain highly visible in his clinical manner throughout his career.
He began as a house surgeon in Amritsar in 1954, worked in orthopaedic surgery in Delhi in 1956, and then made the massive leap to England.
He spent nearly a decade training across the United Kingdom's finest, most demanding surgical institutions: pediatric surgery at Royal Manchester Children's Hospital and Great Ormond Street Hospital; thoracic surgery at Brompton Hospital in London and Alder Hey Hospital in Liverpool. He obtained his FRCS from Edinburgh in March 1959 and from London in May 1959, qualifying in both within a staggering two-month window. He had established himself as a consultant surgeon of genuine, undeniable standing.
In 1962, the call of home prevailed. He returned to India as a Pool Officer in Surgery at AIIMS, New Delhi. After another brief stint in London, he caught the attention of Dr. Santokh Singh Anand and joined PGIMER in Chandigarh as an Assistant Professor in 1965. His elite surgical expertise, forged across the hospitals of northern England, was now being actively applied to build India's premier postgraduate medical center.
In 1968, he made a highly unexpected move. He had successfully treated a sick newborn at PGIMER, deeply impressing the child's father—who happened to have the power to envision a full hospital for the massive Bhilai Steel Plant in central India. Dr. Raj Kumar helped make that vision a reality. The double FRCS from Edinburgh and London was now administering heavy-duty industrial healthcare to steelworkers in Chhattisgarh. He was nothing if not adaptable.
Dr. Sushila Nayar had been treated by Dr. Raj Kumar at PGIMER. Remembering his brilliant hands, she invited him to Sevagram to build a surgery department from scratch. He came on deputation from the Bhilai Steel Plant—a strategically sensible arrangement that offered both the surgeon and the rural institute a safety net if the match failed.
He arrived on June 1, 1972, with a monthly salary of ₹2,250.
The transition was, by his own frank admission, intensely difficult. Sevagram's established code of conduct—mandatory khadi, strict vegetarianism, absolute prohibition of alcohol—was utterly foreign to a man shaped by a Punjabi upbringing, British surgical training, and the rough culture of a steel township. The language was unfamiliar. The food was unfamiliar. The fierce Gandhian austerity was a massive, daily adjustment.
What he found in the Surgery department was equally challenging. There was no postgraduate program, no resident doctors, and notoriously high turnover. With 110 beds split between Kasturba Hospital and the Wardha District Hospital, the monthly workload ran to around eight major and sixteen minor surgeries—a microscopic volume by his standards.
He built what he could within these crushing constraints. He conducted theory classes and bedside clinics with the relentless commitment of a man who had trained at Great Ormond Street and believed medical education should look exactly like that.
His examination standards were notoriously high and rigidly consistent. In 1975, only fifteen of twenty-six surgery students managed to pass under his scrutiny. When a student from a highly influential family failed, heavy administrative pressure arrived from above demanding the boy be passed. Dr. Raj Kumar flatly refused. His counter-argument was surgically precise: If this student is to pass, then every other student who failed must also be passed. The administrative pressure instantly dissolved. The fairness held.
In the sun-drenched Sevagram of the early 1970s, he was entirely distinctive. Tall, handsome, with salt-and-pepper hair and expressive eyes behind spectacles, he carried himself with the quiet, unshakeable confidence of someone who had survived Brompton Hospital and was therefore not particularly intimidated by rural administrative friction. An Arya Samaji who shunned idol worship, he nonetheless appeared every Tuesday at the local Hanuman temple to recite the Hanuman Chalisa softly. His devotion was simple and entirely his own.
He and his wife, Anjana—a gifted classical musician from Delhi—lived in Guru Nanak Colony. Anjana ran the cooperative store in Sevagram and taught nursery children with patient attention. Their home constantly echoed with the deep resonance of a tanpura and the voices of their two sons, Shiv and Gautam.
The boys experienced a magical Sevagram childhood, scaling the massive jackfruit tree in their backyard and watching local snake charmers catch cobras with daring ease. Shiv would go on to become a successful laparoscopic surgeon in Delhi, while Gautam completed IIT and IIM to settle in Mumbai. The surgeon's sons carried the immense discipline their father had modeled, successfully applying it to different fields.
Four years in, the profound cultural tensions between Dr. Raj Kumar's formation and Sevagram's strict code became irresolvable. The khadi, the vegetarianism, the prohibition—these things had never truly become comfortable for him. On July 31, 1976, just a few months past his forty-sixth birthday, he resigned.
He returned briefly to Bhilai, secured voluntary retirement from the Steel Plant, and moved to Delhi. At Holy Family Hospital, he served for nearly three decades. It was the long, stable second act of a career that had already included Britain's finest surgical centers, AIIMS, PGIMER, and the grueling, foundational years of MGIMS.
He died peacefully in his sleep at his Delhi home on June 25, 2019, at the age of eighty-nine. Those who knew him reported that he remained sharp and deeply committed to his values until the very end.
He was the man who had rebuilt his life after the Partition riots destroyed his exams, who had adapted to more institutional cultures than most surgeons encounter in three lifetimes, and who had flatly refused to pass an influential student. His Sevagram years were only four out of eighty-nine, but they were difficult, vital years that produced something incredibly durable: a Surgery department where none had existed, built to standards that a double FRCS considered acceptable.
The jackfruit tree is gone now. The snake charmers have vanished. Anjana's tanpura fell silent years before the end. But what remains in Sevagram is a functioning surgical department, and the lingering memory of an examination standard that was applied without the slightest regard for who was asking for an exception.
| 1930 | Born, 12 December, Gujranwala — father served in British Army; dropped surname Chopra as Arya Samaji practice |
| 1947 | Partition — examination papers destroyed in Lahore riots; forced to retake the year |
| 1947 | Admitted to inaugural class, Amritsar Medical College — classmates included Dr. P. Venugopal and Dr. J.S. Guleria |
| 1953 | Completed MBBS, September |
| 1954 | House surgeon, Amritsar |
| 1956 | Orthopaedic surgery, Delhi — then moved to United Kingdom |
| 1956 | Training — Royal Manchester Children’s Hospital, Great Ormond Street, Brompton Hospital London, Alder Hey Liverpool |
| 1959 | FRCS Edinburgh, March · FRCS London, May — both within two months |
| 1962 | Returned India — Pool Officer in Surgery, AIIMS New Delhi |
| 1965 | Assistant Professor, PGIMER Chandigarh — under Dr. Santokh Singh Anand |
| 1968 | Joined Bhilai Steel Plant Hospital, Chhattisgarh |
| 1972 | Arrived MGIMS, 1 June — on deputation from Bhilai Steel Plant; salary ₹2,250 |
| 1975 | Refused to pass influential student who had failed — administrative pressure dissolved |
| 1976 | Resigned, 31 July — returned to Bhilai, then moved to Delhi |
| 1976 | Joined Holy Family Hospital, Delhi — served nearly three decades |
| 2019 | Died peacefully in his sleep, 25 June, Delhi — aged eighty-nine |
Dr. Ravinder Narang
MS General Surgery, PGI Chandigarh (1969)
He had almost left on the very evening he arrived.
The Dakshin Express had pulled into Wardha East station well past dusk. The platform was dimly lit and uninviting. The mosquitoes on the hostel terrace were relentless. The breakfast at the local hotel the next morning was entirely tasteless. The hospital itself was a quiet, bare-bones village institution, possessing absolutely nothing of the kinetic energy of Chandigarh or Delhi. By the following afternoon, Dr. Ravinder Narang had firmly decided: one day was enough. He packed his bags and walked back toward Wardha East station, determined to board the first train back to Delhi.
He was stopped—twice.
First by Dr. Dhawan, who mentioned that the Head of Surgery, Dr. Raj Kumar, wanted to see him before he left. Narang flatly refused the meeting and boarded the train anyway. Then, a week later, Dr. Raj Kumar actually tracked him down in Delhi and made the case directly: Give it a few months. After that, the choice is entirely yours.
Caught between his initial doubt and an inexplicable pull he could not quite name, Dr. Narang sighed and agreed. He returned to Sevagram in June 1973.
He finally left on December 1, 2020—exactly 17,280 days later.
Ravinder Narang was born on December 7, 1940, in Sargodha, Punjab (now in Pakistan). His father was a doctor. Watching his father endure the long hours, the heavy sacrifices, and the particular toll of a life surrendered to other people's emergencies gave young Ravinder deep pause when considering medicine for himself. In 1947, when he was seven, the extreme violence of Partition forced his family to flee Sargodha with only what they could carry. They began again in Ludhiana, alongside hundreds of thousands of displaced families across the bleeding subcontinent.
He attended Arya Samaj High School, proved bright and intensely curious, and eventually set his sights on medicine. He quickly discovered, however, that Dayanand Medical School required five years' tuition paid upfront—a sum his refugee family simply could not produce. He applied to the new Medical College at Rohtak and found himself 114th on the waitlist. He applied to Christian Medical College, Ludhiana, and was rejected. Defeated, he enrolled in a BSc Honours program at Punjab University in Chandigarh, actively arranging his mind for a completely different future.
Three months later, the Rohtak waitlist miraculously cleared. He enrolled immediately, completing his first three years at Medical College, Patiala (where the program had temporarily relocated) before returning to Rohtak. He graduated with his MBBS in 1965. The boy who had spent three months languishing on a waitlist and studying general science had arrived at his medical degree by the longest possible route.
He desperately wanted Internal Medicine for his postgraduate training—he felt it was his true calling—but the seat slipped away. Settling, he chose ophthalmology at PGI Chandigarh. He spent his days sitting in the dim darkness of an examination room, peering through an ophthalmoscope at the narrow, restricted world of the eye. The silence and confinement gnawed at him. "I needed more than just the eye," he would say later. "I needed the whole patient."
He switched to the MS Surgery course, viewing it at the time merely as a necessary stepping stone toward the orthopaedics he truly wanted. Instead, he discovered something profound inside the general operating theatre: a rhythm of precision and absolute purpose that settled the question permanently. In 1969, he earned his MS in General Surgery from PGI Chandigarh under Dr. I.C. Pathak. He would carry Pathak's central aphorism for the rest of his career: "Work with young minds and you'll stay young at heart. A medical school is where you'll find that energy."
From 1969 to 1973, he served as a resident at AIIMS Delhi, training under Dr. Atma Prakash and Dr. B.M.L. Kapur—two of the sharpest surgical minds of the era. It was Dr. Kapur who, when the residency concluded, explicitly suggested he look at Sevagram.
He joined the Department of Surgery on June 1, 1973. It was a department experiencing constant, turbulent transition: Dr. Raj Kumar was at the helm on temporary deputation from the Bhilai Steel Plant, Dr. Karunakar Trivedi had recently departed for Madhya Pradesh, and multiple colleagues were on study leave or in flux.
He adapted. He settled into his role, took charge of the sports section of the student association, and became part of the small, fiercely close-knit faculty community.
When Dr. Raj Kumar departed in July 1976, Dr. Narang stepped up as Department Head. A year later, Dr. Karunakar Trivedi returned in triumph and reclaimed the captaincy. Dr. Narang simply stepped back, continued operating, continued building, and waited. (In 1979, sheer frustration prompted him to apply to BYL Nair Hospital in Mumbai. An offer came through, but housing in Mumbai proved impossible to arrange, and the plan dissolved).
When Dr. Trivedi finally left for good in June 1984, Dr. Narang was asked to lead once more. He accepted. He led the Surgery department continuously for the next two decades, until his retirement in 2005.
His areas of particular mastery were thyroid surgery, parotid surgery, and urology—specifically kidney malignancies and complex stone surgeries of the kidney and ureter. He approached severe abdominal cases with the steady hands and unshakeable judgment of someone who had been operating in a resource-constrained environment long enough to develop techniques uniquely appropriate to that reality. In a rural hospital where what was actually available was rarely what the textbooks assumed, he found ways to make things work.
"I always had a passion for urology," he liked to joke. "I left no stone unturned—not just in my career, but literally, with kidney and ureter stone surgeries."
In 1992, a WHO fellowship took him to the University of California Los Angeles (UCLA), the Mayo Clinic, and the Royal Marsden Hospital. He absorbed exposure to the world's finest, most technologically advanced surgical centers, brought that knowledge back to Sevagram, and successfully applied it within Sevagram's strict constraints.
He fiercely believed in human senses over the machine. "A CT scan or ultrasound gives images," he told his students regularly, "but it's the human touch and connection with the patient that reveal what machines cannot." He was notoriously strict at the bedside and in the theatre—instilling discipline through the heavy pressure of someone who held the standard incredibly high. Yet, he consistently returned the conversation to kindness and empathy the moment the technical instruction was complete. "A good surgeon is never arrogant or difficult. We heal the body and care for those who place their trust in us."
Between 1982 and 2009, he mentored thirty-four MS thesis students, guiding young surgeons until he was sixty-five with the consistency of a man who understood that this was the entire point of being in a teaching hospital.
Between 1990 and 2000, he served simultaneously as Medical Superintendent. He waded through the mountain of paperwork, the complex regulations, the employee disputes, the endless bills, and the brutal procurement of equipment. Crucially, he managed it all while continuing to see outpatients and perform the most difficult surgeries the department faced. The operating room was where his joy lived, and he flatly refused to let administration displace it.
He had dreamed for years of becoming the Dean of MGIMS—the highest institutional achievement available, and the position toward which his entire career seemed to be pointing. But when it finally came within reach, he looked at it with absolute clarity: endless paperwork, strict regulatory rules, and the grinding, daily management of budgets and politicians.
His heart was simply not there. He voluntarily stepped back from the Dean's office and returned to the operating room and the classroom. The dream had shifted. The joy remained.
In the winter of 2020, he walked out of his outpatient clinic for the final time as Emeritus Professor of Surgery. His wife joined him silently as he passed through the corridors he had walked continuously since 1973.
His wife, Dr. Pratibha Narang, had joined MGIMS on the exact same day in 1973 as its first Microbiology lecturer. She had built that department from nothing while he built Surgery. She had gone with him to the Wardha East station on the day he almost left, and she had returned with him when Dr. Raj Kumar persuaded him to come back. Their careers at MGIMS ran in perfect parallel for nearly fifty years: two departments, one campus, one incredibly long commitment.
He had come to Sevagram wanting Internal Medicine, tried Ophthalmology, aimed for Orthopaedics, found General Surgery instead, and spent five decades with it. It was not the fiery romance of first choices, but the deepening, unbreakable bond of a commitment made and kept—the kind of constancy that outlasts passion and becomes something infinitely more reliable.
His mentor Dr. Pathak had told him that a medical school was where young minds would keep his passion alive. He had believed it fully enough to return from the train platform when a man found him in Delhi and said: Give it a few months. The months became forty-seven years. The years became the foundation of a surgery department, thirty-four MS graduates, countless thyroid and kidney operations, and a legacy that will outlast them all.
| 1940 | Born, 7 December, Sargodha, Punjab (now Pakistan) |
| 1947 | Partition — family left Sargodha; began again in Ludhiana |
| 1958 | Applied to Medical College Rohtak — 114th on the waitlist; enrolled BSc Honours, Punjab University, Chandigarh |
| 1958 | Rohtak waitlist cleared — enrolled immediately; first three years at Medical College, Patiala |
| 1965 | Completed MBBS, Medical College, Rohtak |
| 1969 | Completed MS General Surgery, PGI Chandigarh — under Dr. I.C. Pathak |
| 1969 | Resident, AIIMS Delhi — under Dr. Atma Prakash and Dr. B.M.L. Kapur |
| 1973 | Arrived MGIMS, 10 August — almost left the next day; persuaded back by Dr. Raj Kumar |
| 1976 | Acting Head of Surgery — when Dr. Raj Kumar departed |
| 1984 | Head of Surgery — led department for two decades |
| 1990 | Medical Superintendent — managed simultaneously with surgery and teaching until 2000 |
| 1992 | WHO Fellowship — University of Los Angeles, Mayo Clinic, Royal Marsden Hospital |
| 2005 | Retired as Professor and Head — continued as Emeritus Professor |
| 2020 | Left MGIMS, 1 December — 17,280 days after the almost-departure |
A profile of anaerobic infections in surgical patients
Effect of surgery and anesthesia on serum immunoglobulin (IgG, IgM) levels and their clinical correlations
Lymphadenopathy-a clinical ,histopathological bacteriological study
Evaluation of serum copper as a diagnostic and prognostic indicator in malignancies
Splenic autotransplantation : an experimental study in rats
A clinical study of fistula-in-ano
Diagnostic value of vasography in male sterility
Acute appendicitis : a Clinico bacteriological study
A study of burns at MGIMS, Sevagram
Diagnostic value of ultrasound in detection of scrotal pathologies
Correlation of symptoms of upper gastrointestinal tract with endoscopically detectable lesions
Effect of Transcutaneous electrical nerve stimulation on survival of ischemic myocutaneous flap : an experimental study in rats
Application of revised trauma score injury severity score and TRISS methods to predict the outcome of polytrauma patients
Evaluation of postprandial urinary alkaline tide in management of duodenal ulcer
Plasma selenium level in cancer patients
Procapicstic Profile in Septicemia
Study of catheter induced urinary tract infections in hospital patients
Clinicopathological study of thyromegaly and diagnostic value of Fine Needle Aspiration Cytology
Benign prostatic hyperplasia (BPH): Clinical profile and comparative study of transurethral resection of prostatic with Freyer’s open prostatectomy
Comparative study of the prevalence of the surgical conditions in a rural base tertiary hospital rural community
Clinical biochemical bacteriological study of urolithiasis
Clinical profile of Breast cancer evaluation and diagnostic value of bone marrow examination in distant metastasis
Acute abdominal emergencies : retrospective and prospective clinical review of ten years
Correlation of clinical laboratory parameters in the diagnosis of tubercular lymphadenitis
Clinico-radiological study of stricture urethra
A study of postoperative wound infections, sepsis and risk factors in a rural teaching hospital
Blunt abdominal trauma: retrospective prospective review of ten years
Clinical study of burns with retrospective and prospective review of mortality factors
Evaluation of risk factors for diabetic foot in diabetic population
Pattern of gastrointestinal malignancies : retrospective prospective review of ten years
Diagnostic role of ultrasonography in the detection of scrotal pathologies
Non mesh vs.mesh repair of inguinal hernia and its impact on clinical outcome and quality of life
A clinical study of hydatid disease – a retrospective and prospective study
Comparative Study of Pattern of Head Injury in a Tertiary Care Hospital and a Rural Community Hospital
Comparative Study of Pattern of Acute Abdomen in a Tertiary Care Hospital and in a Rural Community Hospital
Evaluation of rapid diagnostic test (RDT) against indirect immunofluorescence assay (IIA) and polymerase chain reaction (PCR) for diagnosis of scrub typhus in central India.
Dr. Ramdas Kisan Belsare
Diploma in Orthopaedics, College of Physicians and Surgeons Bombay (1969)
MS General Surgery, Bombay University (1971)

He had trained as a general surgeon. He held a prestigious MS in General Surgery from Bombay University. What he had in orthopaedics, however, was merely a diploma from the College of Physicians and Surgeons—a perfectly respectable qualification, but hardly the credential one would normally associate with heading a major medical department.
And yet, for the better part of a decade, Dr. Ramdas Kisan Belsare was the de facto Head of Orthopaedics at MGIMS. This happened not by grand design, and certainly not by ruthless ambition, but by the sheer logic of circumstance that Sevagram repeatedly applied to the people it needed most.
The sequence was characteristically Sevagram. Dr. S.C. Ahuja, the actual Reader in Orthopaedics, abruptly left for a two-year deputation to Iran. The department was entirely empty. The hospital administration turned to Dr. Belsare and asked him to simply hold the fort. He agreed, with the quiet, unshakeable practicality that defined absolutely everything he did.
He settled into the role. He became exceptionally good at it. When Dr. Ahuja eventually returned from Iran, Dr. Belsare was understandably reluctant to step aside—he had built something real in the department and did not feel finished building it. Gentle persuasion and careful diplomatic nudging eventually convinced him to return to general surgery, his original domain. Then, within a short span, both protagonists left: Dr. Ahuja in 1981, and Dr. Belsare in 1982, leaving the department to begin another grueling cycle of rebuilding.
He had never sought orthopaedics. He had not even particularly wanted general surgery—his true aspiration had been thoracic surgery, which the management had bluntly declined to offer him. He simply accepted what was available, applied himself completely, and left something highly durable behind. This was his pattern throughout his entire life.
Ramdas Kisan Belsare was born on March 14, 1937, in Talegaon Thakur, a dusty village near Guru Kunj in the Amravati district. His father, Krishnrao, was a farmer. His early education took place entirely within the village and the local district before he entered Government Medical College (GMC), Nagpur, in 1960, graduating with his MBBS in 1965.
He was not content to stop there. He pursued his Diploma in Orthopaedics in Bombay in 1969, and his MS in General Surgery from Bombay University in 1971. The training years that preceded these hard-won qualifications were accumulated across the busiest, most chaotic hospitals Bombay could offer: a house surgeon at GMC Nagpur; a registrar in orthopaedics at MGM Medical College; a casualty medical officer at BYL Nair Hospital; and three grueling years as a surgical registrar in the massive Group of TB Hospitals in Bombay.
Each post was another layer of raw clinical competence deposited quietly, without fanfare, upon the last.
He joined MGIMS on March 1, 1971, as a Lecturer in Surgery. He had wanted thoracic surgery; he was offered general surgery. He accepted the compromise and immediately went to work.
Dr. Sushila Nayar had understood very early that recruiting top-tier faculty to Sevagram—a village with severely limited amenities, located a considerable distance from the urban professional centers where young doctors built their careers—required a strategy far beyond mere newspaper advertisements.
Her solution was elegant and ruthless: hire couples. A surgeon and his wife, an anatomist. A pediatrician and her husband, an ENT surgeon. Two investments in two departments, one single recruitment conversation, and crucially, two people who were infinitely less likely to uproot and leave because each partner's presence securely anchored the other.
The Belsares were among these brilliant paired appointments. Dr. R.K. Belsare in Surgery, and Mrs. Belsare in Anatomy. Together, they gave MGIMS a solid decade. The campus that took shape in the 1970s was a community literally assembled couple by couple: the Chaturvedis, the Narangs, the Ahujas, the Trivedis, the Hariharans, and the Dhawans. Dr. Nayar had built a faculty that was simultaneously a neighborhood—a neighborhood that held itself together through shared purpose and the sheer practical difficulty of both partners leaving simultaneously.
The Belsares lived within this community, raised their children in it, and were deeply shaped by it. Their younger daughter, Sukanya, was born in Sevagram—one of the "campus children" whose earliest memories were of the campus itself.
He had grown up in rural Amravati, and he carried the deep formation of that upbringing directly into his clinical practice in ways that profoundly mattered to his patients.
He spoke Marathi with a distinct regional slang—a raw dialect that felt instantly familiar and deeply comforting to the terrified villagers who came to Kasturba Hospital seeking care. With a wad of tobacco and lime casually tucked under his lip (a habit from his rural roots), he would listen to them. He listened with the particular, focused attention of someone who understood not just what the patient was saying, but exactly what they were not saying: the unspoken fears, the brutal economic constraints that dictated what treatment was actually possible, and the dignity concerns that sometimes prevented rural people from describing their symptoms fully.
He cut through medical jargon with the confidence of someone who thought jargon was entirely beside the point. There were no unnecessary investigations, and no elaborate, theoretical explanations that would have been completely opaque to a farmer who had traveled several hours on a bus just to sit in his clinic. He offered practical, cost-effective solutions that actually fit the difficult lives of the people sitting in front of him. He knew exactly why they had come and exactly what they could afford, and he oriented his entire practice around those two facts.
This quality—of meeting patients exactly where they were—was not a clinical technique he had learned in Bombay. It was a pure expression of where he himself had come from. The dusty lanes of Talegaon Thakur, the farmer father, the education assembled piece by piece—these were not a background he had left behind. They were the very source of his clinical instinct.
In December 1975, when the vacancy in Orthopaedics was most acute and no suitable candidate was forthcoming, he wrote a simple letter to the Principal offering to step in as Reader in Orthopaedics until the position could be properly filled. It was a highly practical solution; Dr. Nayar instantly approved it.
Under his unexpected leadership in Orthopaedics, the Indian Council of Medical Research (ICMR) actively selected MGIMS for a pioneering national study on pediatric disability prevention and rehabilitation. This was not a minor recognition—it signaled to the entire country that a rural department run by a general surgeon holding only an orthopedics diploma was producing research of sufficient quality to attract premier national funding. His unique ability to blend high-volume clinical service with strict academic rigor had made the department highly visible to the ICMR.
When Dr. Ahuja resigned again in 1981, leaving the department leaderless once more, Dr. Belsare calmly absorbed the massive responsibility yet again, taking charge as Professor and Head until he finally departed Sevagram in November 1982.
He left Sevagram for Amravati, joining the district hospital as a surgeon while simultaneously building a thriving private practice. He worked at the district hospital until 1988, and then spent two and a half decades in private practice until 2016. He became a deeply trusted, familiar figure in Amravati's medical circles; his steady hands and quiet, unshakeable confidence earned the continued loyalty of patients who had come to him across a career spanning five decades.
And then, Parkinson's disease arrived.
The master hands that had wielded the scalpel with such flawless precision began to tremble violently. Dementia slowly followed, cruelly dimming the sharp, pragmatic mind that had successfully navigated the complexities of two distinct surgical specialties. Confined to bed in his final years, he bore his devastating illness with the exact same silent, uncomplaining fortitude that had characterized his response to every single circumstance in his life that had not gone as planned—the thoracic surgery that was never offered, the orthopedics department that arrived by accident, the departure he accepted when the moment finally came.
On May 26, 2019, at the age of eighty-two, he died in Amravati.
His legacy multiplied. His elder daughter, Sharmishtha, married a surgeon and became an ENT specialist in Amravati. His younger daughter, Sukanya—born in Sevagram—trained as a computer engineer and eventually found a radically different calling in spirituality; she is now based in San Francisco as a Spiritual Teacher, carrying her father's quiet purposefulness in an entirely different register. His son, Chaitanya, earned a PhD in fruit science. Mrs. Belsare, the brilliant anatomist who had been the "other half" of Dr. Nayar's strategic hiring calculation, had been steadfastly beside him through all of it.
He had arrived in Sevagram desperately wanting to do thoracic surgery. He had been handed general surgery instead. He had been asked to fill in for orthopedics, became exceptionally good at it, was asked to give it back, returned to general surgery, and simply left when the moment came. At no point in his life had he ever made a fuss.
The tobacco and lime under his lip, the Amravati Marathi slang, the rural patients who trusted him implicitly because he spoke their exact language—these things were who he truly was. Dr. Ramdas Kisan Belsare had never needed the institution's formal titles to tell him so.
| 1937 | Born, 14 March, Talegaon Thakur, Amravati district — father Krishnrao, farmer |
| 1960 | Entered Government Medical College, Nagpur |
| 1965 | Completed MBBS, GMC Nagpur — house surgeon, Surgery and Orthopaedics; registrar, MGM Bombay; casualty MO, BYL Nair Hospital; surgical registrar, Group of TB Hospitals Bombay |
| 1969 | Diploma in Orthopaedics, College of Physicians and Surgeons, Bombay |
| 1971 | Completed MS General Surgery, Bombay University |
| 1971 | Joined MGIMS, 1 March — Lecturer in Surgery; had wanted thoracic surgery, accepted general surgery |
| 1975 | Wrote to Principal volunteering to cover Orthopaedics — promoted Reader in Orthopaedic Surgery, 30 December |
| 1977 | ICMR selected MGIMS for paediatric disability prevention and rehabilitation study, September — under his leadership in Orthopaedics |
| 1981 | Dr. Ahuja resigned — absorbed departmental leadership again as Professor and Head |
| 1982 | Left MGIMS, November — joined Amravati district hospital as surgeon; simultaneous private practice |
| 1988 | Left district hospital — private practice in Amravati until 2016 |
| 2019 | Died, 26 May, Amravati — aged eighty-two; Parkinson’s disease and dementia in final years |
Dr. Wasant Keshav Belokar
MS General Surgery, AIIMS Delhi (1969)
MCh Urology, AIIMS Delhi (1975)
On his official Maharashtra Medical Services application form, right beneath the bureaucratic question asking whether he had more than one wife, Dr. W.K. Belokar wrote: "Married (have only one wife)."
This tiny detail—the incredibly dry humor of a highly precise man finding a quiet outlet in tedious paperwork—captures something absolutely essential about him. He was deeply reserved, not particularly expressive, and generally a man of very few words who preferred to let his surgical outcomes speak on his behalf.
But beneath that quiet surface, there was a sharp wit that found its moments, and a profound care for people that expressed itself in actions rather than declarations. For example, returning to Sevagram a full year after his resignation solely to sign a panicking student's thesis, crossing the massive distance between Goa and Maharashtra just to ensure that one piece of unfinished business was honorably completed.
And then, of course, there was the prostate that got stuck in the ceiling light. But that comes later.
Wasant Keshav Belokar was born on March 23, 1940, in Khamgaon, in the Buldhana district of Maharashtra. He attended Government High School and Science College in Khamgaon, acing his matriculation in 1957 with rare distinctions in Physics and Chemistry. When he completed his pre-professional studies, he ranked fourth on the entire Nagpur University merit list—a clear, early signal of the fierce academic seriousness that would carry him through everything that followed.
He joined Government Medical College, Nagpur, in 1959 and graduated with his MBBS in 1964. His early clinical years took him grinding through the Nagpur Medical College Hospital, the district hospital in Amravati, and a rural center at Saoner. Stints as a house officer in General Surgery and ENT refined his raw surgical instincts. Then, in 1966, a brutal All-India selection process earned him a highly coveted postgraduate residency at AIIMS, Delhi—the institution that would shape his surgical identity most completely.
He trained as a surgical resident at AIIMS from 1966 to 1969, earning his MS in Surgery under Professor Atma Prakash (the exact same legendary mentor who had taught Dr. Ravinder Narang). His deep interest in urology took root during this period. The kidney, the ureter, the prostate—he was drawn to the particular demands of a biological system that connected the incredibly precise with the highly mechanical in ways that rewarded both technical skill and immense patience.
In June 1970, while still completing his AIIMS registrarship, he applied for a Lecturer's position at MGIMS. He was selected and officially appointed on July 4, 1970.
There was only one problem: the Surgery department had not yet been formally established.
And so, he began his tenure sitting in the Anatomy department, waiting. Principal Dr. I.D. Singh wrote to assure him that Surgery would soon be introduced. Meanwhile, Professor Atma Prakash wrote to the Principal on his student's behalf with characteristic warmth: "Dr. W.K. Belokar is one of my dearest students. He is brilliant, hardworking, and will bring credit to your institution."
Administrative delays required him to wait for another doctor's departure before he could formally take up his surgical role. He waited with the unshakeable patience of someone who had learned that the right moment eventually arrives. On October 15, 1971, he finally joined MGIMS as a Lecturer in Surgery.
Two years in, hungry for greater specialization, he secured study leave to pursue his MCh in Urology at AIIMS. He completed the brutal training on his first attempt and returned to MGIMS in July 1975. Promoted to Reader, he eventually established a separate Urology Division at MGIMS in November 1980, becoming its first head under Professor K.K. Trivedi.
From Khamgaon to GMC Nagpur to building a specialized urology division in a rural teaching hospital in Vidarbha, he had accumulated his clinical competence piece by piece, each step quietly building upon the last.
Inside the operating theatre, Dr. Belokar had a highly particular, slightly dangerous celebratory habit: whenever a difficult prostatectomy was successfully completed, he would toss the removed prostate high into the air in a moment of sheer surgical triumph. It was a seasoned juggler's gesture, expressing in the only available physical language the deep satisfaction of work flawlessly done.
One day, the toss went wrong.
The prostate shot upward with far more force than anticipated and lodged itself firmly inside the surgical ceiling light. The theatre staff scrambled frantically to retrieve it, fighting a losing battle to maintain their professional composure. Dr. Belokar remained completely unfazed, continuing his postoperative work as if absolutely nothing unusual had happened.
He also famously kept his transistor radio playing during operations—one ear attending to the patient's kidney, the other listening intently to Kapil Dev's bowling figures. He saw no contradiction whatsoever. "On a rainy day," he would explain to baffled students, "as I tried to negotiate the dilator through the uneven urethra, I was taken by surprise—much like a batsman facing Kapil's late outswinger!" Both disciplines demanded immense skill, fine control, and the ability to instantly read the pitch—whether that pitch was the human urinary tract or the Feroz Shah Kotla stadium in November. He delivered running cricket commentary as he operated, blending the surgical with the sporting in a way that made the theatre feel like a place of both extreme precision and joyful anticipation.
His praise for students was incredibly rare, and therefore deeply meaningful. "I will give you an MBBS degree straight from my pocket," he would announce when genuinely impressed by a student's performance in examinations. Those who heard it knew they had done something truly worth noting.
When Dr. Belokar resigned to move to Goa in December 1982, he left behind exactly one piece of unfinished business: a student named Abhoy Kumar Sinha. Abhoy was the only MD candidate he had guided, and his complex thesis on the urological manifestations of leprosy was still a year away from completion.
When the departure came with data collection incomplete, Abhoy Kumar faced a terrifying series of compounding administrative problems: Who would sign his work? How would he satisfy the department? How would he convince the university? And without a signed thesis, could he sit his final examinations at all? The questions were not rhetorical; they actively threatened his ability to complete his medical degree.
A full year after his departure, Dr. Belokar suddenly reappeared in Sevagram. He had traveled all the way from Goa for one specific reason: to sign the thesis. With a single stroke of his pen, he cleared every bureaucratic obstacle, validating his student's work and permanently securing his future. And then, he simply returned to Goa.
This is exactly the kind of act that never appears on a curriculum vitae. It required only the quiet decision to travel back to honor a commitment made before circumstances changed. Dr. Belokar made the decision without apparent deliberation, because the obligation to the student was clear, and for him, that was entirely sufficient.
He joined Goa Medical College as Professor of Surgery on December 6, 1982. By January 1994, he had risen to become Dean—leading the institution with the exact same quiet authority that had defined his surgical career. He served on the Goa Medical Council, and eventually on the Medical Council of India, contributing to the regulation of medical education at a national level.
He subsequently served as Director of Urology at hospitals in Sawangi and Nepal. The career that had started in the dusty village classrooms of Khamgaon had extended across multiple prestigious institutions and national governing bodies.
Those who received his official correspondence often noted that he was possessed of an impossibly elegant, calligraphic handwriting—a genuine joy to read in an era when most documents were handwritten, and the quality of the hand still said something profound about the quality of the mind.
He died in 2020. What he had established at Sevagram—the Urology Division, the exacting surgical standards, the elite MCh training he brought back from AIIMS and applied to a rural teaching hospital—remained permanently intact.
As did the prostate, which was presumably eventually retrieved from the ceiling light, properly labeled, and sent to pathology without further incident.
| 1940 | Born, 23 March, Khamgaon, Buldhana district, Maharashtra |
| 1957 | Matriculation with distinctions in Physics and Chemistry — fourth in Nagpur University merit list at pre-professional stage |
| 1959 | Entered Government Medical College, Nagpur |
| 1964 | Completed MBBS, GMC Nagpur — house officer, General Surgery and ENT |
| 1966 | All India selection — surgical residency, AIIMS Delhi under Professor Atma Prakash |
| 1969 | Completed MS General Surgery, AIIMS — continued as surgery registrar until September 1971 |
| 1970 | Appointed MGIMS, 4 July — placed in Anatomy while awaiting Surgery department establishment |
| 1971 | Joined Surgery as Lecturer, 15 October |
| 1975 | Completed MCh Urology, AIIMS under Professor M.S.M. Singh — thesis on kidney stone disease; returned MGIMS 1 July |
| 1975 | Promoted Reader, 1 August — Warner Hindustan Travelling Fellowship; visited urology centres in Madras, Vellore, and Bombay |
| 1980 | Established Urology Division, MGIMS, November — first head under Professor K.K. Trivedi |
| 1982 | Left MGIMS, 1 December — joined Goa Medical College as Professor of Surgery, 6 December |
| 1983 | Returned to Sevagram — signed Abhoy Kumar Sinha’s thesis; cleared every obstacle to his degree; returned to Goa |
| 1993 | Member, Goa Medical Council; later served on Medical Council of India |
| 1994 | Dean, Goa Medical College, January |
| 2020 | Died — the same year Dr. Ravinder Narang retired from MGIMS |
Genitourinary manifestations in leprosy
Dr. Virendra Kumar Mehta
MBBS, MGM Medical College Indore (1966)
MS General Surgery, MGM Medical College Indore (1969)

He could not afford a bicycle in Bhopal. When he arrived in Sevagram and finally started earning a steady salary, he bought one. And then he rode it through the campus for twenty-five years, long after his colleagues had upgraded to scooters and cars.
The bicycle was never an affectation or a performance of austerity. It was simply who he was: a man who had discovered that simplicity was not a sacrifice, but a profound form of freedom. He saw absolutely no reason to abandon it just because academic promotion and seniority had offered him the conventional alternatives.
He addressed his colleagues and his medical residents alike as Shriman—Sir. He rigorously avoided parties, skipped the cinema, and rarely, if ever, spoke of his own achievements. He did not laugh easily, did not publicly display sorrow, did not celebrate victories, and never performed his grief. He dressed his patients' wounds personally in the surgical ward at two in the morning—not because the resident on call was unavailable, but because the patient sitting in front of him needed it done, and he happened to be there.
These things were not empty gestures. They were the highly consistent expressions of someone who had decided very early in life what actually mattered, and who had found absolutely no reason to revise that decision across a quarter-century of surgical practice in a Gandhian village.
Virendra Kumar Mehta was born on October 24, 1942, in Mandsaur, Madhya Pradesh. His father, Shri Sajjanlal Mehta, was a first-class LLB graduate who never practiced law simply because his own mother believed he would be forced to be dishonest in a courtroom. Instead, he became a grain merchant. The household was orthodox Jain; the values were clear, rigid, and highly consistent.
Young Virendra attended school in Mandsaur, pursued a BSc at Holkar College in Indore, and entered MGM Medical College in 1961.
When asked why he chose medicine, he never offered a general, soaring aspiration. He answered with a single, sharp memory: when he was a small child, his grandfather had died simply for lack of medical care. That was the reason.
He graduated with his MBBS in 1966, ranking seventh on the final merit list. He completed his house jobs in Surgery and returned to MGM for his MS in Surgery from 1967 to 1969. During his residency in Indore, he met Jyoti, a nurse from Kerala. After a quiet five-year courtship, they married in 1971. His orthodox Jain family fiercely opposed the union—Jyoti was Christian—but Virendra stood absolutely firm. Holding his ground in the face of intense family opposition was entirely consistent with everything that followed: he was a man who knew his own mind and refused to be deflected by social pressure.
In Bhopal, they built a stable life. They secured a government quarter in Idgah Hills. Their two children, Manoj and Sonali, were born there. They had good schools and the comfortable amenities of a city. And then Dr. K.K. Trivedi, who was actively building the Surgery department at MGIMS, invited him to Sevagram.
On March 14, 1978, he arrived.
He arrived as a Lecturer, became a Reader in 1981, and was promoted to Professor in December 1995. The titles marked the administrative passage of time, but they failed to capture the specific quality of his daily presence that made him the doctor he was.
In the operating theatre, Dr. Narang—who led the Surgery department for most of Dr. Mehta's tenure—described him as reserved, small, and slender. He was entirely content to support rather than lead, vastly preferring to let his actions speak. This assessment was fiercely accurate. Dr. Mehta never sought the spotlight. He sought only the patient.
Between 1985 and 2004, he mentored twenty-four surgery residents, investing in each of them with the painstaking thoroughness of a man who understood that teaching was simply a form of patient care extended into the future. He built incredibly strong relationships with the nursing staff, valuing their bedside experience in ways that resident doctors sometimes failed to do. This mutual respect naturally produced a highly efficient, deeply patient-centered ward environment.
He believed fiercely in cost-effective, humane surgery. Aligning himself with Dr. N.H. Antia's vision—accessible surgery for patients who simply could not afford market rates—he contributed heavily to the Association of Rural Surgeons of India's (ARSI) manual of rural surgery.
The ARSI's core position, which he endorsed without a single reservation, was that rural surgery was not about second-rate surgeons providing second-rate care to second-rate citizens. It was about providing the absolute best possible care within the severe constraints of what rural patients could actually afford, and what rural settings could actually sustain.
He was highly skeptical of market-driven healthcare—the creeping commercialization that prioritized revenue over clinical need. He was equally skeptical of the reflexive adoption of new surgical technologies in settings where the latest innovation was not actually the most appropriate choice. (He could occasionally be resistant to new technologies beyond what was strictly warranted, a limitation that those who worked alongside him freely acknowledged). But his underlying conviction was unshakeable: in a rural hospital serving farmers who had traveled considerable distances with limited resources, the only question that mattered was what was affordable, effective, and genuinely beneficial—not what was newest.
He also served as the chief editor of the MGIMS annual reports from 1995 to 1999, and edited the Journal of Rural Surgery—administrative contributions that reflected his deep seriousness about documentation and the institutional life of the campus.
Jyoti Mehta served as a nursing supervisor at Kasturba Hospital for over a decade. The nurse from Kerala who had become the Jain grain merchant's daughter-in-law against the family's wishes had made Sevagram her home with the exact same quiet determination that had brought her there. At Christmas, she warmly welcomed guests with sweets and gifts, her gentle hospitality serving as the perfect counterpoint to her husband's reserved, monastic solitude.
On January 24, 2000, she died in Sevagram after a brutal battle with breast cancer. She had been diagnosed and treated in the exact same hospital where her husband practiced surgery.
It was the kind of devastating loss that those who do not show emotion publicly must absorb in the only way available to them: by continuing, without any visible alteration, the daily work that had always been the center of their universe. He continued to ride his bicycle. He continued to dress wounds at two in the morning. He continued to respectfully call his colleagues Shriman.
Their son, Manoj, graduated from MGIMS in 1990 and specialized in Ophthalmology. Their daughter, Sonali, graduated in 1991 and pursued Obstetrics and Gynaecology. Both had been educated in Sevagram at Kasturba Vidya Mandir, on the exact same campus where their parents had built their careers. The fierce instinct toward medicine that had been ignited in Virendra by his grandfather's tragic death had moved, through him and Jyoti, safely into the next generation.
He left Sevagram for Ujjain in October 2003. He had been there for twenty-five years—longer than almost anyone in the Surgery department other than Dr. Narang. He had operated relentlessly, taught twenty-four residents, edited two publications, dressed thousands of wounds in the dark, and ridden his bicycle through the campus in the early morning while the rest of the faculty was still asleep or backing their cars out of their garages.
He had not been able to afford a bicycle in Bhopal. In Sevagram, he bought one and kept it for a quarter of a century. As those who watched him understood, it was far more than transport. It was the daily, physical expression of a philosophy: that the gap between what is strictly necessary and what is merely comfortable is rarely worth filling. That simplicity is not deprivation, but precision. And that a man who has decided what actually matters can spend twenty-five years doing exactly that, without ever needing the other things.
His grandfather had died for lack of medical care. He had gone into medicine because of that unnecessary death. And he had spent his entire career ensuring that the patients who arrived at his ward—whatever hour they arrived, and whatever the terrible condition of their wounds—received from him the exact same careful, deeply personal attention that his grandfather had never received from anyone.
| 1942 | Born, 24 October, Mandsaur, Madhya Pradesh — Jain household; father a grain merchant, first-class LLB who chose not to practise law |
| 1961 | Entered MGM Medical College, Indore — chose medicine because his grandfather had died for lack of care |
| 1966 | Completed MBBS, MGM Indore — seventh on merit list |
| 1969 | Completed MS General Surgery, MGM Indore — trained under Dr. S.D. Sharma, Dr. A.M. Ghooi, and Dr. Hissamuddin |
| 1971 | Married Jyoti — nurse from Kerala; family opposed the union; he stood firm |
| 1978 | Arrived MGIMS, 14 March — Lecturer in Surgery; bought his first bicycle |
| 1981 | Promoted Reader, February |
| 1985 | Began mentoring surgery residents — twenty-four students between 1985 and 2004 |
| 1995 | Promoted Associate Professor, September; Professor, December |
| 1995 | Chief editor, MGIMS annual reports — until 1999; also edited Journal of Rural Surgery |
| 2000 | Jyoti died, 24 January — breast cancer; diagnosed at Kasturba Hospital where she had served as nursing supervisor |
| 2003 | Retired and left for Ujjain, 9 October — twenty-five years after arriving; still riding the same bicycle |
A comparative study of biological dressing (placentas) conventional dressing thermal burns
Changes in coagulation system and SDPS test following surgical operations
Effect of hydrocele surgery on spermatogenesis
A clinical profile of head injury cases with gastric acid secretory pattern studies in selected cases
Sclerotherapy for hydrocele using oxytetracycline
Primary closure in acute abscesses.
Clinical evaluation of aqueous extract of human placenta in treatment of non healing wounds
Effect of antineoplastic drugs on wound strength in : an experimental study
Evaluation and clinical correlation of serum amylase in acute abdominal conditions in rural population
An experiment study of intestinal anastomosis in rats using an internal stent
Prevalence of anorectal diseases in rural population
Effect of topical application of phenytoin in different wound
Correlation of Clinico radiological findings with operative or USG findings in rural population
Fila test in surgical manifestation of filariasis
Clinico-immunological correlations of surgical filariasis
Antibiotic prophylaxis in wound infection : an experimental study
Clinico-immunological monitoring of patients of lymphatic filariasis on extended DEC treatment
The effect of neem ointment in wound healing
Comparative study of aloederm ointment with neem cream with sesame oil conventional dressings in wound healing
Prospective retrospective Clinicopathological study of tuberculosis as seen in rural based institution
Changing Clinicopathological trends in acute appendicitis as seen in rural based institution of Vidarbha
Trends in hernia : rural experiences
Pyocele : A rural experience
Trends in trauma : A rural experience
Trends in peritonitis – A rural experience
Dr. Kiran Kher
MBBS, Pandit Jawaharlal Nehru Memorial Medical College Raipur (1973)
MS General Surgery, PJNMMC Raipur (1977)

The clerk at the Dean's office told him flatly that there was no vacancy, and none foreseeable.
Kiran Kher thanked him politely, walked away, and began wandering through the hospital. He noticed the nameboard outside Dr. K.K. Trivedi's office. Summoning his courage, he simply knocked, walked in, and explained that he wanted to join the Surgery department.
Dr. Trivedi listened quietly, nodded once, and told him to get his luggage ready. "Join us in two days."
This is exactly how his MGIMS career began—not through the formal, bureaucratic channel that had just turned him away, but through a direct appeal to the right person, made possible only by his willingness to knock on an unfamiliar door. It was entirely characteristic of the man.
He had deliberately chosen Sevagram over a comfortable government service posting because colleagues spoke highly of its integrity. He had already seen more than enough in Madhya Pradesh's medical colleges—professors bluntly refusing to see poor patients unless they were paid for private consultations, the rich receiving fawning attention while the destitute died unattended in public wards. He understood early that the way medicine was practiced mattered just as much as the medicine itself. He wanted to be in a place where it was practiced properly. So, he got his luggage ready.
Kiran Kumar Kher was born on February 24, 1951. His father, Shri Shrikant Vinayak Kher, was a regional bank manager who was frequently transferred across Madhya Pradesh. Despite the constant relocations, Kiran's family ensured he spent his entire schooling in Raipur, providing him with vital stability. He attended Hindi-medium schools, sitting cross-legged on tat pattis (coir mats) with his classmates, learning under the strict, elemental teaching methods of the era.
In the ninth grade, he made a deliberate, consequential choice: Biology over Mathematics. He understood exactly what he was doing. The Mathematics door was closing; the Medicine door was opening. He completed his pre-medical studies at Ravishankar University in 1968 and earned his MBBS from Pandit Jawaharlal Nehru Memorial Medical College in 1973.
Surgery had begun to deeply fascinate him during his final MBBS year. He carefully studied the way surgeons moved through the hospital—a quiet, unshakeable confidence in the corridors, crisp white coats, and steady hands that held a scalpel without any visible effort. As an intern, whenever he found a spare moment, he would slip into operating theatres uninvited, just to watch. He was not performing enthusiasm for his superiors; he was genuinely, entirely absorbed.
He completed his MS in General Surgery at his alma mater in 1977. His thesis—a clinicopathological study of cervical lymphadenopathy—reflected the highly methodical approach that would come to characterize his entire surgical career.
His house officer salary had been ₹350 per month. As a postgraduate student, ₹533. As a registrar, ₹675. The money was never the point. The hands-on experience was the point, accumulated patiently, year by year, until he was ready for whatever came next.
He arrived at MGIMS on July 2, 1979, as a Lecturer in Surgery. He was a bachelor.
The first floor of the Surgery department housed a small group of young, unmarried doctors who had improvised a secret kitchen in direct defiance of institutional convention. Someone rolled the chapatis. Someone else managed the dal and rice in a steam cooker. Dinner was shared every night with a deep camaraderie that softened the brutal edges of their exhausting days. The kitchen was carefully, desperately concealed from the administration.
One day, Dr. Sushila Nayar found it.
She was absolutely furious. The young lecturers stood their ground and made their case: the local hotel food was unhygienic, there was no community mess available to them, and they simply could not afford to eat out every single day on their modest salaries. The logic held. Dr. Nayar, recognizing reason when she heard it, relented. The kitchen stayed.
His closest friends in those years were Dr. Ulhas Jajoo, Dr. Ramakant Tiwari, and Dr. Panchauli. They were young, unmarried, and still finding their feet in Sevagram, bound together by shared surgical emergencies and late-night conversations. Their communal meals cost less than ₹100 a month. Forty years later, he still recalled that illicit kitchen with the particular fondness of someone who understands that simplicity and sufficiency are not the same thing as deprivation.
He married Praveena Moharikar in 1980—a brilliant postgraduate student in Ophthalmology. They became another of Sevagram's famous "paired appointments," two specialists building their careers in the exact same institution, anchored to each other and therefore deeply anchored to the place.
He worked primarily in Dr. Trivedi's unit, managing a demanding surgical workload: 140 lectures per year, forty-two weeks of bedside postings, and a grueling OR schedule that included mitral valvotomies, hydatid cyst removals, laparotomies, and thyroidectomies.
In 1982, an unusual administrative incident marked a turning point in the department. On a single day, several junior faculty members—including Dr. Ulhas Jajoo, Dr. V.K. Mehta, and Dr. Kiran Kher—were unexpectedly granted postgraduate "guide" status without having applied for it. Once the circumstances became clear, the reason proved to be administrative rather than meritocratic: an influential staff member's daughter urgently needed a postgraduate seat, and to legally secure it for her, all eligible faculty were designated as guides simultaneously.
While the grant of guide status had arrived in a highly irregular manner, Dr. Kher used it straightforwardly and honorably. He supervised two postgraduate students, one of whom—Santosh Prabhu—went on to become a distinguished neurosurgeon.
In the theatre and at the bedside, Dr. Kher was a stark contrast to the loud, boastful stereotype of the surgeon. He was of slight build, wore glasses, and remained perpetually calm and thoughtful. He chose his words carefully. His soft voice was never raised in disagreement. His gentle manner made terrified patients feel instantly at ease—a quality of presence that functions very differently from commanding authority, but is no less effective in a ward environment. He was promoted to Reader in February 1984.
By 1985, harsh financial reality had settled in. Faculty salaries at MGIMS were exceedingly modest—considerably below what urban counterparts were earning. He had observed that professional prestige in the world outside Sevagram was deeply entangled with financial success in ways that he could no longer entirely dismiss. He decided it was time to leave and build a private practice in Wardha.
He prepared for his departure with the exact same practical thoroughness he brought to the operating table. In private practice, a surgeon often had to serve as his own anaesthesiologist—"keeping wickets while bowling," as he wryly described it. So, he turned to the formidable Dr. R.N. Shetti and asked to be taught exactly what he needed to know: intubation, spinal taps, and patient monitoring. The quiet lessons from the master anaesthesiologist were invaluable.
He established Sainath Nursing Home in a small, rented space in Ramnagar. He started with a bank loan and the bare essentials: a table, chairs, a blood pressure apparatus, an operating table, and a suction machine. As Praveena's ophthalmology practice grew rapidly alongside his, they continuously upgraded the clinic, building a thriving hospital through incremental, deliberate investment.
But the ethics he had carried away from Sevagram remained absolutely inviolable.
There was no overcharging. There were no unnecessary surgeries. Crucially, there was zero participation in the deeply entrenched, corrupt system of "cuts and commissions" between surgeons and referring doctors. This exact corruption had been his primary reason for fleeing Raipur's medical establishment in the first place. In private practice in Wardha, surrounded by a fiercely competitive environment where such practices were standard operating procedure, he rigidly maintained the moral code he had absorbed in Sevagram.
He had come to MGIMS seeking a place where medicine was practiced properly. When he eventually left, he simply took that place with him.
Dr. Trivedi had told him to get his luggage ready. He had. And those two days had become six years, and those six years had become the unshakeable moral foundation of absolutely everything that followed.
| 1951 | Born, 24 February, Raipur — schooling entirely in Raipur despite father’s frequent transfers |
| 1968 | BSc Part 1, Ravishankar University, Raipur — had chosen Biology over Mathematics in ninth grade |
| 1973 | Completed MBBS, Pandit Jawaharlal Nehru Memorial Medical College, Raipur |
| 1977 | Completed MS General Surgery, PJNMMC Raipur — thesis on cervical lymphadenopathy under Dr. H.S.D. Sharma |
| 1979 | Clerk turned him away; knocked on Dr. Trivedi’s door instead; told to get his luggage ready |
| 1979 | Arrived MGIMS, 2 July — Lecturer in Surgery; improvised kitchen with bachelor colleagues on the first floor |
| 1980 | Married Praveena Moharikar — ophthalmologist; joined MGIMS 1981 as Senior Registrar, then Lecturer |
| 1982 | Granted postgraduate guide status — supervised two students; Santosh Prabhu became a distinguished neurosurgeon in Kolhapur |
| 1984 | Promoted Reader, 9 February |
| 1985 | Left MGIMS, 2 December — learned anaesthesiology from Dr. R.N. Shetti in preparation for private practice |
| 1985 | Established Sainath Nursing Home, Ramnagar, Wardha — bank loan; table, operating table, suction machine |
An evaluation diagnostic abdominal paracentesis in acute surgical conditions of the abdomen.
Dr. Suhas Jajoo
MS General Surgery, GMC Nagpur (1981)
MCh Plastic Surgery, GMC Nagpur (1983)
His family had mapped out his future with exceptional care. His brother-in-law had identified Latur as the exact right city. An uncle had found a prime, highly lucrative location for a surgical nursing home in Jalgaon.
He held an MCh in Plastic Surgery from Government Medical College (GMC), Nagpur—which happened to be the very first medical college in India to even offer the degree. With that elite credential, highly prestigious government institutions and massively lucrative private practice in any major city he chose were realistic, immediate possibilities. The future seemed perfectly clear, and the path brilliantly lit.
He chose Sevagram instead.
Located just five miles from his parents' house, it was the same village where his elder brother Ulhas had already spent years building a legacy in the Medicine department. It was a place where strict Gandhian values shaped the institutional culture, and where patients came from the poorest villages bearing conditions no one else was equipped to handle. He did not choose it because it was convenient; it was geographically near, but professionally modest. He chose it simply because it was the right place.
"Medicine wasn't just about treating illness," he had learned watching his brother work. "It was about touching lives."
Burn victims, leprosy patients with deformed hands and feet, children with severe cleft lips and palates, and men from the nearby Dattapur colony enduring lifelong catheters because no surgeon had ever offered them relief—these were the patients who would fill his operating theatre in Sevagram. He came knowing exactly who was waiting there, and knowing that he was the person who could finally help them. That was a completely sufficient reason.
Suhas Jajoo was born on November 28, 1955, in Wardha. His grandfather, Shrikrishnadas, had been imprisoned during the freedom struggle and had famously turned down offers to serve as Chief Minister of CP and Berar, and as the Union Finance Minister. He chose simplicity and service over massive political power, absorbing Gandhian values as a daily, personal philosophy rather than a political posture. The Jajoos of Wardha were known for their fierce integrity, their deep humility, and the simple khadi they wore from cradle to grave.
Suhas completed his matriculation in Marathi medium in 1972. His first year of BSc at Jankidevi Bajaj Science College presented two massive challenges simultaneously: learning entirely in English, and shifting from Mathematics (his natural strength) to Biology. His elder brother Ulhas urged the painful shift toward medicine. Suhas pushed past the deep frustration, seeking constant help from his professors, and the brutal year of struggle finally opened the door to Government Medical College, Nagpur, in 1973.
He completed his MBBS in 1977. His rural internship at the Bhadrawati Primary Health Centre—served alongside S.P. Kalantri, Omprakash Singhaniya, and Suresh Batra—planted something deeply durable in his understanding of what healthcare in rural India actually required.
He had originally wanted Ophthalmology, but when he secured only a diploma seat, he refused to accept it and pivoted to Surgery. He joined the MS General Surgery program at GMC Nagpur under Dr. P.H. Soni, focused his thesis on sepsis in burns, and discovered in the grueling process that surgery suited him far more completely than he had ever anticipated.
Plastic surgery presented itself as the natural next step. If general surgery offered the capacity to save lives, plastic surgery offered the miraculous capacity to restore them.
He secured the only available MCh seat at GMC Nagpur. Because the surgical techniques were groundbreaking in India, local expertise was incredibly scarce. Suhas found himself forced to learn complex myocutaneous flaps—a highly advanced reconstructive approach for traumatic or oncological defects—in the only place where practical knowledge was freely available to him: the dissection hall.
Day after day, hour after hour, he practiced relentlessly on cadavers. He typed his massive thesis—all three hundred pages of it—entirely by his own hand.
When he finally presented his research at a major conference in Chandigarh, the elite surgical audience was astonished—not only by the quality of the work, but by the sheer method of its acquisition. "How did you learn this on cadavers instead of human subjects?" The question implied pure incredulity. The answer implied a man who had simply found what was available and used it completely.
He earned his MCh in November 1983, and arrived at MGIMS on March 17, 1984—choosing the rural wards of Sevagram over every lucrative option that had been so carefully arranged for him.
When he arrived, plastic surgery was virtually unknown in Sevagram. Within a single year, he had completely changed that. He repaired cleft lips and palates, giving children with facial deformities outcomes their parents had never imagined possible. He managed complex oral cancer cases that arrived in their brutal final stages, and he addressed severe facial trauma in tight partnership with Dr. Rajiv Borle from Dental Surgery.
But his most transformative contribution was still ahead.
In 1986, he established a dedicated ten-bed Burn Unit at MGIMS. Before this, burn patients received highly erratic and deeply inadequate treatment. Many died not from the burns themselves, but from sepsis and severe malnutrition—the silent, inevitable killers of severe burns in the absence of highly systematic care.
Suhas introduced aggressive wound excision and early skin grafting—massively advanced techniques for that time and place. He replaced weeks of agonizing, fatal deterioration with outcomes achievable in mere days. Patients who would previously have faced a grim, certain prognosis walked out of the hospital within a week.
The results were instantly measurable and absolutely remarkable: 85% of severe burn victims survived under his care. It was a success rate totally unheard of in most rural hospitals of that era. He trained nurses in advanced burn management, refined monitoring protocols, and directed his MS residents to base their theses strictly on burns, sepsis, and malnutrition—because the research questions that most desperately needed answering were the exact ones his patients were dying from.
Sevagram had suddenly become, through the vision and relentless work of one plastic surgeon, an elite center of advanced burn care for rural Vidarbha.
He did not stop at what he had been officially trained to do. When Dr. Kher left in 1985, Suhas stepped up as unit head and instantly identified a critical gap in gastrointestinal diagnostics. He traveled to Nagpur to train under Dr. Shrikant Mukewar, returning to introduce upper gastrointestinal endoscopy to Sevagram—the first person to ever do so. A year later, he sought out a renowned urosurgeon in Pune and fully mastered transurethral prostate resection (TURP).
The patients who most desperately needed the TURP were the elderly men of Dattapur—a village five miles from Sevagram where many leprosy patients had been institutionalized. Several suffered from massively enlarged prostates and were condemned to lifelong catheters simply because no surgical option had ever been made available to them.
Lifelong catheters meant recurrent infections, brutal sepsis, diminished quality of life, and the particular, crushing indignity of total dependency without relief. Suhas partnered with Dr. Arun Tikle from Anaesthesia and began performing TURP surgeries on these patients despite the terrifying clinical challenges: plummeting hemoglobin, the massive difficulty of arranging blood before surgery, and incredibly high complication risks. He brought permanent relief to dozens of men for whom society had completely forgotten.
He also performed extensive, brilliant reconstructive surgery on leprosy patients whose hands and feet had been brutally deformed by the disease, inviting the legendary Dr. Paul Brand and Dr. Ernest Paul Fritschi to MGIMS to share their expertise.
In the operating theatre, he was the kind of teacher who believed in freely passing on what he knew, rather than jealously guarding it. He let residents perform independent surgeries under his watchful eye. He asked the piercing questions that built clinical reasoning rather than blind compliance: "Why this diagnosis? Why this intervention?" His camaraderie with nurses, ward boys, and laboratory technicians was warm, genuine, and highly consistent. He joked with them, listened closely to their concerns, and treated everyone from junior residents to senior faculty with the exact same quiet respect. In a hospital heavily governed by hierarchy and stress, his presence brought profound warmth.
But his rapidly growing influence unsettled some.
In 1989, a sudden administrative directive ordered him to restrict himself exclusively to plastic surgery. He correctly identified it as a thinly veiled attempt to sideline him. It produced his most articulate and sustained argument: in a rural hospital where specialists were desperately scarce, patients routinely arrived with strangulated hernias, ruptured appendicitis, perforated ulcers, and bowel emergencies, alongside burns and deformities. The restriction was clinically senseless, and he loudly said so.
He flatly refused to choose between general surgery and plastic surgery when both were actively essential to his patients' survival. The environment rapidly turned hostile. Colleagues silently withdrew their support. Subtle, daily acts of non-cooperation rapidly accumulated. He recognized, with deep sadness, that the battle had violently shifted from the quality of the clinical work to the toxic politics of the institution. Once that shift occurred, staying meant compromising the absolute moral clarity that had brought him to Sevagram in the first place.
After nine magnificent years of service, he left in December 1992.
He and his wife, Shubhada—a brilliant obstetrician he had married in 1982—established their private practice at Jajoo Wadi, his ancestral home in Wardha.
Their day began at five in the morning in the operating theatre, continued relentlessly through hospital rounds, and stretched deep into the night ensuring every single patient had been seen. The queue outside their clinic never seemed to shorten. No one was ever turned away. Over the following years, they built a highly advanced thirty-bed hospital equipped with modern operating theatres, labor rooms, and diagnostic laboratories—all within the exact same campus where Suhas had been born.
In January 2001, he returned to teaching at Jawaharlal Nehru Medical College in Sawangi as Professor of Surgery. Shubhada joined him three years later. For nearly two and a half decades, they trained entirely new generations of doctors alongside their massive private practice. He mentored nineteen students in plastic surgery, shaping them in the exact manner he had always shaped students: through complex cases, piercing questions, and the unshakeable confidence that comes from being allowed to operate under the eye of someone who truly trusts you.
His daughters, Rucha and Shruti, both became doctors, successfully carrying the medical legacy forward.
The places his uncle had identified for his nursing home, and the city his brother-in-law had proposed—they were not the wrong suggestions. They were simply not Sevagram. They were not Wardha. They were not the place where his grandfather had chosen simplicity over the Chief Ministership, and they were not the place where dying burn patients desperately needed someone who had mastered myocutaneous flaps in a lonely cadaver hall.
He had come to Sevagram by deliberate choice, which was highly unusual. He had stayed for nine years because the work was profoundly real. He had left only because the politics had become more real than the work. And he had ultimately returned to teaching because the fierce instinct toward transmission—toward the next pair of hands, the next surgical mind, the next generation of doctors who would need to kno
| 1955 | Born, 28 November, Wardha — grandfather Shrikrishnadas, Gandhian, declined Chief Ministership of CP and Berar |
| 1973 | Entered Government Medical College, Nagpur |
| 1977 | Completed MBBS — rural internship at Bhadrawati PHC alongside S.P. Kalantri |
| 1981 | Completed MS General Surgery, GMC Nagpur — thesis on sepsis in burns |
| 1982 | Married Shubhada, 26 February |
| 1983 | Completed MCh Plastic Surgery, GMC Nagpur — first in India to offer the MCh; trained on cadavers in the dissection hall |
| 1984 | Arrived MGIMS, 17 March — chose Sevagram over Latur, Jalgaon, and every other arranged option |
| 1985 | Introduced upper GI endoscopy to MGIMS — first in Sevagram |
| 1986 | Established ten-bed Burn Unit — 85% survival rate for severe burns |
| 1986 | Mastered TURP under Dr. Bapat, Pune — performed on leprosy patients of Dattapur |
| 1989 | Directive to restrict to plastic surgery only — refused; institutional environment turned hostile |
| 1992 | Left MGIMS, 28 December — after nine years |
| 1993 | Established Jajoo Wadi Hospital, Wardha — thirty-bed facility built on ancestral campus |
| 2001 | Joined JNMC Sawangi as Professor of Surgery — 19 plastic surgery students trained |
Effect of nutrition subeschar-clysis on morbidity mortality in burns
Clinical profile and prognostic factors in septicemia
Dr. Mrudula Naik-Trivedi
MD Obstetrics and Gynaecology, MGM Medical College Indore (1967)

Professor & Head of Obstetrics and Gynaecology · Two Tenures at Sevagram · The Corridor That Fell Silent
Mrudula Naik was born on January 16, 1941, in Harda, Madhya Pradesh, the fifth of six children of Dadabhai and Anandibai Naik. Her father was a distinguished Gandhian conducting research on cotton at the Charkha Sangh in Mul; he was imprisoned during the 1942 freedom struggle when she was an infant. Her earliest months were shaped by a household committed to something vastly larger than its own comfort.
This formation ran through the family bloodline. Her elder sister Vasantidevi married a man who dedicated his life to the Leprosy Foundation in Dattapur. Her younger brother Girish became a gastroenterologist, practising in the United States before returning to Indore. For the Naiks, service was not a vague sentiment; it was a family inheritance demonstrated across an entire generation of siblings.
Her early education moved through Narsinghpur, Nagpur, and Jabalpur before she entered Jabalpur Medical College in 1959, transferring to MGM Medical College, Indore, in her third year. It was there, as a young intern, that her path first crossed with Dr. Karunakar Trivedi, a surgical registrar. Both came from fiercely Gandhian families. They married on May 26, 1969. She completed her MD in Obstetrics and Gynaecology in December 1967 and was officially deputed by the Government of Madhya Pradesh to join MGIMS in September 1970.
She arrived at an institution that was, in the most literal sense, just beginning. Kasturba Hospital's clinical infrastructure consisted of fifteen beds, three compounders, and Dr. Anant Ranade leading a small team of nurses. The Trivedis were among the very first clinical teachers, desperately preparing for an inaugural batch of students that had not yet arrived, trying to build a hospital that existed more in intention than in reality.
She was promoted to Reader in October 1971 and served as officiating Head of the Department until March 1972. Her legendary ward discipline was not separate from the campus's Gandhian ethos; it was continuous with it. Gandhi's ashrams had been fiercely disciplined places too, proving that simplicity must be accompanied by rigorous expectations of conduct.
Then, in June 1972, her husband was abruptly removed as Head of Surgery — without consultation. He resigned immediately. She resigned in absolute solidarity. In an act of deep professional responsibility, she chose to stay in Sevagram for an additional year before joining him, refusing to abandon her patients and residents mid-stream. It was the most responsible version of solidarity imaginable.
The Trivedis moved to the United States, where Dr. Karunakar Trivedi pursued advanced cardiac surgery training in Cleveland and New York. Dr. Mrudula sat for the ECFMG examinations. Then their second daughter, Anita, was born. Balancing a demanding career in an unfamiliar medical system while raising a newborn proved impossible to sustain. She chose the child — a decision made by a woman who understood her own priorities with absolute clarity.
In 1976, Dr. Sushila Nayar was visiting her niece on Long Island and reached out to the Trivedis. The Emergency in India had made their family's circumstances difficult — relatives had been imprisoned, government positions revoked. Nayar's offer was simultaneously a professional lifeline and a homecoming. She acknowledged what the 1972 departure had been about, and admitted how desperately the hospital needed them. The Trivedis agreed. They returned to India in July 1977.
The seven years that followed were, by the account of everyone who lived through them, genuinely productive and deeply happy. Teaching, gruelling clinical work, and community service seamlessly blended. By 1984, the Trivedis were seriously considering making Sevagram their permanent home. This consideration makes what happened next infinitely more painful — they were not leaving a place they had already emotionally departed; they were violently uprooted from a place they had actively chosen.
During the 1984 student strike, effigies of Dr. Trivedi were burned and vicious abuse was hurled. The administration stood completely aside. To both of them, this silence was a far deeper betrayal than the 1972 removal. In 1972, they had been hurt by a management decision made without consultation. In 1984, they were hurt by a management that cowardly stood aside while violence was openly directed at them. Once again, the Trivedis felt they had no choice but to leave. She left with him, exactly as she had twelve years prior. This was never passivity. It was a fiercely active decision made by a woman who had her own razor-sharp sense of what was tolerable and what was not.
Moving to the MP Cloth Market Hospital in Indore, she took on dual roles as gynaecologist and administrator until 2008. Even after undergoing bypass surgery in her later years, she continued working as a consultant. The iron discipline she had applied to her rural wards applied equally to her own physical recovery.
Her children carried the family's formation into entirely different fields and continents. Rajshree, born in Indore just weeks before the first move to Sevagram, is now a Staff Specialist in Paediatric Intensive Care at John Hunter Hospital in Australia. Anita, born in the United States, completed a Master of Design from the IIT Institute of Design in Chicago and built a career at Thomson Reuters. Apoorv, born in Sevagram in 1979 — a true campus child — earned his MBA from IIM Bangalore and works as a portfolio manager at Moon Capital in Singapore. Three children. Three continents. Three different fields.
Today, Dr. Mrudula Naik-Trivedi continues to practise in Indore. The MGIMS ward that once fell dead silent when she entered is more than forty years behind her now. But that silence, one suspects, follows her still — the highly particular quiet that elite competence and unyielding expectation, sustained consistently across an entire career, eventually earn without ever needing to be performed.
| 1941 | Born, 16 January, Harda, Madhya Pradesh — father Gandhian researcher imprisoned 1942 |
| 1959 | Entered Jabalpur Medical College — transferred to MGM Medical College Indore in third year |
| 1967 | Completed MD Obstetrics and Gynaecology |
| 1969 | Married Dr. Karunakar Trivedi, 26 May — both from Gandhian families; both committed to medicine as service |
| 1970 | Joined MGIMS, 10 August — one of the founding clinical teachers; 15 beds, no department |
| 1971 | Promoted Reader, October — officiating Head of Department until March 1972 |
| 1972 | Resigned in solidarity with husband — stayed one additional year to complete responsibilities before leaving |
| 1973 | Left for United States — ECFMG examinations; daughter Anita born; chose family over American career |
| 1977 | Returned to MGIMS, 1 September — Dr. Nayar’s personal invitation; Professor and Head of OBG |
| 1979 | Son Apoorv born in Sevagram |
| 1984 | Left MGIMS, 15 June — administration’s silence during student strike; second resignation in solidarity |
| 1984 | MP Cloth Market Hospital, Indore — gynaecologist and administrator until 2008 |
| 2008 | Continued as consultant — including after bypass surgery in later years |
Role of vaginal cytology in detecting hormonal status
High risk pregnancy- it’s perinatal outcome
Dr. Archana Acharya
MD. Obstetrics and Gynaecology , BJ Medical College (1966)
If Dr. Mrudula Trivedi was a storm and Dr. Chhabra a rushing wind, then Dr. Acharya was a gentle drizzle — quiet, soothing, nourishing. Fair and petite, her voice soft as a lullaby, she never raised her tone or spoke an unkind word. She communicated with women in a language they understood, her warmth more reminiscent of a doting housewife than a stern professor. Beneath the soft exterior lay a razor-sharp mind that unravelled intricate obstetric challenges with effortless grace — a reminder that strength does not always roar. Sometimes it whispers.
She had grown up in Prabhat Studios, Pune, where her father Sadashiv Kulkarni worked as a recording engineer and the corridors hummed with melodies by Sudhir Phadke and echoed with the measured footsteps of V. Shantaram. She had absorbed, without fully knowing she was absorbing it, the particular quality of an environment where craft was taken seriously and beauty was produced through discipline. She chose medicine over cinema because her dying father asked her to. He did not live to see her enter medical college. And when she married, in 1967, her husband’s name was Prabhat — the same word as the studio, meaning dawn — as though the universe had woven her father’s world into the fabric of her own story.
She arrived at MGIMS on October 26, 1972, on a monthly salary of ₹750. She left on February 16, 1984, not because the work had lost its meaning but because her sons needed schooling that Sevagram could not offer and Raipur could. It was a decision dictated not by ambition but by necessity, made with a heavy heart, the institution’s corridors carrying the echo of what she had given for eleven years.
At eighty-six, she remains as articulate and perceptive as she ever was. Perhaps this is the essence of Prabhat — a dawn that lingers, refusing to let dusk settle too soon.
Archana Acharya was born Usha Kulkarni on June 20, 1939, the eldest of five siblings, into a childhood shaped by the magic of Prabhat Studios. Her father Sadashiv Kulkarni worked as a recording engineer in that golden era of Indian cinema — a man of craft, of technical precision deployed in the service of artistic vision. She moved through the studio’s corridors as a child, enchanted, absorbing a sensibility that would express itself decades later in the particular care she brought to everything she did.
She was born breech — a fact her mother often recounted alongside the superstition that attached to it: a breech-born child had healing power in the foot, could relieve back pain and sciatica by touch. Whether or not she believed it, the idea of healing was in her domestic air from the beginning. Then in 1956, as her father battled gastric cancer, he trusted her with administering his vitamin B12 injections. One day he voiced his deepest wish: that she become a doctor. She chose the white coat over the arc lights. Her father did not live to see her step into medical college.
She attended Modern Girls’ High School and Fergusson College in Pune, excelling in elocution, clearing the eleventh matriculation board with first-division honours and distinctions in Mathematics, Physics, Sanskrit, and — the source material notes with affectionate precision — “Puneri English.” She entered BJ Medical College, Pune, and earned her MBBS in 1962, supporting herself through her studies after her father’s death with the help of teachers, borrowed notes, and borrowed books, passing every examination on the first attempt.
In 1965, she won the prestigious Purandare Gold Medal in her DGO from the CPS Board, Bombay. In 1966, she sat her MD in Obstetrics and Gynaecology at BJ Medical College under Dr. B.J. Paranjape — and failed on her first attempt, not from incompetence but because the department head, serving as examiner, favoured her own candidate. For a student who had never failed, who had won a gold medal the previous year, this was a bitter pill. She appeared six months later and cleared it.
Miraj, the Marriage of Two Dawns, and the Search for Meaning
At Wanless Hospital, attached to Miraj Medical College, she worked brief stints as clinical assistant in radiology, resident in anaesthesia, and junior lecturer in Obstetrics and Gynaecology — each role broadening her perspective before she found her settled ground in women’s health. It was in Miraj that Usha Kulkarni met Dr. Prabhat Kumar Acharya, a junior lecturer in Skin and Venereal Diseases from Chhattisgarh. Theirs was an arranged marriage with barely a meeting or two before the wedding. When word of their engagement spread through the college, colleagues were taken aback — no one had ever seen them together.
Both names meant dawn. Usha and Prabhat — she fluent in Puneri Marathi, he comfortable in Hindi, her Hindi as unpolished as his Marathi. They married on December 17, 1967. After the wedding, she took a new name: Archana. The dawn that had animated Prabhat Studios was now the name of the man she had married, and her own name carried a different meaning — offering, worship, devotion — that would prove quietly prophetic.
They moved to Raipur in 1968. Despite her MD and DGO, she struggled to secure a government assistant surgeon post. For four years they ran a private practice, technically competent but spiritually unsatisfying — they longed for clinical work integrated with teaching, the life of a medical institution rather than a private clinic. Dr. Karunakar Trivedi, a former colleague, suggested Sevagram. Dr. M.M. Arora of Pathology at MGIMS seconded the suggestion. On October 26, 1972, she joined as Lecturer in Obstetrics and Gynaecology. Dr. Prabhat Acharya joined on deputation from the Madhya Pradesh government the same day. By July 1973, he had been promoted to Reader in Dermatology. They had found the place where medicine was not just practised but lived.
Three years in, Iran’s oil wealth was reshaping its healthcare system and drawing Indian specialists with generous salaries and superior working conditions. The government arranged a chartered flight carrying four hundred specialists to Tehran. Dr. Archana Acharya took a position at the 9th Abad Hospital in Abadan from August 29, 1975. Dr. Prabhat Acharya returned to Sevagram after a year. Dr. S.C. Ahuja and his wife — the orthopaedician and the paediatrician — made the same journey.
Dr. Sushila Nayar, with the department stretched thin and the absence of skilled faculty keenly felt, wrote to the Minister of External Affairs and the Minister of State in Home Affairs with the urgency she typically brought to institutional crises. Her message was unambiguous: “We need Dr. Acharya back — now.” No extensions beyond September 1977. By October 12, 1977, Dr. Archana Acharya was back in Sevagram.
She was promoted to Reader on June 1, 1975, then to Associate Professor on September 1, 1983. In the years between the return from Iran and the departure for Raipur, she built the teaching and clinical contribution that her students would carry into their own careers.
The MD programme in Obstetrics and Gynaecology at MGIMS received Nagpur University approval in the early 1980s. The first batch of MGIMS MBBS graduates had the unprecedented opportunity to specialise at their own institution. The thesis requirement stood between them and the degree. All four guides — Dr. Trivedi, Dr. Chhabra, Dr. Samal, and Dr. Acharya — were supervising MD students for the first time. None had mentored one before. The result was a mixture of uncertainty, cautious optimism, and the occasional chaos of collective inexperience.
Dr. Acharya’s student was Dr. Kishore Shah. The thesis she guided him toward was not the cutting-edge research he had proposed — CVP monitoring in eclampsia, oestradiol levels in fertility — but something more fundamental. “You can chase those exotic topics once you’ve earned your MD,” she told him. “Right now, choose something fundamental — something that will serve you in the real world, both in rural and urban settings. And most importantly, something that won’t steal away the hours you should be spending mastering the subject itself.”
The topic he chose was the effect of Valethamate, a smooth muscle relaxant, on cervical dilatation in labour — simple, practical, applicable in any setting. She introduced him to the partograph, the chart that tracks labour and allows timely intervention without expensive equipment. She taught him to read its subtle cues, to anticipate complications before they arose. Decades later, he still uses it. The pragmatist’s gift to the student was not a prestigious research question but a durable clinical tool.
This would be the first and the last thesis she supervised. In the spring of 1984, she walked away from academia — Kishore Shah’s work the single completed expression of her formal teaching contribution to postgraduate education, but not the measure of what eleven years of teaching had given the MBBS students and junior residents who had moved through her ward.
Beyond the labour room and the lecture hall, she brought to Sevagram the particular warmth of a woman who understood that community was built in domestic spaces as well as institutional ones. Her Gauri Ganapati and Shravan Haldi-Kunku celebrations were spectacles of tradition — fragrant flowers, rituals steeped in colour, camaraderie and joy filling the courtyard. She moved between the operating table and the festive gathering with the same ease, as if precision and poetry were not different modes but the same attention directed at different objects.
She was fluent in English, Marathi, Hindi, Urdu, and Persian — the linguistic range of someone who had grown up in the multilingual world of a studio, married a man of a different linguistic formation, and spent her career communicating with patients whose first language was often none of the above. She built bridges between languages as she built bridges between lives, speaking to women in whatever register made them feel heard.
The Departure and What Came After
Their sons attended Kasturba Vidya Mandir, the only school in Sevagram, managing through Class Seven. As they grew, the academic ceiling became visible. The Acharyas sent them to Rajkumar College, a boarding school in Raipur where the family also had ancestral roots. Dr. Prabhat Acharya settled in Raipur ahead of the family. On February 16, 1984, Dr. Archana Acharya formally handed over her charge to Dr. Mrudula Trivedi and left.
She spent four months at the Tata Cancer Hospital in Bombay gaining experience in gynaecologic cancer surgery, then joined private practice in Raipur, eventually establishing Guru Kripa Surgical and Maternity Centre — a small maternity home where new life took its first breath under her care, run with quiet dedication until she chose to close it in 2014. She performed hundreds of hysterectomies free of charge in 1998 and 1999, requesting voluntary donations that did not come. She accepted whatever patients chose to pay, sometimes as little as ₹70 for a post-operative visit. The financial philosophy was consistent with everything else: the work mattered, not the return.
Their son Ravi became an endocrine surgeon in the United Kingdom. Atul became a software engineer in the United States. The studio daughter from Pune, who had learned healing in her father’s sickroom and practised it across four decades, produced a surgical son who operates on glands in the UK and a technical son who builds systems in the US — the formation travelling, as formations do, into unexpected shapes in the next generation.
She lives in Raipur now, alongside Dr. Prabhat Acharya, the days slower but no less meaningful. She draws on Sant Tukaram in her own account of how to bear physical ailment — accept what comes your way with surrender, placing your faith in the divine — with the same quiet grace with which she had moved through every difficulty the eleven Sevagram years had presented. At eighty-six, she remains articulate and perceptive. The dawn that will not let dusk settle.
| 1939 | Born Usha Kulkarni, Pune |
| 1956 | Father’s cancer diagnosis; begins administering his injections at home |
| 1962 | MBBS, BJ Medical College, Pune |
| 1965 | Purandare Gold Medal, DGO, CPS Board, Bombay |
| 1966 | MD Obstetrics and Gynaecology, BJ Medical College (cleared second attempt) |
| 1967 | Married Dr. Prabhat Kumar Acharya; took the name Archana |
| 1968 | Moved to Raipur; private practice with husband |
| 1972 | Joined MGIMS as Lecturer, Obstetrics and Gynaecology (26 October) |
| 1975 | Promoted to Reader (1 June); posted to 9th Abad Hospital, Abadan, Iran (29 August) |
| 1977 | Recalled by Dr. Sushila Nayar; returned to MGIMS (12 October) |
| 1983 | Promoted to Associate Professor (1 September) |
| 1984 | Left MGIMS (16 February); trained at Tata Cancer Hospital, Bombay |
| 1984 | Established Guru Kripa Surgical and Maternity Centre, Raipur |
| 2014 | Closed private practice |
Dr. Kishore Shah · MD Obstetrics and Gynaecology · First MD batch, MGIMS
Thesis: Effect of Valethamate bromide on cervical dilatation in active labour. A practical, rural-applicable topic chosen on Dr. Acharya’s guidance over more complex proposed subjects. She introduced Dr. Shah to the partograph as a core clinical tool during this work. First and only postgraduate student she supervised at MGIMS.
Dr. Prakash Nayar
Professor & Head, Obstetrics and Gynaecology (1972–1977)

Professor & Head, Obstetrics and Gynaecology · Medical Superintendent · Cousin of Dr. Sushila Nayar · Laika Aunty of Guru Nanak Colony
The children of Guru Nanak Colony had their own name for her. Not Dr. P. Nayar, not Professor, not even Aunty in the usual campus fashion. They called her Laika Aunty — after the dog.
Laika was a large, cheerful creature named for the Soviet space dog, and she and Dr. Prakash Nayar were as inseparable as any two beings on the MGIMS campus. You would see them in the evenings, the elegant doctor and her exuberant dog, making their unhurried way through the colony's lanes — Laika's tail a constant metronome against the quiet of Sevagram's evenings. Inside the bungalow, Laika was not a pet so much as a presence, a warm and uncomplicated companion for a woman who had no family of her own in Sevagram. When Laika nudged her hand for a pat, something in Dr. Nayar visibly softened. The children of the campus saw this, understood it, and honoured it in the way children honour things — by naming her after what they saw most clearly.
The nickname stuck. It was, as those who knew her agreed, exactly right.
Dr. Prakash Nayar was born in Agra, the youngest of four siblings, a cousin of Dr. Sushila Nayar. Her brother Dev Prakash Nayar was a prominent educationist during Gandhi's era, and it was under his guidance that she pursued her medical ambitions with the determination that would mark her entire career. She earned her MS, DCh, and FRCOG — qualifications that positioned her among the better-trained obstetricians of her generation.
Her mentor was Dr. Banner, a bond so strong and enduring that when Dr. Nayar retired as Professor and Head of Obstetrics and Gynaecology from Ranchi Medical College in the early 1970s, she brought Dr. Banner with her to Sevagram and cared for her there until she died. It was a characteristic gesture — quiet, loyal, entirely without calculation.
She joined MGIMS in March 1972, succeeding Dr. K. Deshmukh as Professor and Head of Obstetrics and Gynaecology. There is a detail that surfaces only on reflection: years earlier, at Patna Medical College, she had taught Manimala Chaudhary when Manimala was training to become a matron. Neither woman could have known then that their paths would converge in Sevagram, where both would shape a rural medical institution from its earliest years. Life, in the Sevagram story, has a recurring habit of this — the small connections that reveal themselves as consequential only much later.
Her tenure lasted four years, from 1972 to 1977. She was not, by the conventions of academic medicine, a typical department head. She seldom conducted formal bedside clinics or delivered structured lectures. What she did instead — and did exceptionally well — was deliver babies, perform surgeries with calm skill, and create around herself a department atmosphere of maternal warmth that her staff and students absorbed and carried forward.
Her voice was distinctive — hoarse, low, surprising the first time you heard it emerging from someone of such elegant bearing. But those who knew her learned quickly that the voice and the nature were different registers of the same person: both direct, both genuine, both entirely without pretension.
She served simultaneously as Medical Superintendent of the hospital during this period — a dual responsibility that required administrative capacity alongside clinical work. She managed both without apparent strain, in the fashion of a generation that did not compartmentalise professional roles as rigorously as those that followed.
When her tenure as department head ended, she did not simply step away. She guided the transition carefully — passing the department to Dr. Kasturi Lal, and when Dr. Kasturi Lal left, steering Dr. Chhabra into the role in 1977. A year later, Dr. Mrudula Trivedi arrived and took over as head, a post she would hold until 1984. The continuity of the department through these years owed something to Dr. Prakash Nayar's attentiveness to succession — the understanding that a department is not an individual but a living thing that must be handed forward thoughtfully.
She was an elegant woman — impeccably dressed, refined in manner, with a sense of style that sat quietly but visibly alongside her Gandhian institutional context. The local artist Gajanan Ambulkar was moved to capture her in a watercolour portrait, with Laika beside her. It was the kind of portrait that gets made when a presence is felt as distinctive — something worth recording before it passes.
She entertained warmly. Senior faculty and administrators were frequent guests at her home for evenings of Mahjong, Chinese checkers, and Scrabble — games that created a relaxed, communal atmosphere in an institution whose daily life was demanding and whose social occasions were often formal. She was a convivial host, and her home was one of the places on campus where the community's more informal bonds were formed and maintained.
In her later years, committed to Sevagram long after her formal tenure had ended, she built a comfortable three-bedroom house near Dr. Sushila Nayar's residence, directly across from the staff club. It was a statement of belonging — she was not passing through Sevagram but had chosen it as her permanent home. When she died on May 3, 1997, she bequeathed the house to the Kasturba Health Society. It became the P. Nayar Guest House, receiving visitors to the institution she had given her professional and personal life to.
Many of the mothers delivered by Dr. Prakash Nayar are grandmothers now. The babies born under her care are doctors themselves, some of them in the very department she once led. This is the particular legacy of a good obstetrician — measured not in papers published or positions held but in lives that began safely, in families that were spared the worst, in the specific memory of a calm and competent presence at the most vulnerable moment.
She had no family of her own. Laika was her world, and the campus was her community. The children who grew up in Guru Nanak Colony and called her Laika Aunty understood, without being able to articulate it, that she had given everything she had to the place and the people around her — and that this was enough, and perhaps more than enough, to constitute a full life.
The watercolour portrait is somewhere in Sevagram. The guest house carries her name. And in the memory of every mother who delivered under her hands, Dr. Prakash Nayar — Laika Aunty — lives on.
| — | Born, Agra — youngest of four siblings, cousin of Dr. Sushila Nayar |
| — | MS, DCh, FRCOG — among the better-trained obstetricians of her generation |
| — | Teaches Manimala Chaudhary at Patna Medical College — paths converge in Sevagram decades later |
| — | Professor & Head, Obstetrics and Gynaecology, Ranchi Medical College |
| 1972 | Joins MGIMS, March — succeeds Dr. K. Deshmukh |
| 1972 | Medical Superintendent, Kasturba Hospital — dual role alongside department |
| 1972 | Brings Dr. Banner — her mentor — to Sevagram, cares for her until death |
| 1977 | Guides transition to Dr. Kasturi Lal, then Dr. Chhabra |
| 1978 | Dr. Mrudula Trivedi arrives — department continuity secured |
| — | Builds home near Dr. Sushila Nayar’s residence — a statement of permanent belonging |
| — | Portrait painted by Gajanan Ambulkar — watercolour, with Laika beside her |
| 1997 | Dies 3 May, Sevagram — bequeaths house to KHS |
| 1997 | House becomes P. Nayar Guest House, Sevagram |
Dr. Chellamma Hariharan Iyer
MD Obstetrics and Gynaecology (1974)
Reader in Obstetrics and Gynaecology · Seven Years at Sevagram · The Temple Bell in the Corridor
Chellamma Krishnan Iyer was born on August 11, 1948, in Tirunelveli, Tamil Nadu, the eldest of three daughters. Her father, Kechappa Iyer, was a stenographer at Mazagon Dock in Mumbai; her mother, Parvati, was a homemaker whose core conviction was that her daughters must be self-reliant. Mediocrity was simply not an option in their household.
She aimed for admission to a prestigious Mumbai medical college but missed the cutoff by exactly one mark. Undeterred, she enrolled in the Licentiate of the College of Physicians and Surgeons course in Nagpur. A year later, her sheer academic force allowed her to transfer to Grant Medical College, Mumbai, where she completed her MBBS in April 1971. Her early clinical training pushed her through Cama Hospital, Prince Aly Khan, Parsi General, Ismail General, and GT Hospital. She had initially dreamed of becoming a neurosurgeon, but the surgical specialty remained largely inaccessible to women at the time. She pivoted to gynaecology — a field where women practitioners were not just tolerated, but desperately needed — and found in it the perfect combination of elite surgical skill and raw human connection that her temperament demanded.
She arrived late from the hospital, walking with a pronounced limp from a minor injury. It was an arranged marriage viewing — he had come to see the girl — and she greeted him with characteristic unvarnished candour: "I want to study abroad." He looked at her and replied gently: "Well, you can do that right here." They married on November 7, 1973. He was Dr. K.K. Hariharan, the brilliant dentist who had been at Sevagram since 1971, the wiry man with the quick wit who sat across the card table cracking jokes that made the campus matriarchs laugh. She was Dr. Chellamma Krishnan Iyer, who would soon be known across the campus simply as Dr. Hariharan — beloved, radiant, and utterly impossible to overlook.
Together on the MGIMS campus, they were a beautiful study in contrasts: he tall and lean, she petite and radiant; he fluent in drama and storytelling, she fluent in warmth and wit. They were the Hariharans, and for the years they were both in Sevagram, the campus was a demonstrably livelier place because of them.
She joined MGIMS as Lecturer in January 1973, resigned briefly to complete her MD, and returned triumphant in January 1975. In December 1976, following Dr. Kasturi Lal's resignation, she was asked to lead the entire department — while still officially only a Lecturer. A few months later, she took over the sprawling Postpartum Programme. By August 1978, the institution finally recognised the reality of her workload and her promotion was formally backdated.
The Postpartum Programme was staggering in scope: twenty-two wards in Wardha town, fifty-eight remote villages around Sevagram, antenatal and postnatal care, cervical cancer screening, sterilization surgeries, and mass immunisations. The plan envisioned a dedicated gynaecologist paired with a dedicated anaesthesiologist. When the appointed anaesthesiologist took extended leave, the position remained vacant. Dr. Hariharan simply carried the entire burden alone. At Kasturba Hospital alone in 1974, she helped oversee sixty-two major surgeries, three hundred and twenty tubectomies, and one hundred and thirty-nine medical terminations of pregnancy — operating at the scale of a senior professor supported by a massive department, while officially holding the rank of a Lecturer working without an anaesthesiologist.
Her laughter rang through the stark hospital corridors like temple bells in a Tamil village. Her expressive eyes sparkled with constant mischief. She was always impeccably dressed in crisply pleated saris, a red bindi resting on her broad forehead. She moved with the easy, unforced grace of someone entirely comfortable in her own skin.
Her teaching contribution was entirely at the undergraduate level — the department's MD programme was still in its infancy when she left. What those MBBS students carried into their careers was not just clinical knowledge, but the profound experience of learning from someone who made medicine feel like a shared human adventure rather than a rigid, terrifying obligation. She possessed the rare gift of dissolving clinical tension with humour precisely when a complicated labour most required that tension to be broken. Students adored her because they understood instinctively that her warmth and her elite clinical competence were not separate qualities — they were two expressions of the exact same character.
On April 15, 1980, after five years of unbroken exhausting service, she resigned from MGIMS and followed her husband. They moved to Nigeria in 1983, where she worked at Westend Hospital. The Sevagram duet continued flawlessly in West Africa. This was followed by fifteen years in Riyadh, serving women in the Middle East with the same unflagging commitment she had shown in the villages of Vidarbha.
She returned to India permanently in 2004, joining her husband in Patiala. Tragically, he died within a month of her return — the highly specific grief of losing the person who had been by her side through the Bangladesh War, the MD near-failure, Nigeria, Riyadh, Sevagram, and that very first arranged meeting where she had arrived limping and demanding to study abroad. She resumed work in Obstetrics and Gynaecology at JNMC Sawangi, working until she was seventy, then took up consulting in Chandrapur. In 2018 she settled in Dahisar, Mumbai, and endured three years of dialysis for chronic kidney disease, fiercely supported by her family. She died on August 18, 2024 — exactly seven days after her seventy-sixth birthday.
Her elder daughter Anuradha trained in dentistry but forged her own path. Her younger daughter Manisha moved from engineering into digital marketing and found her deepest calling in animal welfare — rescuing stray and injured dogs with a compassion that mirrors her mother's lifelong service to the vulnerable. The woman who arrived at an arranged marriage demanding to study abroad had raised daughters who carried her fierce independence into the next generation.
She had told her future husband she wanted to study abroad. She studied in Sevagram instead. And then in Nigeria. And then in Riyadh. She carried the purpose that had driven her through the frantic wards of Mumbai into every single labour room she ever inhabited, refusing to let her brilliant, ringing laughter dim until her body finally required it to.
| 1948 | Born, 11 August, Tirunelveli, Tamil Nadu — eldest of three daughters |
| 1971 | Completed MBBS, Grant Medical College Mumbai — missed first-choice college by one mark; transferred from Nagpur |
| 1971 | Emergency duty during Bangladesh War — baptism by clinical fire |
| 1973 | Completed DGO, October · Diploma in Family Planning 1974 |
| 1973 | Joined MGIMS, 1 January — Lecturer in OBG · married Dr. K.K. Hariharan, 7 November |
| 1975 | Returned to MGIMS, January — after completing MD |
| 1976 | Led entire OBG department after Dr. Kasturi Lal’s resignation — still officially a Lecturer |
| 1977 | Took over Postpartum Programme — 22 wards in Wardha, 58 villages; ran it alone when anaesthesiologist post fell vacant |
| 1978 | Promoted Reader, August — backdated to reflect actual responsibilities |
| 1980 | Left MGIMS, 15 April — followed husband |
| 1983 | Westend Hospital, Nigeria — with Dr. Hariharan |
| 1989 | National Hospital, Riyadh — fifteen years serving women in the Middle East |
| 2004 | Returned to India — husband died within a month of her return |
| 2004 | JNMC Sawangi — practised until age seventy; then consulting, Chandrapur |
| 2018 | Settled Dahisar, Mumbai — dialysis for chronic kidney disease |
| 2024 | Died, 18 August — seven days after her seventy-sixth birthday |
Dr. Shakuntala Chhabra
MD Obstetrics and Gynaecology, Government Medical College Nagpur (1972)

Shakuntala Chhabra was born on November 22, 1949, in Gondia, the youngest of six children of Amir Chand Chhabra, a forest contractor who had migrated from Rawalpindi. Two childhood experiences crystallised her understanding of what medicine was actually for. At rural eye camps, she watched doctors restore sight to blind patients — skill and kindness functioning as an inseparable unit. At home, she watched their family doctor treat her ailing brother every single time without ever taking a rupee. Both images carried the same essential truth: medicine was the combination of elite competence and raw generosity. She decided she wanted to be exactly that kind of doctor.
She entered Government Medical College, Nagpur, in 1966, graduated MBBS in 1970, and completed both her DGO and MD in Obstetrics and Gynaecology in a blistering two and a half years — an early signal of the intensity she would bring to everything she undertook. When she chose Obstetrics over a more comfortable research or administrative path, her mentors were surprised. But for her, the emotional connection with patients was not supplementary to the clinical work; it was the entire foundation.
In July 1975, during the Emergency, she joined MGIMS as Lecturer. The night of the massive haemorrhage came shortly after her arrival. The mother lay pale, her pulse racing, her skin cold and clammy. The bleeding refused to stop. She was twenty-six years old, newly arrived in Sevagram, fresh from her MD, and entirely alone with the catastrophic emergency unfolding in front of her. That night, she saved two lives. The choice she had made — to be in the wards with desperate women rather than in a comfortable research post — became, in that delivery room, a lifelong mission.
By 1980, like many of her peers, she considered leaving. Prestigious institutions presented themselves as possibilities. Dr. Nayar tried to create a new administrative path in Social Obstetrics to retain her, but Dr. Chhabra declined — she knew her strengths lay in hands-on patient care, not in administration. She chose to stay in the wards. The forty-nine years began to accumulate.
She chose not to marry. Brief breaks at her nearby home offered nothing more than a simple meal and a half-cup of tea before she rushed back. Hunger and fatigue were treated as minor inconveniences. The department was not just her job; it was her entire life.
As director of the Family Planning Unit for seventeen years, she expanded its scope far beyond contraception — introducing cluster immunisations, launching cervical cancer screenings, and educating rural women on reproductive health. The dusty villages of Vidarbha became her field just as much as the hospital ward.
In 1989, a British Council diploma programme in Liverpool deepened her grasp of global maternal healthcare. The WHO invited her to Jakarta as consultant; she went, contributed brilliantly, and when offered a highly lucrative permanent role, she chose to return to Sevagram because her rural department needed her more than Geneva did. Further training took her to Sweden and Maastricht. Over five decades, she produced more than six hundred publications — accumulated through relentless application of research discipline to the clinical problems she encountered every day. The manuscripts she returned to her residents were famously covered in red ink.
In 1987, the sight of a discarded foetal skull near her home in Sevagram shook Dr. Chhabra to her core. She immediately proposed a safe motherhood programme for unwed mothers and abandoned children. Institutional resistance was fierce. Fourteen exhausting years of advocacy and bureaucratic navigation followed. Finally, in 2001, with funding from a Danish agency and the vital support of Dhirubhai Mehta, she secured the licence for an orphanage. She named it Aakanksha — aspiration.
Since its founding, Aakanksha has cared for 492 infants, facilitated 443 formal adoptions, and supported 613 women in acute distress. The foetal skull in 1987 had been the harrowing beginning of a fourteen-year journey toward a building, a system, and a name that meant hope.
She was petite and frail, eating sparingly, dressing simply, spending almost nothing on herself, living steps from the department, and moving briskly through its corridors keeping watch over every detail. Backgrounds, wealth, and political connections held zero weight in her ward. Elite competence was the only accepted currency. Casual attitudes received sharp, public rebukes. The apron was mandatory. The corridor fell silent.
Dr. Kishore Shah, one of her students, described her with precision: "Dr. Chhabra was, without question, the department's fiercest taskmaster. Her passion for obstetrics and gynaecology was a fire that never dimmed, but it burned those who stood too close. She demanded perfection — anything less was unacceptable. And yet, she was a brilliant surgeon, a visionary in her field, and utterly devoted to her patients. Medicine, for her, was not a profession; it was a sacred duty."
Beneath this terrifying exterior lay a truth her students only came to understand over time: the impossibly high standards were never about her ego; they were entirely about the patients who needed those standards held. A woman bleeding to death in a rural hospital at midnight needed the resident standing beside her to have been trained by someone who accepted no excuse for incompetence. Dr. Chhabra had been that terrified twenty-six-year-old resident once. She trained her students exclusively for that moment.
After forty-nine unbroken years, she left MGIMS on March 31, 2024. At seventy-five, she began an entirely new chapter at a medical college in Shirpur, working to build a 750-bed super-specialty hospital for tribal communities.
Somewhere in a remote village she once served, a mother holds her child close — safe, alive, and thriving — simply because Dr. Chhabra was there. This is the ultimate measure of her life. It is enough. It is, in fact, everything.
| 1949 | Born, 22 November, Gondia — youngest of six children; father forest contractor from Rawalpindi |
| 1966 | Entered Government Medical College, Nagpur |
| 1970 | Completed MBBS, GMC Nagpur |
| 1972 | Completed DGO and MD Obstetrics and Gynaecology — two and a half years |
| 1975 | Joined MGIMS, 7 July — Lecturer in OBG; saved two lives on her first emergency night call |
| 1984 | Head of Department |
| 1985 | Promoted Professor |
| 1987 | Discarded foetal skull near home — fourteen-year journey toward Aakanksha begins |
| 1989 | British Council diploma programme, Liverpool — global maternal healthcare |
| 1990 | WHO consultancy, Jakarta — offered permanent role; chose to return to Sevagram |
| 2001 | Founded Aakanksha orphanage — 492 infants cared for, 443 adoptions, 613 women supported |
| 2004 | Promoted Director Professor |
| 2005 | Medical Superintendent |
| 2007 | Dean, MGIMS |
| 2024 | Left MGIMS, 31 March — joined medical college in Shirpur to build 750-bed super-specialty hospital for tribal communities |
Community based screening for gynecological disorders specially for cervical cancer by Papanicolaou and fluorescent microscopy
The impact of maternal anemia on the obstetrical outcome
The obstetrical neonatal factors influencing neonatal jaundice
Ante partum perception of fetal kick count to monitor fetal wellbeing
Sperm antibodies in infertility
Intracervical injection of hyalase in acceleration of labor
Respiratory function tests during pregnancy their relation to pregnancy outcome
Prediction of severity of toxemia of pregnancy and intrauterine growth retardation by glomerular filtration rate and platelet count
Hysterography in menstrual disorders
Screening for impaired glucose tolerance during pregnancy and its impact on pregnancy outcome
Cervical scoring for prediction of onset of labor and its outcome
Genitourinary tract infection in patients of primary infertility with special reference to chlamydia trachoma is
Prediction of preterm labor premature rupture of membranes with special reference to cervico-vaginal infections
Study of cervical erosion by Papanicolaou staining and its relation to chlamydia infection detected by ELISA
Study of cases of recurrent abortions with special reference to antisperm antibodies detected by an ELISA
Prospective study of the predictive value of antenatal biophysical monitoring in high risk pregnancy
Iodine deficiency in women with pregnancy wastage
Clinico Investigative profile of menstrual disorders in perimenopausal woman with special reference to hysterosalpingography, hysteroscopy and ultrasonography
Correlation between maternal medico socio-demographic factors and platelet counts in intrauterine growth retardation with a reference to low dose aspirin in the management
Evaluation of feto-pelvic relationship and labor outcome in nulliparous woman
Clinical study of cases of induced labor with special reference to use of prostaglandin E2 and hyalase
Evaluation of women with chronic pelvic pain without any abdominally palpable Pathology with special reference to transvaginal sonography hysteroscopy and laparoscopy
Study of factors causing and effecting arrest of preterm labor with special reference to double blind study of efficacy of isoxsuprine and ritodrine
Role of Microalbuminuria for prediction of hypertensive disorders of pregnancy PIH/preeclampsia
An institutional based retrospective prospective study of epidemiology of gynecological malignancies in this rural part of eastern Maharashtra
Reproductive morbidity in adolescents- A case control study
Correlation between status of hemolytic, liver enzymes and platelet counts and feto-maternal outcome in cases of pregnancy induced hypertension, pre-eclampsia and eclampsia, a prospective study
Visible reproductive morbidity of community, an institutional based study
Epidemiological Clinico investigative profile of primary dysmenorrhoea
Prediction of hypertensive disorders by measuring early second trimester maternal serum beta human chorionic gonadotropin
Cesarean Section for non progress of labor in a rural institute (retrospective analysis and prospective study)
Trends in hysterectomy: rural experiences
Study of oligohydramnios with special reference to attempts at optimum outcome through prophylactic ante partum amino infusion as an interventional strategy
Analysis of retrospective case records and prospective cases of ovarian malignancy to study the factors affecting progress and prognosis
Study of feto-neonatal outcome in pregnancies complicated by third trimester vaginal bleeding with special reference to feto-maternal hemorrhage and fetal blood in vaginal blood
Trends, progress and prognosis in carcinoma cervix
Prevalence and Clinico – sonographic biochemical profile of polycystic ovary syndrome in rural women of reproductive age with menstrual irregularities
Carbohydrate and lipid derangements in pregnancies with hypertensive disorder with special reference to perinatal outcome
Incidence, Clinico – biochemical -sonographic profile of premenopausal women with polycystic ovarian syndrome
Clinico – sonographic evaluation of pregnancy in first trimester with special reference to placental site and dimensions for predicting pregnancy disorders and feto-maternal outcome
Causes and effect study of bleeding in first half of pregnancy
Analysis of retrospective cases and prospective study of admission pattern, reason and outcome of critically ill Obstetrics patients at a rural medical institute
Study of clinical investigation, surgical histopathological diagnosis and staging of carcinoma cervix by prospective and retrospective analysis
Analysis of Retrospective Cases and Prospective Study of Admission Pattern, Reasons and Outcome of Critically Ill Obstetric Patients At A Rural Medical institute
Perinatal Outcome in cases of Term and Preterm Prelabour Rupture of Membranes with Special Reference to Body Mass index, Haemoglobin Status, Amniotic Fluid index, Cervical Score and Cervical and Vaginal Colonization.
Retrospective Analysis of Records of Cases of Fetal Growth Restriction (FGR) to Know the Relationship between Anaemia and FGR and Prospective Study of Pregnant Women with FGR to Find Out Correlation Between Anaemia, Cardiac Output and FGR/Maternofetal Outcome.
Cause and Effect Study of intrapartum Foetal Distress in Women with No Risk Factors.
A Cause and Effect Study of Women with Early onset and Late onset Hypertensive Disorders in Pregnancy, Labour and Postpartum with Special Reference to Serum and Urinary Calcium As A Predictive Marker.
A Clinicopathological study of women with complex and/or atypical endometrial hyperplasia and endometrial carcinoma with special reference to risk factors including lifestyle diseases and polycystic ovarian syndrome
Dr. Swarnalata Samal
DGO, Nagpur University (1975) · MD Obstetrics and Gynaecology (1976)

Professor of Obstetrics and Gynaecology · Thirty-Six Years at Sevagram · The Department's Beating Heart
Swarnalata Samal was born on April 14, 1948, in Kusupur, a village in Odisha whose rural quietness gave her early formation its particular character — a quiet strength and a deep, unshakeable empathy that would persist through every subsequent environment. She graduated with distinction from Srirama Chandra Bhanja Medical College, Cuttack, in 1970. She chose Obstetrics and Gynaecology because it was the field where the most direct, immediate intervention in women's lives was possible — where the stakes at every delivery were the absolute highest in clinical medicine.
In 1972, her husband Dr. Nasiruddin Khan — who would later take the surname Samal — joined MGIMS as a house officer in Medicine, eventually becoming a Lecturer in Pathology. Swarnalata joined the OBG department in May 1972 without her postgraduate degree. Together, they made the thousand-kilometre journey from Odisha to Vidarbha, stepping into a new land, a new language, and a culture that bore no resemblance to what either had grown up in. They married in 1973.
They quickly realised that pursuing two postgraduate degrees simultaneously was impossible; their finances simply did not permit it. Dr. Khan made the decision that permanently settled the question: her education would come first. Relieved of financial worry, she earned her DGO with top marks from Nagpur University in 1975, and her MD in November 1976. She returned to MGIMS immediately, rejoining as Lecturer and beginning the long, steady climb that would see her reach Professor in 1985.
When she returned with her MD, the department was remarkably thin. Dr. P. Nayar had retired, Dr. Kasturi Lal had recently left, and Mrs. Hariharan was about to take study leave. The remaining team consisted of just three young lecturers: Dr. Samal, Dr. Kane, and Dr. Shakuntala Chhabra. This small team and the crushing clinical responsibility gave Dr. Samal room to develop as a practitioner far faster than a larger, deeply hierarchical department would have allowed. Her surgical skill became exceptional — she eventually mastered laparoscopic surgery and embraced robotic surgery, a commitment to remaining current that could easily have settled into familiar, comfortable procedures years prior.
Her ability to handle brutal medical cases with absolute calm was the clinical expression of the same temperament that made her so approachable at the bedside. She never added her own anxiety to the panic already present in a complicated delivery. The patient felt seen. The resident felt guided rather than tested.
In the 1990s, a terrible scooter accident left Dr. Samal with a severe head injury that required hospitalisation at a neurology centre in Nagpur. Dark doubts circulated around the campus about whether she would ever regain the sharp cognitive function her surgical work required. Weeks after the accident, she was back in the hospital: delivering babies, performing complex surgeries, and guiding postgraduate students through their theses. The doubting voices were answered by the only answer that actually matters in medicine: the immediate resumption of the work.
The departmental headship came with its own difficulty. When Dr. Chhabra was elevated to Dean in 2007, Dr. Samal was initially passed over. Her decades of service, her clinical excellence, and her relentless mentoring had apparently not been sufficient to determine the succession in her favour. She found this deeply painful. Crucially, she did not accept it passively. She wrote a letter to the management — sincere, highly specific, and utterly unvarnished, setting out exactly what she had done for MGIMS across three decades. Honest without being aggrieved, fiercely assertive without being demanding. The management read it, reconsidered, and appointed her. The quiet woman who had never sought the spotlight was, when the moment required it, more than capable of making the case for exactly what she deserved.
The home she and Dr. Khan built in Sevagram was named Saraswati Sadan — invoking the goddess of knowledge and learning. Students constantly came to them seeking advice not just on medicine, but on life. They found a family away from family. They found two doctors who had crossed religious boundaries — he was Muslim, she was Hindu — without ceremony, simply because they had found in each other's deep values a greater commonality than any artificial boundary could mark.
Between 1983 and her retirement, she mentored twenty-one residents through their postgraduate degrees. The students who trained under Dr. Chhabra and Dr. Samal in the same department received two radically different but equally vital formations. The fiercest taskmaster taught them that clinical standards had no exceptions. The department's beating heart taught them that standards could coexist with warmth — that competence was entirely compatible with gentleness, and that a patient's unspoken fear deserved to be treated just as urgently as their documented symptom.
After retiring from MGIMS in 2008, she spent ten more years heading the department at JNMC Sawangi, followed by private practice in Wardha. Then came severe dengue encephalitis — a harrowing month in the ICU, her body tested once again. She survived. Then came the devastating death of Dr. Narendra Samal, her husband of fifty years — the man who had put her education first in 1973. On February 26, 2024, her own death arrived at home, leaving behind two sons — an orthopaedician and a physiotherapist.
She had spent fifty-two years in medicine. She loved nature and plants. She brought breakfast to young mothers who needed rest. She fed homeless women in her ward. She spoke in broken English that needed absolutely no refinement, because profound warmth requires no translation. She had never carried the air of a conventional professor. And that was, in the end, exactly what made her one of the most significant ones the institution ever had.
| 1948 | Born, 14 April, Kusupur, Odisha |
| 1970 | Completed MBBS with distinction, Srirama Chandra Bhanja Medical College, Cuttack |
| 1972 | Joined MGIMS, 1 May — Lecturer in OBG; thousand-kilometre journey from Odisha with husband |
| 1973 | Married Dr. Nasiruddin Khan (later Samal) — he was Muslim, she was Hindu; he deferred his postgraduate degree so she could study first |
| 1975 | Completed DGO, Nagpur University — top marks |
| 1976 | Completed MD Obstetrics and Gynaecology, November — rejoined MGIMS immediately |
| 1983 | Began guiding postgraduate students — twenty-one residents mentored until retirement |
| 1985 | Promoted Professor |
| 1990s | Severe scooter accident — head injury; hospitalised Nagpur; returned to surgery weeks later |
| 2007 | Appointed Head of Department — after writing letter to management challenging initial decision to pass her over |
| 2008 | Retired from MGIMS, 30 April |
| 2008 | Head of Department, JNMC Sawangi — ten years; then private practice Wardha |
| 2020s | Severe dengue encephalitis — one month in ICU; survived |
| 2024 | Died, 26 February, at home — husband had predeceased her |
A study of prevalence of hepatitis B surface antigen (HBsAg) in pregnant woman and in the cord blood of their newborns
Clinical pathological analysis of recurrent abortions with special reference to hysterography.
Use of hyoscine -n butylbromide (buscopan) as a cervical spasmolytic agent in acceleration of labor
Clinic pathological evaluation of infertility cases with special reference to endometrial glycogen
Prediction of fetal outcome in threatened abortion by maternal serum alpha fetoprotein
Ultrasound evaluation of bleeding in early pregnancy
Endometrial aspiration cytology study and its correlation with histopathology
Clinic pathological bacteriological profile of genital tuberculosis
Comparative study of Para cervical block in labor using bupivacaine lidocaine
Clinic pathological analysis of dysfunctional uterine bleeding
Estimation of fetal weight by Dawn’s method, Johnson’s method and ultrasonographic arson’s formula
Comparative study of oral prostaglandin (PGE) versus intravenous oxytocin in induction and augmentation of labor
Efficacy of transvaginal salpingo-sonography for evaluation of fallopian tube patency in comparison to hysterosalpingography and laparoscopic chromopertubation
The detection of hyperprolactinemia through serum prolactin estimation in infertility cases and its management
Clinical and pathological study of post-sterilized women undergoing hysterectomy with special reference to fallopian tube
Comparative study of ovulatory pattern in spontaneous and induced cycles in infertile women
Comparative study of prostaglandin E1 analogue(misoprostol) vs. prostaglandin E2 dinoprostone for induction of labor
Doppler velocimetric study of maternal uterine, fetal umbilical and middle cerebral artery in hypertensive and normotensive pregnancy
A comparative study of oral mifepristone and vaginal misoprostol to vaginal misoprostol alone for termination of early pregnancy
Comparative evaluation of efficacy and safety of tranexamic acid with ethamsylate and tranexamic acid in control of menorrhagia
Dr. Pradip Sambarey
MD Obstetrics and Gynaecology, Government Medical College Nagpur (1982) ·
PhD (Male Infertility) Nagpur University

Reader in Obstetrics and Gynaecology · Six Years at Sevagram · Ten Thousand Surgeries, A Hundred Thousand Hours of Teaching
Pradip Sambarey was born on December 30, 1955, in Nagpur, to Wamanrao — a stern yet fair central government officer — and his soft-spoken wife. He attended Jamdar Primary School and CP & Berar High School, displaying the quiet, relentless diligence that would distinguish his entire career. In his tenth-grade board examinations, he stood fifth in the entire state. A prestigious national merit scholarship arrived, and stayed with him through his years at Government Medical College, Nagpur.
His internship took him to Kuhi, a remote village where obstetric emergencies decidedly did not move slowly. Inside mud-walled labour rooms, alongside his friends Ajit Pradhan, Dilip Magarkar, and Mohan Gupte, he encountered medicine in its most unmediated form — the desperate cries of newborns, the anxious eyes of expectant mothers, and sudden complications that no textbook had fully prepared him for. This was where he learned that medicine was human, highly unpredictable, and deeply personal.
He graduated MBBS from GMC Nagpur in 1977. In a cohort where most male peers gravitated toward General Surgery or Medicine, he chose Obstetrics and Gynaecology — then considered almost exclusively a woman's domain. It was a choice that drew quiet scepticism. "During our final MBBS," he recalled, "the three of us — Deshpande, Laul, and I — scored remarkably well in Obstetrics and Gynaecology. During my internship, I delivered quite a few babies, and somewhere along the way, Gynaecology simply began to draw me in." He earned his MD in 1982 and arrived in Sevagram on March 1, 1984.
He stepped into a department in massive transition. The formidable Dr. Mrudula Trivedi was at the helm, her ward running with clipped precision. Dr. Shakuntala Chhabra was intensely managing associate professor responsibilities alongside her massive rural outreach projects. Dr. Samal, ever composed, served as Reader. The clinical setting was substantial for a rural teaching hospital: 111 teaching beds, 27 reserved for newborns, five labour beds in the department, and two additional beds at the district hospital.
He was a fellow GMC Nagpur alumnus alongside Dr. S.P. Kalantri in Medicine and Dr. Suhas Jajoo in Surgery — familiar faces that made Sevagram's unique combination of Gandhian austerity and fierce intellectual camaraderie easier to navigate. His clinical approach was methodically paced and deeply measured. Over time, some patients began actively bypassing senior faculty to seek his opinion specifically. This dynamic was noticed, and duly noted, though not always warmly by those who had been bypassed.
The research direction that would define his scholarly contribution arrived through an adjacent discipline. Dr. K.N. Ingle, Professor of Physiology, ran a laboratory specialising in male infertility testing. Sambarey shifted his ongoing PhD work to MGIMS and redirected it toward the uncharted territory that Ingle's laboratory opened — exploring male infertility across its full dimensions: biological factors, psychological stressors, age gaps between partners, inter-spousal relationships and their impact on sperm count, and traditional remedies as adjunct approaches in selected cases.
Typing resources were scarce in Sevagram. He typed his massive thesis himself — binding, re-binding, and painstakingly correcting errors through the long, solitary process of preparation. When he finally left in January 1990, official confirmation had not yet arrived. Months later, a letter from Nagpur University reached him: his PhD had been officially approved, the viva waived, and the certificate was in the mail. He became the very first obstetrician in the region to hold a doctoral degree in male infertility.
In 1989, the Maharashtra Public Service Commission advertised new posts. He applied. His interview lasted forty minutes; the panel was thoroughly impressed, and he was offered a position in Pune. "Had they sent me to Nanded or Ambajogai, I would have stayed in Sevagram." It was not dissatisfaction with MGIMS that drove his departure, but the specific geography of the offer combined with the needs of his growing family. Their daughters were young, and Pune promised educational opportunities that Sevagram, for all its clinical richness, could not match. His wife, Dr. Prajakta Divekar — who had joined Sevagram as a registrar in Ophthalmology and risen to Associate Professor — left with him.
From Sevagram, he moved to BJMC Pune in 1990, spending twelve years there. Then Dhule in 2002, where he rose to Professor. Then Ambajogai in 2012. Finally, he returned to BJMC Pune in 2015 as Head of Obstetrics and Gynaecology — leading the department for four years with the quiet, unshakeable authority of someone who had been building toward that role since standing in a mud-walled labour room in the mid-1970s. He retired on December 31, 2019.
His younger daughter Avanti had been delivered in Sevagram by Dr. Swarnalata Samal — a small, deeply poignant link between the professional and the personal. The very institution that had shaped his clinical hands had also, in the most literal way available, brought his daughter into the world. Avanti earned her PhD in Bioinformatics and continues her research in Michigan. Shiwani works in Computer Science in Seattle.
Ten thousand Caesarean sections. But a lifetime of teaching that dwarfed them. The hundred thousand hours of teaching was the actual work.
| 1955 | Born, 30 December, Nagpur — father central government officer |
| 1973 | Stood fifth in Maharashtra state board examinations — national merit scholarship |
| 1977 | Completed MBBS, GMC Nagpur — internship in mud-walled labour rooms, Kuhi village |
| 1982 | Completed MD Obstetrics and Gynaecology |
| 1984 | Joined MGIMS, 1 March — Lecturer in OBG |
| 1986 | Promoted Reader |
| 1987 | Began PhD in male infertility — Physiology laboratory with Dr. K.N. Ingle; typed entire thesis himself |
| 1990 | Left MGIMS, 31 January — BJMC Pune; PhD certificate arrived months later — viva waived |
| 1990 | First obstetrician in the region with doctoral degree in male infertility |
| 2002 | Professor, Government Medical College, Dhule |
| 2012 | Government Medical College, Ambajogai |
| 2015 | Head of Department, BJMC Pune — four years |
| 2019 | Retired, 31 December — 42-year career; approximately 10,000 Caesarean sections |
Dr. Shubhada Jajoo
MD Obstetrics and Gynaecology, Solapur (1983)
PhD JNMC Savangi Wardha (2019)

Shobha Tapade — she became Shubhada Jajoo after her marriage — was born on June 13, 1957, in Tadavale, a small village near Barshi in Maharashtra. Her parents, Ratanlal and Godavari, had eleven children and severely limited means. She was the youngest. The family could not always sustain school fees. There were literally no chairs to offer when the prominent Jajoo family came to visit.
The dream crystallised on a specific day during a visit to Beed. Her mother fell ill, and Shubhada watched the doctor at work — calm, composed, commanding absolute respect without effort. A door opened in her mind. If medicine was out of reach, she told herself, life itself was simply not worth living. This was not childhood melodrama; it was the cold determination of a child who had identified the one thing capable of changing her entire trajectory.
Her elder brother Lakshminarayan took her to Barshi; her brother-in-law provided a roof and bore the cost of her education. She ranked first in her school and sixth in the entire Barshi division — an achievement that required a daily six-kilometre walk to a boys' mathematics class, because no mathematics class existed for girls. During her pre-degree years at Dayanand College in Solapur, the hostel served dry rotis and cold, watery dal, and no one called to check whether she was managing. She managed. In 1976, she entered Dr. Vaishampayan Memorial Government Medical College, Solapur, and earned her MBBS in 1980 with medals for academic excellence.
The MD seat at GMC Nagpur seemed ideal — her husband was pursuing super-specialisation there, her in-laws were in nearby Wardha, and her friends were in Nagpur. The department's reality pointed elsewhere. It was steeped in vicious politics and power struggles that had nothing to do with medicine. Just one month in, she made the staggering decision to leave. Leaving meant risking the entire specialisation she had been working toward since childhood. But some decisions come from a bedrock of self-respect that cannot be argued with. She returned to Solapur on faith alone.
In 1983, she secured an MD seat in Solapur. The civil hospital provided a relentless stream of gynaecological and obstetric emergencies that honed her clinical instincts rather than breaking her. By 1985, armed with her MD, she moved to Wardha, stepped briefly into the Civil Hospital post vacated by Dr. Rani Bang, and applied to MGIMS. Why MGIMS? She had a ready answer: "Because that's where the academics were."
She joined MGIMS on October 1, 1985, exactly seven months pregnant. She had applied for the post in March and appeared before the interview board in September — a formidable panel that included Dr. Sushila Nayar, Dr. B.S. Chaubey, Dr. M.P. Dwivedi, and four others. Selected from three highly qualified candidates, she arrived carrying her daughter Rucha just two months ahead of the birth. Her maternity leave lasted exactly six weeks. Then she was back, the newborn in the background and the gruelling hospital work in the foreground, the two massive demands running simultaneously.
She joined Dr. Swarnalata Samal's unit and found in her superior a model of professional character that was the exact opposite of everything the toxic GMC Nagpur department had represented — humble, self-effacing, allowing residents and faculty to take full credit for their work. For Shubhada, who had grown up in a household where the generosity of others had made her education possible, this quality resonated deeply.
She introduced magnesium sulphate for treating eclampsia — a direct, vital departure from the lytic cocktail that had been standard — and patient outcomes immediately improved. She taught Dr. Samal how to perform laparoscopic tubectomies, a skill her mentor would carry forward for the rest of her career. She brought tight organisational structure to the department's examination processes. The clinical pace was relentless: with only two units in the department, every other day was OPD or surgery, interspersed with deliveries, emergency C-sections, medical student lectures, and postgraduate training.
She was promoted to Reader in August 1989. She would finally lead her own unit, mentor postgraduates, and conduct independent research. The autonomy she had been working toward for years was finally within reach. Four days after Christmas in 1989, she abruptly resigned. Pressure from her in-laws to leave Sevagram and establish a private practice in Wardha had mounted, and the family decision was made.
She turned the family home into an eight-bed hospital, acquired an ultrasound machine and a laparoscope, and began building again from scratch. Her husband Suhas eventually joined her. In 2001, academia called her back — she began teaching part-time at JNMC Sawangi. By 2011, she was a full Professor, a postgraduate guide, and a PhD holder.
The university ceremony at which she received her PhD provided a moment of profound poetic justice. At the exact same ceremony, her younger daughter Shruti received a gold medal for standing first in Anaesthesiology. Union Minister Nitin Gadkari presided over both awards. The woman who had walked six kilometres for a mathematics class was now being formally recognised alongside the daughter who had followed her into medicine, standing entirely equal beside her.
Her elder daughter Rucha — born just two months after her mother joined MGIMS in 1985 — became a laparoscopic surgeon, following her father. Shruti became an anaesthesiologist, following her mother into academia. In October 2024, Dr. Shubhada Jajoo retired from her academic post at JNMC Sawangi. She has finally stepped away from Obstetrics, focusing entirely on Gynaecology — trading the relentless midnight emergencies of the labour room for the measured precision of scheduled surgery. After a lifetime anchored to hospital wards, she is finally travelling, discovering the vast geography of India at her own pace. The village girl from Tadavale who had no chairs to offer when guests visited is still making the dream true today.
| 1957 | Born, 13 June, Tadavale, near Barshi — youngest of eleven siblings; father Ratanlal, mother Godavari |
| 1970s | Walked six kilometres daily to a boys’ mathematics class — no class existed for girls |
| 1976 | Entered Dr. Vaishampayan Memorial Government Medical College, Solapur |
| 1980 | Completed MBBS, Solapur — medals for academic excellence |
| 1981 | MD seat, GMC Nagpur — left after one month; toxic departmental politics; returned to Solapur on faith |
| 1982 | Married Dr. Suhas Jajoo, 26 February — Wardha’s Gandhian family; no chairs to offer when they had come to visit |
| 1983 | MD Obstetrics and Gynaecology, Solapur — relentless civil hospital emergencies |
| 1985 | Joined MGIMS, 1 October — seven months pregnant; daughter Rucha born two months later |
| 1985 | Introduced magnesium sulphate for eclampsia — replacing lytic cocktail; patient outcomes immediately improved |
| 1989 | Promoted Reader, August |
| 1989 | Left MGIMS, 29 December — family decision; built eight-bed hospital in Wardha with husband |
| 2001 | Began part-time teaching, JNMC Sawangi — academia calling her back |
| 2011 | Full Professor and postgraduate guide, JNMC Sawangi · PhD awarded — at same ceremony as daughter Shruti’s gold medal |
| 2024 | Retired from JNMC Sawangi, October — continues practice with husband and daughter Rucha in Wardha |
Dr. Sudershan Kumar Dhawan
MD Ophthalmology, PGI Chandigarh (1969)

Associate Professor of Ophthalmology · Six Years at Sevagram · The Lens Through Which Students Learned to See
A life in medicine is often defined by the specific lens through which a physician views the world and the people within it. For Dr. Sudershan Kumar Dhawan, that lens was crafted early, polished by a heritage of duty, and focused sharply on the margins of society where care was needed most.
Born on November 2, 1943, in Sarai Amanat Khan—a historic village situated twenty-nine kilometers southwest of Amritsar—Sudershan entered a family deeply rooted in the Khatri tradition of service. It was a lineage where public duty and administration went hand in hand. His father, Shri Hukam Chand Dhawan, served as the Deputy Director of Health Services in Haryana. Shri Hukam Chand was a man of unshakeable discipline, casting a long, respectable shadow over his household in Chandigarh. Yet, he managed to foster an atmosphere where strict order was beautifully tempered by grace and intellectual curiosity.
Young Sudershan inherited this foundational resolve, but he also brought his own distinct spark to the family dynamic. It was the kind of vibrant, mischievous energy visible at the corner of an eye just before a smile breaks—a warmth that would later become his hallmark in hospital wards and remote village camps alike. He completed his foundational schooling in the disciplined environs of Ferozepur Cantt and his intermediate years in Hoshiarpur, gradually building the academic rigor required for the medical profession. He subsequently entered the prestigious Medical College in Amritsar, graduating with his MBBS degree in 1966, stepping into a newly independent India that desperately needed skilled clinicians.
Driven by a desire to specialize and refine his surgical skills, Dr. Dhawan entered the Postgraduate Institute of Medical Education and Research (PGI) in Chandigarh to pursue his MD in Ophthalmology. There, he trained under the watchful eye of Dr. R.S. Gupta, a mentor who demanded excellence. Dr. Dhawan’s thesis, which meticulously examined the complexities of glaucoma surgery, set the stage for a career defined by precision and sight restoration.
It was during his grueling residency at PGI that the defining ethos of his career began to take shape. He did not confine his learning to the sterile, well-lit corridors of the premier institute. Instead, he traveled extensively around the peripheries of Chandigarh, conducting population screening for blinding eye disorders. This was the birth of his outreach instinct—an irrepressible drive to take medicine to the patient rather than waiting for the patient to reach the hospital. It was a philosophy that would later propel him into the deepest, dustiest corners of Vidarbha, and one that would never leave him across the decades and continents that followed.
Crucially, PGI was also where the most important partnership of his life began. It was there he met Dr. Chanchal. Originally from Shimla, she had studied in Patiala and carried herself with the unshakable calm of someone who knew precisely who she was and what she valued. Where he was dynamic and expressive, she was steady and serene. They recognized in each other a shared dedication to their craft and a complementary spirit. They were married in 1970, sealing a partnership that would serve as the bedrock of their personal and professional lives. Two years later, fueled by a desire to serve where they were needed most, the young couple left the comforts of Chandigarh for a remote village in central India.
When the Dhawans arrived at the Mahatma Gandhi Institute of Medical Sciences (MGIMS) in Sevagram in January 1972, the institution was a mere three years old. It was a fledgling medical college set in a profoundly rural landscape, where the dust of the plains met the towering ideals of its founders. At that time, its Gandhian values were its most developed infrastructure; physical resources were scarce, and the challenges of rural healthcare were monumental.
Upon arrival, they were introduced to Dr. Anant Ranade, an Ayurved Visharad. Though he lacked a modern allopathic medical degree, Dr. Ranade was a local legend who had single-handedly restored sight to thousands of villagers through makeshift eye camps across Maharashtra. His reputation, built entirely through relentless clinical skill and deep compassion, humbled the highly trained new arrivals immediately. It was a profound lesson in the realities of rural medicine: community trust and practical outcomes often mattered more than formal pedigrees.
The transition to this austere environment was softened by the immense warmth and visionary leadership of Principal I.D. Singh and the formidable Dr. Sushila Nayar. Under their guidance, the village slowly ceased to feel like a remote exile and transformed into a deeply cherished home. Together, Dr. Sudershan and Dr. Chanchal Dhawan took on the Herculean task of building the ophthalmology department from the ground up, shaping both its clinical protocols and its academic curriculum during its most formative years.
The Dhawans quickly realized that in a place like Sevagram, the hospital could not be the sole locus of care. They took the ophthalmic department to the people, organizing and executing expansive eye camps in the most remote, underserved corners of the Vidarbha region. This included venturing into dense, forested areas troubled by Naxalite insurgency, such as Gadchiroli, Bhamragarh, and Sironcha.
These expeditions were not without significant risk, requiring delicate navigation of both geographical isolation and regional volatility. Dr. Dhawan personally led teams of young registrars, including Dr. Sanjay Gadre and Dr. D.P. Singh, venturing into the hinterlands. He carried the dual burden of ensuring the absolute safety of his team while guaranteeing the surgical success of their mission. Under his leadership, these grueling rural camps were never treated as mere supplementary activities or extracurricular charity; they were integrated directly into the postgraduate training. The camps were the curriculum, offering the most effective, hands-on delivery of medical education while providing miraculous, life-changing interventions for tribal populations who had been blind for years.
As an educator, Dr. Dhawan was a force of nature. His theory lectures were not dry recitations of medical textbooks; they were captivating performances. He animated his teachings, texturing them with real, complex cases drawn from the wards, and laced his delivery with a sparkling, dry wit that kept even the most exhausted, sleep-deprived residents entirely attentive.
However, his true mastery as an educator was revealed in the operating theatre. He believed in building the surgeon’s hand alongside the physician’s mind. His philosophy was clear and methodical: "Observe first. Assist next. Then do it yourself." Surgery, especially ophthalmic surgery in that era, was an incredibly tense endeavor, but students universally found his presence beside them at the operating table more reassuring than intimidating.
When a treacherous retinal detachment presented itself, he did not panic or take over abruptly; he broke the procedure down for his students like a logical puzzle. When a resident struggled with a delicate corneal suture, he gently guided their trembling hands until the microscopic stitch settled flawlessly, like silk. He possessed the rare, vital ability to correct a student’s mistake without crushing their spirit—the hallmark of a master teacher who understood that a young surgeon's confidence is itself a critical clinical instrument.
Despite their monumental contributions to building the department, the postgraduate program they had envisioned for Sevagram encountered insurmountable bureaucratic hurdles. Dr. L.P. Agarwal, a doyen of ophthalmology at AIIMS and an advisor to Dr. Nayar, strictly adhered to rigid academic guidelines and refused to approve Dr. Dhawan's promotion to Professor. The rationale was purely technical: the position required more formal years in a recognized teaching hospital than Dr. Dhawan had accumulated on paper, entirely discounting the massive, untraditional clinical volume he had managed in the rural camps.
It was a deeply frustrating administrative roadblock, but serendipity intervened. The Government of Maharashtra, seeking to modernize its medical education system, advertised a large number of faculty posts and deliberately looked beyond the usual red tape to find proven clinical leaders. Dr. Dhawan applied, and his undeniable track record spoke for itself. He was selected.
In 1977, leaving behind a campus that had given them six years of foundational, life-altering work, he and Dr. Chanchal packed their bags and moved to Pune. He was appointed as Professor and Head of Ophthalmology at B.J. Medical College, with Dr. Chanchal joining as an Associate Professor. Their arrival marked a historic shift for the institution, as they were the very first full-time staff members appointed to replace the outdated honorary system, bringing a new era of academic rigor and full-time dedication to the department.
Their tenure in Pune was relatively brief before duty called them into the center of a profound medical crisis. In January 1981, both Dr. Sudershan and Dr. Chanchal Dhawan were urgently transferred to Government Medical College (GMC) in Nagpur. The institution was reeling from a devastating and highly publicized tragedy: an unfortunate incident in which fourteen patients had irreversibly lost their eyesight following botched cataract surgeries. The catastrophe had resulted in the immediate suspension of all three existing unit heads, creating a massive vacuum of leadership, skill, and—most importantly—public trust.
The Dhawans stepped into this volatile, tense environment with characteristic resolve. They knew that trust could not be rebuilt through administrative memos; it had to be earned back, one successful surgery at a time, directly in the community. Operating under the National Programme for Control of Blindness, they secured a mobile ophthalmic unit from the Government of India.
Over the next five years, they launched a breathtakingly ambitious campaign of outreach across the most isolated areas of the state. The sheer volume of their work was staggering: they organized and conducted an average of 370 eye camps per year. These camps not only restored sight to thousands of marginalized citizens, effectively healing the fractured relationship between the government hospital and the public, but they also served as an unparalleled, intensive training platform for a new generation of postgraduate students. Under Dr. Dhawan’s leadership, the unit’s clinical performance was adjudged the best in the entire state of Maharashtra for five consecutive years. In recognition of this extraordinary, sustained community service, the Government of Maharashtra honored Dr. Dhawan with the prestigious “Best Surgeon” award for four consecutive years.
During his years in Nagpur, Dr. Dhawan became an iconic figure, remembered as much for his distinct style as his surgical brilliance. In the sterile corridors and bustling Eye OPD of GMC Nagpur, he was always impeccably turned out. He defied the drab aesthetic of the era, wearing vividly colored T-shirts paired with sharply tailored jeans, his shoes polished to a mirror finish. He could often be seen steering his pristine white Ambassador car with one hand, waving familiar, cheerful greetings with the other.
Inside the hospital walls, however, he was an uncompromising disciplinarian. Protocols were sacred, appointments were rigidly expected, and junior doctors knew that doors were to be knocked upon before entering. Yet, the moment he stepped out of the city and into the dust of the village camps, he shed all formality. In the rural hinterlands, he was deeply egalitarian—sitting on the floor to share simple meals with the locals, exchanging jokes in the vernacular, and casually borrowing music cassettes from his students to play during long, bumpy jeep rides. He understood that structure and spontaneity served vastly different purposes, and he possessed the rare emotional intelligence to know exactly which approach each situation required.
Having conquered the challenges of rural and urban Indian healthcare, the Dhawans embarked on an entirely new chapter in 1985, moving to Riyadh, Saudi Arabia. What was perhaps initially viewed as a temporary international stint evolved into a monumental thirty-seven-year tenure at the National Hospital in Riyadh. This span of continuous professional service in a single overseas institution is longer than most medical careers in their entirety.
Throughout his nearly four decades in the Middle East, Dr. Dhawan endeavored to uphold the absolute highest standards of professional excellence. He viewed himself not just as an expatriate physician, but as a true ambassador of Indian medical expertise. Despite his deep integration into the Saudi medical community, his heart remained tethered to his roots. "It was a matter of great pride for me to hoist the Indian national flag on 15th August 2021 at a ceremony attended by hospital staff of diverse nationalities, including Saudi colleagues," he recently recalled in a heartfelt message.
In 2011, his exceptional global contributions were formally recognized when he was conferred the Hind Ratan Award, celebrating his achievements as a member of the Indian diaspora. Reflecting on this massive chapter of his life, he described his years in Riyadh as "deeply fulfilling and professionally enriching." Finally, having given their all to the profession, Dr. Dhawan and Dr. Chanchal returned to Pune in March 2022 to enjoy a well-earned retirement.
It is impossible to tell the story of Dr. Sudershan Dhawan without speaking of Dr. Chanchal Dhawan. She was, by universal testimony of all who knew them, his perfect complement and his greatest strength. Where he could effortlessly command a crowded room with his dynamic presence and sharp wit, she softened the environment with her calm, steady warmth. She never raised her voice in anger, never sought the spotlight for her own accomplishments, yet her influence on the hundreds of students who passed through their departments was profound and lasting. It was the particular, enduring kind of influence that quiet grace produces in those who are fortunate enough to be in its proximity long enough to absorb its high standards.
Their partnership was deeply intertwined with the geography of their careers. Their daughter, Samridhi, was born in Sevagram in 1977, a beautiful parting gift from the rural campus that had given them six years of foundational work. Their son, Sidhartha, was born a few years later in Pune on December 13, 1980. Through the dust of the Vidarbha camps, the high-stakes crisis in Nagpur, and the decades of expatriate life in Riyadh, Dr. Chanchal was the steadying force. On October 20, 2023, Dr. Chanchal Dhawan passed away in Pune. She had been present through all of it—the calm that completed the sparkle, the unshakeable grace that made the massive structure of their shared life habitable and beautiful.
Today, Dr. Dhawan’s students are scattered across the globe, leading departments and running practices on multiple continents. Yet, when they look back on their training, they remember two specific things above all else. First, they remember the awe of watching the restored sight of marginalized patients who came to the dusty eye camps in Gadchiroli and Sironcha, leaving able to see a world that had been dark to them for years.
Second, they remember the profound privilege of being taught by a man who fundamentally understood that vision—both the clinical mechanics of the eye and the human empathy required to treat the soul—was what medicine was actually for. The Dhawans had acted as lenses, as one moving tribute beautifully put it, through which generations of young doctors learned to see not just the pathology of disease, but the dignity of humanity. It was a lesson they taught flawlessly, primarily because, between 1972 and 1977, in a remote village with more ideals than infrastructure, they had learned it so perfectly themselves.

| 1943 | Born, 2 November, Sarai Amanat Khan, near Amritsar — father Deputy Director of Health Services, Haryana |
| 1966 | Completed MBBS, Medical College Amritsar |
| 1969 | MD Ophthalmology, PGI Chandigarh — thesis on glaucoma surgery under Dr. R.S. Gupta |
| 1970 | Married Dr. Chanchal — from Shimla; studied in Patiala |
| 1972 | Joined MGIMS, 5 January — Lecturer in Ophthalmology; with Dr. Chanchal |
| 1972 | Eye camps — Gadchiroli, Bhamragarh, Sironcha; Naxalite-affected areas of Vidarbha |
| 1977 | Daughter Samriddhi born in Sevagram |
| 1977 | Left MGIMS, 1 December — promotion blocked by Dr. L.P. Agarwal and Goa Medical College |
| 1977 | Professor and Head of Ophthalmology, BJ Medical College, Pune — Dr. Chanchal as Associate Professor |
| 1981 | Moved to GMC Nagpur — following successful MPSC examination |
| 1985 | Joined National Hospital, Riyadh, Saudi Arabia — thirty-seven years |
| 2022 | Returned to Pune, March |
| 2023 | Dr. Chanchal Dhawan died, 20 October, Pune |
Dr. Chanchal Dhawan
MS Ophthalmology, PGI Chandigarh (1972)

Lecturer in Ophthalmology · Five Years at Sevagram · The Calm That Completed the Sparkle
Chanchal grew up in Shimla, a hill town whose particular quality of light, crisp air, and rolling landscape grants those raised there a permanent relationship with beauty and calm. It is a quietness that tends to persist in the bones, no matter where life takes them. She completed her MBBS at Medical College, Patiala in 1968, moving from the cool hills to the sprawling plains of Punjab, before entering PGI Chandigarh to pursue her MS in Ophthalmology.
At PGI, she and Dr. Sudershan Dhawan found themselves in the same demanding department. She was two years his junior. Their first conversations were rooted in the rigours of medicine — the complexities of the cornea, the delicate pressures of the anterior chamber — but they evolved into conversations about meaning, purpose, and the shape of the lives they wanted to lead. They were married in 1970. When Sudershan left for Sevagram in January 1972, Chanchal remained behind to complete her MS. When her degree was secured, she followed him into the unknown.
Dr. Chanchal Dhawan arrived in Sevagram in January 1973. The transition from the cool elevations of Shimla and the modern grids of Chandigarh to the fierce heat and red dust of Wardha was stark. MGIMS was barely three years old — a fledgling institution where Gandhian ethos was far more developed than its physical infrastructure. The couple was immediately humbled by the presence of Dr. Anant Ranade, the Ayurved Visharad whose legendary eye camps had restored sight to thousands of villagers across Maharashtra without the formal credentials that usually authorised such work. His presence taught a vital lesson: sheer commitment and raw skill could achieve miracles that institutional structures could not.
Joining as registrar and rising quickly to Lecturer, Dr. Chanchal Dhawan helped transform the department into a genuine partnership. For the next five years, two ophthalmologists of vastly different temperaments and entirely complementary strengths built the clinical and educational foundations of a specialty that had not previously existed at the institute.
If he was Mohammad Rafi, she was Asha Bhosale. Dr. Bajrang Prasad Pandey, a 1970 batch student who trained under both Dhawans and later retired as Professor of Pharmacology from BHU, offered this precise comparison: Rafi's voice had a soaring, undeniable presence. Bhosale's was just as brilliant, but operated in a different register — gentler, sharper, and completely its own. The point was not that one was lesser. The point was that they were genuinely different, each fundamentally necessary, harmonising into a duet that neither could have sustained alone.
Her teaching had a rhythm all its own — quieter than her husband's theatrical, animated performances, but no less thorough. In the operating theatre, her quietness was her greatest teaching tool. Ophthalmology is a discipline of microscopic margins, where a tremor of the hand can mean the difference between light and darkness. When a student hesitated over a delicate procedure, her steady presence beside them was an anchor. She did not berate or rush; she instructed through the transmission of calm, teaching them that a surgeon's composure is just as critical as the sharpness of their scalpel.
She was a vital force in the eye camps held in Gadchiroli, Bhamragarh, and Sironcha — remote districts of Vidarbha deeply troubled by Naxalite activity, where specialist care was an unheard-of luxury. In these villages, the Dhawans shed the door-knocking institutional formality of the hospital. They ate simple meals with the locals, shared long conversations under the shade of trees. Dr. Chanchal brought to these dusty camps the exact same quality she brought to the sterile wards: boundless warmth without the need for performance, and elite competence without a trace of arrogant display.
In 1977, the Sevagram campus gave the family its first child, Samriddhi. The village that had provided the crucible for their professional formation had now given them a family.
They moved to Pune — she as Associate Professor of Ophthalmology at BJ Medical College alongside her husband. Then to GMC Nagpur in 1981. Then, unexpectedly, to Saudi Arabia: thirty-seven years at the National Hospital in Riyadh. For three and a half decades, Dr. Chanchal Dhawan applied the same precision and deep empathy she had honed in Sevagram's bare-bones department to the gleaming clinics of the desert capital. The grace that had marked her presence in a rural Indian hospital persisted in the modern global one.
The students she had formed in Wardha were growing into professors, department heads, and leading practitioners across India, the UK, and the US. They carried her quiet voice in their own clinical habits — the careful, unhurried slit-lamp examination, the quality of deep attention that ensures every patient is treated as a breathing human being rather than a fascinating medical case.
Dr. Chanchal and Dr. Sudershan Dhawan returned to Pune in March 2022, carrying the accumulated weight and wisdom of a life beautifully lived. They had been by each other's side since PGI Chandigarh — since the conversations about medicine had turned into a marriage, and that marriage had turned into a sprawling life across Shimla, Patiala, Chandigarh, Sevagram, Pune, Nagpur, and Riyadh.
She had barely begun to inhabit this final, restful chapter. On October 20, 2023, Dr. Chanchal Dhawan passed away suddenly in Pune. Without her quiet grace, the ophthalmology department the Dhawans built from the red dirt of Sevagram would have been a profoundly different, and undoubtedly lesser, place. She had grown up in the Shimla hills where the light is particular and the calm runs deep into the earth. She carried that light and that calm to every patient she touched.
| 1946 | Born, Shimla — grew up in the hills whose calm she carried through every chapter of her life |
| 1968 | Completed MBBS, Medical College Patiala |
| 1972 | Completed MS Ophthalmology, PGI Chandigarh |
| 1970 | Married Dr. Sudershan Kumar Dhawan — partnership that would span half a century and multiple continents |
| 1973 | Joined MGIMS, 1 January — Registrar, then Lecturer in Ophthalmology |
| 1973 | Eye camps — Gadchiroli, Bhamragarh, Sironcha; Naxalite-affected areas of Vidarbha |
| 1977 | Daughter Samriddhi born in Sevagram |
| 1978 | Left MGIMS, 28 January — Associate Professor, BJ Medical College Pune |
| 1981 | GMC Nagpur — following transfer orders during infectious disease outbreak |
| 1985 | Joined National Hospital, Riyadh, Saudi Arabia — thirty-seven years |
| 2022 | Returned to Pune, March |
| 2023 | Died, 20 October, Pune — suddenly; likely heart attack |
Dr. Vishwanath Chaturvedi
MS Otolaryngology, AIIMS New Delhi (1970)

Professor & Head of Otolaryngology · Medical Superintendent · Thirty Years at Sevagram · The Man Who Came Back
Vishwanath Chaturvedi was born on November 2, 1941, in Mumbai, into a traditional Brahmin family with roots in Mathura. He studied at Ramjas College, Delhi University, entered AIIMS in 1961, and graduated MBBS in 1965. He completed his MS in ENT from AIIMS in 1970, working subsequently as Assistant Surgeon at Safdarjung Hospital before taking up a lecturership in ENT in November 1971.
In the Paediatrics ward during his house job years, he had been the only man among seven house officers. His tall, handsome stature and deep resonant voice set him apart. Pushpa Abhichandani noticed. They married in June 1971 — an intercaste union quietly resisted by his traditional family, quietly navigated by Pushpa through the patient work of connection rather than confrontation.
Dr. Sushila Nayar, building MGIMS's clinical faculty in 1972, asked Dr. Santosh Kumar Kackar, head of ENT at AIIMS, for recommendations. Kackar suggested Chaturvedi. On February 17, 1972, he and Pushpa boarded a train to Sevagram, unaware in any precise sense of what awaited them.
He looked at his payslip, turned to Pushpa, and apologised for bringing her to Sevagram. ₹650 per month — less than he had earned in Delhi. The accommodation assigned to them on arrival had turned out to be a mud-plastered hut near Gandhiji's ashram. They sought better arrangements, moved through the guesthouse, the boys' hostel where he served as warden, Ramkrishna Colony, Vivekananda Colony, before finally building their own home in Dhanwantari Colony in the early 1990s. The journey from the hut to the home took nearly twenty years.
Pushpa did not hold the apology against him. When the offer came from Bombay in 1975 — a Reader's post at Grant Medical College, the fast-paced city life, the salary that would have made ₹650 seem very far away — it was the purpose-driven life of Sevagram that proved stronger. He resigned eight months after joining Grant Medical College and came back. He stayed for thirty years.
MGIMS had no dedicated ENT department when he arrived. He shared space initially with Dr. Hariharan, treating patients in the dental OPD and admitting cases to the surgery ward. He and Dr. Ravinder Narang would wait together at Babulal's canteen for patients arriving by bus from the surrounding villages.
He rose through the institutional ranks: Reader in 1974, Associate Professor in 1979, Professor in 1985. ENT separated from Surgery at Nagpur University in 1978. The MS programme launched in 1980 and its first graduate emerged in 1983. Between 1982 and 2001, he mentored twenty-six postgraduate students — Dr. Ravindra Behl of the 1974 batch as his first, Dr. S. Shiral as his last. Over three decades, he produced more than a hundred research papers.
In 1981, he accepted a faculty position in Benghazi, Libya, heading the ENT department at Hawari Hospital for two years. Mrs. Chaturvedi served simultaneously as Associate Professor at Benghazi Children's Hospital. He returned to Sevagram after his leave, revisiting Benghazi as a visiting professor in later years.
His lectures were memorable in the specific way that great teaching is memorable — not because of theatrics but because of clarity. A booming voice and impeccable English were the instruments; the method was structural, breaking intricate subjects into logical, manageable sequences that ensured retention. Students who were intimidated by his initial formality typically found, over time, that the firmness was in service of their development rather than his authority.
As founding editor of the Journal of MGIMS, he brought to medical publishing the same methodical quality he applied to surgery and teaching. The inaugural issue was released in 1995; he secured the ISSN registration and established the journal's academic credibility. Before this, he had compiled MGIMS's annual reports and a collection of research papers covering the institute's first twenty-five years.
In 1999, he organised the country's first exclusive live surgical workshop on endoscopic dacryocystorhinostomy — a procedure at the intersection of ENT and ophthalmology, technically demanding, then relatively new in its endoscopic form in India. Eminent surgeons Dr. Nishi Gupta, Dr. V.P. Sood, and Dr. Steven Roy attended.
He took on administrative responsibility in June 2000 as Joint Medical Superintendent, becoming Medical Superintendent for a year. He retired formally on November 30, 2001. The lung cancer diagnosis had arrived while preparations were underway for his younger son Rajiv's wedding. He continued arriving at his office by noon through the chemotherapy — a lifelong non-smoker and teetotaler, the disease arriving without the conventional risk factors, its cruelty intensified by apparent arbitrariness.
Six weeks before his death, he symbolically transferred his responsibilities to Dr. A.P. Jain — recognising his successor in the manner of someone settling affairs with deliberateness. He died on January 14, 2002. His tenure had begun on February 18, 1972. The deep, resonant voice that Pushpa had noticed across the Paediatrics ward at AIIMS had echoed through thirty years of ENT lectures, and then fell silent in Sevagram on the fourteenth of January.
His elder son Amit, an orthopaedic surgeon, practises in Ajman and is married to Dr. Sona Dass, an anaesthesiologist — both MGIMS alumni. His younger son Rajiv, a radiologist in Abu Dhabi, is married to Dr. Deepti, a paediatric endocrinologist — also MGIMS alumni. The wedding that the lung cancer diagnosis had interrupted went forward.
Pushpa, who had bridged the intercaste gap through connection rather than confrontation, who had adapted from Delhi's comforts to a mud-plastered hut, who had accompanied her husband to Benghazi and back, who had watched him arrive at his office by noon through chemotherapy and then watched him die — has found, in her widowhood, a new passion in painting. The woman who had adapted to everything that was asked of her has made herself at home in the silence of the canvas as well.
| 1941 | Born, 2 November, Mumbai — traditional Brahmin family with roots in Mathura |
| 1961 | Entered AIIMS, New Delhi |
| 1965 | Completed MBBS, AIIMS |
| 1970 | Completed MS ENT, AIIMS |
| 1971 | Married Pushpa Abhichandani, June — intercaste union; Assistant Surgeon, Safdarjung Hospital |
| 1972 | Arrived MGIMS, 18 February — mud-plastered hut; salary ₹650; no dedicated ENT department |
| 1974 | Promoted Reader · Dr. Ravindra Behl — first postgraduate student |
| 1975 | Joined Grant Medical College, Bombay — resigned eight months later and returned to Sevagram |
| 1978 | ENT separated from Surgery at Nagpur University |
| 1979 | Promoted Associate Professor |
| 1980 | MS programme launched — first graduate 1983 |
| 1981 | Head, ENT department, Hawari Hospital, Benghazi, Libya — two years; wife simultaneously Associate Professor, Benghazi Children’s Hospital |
| 1985 | Promoted Professor |
| 1990 | Built own home, Dhanwantari Colony — eighteen years after arriving in a mud-plastered hut |
| 1995 | Founded Journal of MGIMS — securing ISSN registration; inaugural issue released |
| 1999 | Organised country’s first exclusive live surgical workshop on endoscopic dacryocystorhinostomy |
| 2000 | Joint Medical Superintendent, June — Medical Superintendent, one year |
| 2001 | Retired, 30 November — lung cancer diagnosis; continued to office by noon through chemotherapy |
| 2002 | Died, 14 January, Sevagram — thirty years to the day after his tenure began |
Vestibulo cochlear function test in cases of cervical spondylosis presenting with vertigo
Tympanometry in chronic tonsillitis and its relation with the type of infection
Study of sensorineural hearing loss
Clinico pathological study of oral submucous fibrosis
Ear Nose Throat manifestation of goiter with special reference to hearing
Clinical profile and immunology humoral response and coagulopathies in oral submucous fibrosis
Clinico audiological profile of tinnitus
Clinical profile of Bell’s palsy with special reference to site of lesion and virus antibody study against herpes simplex type 1
Clinical profile of mastoiditis as seen in rural based hospital
Study of oral lesions in rural population
Clinical profile of tracheotomy in rural area
Study of congenital sensorineural hearing loss with delayed development of speech language
Clinico pathological study of allergic rhinitis with special reference to the efficiency of various treatment modalities
Dr. Raj Mridul Raizada
MS Otolaryngology, Gandhi Medical College Bhopal (1979)

Raj Mridul Raizada was born on September 16, 1952, into a family of distinction. His father Kailash Bihari Raizada was a Supreme Court advocate based in Bhopal — a man of precision and argument whose professional formation shaped the household's values. Raj absorbed them and redirected them into medicine.
He completed his BSc from Bhopal University in 1970, his MBBS in 1975, and his MS in ENT in 1979, all from Gandhi Medical College, Bhopal. He was, as he remained throughout his career, thoroughly and proudly Bhopali — a city whose culture of grace, courtesy, and refinement he carried into every interaction. His speech carried the lilting Malwi dialect. His manner was gentle. Hospitality came naturally to him, a reflection of the warmth instilled in childhood and never set aside in the decades that followed.
He had married Rekha Raizada, an obstetrician who would build her own practice — RR Nursing Home — in Wardha. He joined MGIMS on September 10, 1980, as Lecturer, entering a department led by Dr. Chaturvedi that was finding its footing following ENT's separation from Surgery at Nagpur University in 1978. The MS programme had just launched. He would be part of its consolidation for twenty-four years.
In the operating theatre, Dr. Raizada was deliberate and unhurried — a safe surgeon, if a somewhat slow one, by the honest assessment of those who worked alongside him. The pace was not incompetence. It was the expression of a temperament that preferred precision over speed, that approached each procedure with methodical care, and that produced the near-bloodless field and unshakable calm that Dr. Ashish Varghese — a 1989 MGIMS alumnus, later Professor of Otolaryngology at CMC Ludhiana — would remember as defining qualities of the penetrating neck injury surgery twenty-five years after the night it happened.
He won the Best Paper Award at the Vidarbha AOI Conference in 1980 and again in 1981 — consecutive years, early in his career, establishing his research credibility before the slow institutional promotion ladder had moved past Lecturer. He organised ENT conferences and workshops throughout his career, understanding that the specialty's development in rural Vidarbha required building a regional community of practitioners.
Between 1988 and 2004, he mentored nineteen postgraduate students — Dr. Prakash Nagpure of the 1980 batch as his first, Dr. Bhushan Patil of the 1993 batch as his last. He was available beyond working hours. He ensured theses were submitted on time. Before university examinations, he held revision sessions on operative surgery that drew the highest attendance of any teaching session in the department — which is, in its way, the most complete measure of a teacher's standing among the taught.
Dr. Nagpure recalled a specific moment: a disagreement with a senior over ward duties had escalated into conflict. Professor Raizada stepped in, resolved it with quiet wisdom, and in the resolution taught something about communication and conflict management that the technical curriculum did not contain. Dr. Varghese recalled the eleven p.m. surgery. Both memories carried the same essential quality — a man who was present when presence was needed, who managed difficulty without adding to it.
A patient arrived with a penetrating neck injury late at night. Professor Raizada was living in Wardha. He received the call, drove to Sevagram, changed, and was ready in the operating theatre before the patient arrived. The surgery began at eleven in the evening and lasted until four in the morning. He never raised his voice at the residents through any of it. A near-bloodless field, unshakable calm, and at the end, a patient who had survived an injury that could easily have gone the other way. That is the portrait his students gave him. It is the one he deserves.
Mrs. Rekha Raizada's nursing home was in Wardha; his operating theatre was in Sevagram. The home the Raizadas kept was, by their students' memory, a warm one. Mrs. Raizada greeted visiting residents with high tea and snacks, dissolved their stress with humour, teased her husband in good spirit, made them laugh. The laughter occasionally inspired a gentle anxiety — the students confessed, with the affection of those who survived it, that they sometimes worried the good mood might translate into extra assignments the next morning. It rarely did.
His daughter Mridul earned her MD in Paediatrics from MGIMS. His son Mukul, of the 2010 batch, completed his MD from GMC Aurangabad before joining his mother's nursing home in Wardha. The institutional connection extended into the next generation in the pattern that Sevagram repeatedly produced.
The promotion to Additional Professor came in April 1997, and to Professor in March 2004 — six months before his death. The timeline carries a quiet institutional comment: a man who won consecutive best paper awards in his first year, who mentored nineteen postgraduate students, who organised regional conferences and drove to Sevagram at eleven p.m. for emergency surgery, reached the rank of Professor six months before a massive heart attack took him on October 5, 2004. He was fifty-two years old.
The rank was the system's measure. The students' memories were the actual measure. Many of his students went on to become professors and department heads. They carry what he gave them. He died on October 5, 2004. Barely six months a Professor. Twenty-four years a teacher.
| 1952 | Born, 16 September, Bhopal — father Kailash Bihari Raizada, Supreme Court advocate |
| 1970 | Completed BSc, Bhopal University |
| 1975 | Completed MBBS, Gandhi Medical College Bhopal |
| 1979 | Completed MS ENT, Gandhi Medical College Bhopal |
| 1980 | Joined MGIMS, 10 September — Lecturer in ENT |
| 1980 | Best Paper Award, Vidarbha AOI Conference — repeated 1981 |
| 1988 | First postgraduate student — Dr. Prakash Nagpure, 1980 batch |
| 1997 | Promoted Additional Professor, April |
| 2004 | Promoted Professor, 16 March — six months before his death |
| 2004 | Died, 5 October, Sevagram — massive heart attack; aged fifty-two; tenure and life ending on the same day |
Planimetric study of mastoid pneumatization and clinical profile CSOM in children
Clinico pathological profile of atrophic rhinitis and the role of intranasal placentrex therapy
Neonatal nasal septal deformities
A Clinical Profile of CSOM with special reference to TM perforation and measurement of eustachian tube opening pressure
Clinical pathological study of chronic maxillary sinusitis with special reference to annual washout by canine fossa inferior meatus routes
Clinical profile of epistaxis.
Role of Ginkgo biloba extract in acquired sensorineural hearing loss
Otological problems and prevalence of hearing loss in school going children in around Sevagram with emphasis of primary secondary ear care
Prevalence of nasal, oral pharyngeal condition with special reference to cervical lymphadenopathy in school going children in around Sevagram
Clinical profile of hoarseness of voice
Clinical profile of oral submucous fibrosis with special reference to the role of beta carotene (antoxid) in its treatment
Clinicopathological evaluation of neck mass
A study of human nasal cycle
Effects of radiation therapy and chemotherapy on ontological structure in head neck and esophageal malignancies
Clinical profile of vertigo and role of Apley’s canalith repositioning maneuver in benign paroxysmal positional vertigo
Study of symptomatic deviated nasal septum
Congenital anomalies in ENT and neonatal screening for hearing loss in a rural based hospital
Morbidity pattern ,treatment outcome quality of life expenditure analysis of head neck esophageal malignancy in a rural based hospital
Dr. S.K.T. Jain
MS Otolaryngology, Gandhi Medical College Bhopal (1983)
Reader in Otolaryngology · Ten Years at Sevagram · The Man Who Arrived Single and Left as Four
Suresh Kumar Tarachandji Jain was born on February 22, 1956, in Sagar, Madhya Pradesh, the fourth of seven siblings in the household of Shri Tarachandji Jain, an accountant in a private firm. He attended Hindi-medium schools and found in the classroom a deep attraction to mathematics. In his eleventh year, he chose pure mathematics without hesitation.
An elder brother intervened. The job prospects for engineers were poor; biology offered a better path. SKT protested — he found more beauty in numbers than in dissecting plants and animals — but elder brothers, in this family as in many, prevailed. Within a year, he had mastered botany and zoology with the diligence of someone who had decided that if the subject was now his, he would command it. The MP Pre-Medical Test of 1974 yielded an aggregate of 64% that was enough for Gandhi Medical College, Bhopal.
At Gandhi Medical College, there were two Suresh Kumar Jains. Fees were mixed up. Documents were interchanged. The Dean decided to append their fathers' initials. Suresh Kumar Tarachandji Jain became SKT Jain. When Maharashtra's bureaucracy later attempted to simplify him to plain "Suresh Jain," he declined firmly. The identity had been acquired through administrative chaos in a dean's office in Bhopal, but it was his, and it was not up for revision.
ENT was not his ambition. He was drawn toward ophthalmology or orthopaedics. Both filled up quickly. ENT was what remained. He accepted it with reluctance that transformed, with time and good training, into growing enthusiasm. He completed his MS in General Surgery under Dr. Jagdish Gulati, whose thesis assignment — evaluation of sensorineural deafness — pulled him further into the specialty he had not initially chosen. Word of a lecturer's vacancy at MGIMS reached him in 1984. He appeared for the interview and got the post.
He entered a department of two faculty members: Dr. V.N. Chaturvedi, the disciplinarian from AIIMS who believed in meticulous documentation, methodical patient examination, and unwavering surgical precision; and Dr. R.M. Raizada, thorough and deliberate, whose unhurried manner in the operating theatre produced the near-bloodless field and unshakable calm that his students remembered across decades. Two very different temperaments, both insisting on the same underlying standard of care. SKT absorbed what each had to give.
The department in those years was genuinely busy — thirty beds, nearly nine thousand outpatients annually, five hundred and seventy admissions, three hundred and eighty operations. Community health work alongside the medicine department: village visits, school health surveys, screening camps that took specialist care to people who could not access it otherwise. The programme had just achieved independent examination status at Nagpur University for the first time in December 1983.
He witnessed tragedy in this period. Dr. Shyam Sunder Rathi, a postgraduate student who had already published international research on electrogustometry in Hansen's disease, died unexpectedly of a lung disease. The loss left the department shaken in the way that the death of a young colleague always does — the particular weight of potential unrealised adding to the ordinary grief of loss.
He was promoted to Reader in ENT. The next step — Associate Professor, then Professor — required vacancies that did not open. Dr. Chaturvedi and Dr. Raizada were firmly in place, their tenures extending well beyond what the department's promotional structure could accommodate for a third faculty member. The institution that had offered ethics, community, purpose, and genuine clinical experience could not always offer the promotional pathway that sustained a career across its full span.
He mentored two postgraduate students during his decade: Dr. Amreliwala, who worked on myiasis, and Dr. G.P.S. Gill, who asked why taste changes in anaemia — both questions rooted in the clinical reality of a rural hospital's patient population. He co-edited annual reports and served as Secretary of the Academy of Medical Sciences.
In 1986, he married Sunita from Jhansi. Shruti was born in Sevagram. Shubhi was born in Sevagram. "When I came to Sevagram, I was single. When I left, we were four." The campus had become the context of his family's earliest formation.
Ten days before completing a full decade, on the morning of his thirty-eighth birthday, he left for Nanded, where a newly established government medical college needed an ENT department. He built it, then was transferred to GMC Nagpur for six years, then to Akola — another fledgling institution needing a strong ENT foundation. He took the responsibility. In 2012, he joined Indira Gandhi Medical College, Nagpur, as Professor. In 2015, he was transferred to Aurangabad, where he remained until retirement in 2020.
Eighteen postgraduate students guided over his career. Forty research papers published. Additional charge of Dean at Akola — the administrative trust placed in a man who had spent decades building departments in places that needed them rather than polishing his position in places that were already established. He built his home in Nagpur and settled. He had done the work. Enough was enough.
Shruti is in Pune with TCS. Shubhi is in Germany with her husband. The daughters born in Sevagram have carried the formation of that campus into lives on different continents. In the quiet lanes of Nagpur, SKT Jain lives with the satisfaction of a life well lived — not with nostalgia but with a clear accounting of what the decades had contained: the dean's office where administrative chaos gave him his name; the elder brother who redirected him from mathematics to biology; the ENT specialty he had not originally chosen but had thoroughly mastered; the ten years in Sevagram where he had arrived single and left as four.
| 1956 | Born, 22 February, Sagar, Madhya Pradesh — fourth of seven siblings |
| 1974 | MP Pre-Medical Test — admitted Gandhi Medical College, Bhopal |
| 1974 | Name changed to SKT Jain — Dean appended father’s initials to distinguish two Suresh Kumar Jains |
| 1983 | Completed MS ENT, Gandhi Medical College Bhopal — thesis on sensorineural deafness under Dr. Jagdish Gulati |
| 1984 | Joined MGIMS, 6 March — Lecturer in ENT |
| 1986 | Married Sunita from Jhansi |
| 1986 | Promoted Reader in ENT |
| 1988 | Daughter Shruti born in Sevagram |
| 1991 | Daughter Shubhi born in Sevagram |
| 1994 | Left MGIMS, 22 February — his thirty-eighth birthday; joined government medical college, Nanded |
| 1994 | Built ENT department, Nanded · transferred GMC Nagpur six years later |
| 2000 | GMC Nagpur · then Akola — additional charge of Dean |
| 2012 | Professor, Indira Gandhi Medical College, Nagpur |
| 2015 | Transferred Aurangabad — until retirement 2020 |
Myiasis in ear, nose and throat with special reference to atrophic rhinitis
Taste sensation in cases of anemia
Dr. Prabhat Kumar Acharya
DVD & DDV: Bombay University (1965) & CPS Bombay (1966)
In 1966, inside a hospital ward in Cuttack, a young Dr. Prabhat Acharya stood and watched a ward boy take a single skin biopsy, cut it into four pieces, fill out four separate forms under four entirely fabricated patient names, and file them as the foundational data for an MD thesis.
His stomach turned. Just two months into his MD program, rather than complete a degree in an institution where this kind of academic rot was permitted, he walked away.
He had no stipend. He had been eating only once a day. He had been earning a meager Rs. 16 per consultation in his supervisor's private clinic, quietly channeling patients from the OPD and wards exactly as directed. None of this was sufficient reason to compromise his integrity and stay. He simply left.
Forty years later, at eighty-seven, he speaks of those years with a faint, knowing smile: "Medicine and humanity were skin deep." He means it partially as a compliment to the era—to the directness, the raw clinical instinct, and the physical contact between doctor and patient that expensive technology would later interrupt. But the phrase also describes something else entirely: the terrifying thinness of the membrane between integrity and its opposite, and the absolute necessity of knowing exactly which side of it you stand on.
Born on November 26, 1937, in Murta—a small village in what is now Chhattisgarh—he was a farmer’s son. There was no career guidance, no coaching, and no grand plan for the future. Instead, his path was anchored by a quiet, private tragedy: when Prabhat was eighteen and just beginning his medical studies, his younger brother died from the side effects of Chloromycetin. It was a brutal introduction to the double-edged sword of medicine. He became a doctor, he admits with his characteristic candor, simply because he secured good marks in biology; yet the memory of that loss ensured he never viewed a prescription as a mere piece of paper.
The elders of the family added a practical consideration that appealed deeply to his father: a doctor never retires. Unlike a government post or a corporate job, medicine offered the freedom to work for as long as one was physically able. Money was not the primary attraction. What mattered was the idea of a life defined by continuous purpose rather than a fixed period of service
He completed his early schooling in Mungeli and Raipur. In 1957, he entered Netaji Subhash Chandra Bose Medical College. He describes his academic habits with the same blunt honesty he brings to every period of his life: "We never took studies seriously. We played cards, bridge. I studied only in the last month before exams." He passed his MBBS in 1962. (Fifty of his seventy batchmates failed anatomy on their first attempt—the result of a visiting external examiner from Nagpur who believed failure built character. He was never invited back).
He moved to Mumbai in 1964 to specialize in dermatology, training at Topiwala National Medical College and earning his DVD and DDV from the College of Physicians and Surgeons. Then came Cuttack, the fabricated biopsies, and his immediate departure.
In January 1967, he joined Wanless Hospital in Miraj as a junior lecturer in dermatology. The hospital had taken the highly unusual step of partnering with the new Government Medical College, serving as its sole teaching facility. This unique arrangement drew incredibly complex, unusual cases—the exact kind that private nursing homes flatly declined. The dermatology ward saw conditions that routine practice rarely encountered, and Acharya saw them daily.
It was here he also met Usha Kulkarni, a junior lecturer in obstetrics and gynecology. She was the undisputed favorite of the campus—sought after, admired, referred to by her peers as a "fresh rosebud." Gossip circulated endlessly. Yet, nobody had ever seen the two of them together, which made perfect sense: theirs was a traditional, arranged marriage. They met only once or twice before the wedding. When the announcement was finally made, the college buzzed with genuine shock. They married on December 17, 1967. After the wedding, she took the name Archana.
By 1968, he was teaching in Raipur. But the city had not been kind to Archana—there was no teaching post available for her, her private practice was struggling, and money was painfully tight. When Dr. Karunakar Trivedi, the Medical Superintendent at MGIMS, reached out to offer positions to both Acharyas, Sevagram offered exactly what they needed: a completely fresh start.
He officially joined Mahatma Gandhi Institute of Medical Sciences (MGIMS) on October 23, 1972, as a Lecturer in Skin and Venereal Diseases. Deputed to MGIMS by a letter from Mr. Prakash Chandra Sethi, the Chief Minister of Madhya Pradesh in July 1972—while serving as a lecturer in the same specialty at Gajra Raja Medical College, Gwalior—he was promoted to Reader just nine months later. At the time, the dermatology outpatient department was little more than a narrow, airless room tucked inside the Medicine department, where patients arrived bearing scabies, syphilitic sores, fungal infections, and leprosy—the brutal, highly visible diseases of poverty and proximity, carried by people who had nowhere else to go.
There were no immunological tests, no sophisticated biologics, and no lasers. Treatment consisted of a tube of Whitfield's ointment, a prescription for dapsone, and a reassuring word. He referred severe cases, like Stevens-Johnson syndrome, to the physicians. The specialty was, as he puts it, simple and profoundly unglamorous.
In the evenings, he played bridge with Dr. Chella Hariharan. The campus was populated by colleagues his own age who had navigated their own circuitous routes to Sevagram. They all earned modest salaries and lived simply, renting their furniture by the month—a steel cot for Rs. 2, a chair for Re. 1. By the end of the month, the passbook usually showed almost nothing. "Quietly," he recalls, "everyone was looking for better opportunities. But they were rare."
In June 1975, the Emergency was declared across India. Meanwhile, Iran—flush with exploding oil wealth—was building hospitals far faster than it could staff them. They began aggressively hiring Indian doctors at salaries that bore absolutely no resemblance to what Sevagram paid. Dr. S.C. Ahuja, an orthopedician from the MGIMS campus, went first. The Acharyas soon followed.
The Indian government arranged a special chartered flight carrying four hundred doctors directly to Tehran. Archana joined the 9th Aban Hospital in Abadan in August 1975. Four months later, Prabhat resigned from MGIMS and joined her in an insurance hospital.
"We earned in a month what we used to make in a year in Sevagram," he says. "Add a bonus and free tickets to India, and we couldn't have asked for more."
The lucrative chapter was cut short after a year by a severe peptic ulcer. He returned home. But upon coming back, Sevagram suddenly felt different—too slow, too small after the scale of Tehran. Instead of returning to campus, he set up a private practice in Nagpur at Rani Jhansi Square, commuting daily by train and riding his scooter fifty miles twice a week to Yavatmal for consultations. Archana eventually returned to MGIMS in October 1977, rising to the rank of Associate Professor.
In February 1981, he sought reinstatement at MGIMS as a Reader. He returned with two specific requests: UGC pay scales, and the formal separation of Dermatology into its own distinct department.
The administration granted the department separation. However, the pay scales came with a massive, unworkable catch: he would need to obtain an MD within three years. The administration offered to explore having him register in Mumbai or Pune while he somehow continued his teaching duties at Sevagram.
The condition was functionally impossible. An MD required a full, two-year residency physically present at the place of registration, which was entirely incompatible with holding a full-time teaching post at MGIMS. Furthermore, other medical colleges vastly preferred their own internal candidates. The path was closed before it even opened. He worked under this strained arrangement for three years before leaving in February 1984—this time, permanently.
The final catalyst for his departure was the school's language policy. Dr. Sushila Nayar had mandated Hindi as the strict, sole medium of instruction at Kasturba Vidya Mandir. The Acharyas' sons, Ravi and Atul, had been happy there. But in a rapidly globalizing world, the question of English instruction was not an abstract debate for a father looking at his children's futures. In 1983, they enrolled their boys at Rajkumar College in Raipur, one of the oldest boarding schools in central India. Two weeks after Diwali, the Acharyas packed up and left Sevagram.
In Raipur, they built the Gurukripa Surgical and Maternity Centre—a ten-bed facility kept deliberately small to avoid the crushing bureaucratic overhead that plagued larger institutions. He handled the dermatology consultations, while Archana ran the obstetrics and gynecology practice. They ran it beautifully together for decades, until Archana's knee replacement in 2014 made the grueling hours untenable. They simply closed the clinic and retired, letting go of the building and the practice they had sustained with apparent, graceful ease.
In his private practice, he occasionally changed patient names on biopsy forms—always with their explicit consent—when testing for suspected leprosy. He did this to fiercely protect them from the devastating social consequences of a positive result. He had seen firsthand what the brutal stigma could do: a woman diagnosed with indeterminate leprosy early in his career could not bear the social isolation that followed, and died by her own hand. The biopsy form was a small, quiet place where he could act on that tragic knowledge, and he did.
Today, he is eighty-seven. His sons Ravi and Atul are highly successful and settled in the UK and the US. He and Archana live peacefully in Raipur. He begins every single morning with yoga, pranayam, and meditation. He still drives his scooter. He still drives his car. He writes poetry on his iPad.
On March 30, 2025, he emailed a poem to a friend. It began: Time flew away on wings, I do not know if I kept pace; eighty-seven years have passed like yesterday's dream. It ended: In Sevagram, I found boundless affection—that is the treasure of my life; at every turn in the road, its memory comes to me. The final line: Om Tat Sat.
He has never expressed a single regret about his circuitous path—not the abrupt departure from Cuttack, not the lucrative Iranian detour, and not the MGIMS years he ultimately gave up by choosing to leave. He applied his own ethical and practical standards consistently, and he accepted the consequences of every choice. Medicine and humanity were skin deep. He meant it as a precise description, never as a complaint. For Dr. Prabhat Acharya, the depth—wherever he managed to find it—was always enough.
| 1937 | Born, 26 November, Murta, Durg district, CP and Berar (now Chhattisgarh) |
| 1957 | Entered Netaji Subhash Chandra Bose Medical College, Raipur |
| 1962 | Completed MBBS |
| 1964 | Trained in Dermatology — Topiwala National Medical College, Mumbai; earned DVD and DDV |
| 1966 | Left MD programme, Cuttack — witnessed fraudulent biopsy thesis; walked away two months in |
| 1967 | Joined Wanless Hospital, Miraj — junior lecturer, Dermatology |
| 1967 | Married Usha Kulkarni (Archana), 17 December — junior lecturer, OBG |
| 1968 | Joined JNMMC, Raipur |
| 1972 | Joined MGIMS, 23 October — Lecturer, Skin and Venereal Diseases; promoted Reader nine months later |
| 1975 | Left MGIMS — chartered flight to Tehran with 400 Indian doctors |
| 1975 | Joined insurance hospital, Abadan, Iran — earned in a month what Sevagram paid in a year |
| 1976 | Returned India — peptic ulcer; set up private practice, Nagpur |
| 1981 | Rejoined MGIMS, February — Dermatology separated from Medicine department |
| 1984 | Left MGIMS, February — MD residency condition unworkable; boys enrolled at Rajkumar College, Raipur |
| 1984 | Established Gurukripa Surgical and Maternity Centre, Raipur — ten beds, deliberately small |
| 2014 | Retired — closed Gurukripa after Archana’s knee replacement made the hours untenable |
Dr. Pushpa Chaturvedi
MD Paediatrics, AIIMS, New Delhi (1970)

In 1977, a colleague's premature baby arrived into the world weighing just 750 grams. Born at seven and a half months, the infant was desperately ill with hyperbilirubinemia and acute respiratory distress syndrome. Her chances of survival were grimly assessed as slim.
Dr. Pushpa Chaturvedi had just established a modest, bare-bones neonatal unit at MGIMS. She simply refused to give up on the infant. She had been scheduled to travel to the World Paediatric Conference in New Delhi, but she abruptly canceled her trip—entirely unwilling to leave a critically ill child merely to attend a conference about children. She stayed in Sevagram, sleeping near the ward with her team, until the crisis finally passed.
Decades later, her phone rang. The voice on the line belonged to Samriddhi Dhawan—forty-six years old, thriving, calling all the way from the United States just to tell Dr. Chaturvedi that she was well. That she existed. That the refusal to give up in 1977 had produced a full, beautiful life.
It is exactly the kind of phone call that makes the canceled conferences, the sleepless nights, and the decades spent in a rural village far from prestigious city hospitals feel like the only correct set of choices a person could have made.
"I always enjoyed being around children," she once said. "They are fun, sincere, and full of life. But when they fall ill, they seem like wounded angels."
Pushpa Abhichandani was born on December 4, 1942, in Nowshera, Sindh (now in Pakistan), into a family rooted in the law. Partition shattered that stability when she was still young. The family's harrowing escape from Sindh was made by ship from Karachi to Mumbai, because the trains running across the bleeding border had become too dangerous.
Her father, an agricultural soil chemist stationed in London by the Sindh Government at the time, spent six agonizing months negotiating his return to India. In his absence, the newly displaced family endured the profound hardship of refugees without a patriarch—dependent entirely on strangers, carrying only what they could physically salvage, forced to begin again from nothing.
When her father finally joined the Indian Council of Agricultural Research, he was transferred repeatedly across the country. A significant posting in Cuttack, Odisha, gave Pushpa her schooling at the esteemed Stewart School, where she emerged as a brilliant student. Her formative years in Odisha gave her something far more durable than a curriculum: a genuine, lifelong love of rural life, and a deep respect for the simplicity of people who lived close to the land. This would prove absolutely essential. When she eventually found herself standing in a mud-plastered hut in Sevagram years later, she did not recoil.
After completing her MBBS at SCB Medical College in 1965, she went to Delhi for house jobs at AIIMS. She enjoyed delivering babies in Obstetrics, but could not imagine a career organized entirely around pelvic examinations. The pediatric wards, by contrast, absorbed her completely. Six months there permanently settled the question.
During this period, she met Dr. Vishwanath Chaturvedi—the lone male among seven house officers. He was tall, charismatic, with a commanding voice and refined demeanor. They married in June 1971 in an intercaste union that his deeply traditional family initially found difficult to accept. She won them over, as she won over most things that resisted her, through immense patience and quiet determination.
She completed her MD in Paediatrics under Dr. O.P. Ghai, the legendary pioneer who built AIIMS's foundational pediatrics department. Her thesis on child growth was so precise that Dr. Ghai included its images in his seminal textbook, Essential Paediatrics. In May 1970, she received her MD alongside a gold medal for the best postgraduate, presented by the Union Health Minister.
In 1972, Dr. Sushila Nayar was hunting for faculty for her new medical college in Sevagram. When the offer came, Pushpa chose to leave her prestigious position in Delhi to accompany her husband.
At MGIMS, Dr. Nayar offered Dr. V.N. Chaturvedi a Lecturer's position, but offered Pushpa only a Registrar's role. Pushpa had already been a Registrar at AIIMS. She declined the offer—firmly, and without apology. Impressed by her absolute clarity, Dr. Nayar immediately upgraded the offer, appointing her as a Lecturer in Paediatrics.
On February 17, 1972, the Chaturvedis boarded a train to Wardha.
A car took them from the station to their assigned campus housing. What they found was a literal mud-plastered hut with a thatched roof. In May 1972, Pushpa gave birth to their first son, Amit. When she returned to Sevagram with the infant, they moved into a small, basic quarter near the nurses' hostel.
The Paediatrics department she had been hired to join did not actually exist yet. There was no OPD and no dedicated ward—only a borrowed corner of the Medicine OPD, a single makeshift table, a chair, and whatever sick children happened to wander up from the village bus stand.
"When I joined as a lecturer, my salary was ₹650," she recalled. "VN was in tears when he saw the place and my payslip."
She did not share his tears. Her years in Odisha had taught her how to love a village, and Sevagram, with its stark simplicity and massive purpose, instantly became home.
She briefly left Sevagram in January 1974 for a Reader position at Indira Gandhi Government Medical College in Nagpur—a professional grade that the nascent MGIMS could not yet offer her. But after just one year, she returned. Sevagram was home, and she knew it.
She came back as a Reader in 1975, and by 1984, she was a full Professor. Over the next three decades, she built Paediatrics at MGIMS from a single makeshift table into a nationally respected department. She established the neonatal unit, launched the MD program in 1980, mentored forty-six residents, and published 176 papers on childhood diarrhea, neonatal mortality, and infant nutrition.
In 1991, a workshop on human lactation in Wardha produced a landmark recommendation: the establishment of a national advocacy group for breastfeeding. Dr. Chaturvedi, alongside Dr. S. Chhabra, became a founding member of the Breastfeeding Promotion Network of India (BPNI)—an organization that fundamentally shaped national infant feeding policy for decades. From a small workshop in Wardha, massive, consequential things emerged.
She was a pediatrician who firmly believed the educational function of her role was utterly inseparable from the clinical one. Teaching anxious rural families that a fever was merely a symptom rather than a disease, that not every cough required heavy medication, and that most diarrhea resolved without intervention—this was, to her, just as vital as writing a prescription.
The true joy of pediatrics, she insisted, lay in the enduring relationships forged with children and their families.
On January 14, 2002, Dr. V.N. Chaturvedi died of lung cancer. The devastating diagnosis arrived just as the family was joyously preparing for their younger son's wedding. He had been a constant, anchoring presence across thirty years of Sevagram life: the ENT surgeon who had ridden the same train, the man who had wept at her first payslip, the person with whom she had built absolutely everything. His death left an irreplaceable void.
She retired from MGIMS in 2008, continuing as an Emeritus Professor until 2011 before taking an adjunct faculty role at Gulf Medical University in the UAE. In retirement, her brilliant mind simply found new languages: poetry, blogging, and painting. During the COVID-19 pandemic, she turned to canvas and brush, producing vibrant paintings that captured the exhaustion and devotion of health workers, finding in visual art a register of deep feeling that a medical chart could never contain.
Her sons, Amit and Rajiv—both MGIMS alumni married to MGIMS alumni—now practice in Ajman and Abu Dhabi. The institution that had begun for her in a mud hut in a Gandhian village had produced, across three generations of the Chaturvedi family, doctors serving patients across three different countries.
"I love and long for Sevagram," she reflected, "because I cherish rural life. People here were simple and unpretentious. The family-like atmosphere made me feel at home, and I never once regretted leaving AIIMS."
She had made that decision in 1972 in a mud-plastered hut, on a salary that made her husband weep. And she had never regretted it once.
| 1942 | Born, 4 December, Nowshera, Sindh |
| 1947 | Partition — family fled by ship from Karachi to Mumbai; father abroad in London |
| 1961 | Entered SCB Medical College, Cuttack — MBBS class of 1961 |
| 1965 | Graduated MBBS, Utkal University |
| 1970 | Completed MD Paediatrics, AIIMS — under Dr. O.P. Ghai · Sorel Catherine Freymann Award · gold medal, best postgraduate |
| 1971 | Married Dr. Vishwanath Chaturvedi, 2 June — intercaste; met at AIIMS house jobs |
| 1972 | Arrived MGIMS, 17 February — declined registrar post; appointed Lecturer |
| 1972 | First home: mud-plastered hut with thatched roof; salary ₹650 |
| 1974 | Brief posting at Indira Gandhi Government Medical College, Nagpur — Reader |
| 1975 | Returned to MGIMS as Reader |
| 1980 | Launched MD Paediatrics programme, August |
| 1981 | Posting to Libya — Associate Professor and Head, Infectious Disease Unit, Al Fateh Children’s Hospital, Benghazi |
| 1983 | Returned to MGIMS |
| 1984 | Promoted Professor |
| 1991 | Co-founded Breastfeeding Promotion Network of India — from Wardha workshop |
| 2002 | Dr. V.N. Chaturvedi died, 14 January — lung cancer |
| 2008 | Retired from MGIMS, 10 July — continued as Emeritus Professor until 2011 |
| 2011 | Joined Gulf Medical University, Ajman — adjunct faculty until 2015 |
Impact of maternal nutrition on the nutritional status of the newborn
Clinical and immunological study of leprosy in children
Neonatal hypothyroid screening in Wardha -a pilot study
Immunoglobulin-g and complement-3 levels in full term intrauterine growth retarded babies of various etiology
An epidemiological study of congenital malformations in newborn
Factors affecting the incidence and mortality of birth asphyxia
Epidemiology of low birth weight babies
Cord and maternal serum IgM as a screening test for perinatal infection in idiopathic IUGR babies
Study of single dose of combination of mebendazole and 1-tetramisole in helminthic infestation in children and study of a new drug delivery system in children
Transcutaneous bilirubinometry as a screening method for neonatal jaundice
Immunodiagnosis of filariasis in children by stick ELISA
Fine needle aspiration cytology as a diagnostic tool in pediatric lymphadenopathy
Occult filariasis in children immuno diagnosis by stick ELISA
A study of clinical profile in multidrug resistant enteric fever
Detection of filarial antibodies by ELISA in cord serum and breast milk of filarial antibody positive mothers
Acute respiratory infections in children -a hospital based study
Potential of Mycobacterium tuberculosis excretory – secretory antigen in Immunodiagnosis of childhood tuberculosis
Breast feeding practices in a rural hospital
ELISA using KS- antigen of Mycobacterium tuberculosis in Immunodiagnosis of childhood tuberculosis
Weight gain pattern in exclusively breast fed infants
Acute lower respiratory tract infections in children
Serum and cerebrospinal fluid adenosine delaminate activity in the diagnosis of tuberculosis in children
Anthropometric measurements in newborn with special reference to foot length
Normal blood pressure and prevalence of hypertension in school going children
Indirect ELISA using ESAS-DE, antigen of Mycobacterium tuberculosis in Immunodiagnosis of childhood tuberculosis
Prevalence and clinical prediction of hypoxemia in acute pneumonia in children
Clinical profile of sickle cell disease with special reference to hepatic involvement
Delivery room management of neonates born through meconium stained amniotic fluid and the development of meconium aspiration syndrome
Impact of baby friendly hospital initiative: in a rural hospital
Polycythemia in the newborn
Modified Glasgow coma scale scores in febrile unconscious children
Validating the efficacy of clinical parameters in diagnosing streptococcal pharyngitis
Neonatal and perinatal outcome in a rural hospital with special reference to Cesarean Section
Coronary risk factors in children of parents with coronary artery disease/hypertension/diabetes
UTI in febrile children
Cardiac status in sickle cell anemia and sickle cell trait
Physical and sexual growth of adolescent girls, their knowledge and attitude regarding reproductive health
A comparative study of clinical efficacy of home made spacers and nebulizers in bronchodilator therapy in children with acute asthma
CT scan in seizure disorder in children
Assessment of Yale observation scale to predict bacteraemia in febrile children aged 3-36 months
Microalbuminuria as a predictor of sickle cell nephropathy.
Assessment of clinical criteria and pulse-oximetry in identification of hypoxemia in acute lower respiratory tract infections in children under- five years of age
Kangaroo mother care and massage in low birth weight neonates
Nestroft as a screening test for thalassemia carriers in Sindhi community of Wardha
Incidence and management of birth asphyxia and impact of neonatal resuscitation training programme
Dr. Shashi Prabha Ahuja

Reader, Department of Paediatrics · Eight Years at Sevagram · The Best Years of Her Life
She did not choose her sons' names. Manimala Chaudhary — Chhoti Behenji, as she was known across Sevagram — decided them. The boys would be called Nitin and Tushar. There was no debate. In an era when life in Sevagram was built on trust and community, this was not an imposition but a gesture of belonging — an expression of the close-knit bonds that made the campus feel less like an institution than a large, occasionally complicated family.
Dr. Shashi Prabha Ahuja told this story with warmth rather than bemusement, because she understood what it meant. You did not give the naming of your children to someone else unless you trusted them completely, unless the community had absorbed you fully enough that its matriarchs felt entitled to weigh in on the shape of your family. Sevagram had done that to her and her husband within the first years. "We were comfortable in Sevagram," she said. "Had we not been, we would never have stayed for eight years. We were vegetarians, we wore khadi, and we found profound serenity there. Those were our best years."
They had come for a year. Eight years passed.
Shashi Prabha Berry was born on December 19, 1942, in Ludhiana, into a household where medicine was the ambient condition. Her father, Dr. Ram Gopal Berry, was an ophthalmic surgeon. The path toward medicine was familiar and naturally taken.
She entered the medical college in Rohtak in 1960 — part of its first MBBS batch, the students who would define what the institution was before it had defined itself. She graduated in 1965. Among her classmates was Dr. Ravinder Narang, who would later become a surgeon at MGIMS. Fate was already arranging the Sevagram connections, though neither of them knew it yet.
She completed her MD in Paediatrics at Maulana Azad Medical College under the mentorship of Dr. P.N. Taneja, then spent three years at Christian Medical College, Ludhiana. A brief three months at CMC Vellore followed, and it was there, in passing, that she encountered a small advertisement in The Hindu: a teaching post at Kasturba Hospital, Sevagram. She applied. The call came. On September 1, 1973, she and her husband arrived in the village that would hold them for the next eight years.
The Paediatrics department in 1973 was modest in the particular way that everything at MGIMS was modest in those years — not inadequate so much as in the process of becoming. There was no dedicated head; Dr. S.P. Nigam from the Medicine department managed it alongside his other responsibilities. A year after Dr. Ahuja's arrival, Dr. G.S. Gurumurthy from CMC Vellore joined as department head and patient numbers began to climb.
The region had no alternative. Kasturba Hospital was the only teaching hospital serving rural Vidarbha, and its paediatric ward received babies from villages across a wide radius — infants and children whose families had travelled considerable distances because there was nowhere else to go. When the Civil Hospital in Wardha eventually ceased admitting infants, Sevagram became the region's sole paediatric referral centre, and the numbers reflected the weight of that responsibility. From 5,000 outpatients and 300 admissions in the early years, the department grew to over 7,000 outpatients and 791 admissions by 1976 — a more than doubling of workload in three years, absorbed by a small team building its structure while simultaneously carrying its clinical burden.
The department organised itself into two units: one led by Dr. Chaturvedi and one by Dr. Ahuja. Together they ran the wards, conducted rural outreach clinics in Deoli and Pulgaon, and led immunisation drives into the surrounding villages — bringing paediatric care to children who would not otherwise have reached it. This was the Gandhian logic of MGIMS made practical: the hospital reaching toward the village rather than waiting for the village to reach the hospital.
Within a year of joining, Dr. Ahuja was promoted to Reader. The promotion recognised what her colleagues and students already understood — that she brought to the paediatric ward a quality that was both clinical and human, a capacity to hold the chaos of sick children and frightened parents with a steadiness that made the ward feel safe.
In 1975, she left Sevagram on a two-year deputation to Iran, part of a team of Indian doctors addressing a healthcare crisis there. She returned to Sevagram in December 1977, was offered accommodation in Flat 3 of the newly constructed Vivekananda Colony quarters, and resumed her position in a department that had continued to grow in her absence.
By 1979, Paediatrics had thirty beds and twelve nursery beds. Weekly general club meetings, case discussions, and clinical reviews had become routine — the structural signs of a department that had found its shape. The clinical volume was large and the team was small, and the work was serious and unrelenting in the way that paediatric work at an understaffed rural referral centre is always serious and unrelenting.
But the career ceiling was equally real. Dr. Chaturvedi led the department, and the hierarchy offered no path beyond Reader for Dr. Ahuja. The professorship that might have come under other circumstances did not come here. When the MD Paediatrics programme began, no postgraduate student was registered under her guidance — a limitation that went beyond the professional to the pedagogical. What was an academic role if it offered no opportunity to mentor?
This tension had a particular texture. Dr. Ahuja and Dr. Chaturvedi were nearly the same age, both married to faculty members at the institute, both serious clinicians, both women navigating a professional hierarchy in which such positions were rare and the available space limited. Their presence under the same roof created what those who knew them described as an unspoken rivalry — not hostile, but real, running beneath the surface of their daily professional relationship, and pushing both of them toward the excellence that competition sometimes produces. They were not enemies. They were two capable women in a space designed for one, and they both knew it.
Dr. Ashok Mehendale, from the MGIMS class of 1976, remembered her with specific precision: "She was petite, loving, and gentle — a perfect paediatrician. The way she handled newborns and young children was remarkable. She brought calm to the chaos of the paediatric ward and taught us with grace and patience."
Dr. Hariom, from the class of 1974, offered the clearest clinical tribute: "She was a soft-spoken yet sharp clinician. I was once amazed by her keen diagnostic skills when she identified a child's painful swelling as scurvy — a diagnosis I had completely overlooked." He added, with the specificity of genuine regret: "Had the Ahujas not left Sevagram, I would have been privileged to be her postgraduate student."
The scurvy diagnosis is worth pausing on. It was not a dramatic case — no emergency intervention, no high-stakes procedure. It was a child with painful swelling, and Dr. Ahuja recognised what it was when the student in front of her had not. This is clinical teaching at its most essential: the supervisor's eye seeing what the trainee's eye cannot yet find, and the gap between them becoming the education.
Three students, three registers of memory: the clinical warmth, the diagnostic sharpness, and the quality of presence. Together they describe a paediatrician who was fully suited to her specialty — gentle enough for the children, precise enough for the diagnoses, present enough for the students to remember her decades later.
On February 6, 1981, Dr. Ahuja left Sevagram to take charge of the Paediatrics department at B.L. Kapoor Hospital in Ludhiana. She spent the next decade shaping paediatric care there before eventually moving into private practice. Research publications were not her hallmark; she did not leave behind a bibliography. What she left behind was the foundation on which others built — the generations of paediatricians who had learned to handle newborns under her guidance, the outreach clinics that had carried vaccines to Deoli and Pulgaon, the ward culture of calm competence in the face of the constant distress that paediatric medicine presents.
She had come for a year. Chhoti Behenji had named her sons. She had worn khadi and found serenity in a Gandhian village far from Ludhiana, and eight years had passed before she was ready to leave.
The best years, she said. The best years of her life.
| 1942 | Born, 19 December, Ludhiana — father Dr. Ram Gopal Berry, ophthalmic surgeon |
| 1960 | Entered Medical College, Rohtak — first MBBS batch |
| 1965 | Completed MBBS — classmates included Dr. Ravinder Narang, future surgeon at MGIMS |
| 1965 | Completed MD Paediatrics, Maulana Azad Medical College — under Dr. P.N. Taneja |
| 1970 | Joined Christian Medical College, Ludhiana — until April 1973 |
| 1973 | Saw advertisement in The Hindu at CMC Vellore — applied for teaching post, Sevagram |
| 1973 | Arrived MGIMS, 1 September — with husband; promoted Reader within the year |
| 1975 | Left on two-year deputation to Iran |
| 1977 | Returned to MGIMS, December — Flat 3, Vivekananda Colony |
| 1979 | Department: 30 beds, 12 nursery beds — over 7,000 outpatients annually |
| 1981 | Left MGIMS, 6 February — took charge of Paediatrics, B.L. Kapoor Hospital, Ludhiana |
Dr. Anand Prakash Dubey
MD Pediatrics: Gandhi Medical College, Bhopal (1979)

When Dr. Anand Prakash Dubey entered the Dean's chamber at Gandhi Medical College, Bhopal, to formally declare his postgraduate specialization, every professor of Medicine in the room had their eyes fixed on him. He had ranked second in his entire MBBS batch. The Medicine department desperately wanted him. He had spent the long walk to that room weighing his options—Medicine, which he genuinely loved, and Paediatrics, which had quietly captured something much deeper inside him.
He chose Paediatrics.
His Medicine mentors were visibly disappointed. The pediatricians quietly celebrated. They had gained, according to the immediate assessment of the room, an absolute gem.
What drew him to children was not complicated to explain. It was the irresistible pull of them—their directness, their inherent trust, and the highly specific quality of caring for patients who could not yet advocate for themselves. He had grown up in Khapariya, a tiny village of barely a hundred families in Madhya Pradesh, where his father, Ram Karan Dubey, was a traditional Ayurvedic practitioner. Long before he possessed the medical vocabulary for it, young Anand understood what it meant to be a small person in desperate need of someone's competent, gentle attention. Paediatrics gave him the chance to be exactly that person for others.
Born on September 22, 1952, he was educated entirely through Hindi-medium schools—first the village school, then the Government School in Seoni Malwa Tehsil. He absorbed the complex rules of science and mathematics in the language he naturally thought in, rather than the language that carried institutional prestige.
When he reached Motilal Vigyan Mahavidyalaya in Bhopal for his BSc Part 1, a critical question arose: Should he take the Pre-Medical Test (PMT) in English or Hindi? His teacher's advice was sharp and direct: Your strength is in the science. Master the concepts first. You have time for English later. He listened.
In the very first sitting of Madhya Pradesh's newly introduced PMT—a massive, single examination for six medical colleges serving a state that then included present-day Chhattisgarh—Anand topped the entire Bhopal center and ranked eighth statewide. In his rural tehsil, this was as rare as a tailender scoring a Test century. His photograph was splashed across the local newspaper; his family was overwhelmed.
He entered the 1970 batch at Gandhi Medical College, Bhopal, sweeping medals in every examination. He completed his MD in Paediatrics in April 1979 under the mentorship of Dr. N.R. Bhandari. His thesis on iron status in children, comparing breastfed infants with those on top feeding, gave him his first rigorous encounter with clinical research. Soon after, he arrived in Delhi as a Senior Resident at Kalawati Saran Children's Hospital.
Delhi was only ever meant to be temporary. He was a brilliant young pediatrician without a permanent post, uncertain of what came next. His MBBS classmate, Dr. R.M. Raizada—who would later become Head of Otolaryngology at MGIMS—was already stationed in Sevagram, urgently pushing him to apply for a permanent Lecturer position rather than remain in flux in the capital.
The pull was geographical as much as professional: his maternal uncle lived in Nagpur, and his mother's family roots were in nearby Chhindwara. A fortnight after Holi in 1980, he finally applied. Confirmation arrived within days. On July 1, 1980, he arrived in Sevagram.
He moved into 5 Guru Nanak Colony with rented furniture, a second-hand Bajaj Super scooter, a Kelvinator refrigerator, and an LPG cylinder. For a young doctor from a village in Madhya Pradesh, Sevagram felt less like a professional compromise than a spiritual homecoming. The stark simplicity of the campus did not unsettle him in the slightest; he felt instantly at home.
The Paediatrics department he joined consisted of exactly four members: Dr. Pushpa Chaturvedi, Dr. Shashi Prabha Ahuja, Dr. V.R. Deshmukh, and himself. Within months, both senior colleagues were gone—Dr. Ahuja left for Ludhiana in February 1981, and Dr. Chaturvedi departed for Libya in March.
Two young lecturers—Dr. Dubey and Dr. Deshmukh—were suddenly left alone to run the entire pediatric service of a massive regional referral center. They were supported only by two MD registrars: M.J. Khan, the first student to enter the MD program, and Arvind Garg.
For nearly a year, they held the hospital together by sheer force of will. Paediatric wards in that era offered fiercely basic care. Neonatology was still a nascent concept across India; pulse oximeters and mechanical ventilators were entirely unknown, and a dedicated pediatric ICU was non-existent.
In Sevagram's frequent, torrential rains and snake-ridden nights, the faculty walked to the wards in pitch darkness. They were always first on call, simply because there was no one else to call. The work was brutally demanding, the staffing terrifyingly thin, and the sick children continuously arriving.
Dr. Dubey's manner through this intense crucible was consistently described by those who worked alongside him: gentle, soft-spoken, and exceptionally mild-mannered. This gentleness was not a weakness—it was the exact quality that made terrified parents trust him and sick children allow him to examine them. For a pediatrician in a rural ward, it was the most essential instrument he possessed.
In March 1982, Dr. Baldev Bhatia arrived from Banaras Hindu University as Reader and Head, finally restoring the department to adequate staffing. Dr. Narayan Bahadur Mathur joined six months later. A year after that, MGIMS students sat for their Paediatrics examination as a standalone subject in their final MBBS for the very first time—a crucial marker of departmental maturity, achieved by men who had spent years building toward it in impossibly difficult conditions.
On January 2, 1985, Dr. Dubey was promoted to Reader. But by December of that year, the department was in transition again, and Dr. Dubey felt the undeniable pull of further academic development that the MGIMS structure could not yet provide. He left with a heart full of nostalgia and profound gratitude.
His memories of Sevagram remained fiercely vivid forty years later: The exhausting Sirpur Kaghaznagar medical camp. The cine club in the anatomy lecture hall. The Madras Hotel, Indian Coffee House, and names of colleagues who became lifelong friends. On August 7, 1985, his elder son Ashwini had been born in his Type 2 Quarters. Sevagram had given him fatherhood as well as medicine.
He joined Maulana Azad Medical College (MAMC) in New Delhi as an Assistant Professor, eventually rising to become Director-Professor of Paediatrics in 2008 and Head of the Department from 2004 to 2014. After retiring from MAMC in 2017, he established the Paediatrics postgraduate program at the ESI Model Hospital in Delhi.
His contributions to national pediatric policy were monumental. He advised the DCGI on critical COVID-19 vaccination decisions, served as Executive Editor of Indian Paediatrics, and provided vital guidance to the National Technical Advisory Group on Immunisation (NTAGI) and the WHO.
The boy from Khapariya—who had topped the Hindi-medium PMT, chosen children over prestige in the Dean's chamber, and held a rural department together through the snake-ridden Sevagram dark—had become one of the most consequential voices in Indian child health policy.
The trajectory was never accidental. It was the sheer accumulation of specific qualities applied consistently over a lifetime. Back in Bhopal, Dr. Bhandari had told his brilliant young student: Your brilliance deserves a larger stage. Dr. Dubey had gone to Delhi, then to Sevagram, then back to Delhi, and finally to the national bodies where health policy for millions of children was shaped. The stage had, indeed, been large enough.
| 1952 | Born, 22 September, Khapariya, Narmadapuram district, Madhya Pradesh |
| 1970 | Topped Bhopal PMT centre — ranked 8th statewide; entered Gandhi Medical College, Bhopal |
| 1975 | Completed MBBS — medals in each examination; ranked second in batch |
| 1979 | Completed MD Paediatrics, April — under Dr. N.R. Bhandari; thesis on iron status in infants |
| 1979 | Senior Resident, Kalawati Saran Children’s Hospital, Lady Hardinge Medical College, Delhi |
| 1980 | Arrived MGIMS, 1 July — 5 Guru Nanak Colony |
| 1981 | Dr. Ahuja and Dr. Chaturvedi departed — held Paediatrics department with Dr. Deshmukh and two MD registrars |
| 1982 | Dr. Baldev Bhatia arrived from BHU as Reader — department restored to adequate staffing |
| 1984 | MGIMS students sat Paediatrics as standalone final MBBS subject for first time |
| 1985 | Promoted Reader, 2 January |
| 1985 | Elder son Ashwini born, 7 August — at 5 Type 2 Quarters, Sevagram |
| 1985 | Left MGIMS, December |
| 1986 | Joined Maulana Azad Medical College, New Delhi — Assistant Professor |
| 2004 | Head of Paediatrics, MAMC — until 2014 |
| 2008 | Director-Professor, MAMC |
| 2017 | Retired from MAMC — joined PGIMSR ESI Model Hospital, Basaidarapur, Delhi |
| 2018 | Established Paediatrics postgraduate programme at PGIMSR — served until 2022 |
Dr. Mukesh Agrawal
MD Paediatrics. (Gandhi Medical College, Bhopal, 1985)

Five candidates from Bhopal had arrived in Sevagram for faculty interviews. None of them owned a single piece of khadi clothing. Under Dr. Sushila Nayar's strict regime, wearing khadi on campus was a non-negotiable requirement, particularly for a job interview. As panic rapidly spread among the applicants, a kind soul in Sevagram quietly produced a single khadi shirt. What followed was a highly coordinated relay race: one candidate put on the shirt, walked into the interview room with an expression of appropriate Gandhian gravity, walked out, and immediately passed the garment to the next man. Five men, one piece of fabric, and the exact same practiced expression of propriety repeated five times in succession. If the shirt had a voice, the candidates later agreed, it would have laughed out loud.
This story has been told and retold by the Bhopal cohort who came to Sevagram in the mid-1980s, always with the particular fondness of people who survived something mildly absurd together. Dr. Mukesh Agrawal was one of those relay runners. He got the position. He stayed for five and a half years.
He helped build a functioning pediatric department from modest foundations, published fifteen research papers, and eventually left for Mumbai. There, he rose to become Professor and Head of Paediatrics at KEM Hospital—one of India's most prestigious teaching institutions—and published a textbook of pediatrics that is now in its third edition.
But the borrowed khadi shirt was the beginning.
Mukesh Agrawal was born on February 2, 1959, in Sehore, Madhya Pradesh. The eldest of three children, his father was a primary school teacher who was frequently transferred across the rural tehsils. The family moved with the postings through Shikarpur, Bhatkhedi, and Ichhawar.
In these small villages, Mukesh studied by lantern light in Hindi-medium schools, absorbing the complex rules of science in the language of his thinking rather than the language of professional advancement. These humble conditions produced a highly specific kind of resilience—not the dramatic overcoming of sudden adversity, but the quiet absorption of ordinary difficulty, day after day, until the difficult simply becomes the normal.
He cleared the Madhya Pradesh Pre-Medical Test (PMT) and entered Gandhi Medical College (GMC), Bhopal, in 1976. When asked why he chose medicine, his answer possessed a characteristic directness: it was simply the natural choice for a boy who had studied biology during a time when doctors seemed almost magical to village children. They were the only ones who could give injections; they were the ones who arrived when things were deadly serious.
He earned his MBBS in 1981 with medals and secured a postgraduate residency in Paediatrics under Dr. N.R. Bhandari—the exact same mentor who had guided Dr. A.P. Dubey five years earlier. In Bhopal's medical culture of the early 1980s, academic research was almost nonexistent. Doctors were entirely absorbed in clinical work and private practice; the idea of writing and publishing papers was practically unknown.
This baseline reality would matter immensely later, when Sevagram changed his relationship to academic medicine entirely.
The 1984 Bhopal gas tragedy had many doctors urgently reconsidering their futures in the city. Meanwhile, the MGIMS Paediatrics department had simultaneous vacancies following the departures of Dr. Dubey and Dr. Mathur. (The running joke among applicants was that the train from Bhopal to Sevagram was always full of job candidates). Dr. Agrawal applied in July 1985 and joined on November 5.
He settled into Kabir Colony with a cohort of unmarried doctors—Raj Shrivastava, S.K.T. Jain from ENT, B.M. Loya from Surgery, and Padmakar Tripathi from Microbiology. They formed an impromptu joint family bound tightly by friendship, extreme frugality, and the communal management of their modest salaries. Meals were shared. Debates were spirited. The question of whether spending an extra rupee for a cup of tea constituted reckless financial extravagance was a recurring philosophical problem.
In May 1986, he married Reena, who arrived from Indore with an MSc in Chemistry, a razor-sharp mind, and an immediate ability to navigate the peculiar demands of Sevagram life.
In 1987, their daughter Paankhi was born. The night of her birth remains one of his most vivid Sevagram memories—not just for the overwhelming joy of fatherhood, but for what Dr. S. Chhabra did. When Reena went into labor, Dr. Chhabra stayed by her side through the entire night, armed only with a thermos of hot tea and an English novel. She flatly refused to leave until the delivery was safely completed the next morning. This was the true quality of the Sevagram community: a senior colleague staying awake the entire night simply because that was what you did for your own.
When Dr. Agrawal joined, the department was led by Dr. Pushpa Chaturvedi. It was a small, fiercely dedicated team managing a 30-bed ward. The Neonatal Intensive Care Unit (NICU) was a compact cubicle adjacent to the maternity complex, caring for premature neonates with incubators and radiant warmers. Mechanical ventilators were a distant dream; the team compensated with raw clinical skill, resourcefulness, and constant vigilance.
Dr. Chaturvedi's absolute insistence on research became the defining feature of his academic environment. She quizzed her junior faculty relentlessly: What manuscript are you working on? Have you submitted your paper? How is the data collection going? In Bhopal, Dr. Agrawal had never written a single paper. In Sevagram, under this sustained, inescapable pressure, he discovered he actually had something to say.
In 1990, he published "The Infant's Cry in Health and Disease" in the National Medical Journal of India (NMJI). Under the editorship of Dr. Samiran Nandi, the journal was offering ₹1,000 per accepted article as a powerful incentive for young researchers. The sum was hardly trivial; it covered a full month's worth of books and meals. More importantly, the publication was a profound intellectual vindication. He quickly followed it with "Hypnotherapy in Children," also in NMJI.
By the time he left Sevagram, he had fifteen publications to his name—a rock-solid research foundation built almost entirely under the influence of a department head who simply refused to accept the absence of scholarly output as a normal condition.
Three things prompted his departure in 1991. First, his daughter Paankhi was growing up, and the English-medium schooling options in Sevagram were severely limited. Second, the gravitational pull of Mumbai—a vastly larger professional stage with complex clinical cases and deep institutional resources—was undeniably real. Finally, the promotion structure at MGIMS had created an invisible ceiling: he had reached Reader, but the rank of Professor seemed inaccessible, as the hierarchy above him was occupied and unlikely to shift.
He took the Maharashtra Public Service Commission examination, entering a massive wave of recruitment as Brihanmumbai's teaching hospitals transitioned to full-time faculty positions. He passed. On May 10, 1991, he left Sevagram. (His successful departure inspired others; Dr. S.K.T. Jain and Naresh Kumar soon followed the exact same route).
What followed was thirty-five staggering years across Mumbai's premier teaching institutions. He rose to become Professor and Head of Paediatrics at Seth G.S. Medical College and KEM Hospital from 2010 to 2022. He mentored more than seventy postgraduate students, contributed to massive vaccine trials for rotavirus and influenza, and chaired Mumbai's Adverse Events Following Immunisation committee during the COVID-19 pandemic. His textbook of pediatrics is a standard national reference.
The village boy who had studied by lantern light in Sehore, who had passed the single khadi shirt in the interview relay race, and who had been ordered by a determined department head to start writing manuscripts, had become one of the country's most significant pediatric educators.
"Those were truly golden days," he said of his time in Sevagram. He was not talking about Mumbai, with its prestigious legacy institutions and large salaries. The golden days were the evening badminton matches, the sugary tea and pakoras, the communal dinners in Kabir Colony, the cramped NICU, and the one borrowed khadi shirt passed desperately from candidate to candidate.
| 1959 | Born, 2 February, Sehore, Madhya Pradesh |
| 1976 | Entered Gandhi Medical College, Bhopal — cleared Madhya Pradesh PMT |
| 1981 | Completed MBBS — with medals |
| 1984 | Completed MD Paediatrics under Dr. N.R. Bhandari, GMC Bhopal |
| 1985 | Arrived MGIMS, 5 November — Kabir Colony |
| 1986 | Married Reena, May — MSc Chemistry, Indore |
| 1987 | Daughter Paankhi born — Dr. S. Chhabra stayed the entire night with thermos of tea and a novel |
| 1990 | Published “The Infant’s Cry in Health and Disease” — National Medical Journal of India |
| 1990 | Published “Hypnotherapy in Children” — NMJI |
| 1991 | Left MGIMS, 10 May — Maharashtra Public Service Commission; S.K.T. Jain and Naresh Kumar followed |
| 2010 | Professor and Head of Paediatrics, Seth G.S. Medical College and KEM Hospital — until 2022 |
| 2022 | Retired from KEM — textbook of paediatrics in its third edition |
Dr. Ramakant Nagesh Shetti
MS Anaesthesiology, Amritsar (1968)

Dr. Ramakant Nagesh Shetti—called Babu by his family and R.N. Shetti by the world—was born on March 24, 1939, in Gulbarga. He was the eldest of ten children born into a household that prioritized education. His father, Dr. Nagesh Subrao Shetti, was a self-made physician of the British era who had walked barefoot out of Ankola as a boy. Mentored by a distant relative and eye surgeon, Dr. Ekanth, the elder Shetti trained in Bijapur and was certified at the Henderson Eye Institute before establishing a practice in Gulbarga.
His mother, Sushilabai, taught mathematics and lived by strict logic. At her husband’s urging, she traveled alone to Hyderabad in the 1940s to complete her degree, leaving her younger children in the care of young Babu and his elder siblings for two years. She eventually retired as the headmistress of the Kanya Government High School. This decision permanently planted in the household the belief that knowledge was the greatest inheritance. It was also a household where Sushilabai could rarely find the cream to make buttermilk; growing up surrounded by the family’s buffaloes, young Babu had a voracious appetite for dairy and usually swooped in to eat the cream first.
Shetti excelled academically, topping the Pre-University Certificate for the Gulbarga district. He completed his XII standard from Bombay University in 1958 and entered Mahatma Gandhi Medical College under Osmania University, graduating with his MBBS in 1963. Anaesthesia—the silent, high-stakes art of keeping life suspended between breath and blade—drew him in completely. He began as a tutor at Osmania General Hospital, followed by stints at Gandhi Hospital and the Cancer Hospital in Hyderabad, before joining the General Hospital in Guntur in 1965. That same year, he earned his Diploma in Anaesthesiology.
He secured a teaching post at H.K.E. Society’s Mahadevappa Rampure Medical College in Gulbarga in 1966. In 1968, he traveled to Amritsar to train under the legendary Dr. Pritam Singh, earning his MS and FICS. His thesis examined chloroform’s effects on the heart rate and blood pressure of dogs. He returned to Gulbarga in 1968, rising to the rank of Associate Professor.
He married Rajani, a devoted homemaker from Ankola. Shetti was her most ardent admirer, encouraging her passion for the arts. She painted for the annual exhibition in Sevagram and learned classical music from Mr. Ambulkar at the Gandhi Ashram. At his insistence, she wrote poetry in Kannada, which was published on the first anniversary of his passing. Together, they raised four children: Namrata, Nagesh, Nivedita, and Nikhilesh. He instilled in them a love for travel; today, they live across different continents, though none pursued medicine.
On February 14, 1975, Dr. Shetti arrived at the Mahatma Gandhi Institute of Medical Sciences (MGIMS) in Sevagram by bus and train. His appointment was Professor of Anaesthesiology at a salary of ₹2,632.20. That year, he was elected a Fellow of the International College of Surgeons. His luggage consisted of two bags: one for clothes, and a massive second bag filled entirely with books and journals.
His arrival at the hospital each morning was heralded by the roar of his Vespa scooter. At the first sputter of its engine, orderlies would scramble to mop already gleaming floors to ensure they appeared busy the moment the professor entered. The department was then in its infancy, comprising Dr. A.C. Tikle, Dr. Naphade, and Dr. K.B. Jain. Working with Boyle’s machines and manual BP monitors, Shetti administered cardiac anaesthesia for open mitral valvotomy and pericardiectomy performed by the surgeon and Medical Superintendent, Dr. K.K. Trivedi.
In the theatre, Shetti commanded absolute authority. Pin-drop silence prevailed the moment he entered. Under his strict supervision, he guided the MD postgraduate studies of S.M. Srivastava (bupivacaine and post-spinal headaches), R.K. Tiwari (infection risks from anesthesia equipment), and S.S. Khot (centbucridine). This standard extended beyond the theatre. One Sunday, discovering a duty resident had slipped away to watch the television serial Mahabharata, Shetti drove to the hospital and summoned the doctor back immediately. The rule he enforced—that no doctor leaves a ward unattended without the next shift arriving—is followed to this day.
His dedication was absolute. When a student named Alex suffered a grievous head injury in a road accident, Dr. Shetti cancelled a fully planned family holiday, with tickets already booked. Leaving his lunch table, he rushed to the hospital for the brain surgery. When colleagues coaxed him to continue his vacation, he replied, "Vacations can wait... cities and palaces will not disappear." He stayed by the student’s side for the forty-eight critical hours that followed.
On November 17, 1977, he became Vice Principal of MGIMS, receiving a monthly allowance of ₹150. Collaborating with Dr. M.L. Sharma, he maintained strict academic discipline. From 1982 to 1985, he edited the Indian Journal of Anaesthesiology. Assisted by his resident Dr. Sanjay Khot and stenographer Kuljeet Singh, he meticulously reviewed manuscripts. Each month, they traveled to Nagpur to source paper, oversee printing, and mail copies.
His administrative brilliance was immortalized in the Sevagram landscape. Partnering with three technicians—Kiran Munjewar, Jaipal Yelwatkar, and Mr. Khodke—he successfully negotiated with the Kasturba Health Society to form a residential cooperative for staff. He disarmed resistant clerks to ensure technicians, nurses, and paramedics received plots of land. He acquired a plot for himself but never built on it; years later, he quietly transferred it to Dr. Sushil Verma of Pharmacology.
Shetti was a polymath, fluent in Kannada, Hindi, Marathi, Telugu, English, and Urdu. He possessed a discerning ear for Hindustani classical music, identifying gharanas and ragas from maestros like Mallikarjun Mansur and Bade Ghulam Ali Khan. He found peace in the voices of Pandit Bhimsen Joshi, Kishori Amonkar, and Jagjit Singh, and adored the ghazals of Mehdi Hassan and Ghulam Ali. He would visit Rhythm House in Bombay just to record his choice of music onto cassettes.
His library spanned Shakespeare and Gandhi to Ayn Rand and Mario Puzo. He followed the news daily across multiple languages and curated the Sevagram cine club, organizing fortnightly screenings in the anatomy lecture hall. He watched The Guns of Navarone eleven times and admired actors like Gregory Peck and Dev Anand.
At home at 13 MLK Colony, he helped his wife in the kitchen and watered the garden. Children were drawn to his ability to make them laugh. He held an intense passion for cricket and shared a vibrant camaraderie playing tennis with Dr. Trivedi. He was an unapologetic foodie, traveling to the Wardha railway station for fresh vadas and favoring the India Coffee House at MGIMS. Frequently reminded by his wife to lose weight, he would set out on long walks from Sevagram to Wardha, or later, a six-kilometer trek from Bambolim to Panjim.
His life mantra was "Work is worship," and his mornings began with devotion to Guru Raghavendra Swami and Shirdi Sai Baba. From the puja room, he would recite "Om sahana vavatu..." and "Poojyaya Raghavendraya..." before eating his first morsel of food. Influenced by Gandhian philosophy, he wore khadi. He also took a deep interest in Vinoba Bhave’s Gitayee. He treated Vinobaji medically and attempted to establish a society with the Aggarwals of Warud to spread the book's teachings.
His loyalty to his staff was legendary. He forged a deep bond with Ram Bhau, a technician who called him "Doctor Sahib." When Shetti underwent complicated kidney stone operations at MGIMS and Osmania Hospital, Ram Bhau traveled with him to attend to his needs. Shetti would reciprocate by visiting the technician's home to enjoy bondas prepared by Mrs. Ram Bhau. Another silent soul, Chandorkar, worked diligently beside him in the theatre.
On December 15, 1983, at the age of 44, Dr. Shetti left the MGIMS operating theatre for the last time. He moved to Goa Medical College (GMC) as Professor and Head of Anaesthesiology. His student, Dr. Sanjay Khot, followed him to Goa to serve as a senior resident. In Goa’s humid climate, khadi shirts crumpled within an hour, yet Shetti wore them every day.
During his 17-year tenure in Goa, he was appointed Honorary Consultant to the Armed Forces for Goa State, chaired the International Conference of Anesthetists in Amsterdam in 1993, and delivered the Venkat Rao Oration in 1995. He helped form GOMECO, a residential society for GMC doctors, and often opened his home to poor families traveling from afar. When he retired in 2000, receiving the Millennium Achiever Award, his photograph was installed outside the GMC operating theatre.
He then became Dean at D.Y. Patil Medical College in Kolhapur, where his efforts to instill discipline led to a physical assault by class IV employees. Despite a grievous neck injury, he remained undeterred, finishing his career at MVJ Medical College in Bengaluru and acting as a project consultant for hospitals in Margao and Bangalore.
In June 2004, he was diagnosed with acute myeloid leukaemia. His haematologist at CMC Vellore, Dr. Mammen Chandy—who helped establish India’s first bone marrow transplantation program at Christian Medical College, Vellore, in 1986—recorded in his case notes that he was “a determined professional… aware of the disease,” who chose to forgo chemotherapy, fully understanding its side effects. Dr. Shetti did not wish to burden his family in the final stage of his illness and decided to face the cancer on his own terms.
Confined to his bed, he spent his final days reading Dan Brown’s The Da Vinci Code and having his children read the Sai Satcharitra to him. He listened to the music of Bhimsen Joshi and Mehdi Hassan. He had once inscribed Robert Frost’s lines in his diary: "The woods are lovely, dark and deep. / But I have promises to keep, / And miles to go before I sleep." He had kept those promises. He died three months after his diagnosis, at sixty-five. He met the end exactly as he had lived—on his own authority and without flinching.
| 1939 | Born, 24 March, Gulbarga — first of ten children |
| 1963 | Completed MBBS, Mahatma Gandhi Medical College, Osmania University |
| 1965 | Completed Diploma in Anaesthesiology |
| 1968 | Trained under Dr. Pritam Singh, Amritsar — MS and FICS; thesis on chloroform’s cardiac effects in dogs |
| 1975 | Arrived MGIMS, 14 February — Professor of Anaesthesiology; salary ₹2,632.20; one bag contained only books and journals |
| 1977 | Appointed Vice Principal, 17 November |
| 1978 | Established housing cooperative society — negotiated with Manimala Chaudhary; plots for technicians, nurses, clerks, paramedics |
| 1982 | Appointed Editor, Indian Journal of Anaesthesiology — until 1985; monthly trips to Nagpur for printing and dispatch |
| 2004 | Diagnosed with acute myeloid leukaemia, June — declined chemotherapy; died three months later, aged sixty-five |
Study of the concentration effect ratio of hyperbaric Bupivacaine in spinal analgesia its relation to postspinal headache
Anesthesia equipment as a source of infection
Evaluation of centbcridine for spinal analgesia: A double blind study
Dr. Arun C. Tikle
MD Anaesthesiology, Government Medical College Nagpur (1977)
Overworked, often visibly exhausted, operating with whatever the rural department currently had available—which in the 1970s meant a Boyle's machine, ether, and sheer clinical intuition—he never hesitated. Senior surgeons who worked alongside him during those bare-bones years would recall this quality decades later with the particular wistfulness of people who know they will never see its like again.
He was the son of a Deputy Superintendent of Police, which perhaps explains his unyielding dedication to duty. It does not, however, explain the gentleness. That came from somewhere else entirely—from his own particular nature, which consciously chose kindness over command and softness over authority in every interaction, every single day, for twenty-six years.
Arun Chintaman Tikle was born on July 25, 1944, in Yavatmal, Maharashtra. He entered Government Medical College (GMC), Nagpur, in 1963 and graduated with his MBBS in 1967.
He had deeply wanted to be a surgeon. He enrolled in an MS General Surgery program, but just six months in, severe financial constraints forced him to stop. He stepped back, calmly assessed his situation, and pivoted entirely to Anaesthesiology—the specialty that put him, as he would later say with a quiet smile, "on the other side of the operating table."
The forced detour became his life's vocation. He earned his Diploma in Anaesthesiology in 1971. On March 6, 1973, he joined MGIMS Sevagram as a Lecturer in Anaesthesiology. His first salary was exactly ₹740 per month. He accepted it without a single word of complaint.
The operating theatre of early MGIMS was housed in the old hospital building and equipped strictly with what was available, rather than what was ideal.
There was a Boyle's machine delivering anesthetic gases, with ether serving as the primary agent. There was exactly one Puritan Bennett ventilator, which had to be nervously shared between Medicine and Paediatrics. There were no recovery rooms. There were no pulse oximeters. There were no multiparameter monitors. "Monitoring" was entirely clinical: watching the pulse, observing the rise and fall of respiration, checking the patient's skin color, and measuring blood pressure manually with a mercury sphygmomanometer.
The anaesthesiologist's skill and experience were the monitoring system.
In 1977, four years after joining, Dr. Tikle took study leave to complete his MD in Anaesthesiology at GMC Nagpur, returning with formal postgraduate credentials to a department where none of the original faculty had held them. He became a Reader in 1980, assumed the department headship in December 1983 (succeeding the formidable Dr. R.N. Shetti), and was appointed Head of the Operating Theatres in 1986.
He and Dr. Shetti had been striking contrasts as colleagues. Shetti was imposing and authoritative—a presence felt immediately the second he entered a room. Dr. Tikle was soft-spoken and gentle, moving effortlessly between theatre orderlies, technicians, surgeons, and residents without ever needing to assert his authority. Where Shetti's influence was felt through force, Tikle's was felt through profound kindness. The department had been shaped by both, and the transition from one to the other had been absorbed without a single fracture.
The stories of Dr. Tikle in the operating theatre share one incredibly consistent feature: his absolute calm in the face of things going disastrously wrong.
Hypotension, hypoxia, unexpected hemorrhages mid-procedure—he navigated terrifying crises without allowing a single trace of anxiety to cross his face. He never communicated to surgeons or patients that a situation was deteriorating. This composure was not a performance; it was the hard-earned product of years of working in rural conditions where equipment routinely failed and improvisation was simply not optional. He had learned early that panic in an OR is highly contagious and utterly useless, and that the single most important thing an anaesthesiologist can give a surgical team is confidence.
He worked alongside Dr. K.K. Trivedi on highly complex cardiac procedures—open mitral valvotomy and pericardiectomy—conducted with the starkly limited monitoring resources of the 1970s. That such massive procedures were performed successfully at MGIMS in that era was a testament to two specialists pushing together against the absolute limits of what their setting could reasonably achieve.
Between 1984 and 1998, he mentored twenty-two MD students through their postgraduate training. He invested deeply in these students, not because the administrative structure required it, but because he intimately understood the terror young doctors faced when learning a specialty where a single error has immediate, fatal consequences. He prioritized their success over his own convenience, regularly, and entirely without announcement.
His blood pressure had been dangerously elevated for years, its exact cause unclear, and its management severely limited by the diagnostic tools and medications available at the time. On February 1, 1993, he suffered a massive heart attack. Thrombolysis was administered, but persistent chest pain required an urgent transfer to Bombay Hospital for coronary artery bypass surgery. He was only forty-eight.
During this terrifying family crisis, his son Harshvardhan sat for his MGIMS entrance examinations, writing three comprehensive science papers and a paper on Gandhian Thought while his father was actively recovering from open-heart surgery.
Dr. Tikle returned to work. He never allowed his compromised health to interfere with his responsibilities in any way that was visible to others. Vacations were routinely missed. Night calls were answered even when he was not officially scheduled. His colleagues were covered when they were overwhelmed. The pattern of exhausting service continued exactly as before, simply with the additional, dangerous variable of a failing cardiovascular system.
In the early hours of August 20, 1999, he died of a brain hemorrhage in the old Medicine ICU at Kasturba Hospital—the exact same institution where he had worked for twenty-six years. His family and friends were present, including Dr. Ulhas Jajoo, who remained steadily by his side. Understanding that death is a natural part of life, the family declined aggressive, futile interventions and allowed him to pass peacefully, with the exact same quiet dignity that had characterized everything he had done in life. He was fifty-five years old.
His wife, Kanchan, whom he had married in 1972, served as the warden of the MGIMS Girls' Hostel for twenty years, remaining a steadfast pillar of the campus long after his death until her retirement in 2010. She had been his steady companion through the colony quarters, the years of unreliable health, the cardiac surgery, and the final, quiet hours.
Their son, Harshvardhan, graduated from MGIMS in 1993 and completed his MD in Anaesthesiology from the exact same institution. He took the precise path his father had taken, in the department his father had built, anesthetizing patients in the very operating theatres where his father had once stood. (He now practices in Mumbai, while their daughter, Devyani, lives in Nagpur).
Gardening, cooking, and long solitary walks—these were the quiet pleasures of a man who did not need much outside the operating theatre and his small circle of friends. He had been handed a painful detour at twenty-six when his money ran out and his dream of surgery became impossible. He took that detour with deep equanimity and turned it into a magnificent life.
For twenty-six years in Sevagram, through inadequate equipment, institutional instability, and his own rapidly declining health, he had given the desperate surgeons his reliable "yes." And none of them ever had cause to regret it.
| 1944 | Born, 25 July, Yavatmal, Maharashtra |
| 1963 | Entered Government Medical College, Nagpur |
| 1967 | Completed MBBS |
| 1967 | Enrolled MS General Surgery — left six months in due to financial constraints; pivoted to Anaesthesiology |
| 1971 | Completed Diploma in Anaesthesiology |
| 1972 | Married Kanchan |
| 1973 | Joined MGIMS, 6 March — Lecturer in Anaesthesiology; salary ₹740 |
| 1977 | Study leave — completed MD Anaesthesiology, GMC Nagpur |
| 1980 | Promoted Reader |
| 1983 | Assumed department headship, December — succeeding Dr. R.N. Shetti |
| 1986 | Appointed Head of Operating Theatres |
| 1993 | Massive heart attack, 1 February — thrombolysis; coronary artery bypass surgery, Bombay Hospital; aged forty-eight |
| 1993 | Son Harshvardhan graduated MGIMS — sat entrance examinations while father was in cardiac surgery |
| 1999 | Died, 20 August — brain haemorrhage, Medicine ICU, Kasturba Hospital; aged fifty-five |
Postoperative morbidity and mortality in controlled and uncontrolled hypertensive patients
Combination of pentazocine and diazepam in short surgical procedures
Evaluation of use of extradural analgesic agents for postoperative pain relief
Evaluation of local analgesia in poor risk patients
Neonatal response related to induction delivery uterine incision delivery time related to general spinal anesthesia
Evaluation of use of intrathecal buprenorphine hydrochloride for postoperative pain relief
Comparative study of maternal neonatal neurological responses in general spinal anesthesia
Effects of various concentrations of inhalation anesthetic agents on maternal neonatal responses
Evaluation of glycopyrrolate and atropine along with neostigmine during reversal of neuromuscular black
Comparative study of cardiovascular effects of vecuronium pancuronium in anaesthetized patients
Intranasal opiates on alternative route for- premedication
Clinical efficacy of oral clonidine as premedication
Effect of metoprolol on circulatory responses to tracheal intubations
Blood loss in tonsillectomy
Comparative study of intubating conditions with non – depolarizing muscle relaxants
Use of atracurium for Caesarean Section
Comparison of preemptive epidural tramadol with ketamine for postoperative pain relief
Efficacy of prophylactic intravenous ondansetron for prevention of postoperative nausea and vomiting in pediatric patients
Comparative study of prophylactic intravenous ondansetron metoclopramide in control of postoperative nausea and vomiting in gynecological surgery
Efficacy of esmolol for controlling the hemodynamic responses to endotracheal intubations
Evaluation of use of intrathecal neostigmine for postoperative pain relief
Dr. Sudha Jain
MD Anaesthesiology, Indira Gandhi Government Medical College Nagpur (1985)

She had desperately wanted to be a surgeon. Dr. A.M. Bhole, the surgery department head at Indira Gandhi Government Medical College in Nagpur, dismissed the ambition with the exact, irritating confidence of a man who has never once had to question his own assumptions. "Surgery is not for women," he told her. The scalpel, apparently, was too heavy for her hands.
Dr. Aalok Ghosh, a professor of anaesthesiology, offered a radically different view. "Anaesthesia," he told her, "is a balance of science and skill. It is a thinking doctor's field." She was persuaded. She spent the next three years immersing herself in the high-stakes world of inhalational agents and intravenous drugs, completed her MD in April 1985 with a thesis on anaesthetic techniques for direct laryngoscopy, and arrived in Sevagram that November.
It was the beginning of a magnificent, sprawling career that would span leprosy wards in Seoni, high-tech cardiac theatres in Delhi, a rural ICU in Madhya Pradesh, and thirty-two years across two separate tenures at MGIMS. She would ultimately shape the Sevagram anaesthesiology department into something considerably greater than what she had found.
The surgeon who refused to have her lost a good doctor. Anaesthesiology gained a master.
Sudha was born on December 20, 1958, in Chandrapur, the eldest of four children. Her father, Dr. Kapoor Chand Jain, began his career as a laboratory technician at the Government Hospital before transitioning to Ayurvedic medicine, eventually rising to become a Professor and Head of Department at the Government Ayurvedic College in Nagpur. Her mother was the quiet, steady anchor of the household.
Sudha's early education took place in a Hindi-medium school in Mandi Bamora, Madhya Pradesh. Multiple classes were held simultaneously in a single hall, with students sitting on simple floor mats. It was the kind of elemental, bare-bones simplicity that either permanently defeats ambition or forges unbreakable resilience. In her case, it forged resilience.
She moved to Nagpur for her later schooling, completing her pre-medical studies as a National Merit Talent Scheme scholar who excelled effortlessly in both academics and extracurriculars. In 1976, she gained admission to Indira Gandhi Government Medical College.
When the surgery door was abruptly slammed shut by casual sexism, the anaesthesiology door was opened by genuine respect for her intellect. She walked through it without a single regret. In 1985, seeking stability and a place to actually build something rather than endure the constant specter of government transfers, she answered an advertisement for a Lecturer’s post at MGIMS.
During her interview, Dr. Sushila Nayar grilled her on Ludwig's angina. Dr. Mankeshwar questioned her on severe tetanus. Sudha answered with growing, unshakeable confidence. While another candidate was initially selected above her, he did not take the post. On November 8, 1985, she arrived in Sevagram.
The contrast with her government training environment was immediate and striking. By the standards of 1985, the operating theatres at MGIMS were impressively equipped. There were upgraded Boyle's Anaesthesia Machines with Mark 2 and Mark 3 Halothane vaporizers. There was an ample supply of nitrous oxide—a gas that was both expensive and absolutely essential for high-risk cases. Thiopental was used routinely for induction, alongside non-depolarising neuromuscular blockers considered far too costly for most government institutions.
While Mayo Hospital in Nagpur—the largest district hospital in Vidarbha—routinely had to suspend major elective surgeries in May because the brutal heat made the operating rooms unworkable, MGIMS was actively constructing centrally air-conditioned theatres.
During her first weeks, the ORs were temporarily housed in the former Burns ward while renovations proceeded. But the institutional commitment to excellence was deeply visible. She found a well-equipped blood bank, a reliable post-anaesthesia care ward, and a culture where anaesthesiologists were integral to the full spectrum of patient care. Here, they monitored complex cancer surgeries with raw clinical skill rather than electronic equipment, bringing deep judgment to the operating table.
She rose to Reader in August 1989. The department remained critically understaffed throughout her first tenure—a massive constraint she managed with quiet, iron determination rather than complaint.
In 1992, two things happened simultaneously. She cleared the MPSC examination, securing a government posting at the newly opened medical college in Yavatmal. She also married Dr. S.C. Jain, a Surgical Specialist at the Government District Hospital in Seoni. Wanting to be near her new family, she resigned from Sevagram.
But Dr. K.N. Ingley, the former Physiology Head at MGIMS who had recently joined the new medical college in Sawangi, saw in her exactly the person needed to build an anaesthesiology department from absolute scratch. He convinced her to take the challenge. She became Jawaharlal Nehru Medical College’s first Professor and Head of Anaesthesiology. The institution was just twelve kilometers from Sevagram, but a world apart in character—a for-profit venture still finding its identity. She built the foundation, stayed two years, and then moved to Seoni to finally join her husband.
In Seoni, the master anaesthesiologist deliberately pivoted to become a Leprosy Medical Officer. She conducted door-to-door village work, diagnosing, treating, and restoring basic human dignity to patients whose condition carried brutal social stigma. Finding the exact same Gandhian impulse toward service that Sevagram had planted in her, she contributed to the National Leprosy Elimination Programme for three years, presenting her vital work at the World Leprosy Congress in Agra in 2000.
When Seoni District Hospital established a six-bed ICU in 1999, she immediately trained at GMC Nagpur and managed the unit for two years. Relentlessly seeking new skills, she trained as an observer in cardiac anaesthesia at ESCORTS Hospital in Delhi in 2001, returning to assist with cardiac surgeries at Nagpur's Super-Specialty Hospital.
In 2004, she came back home to Sevagram. This time, she brought her husband with her. Taking voluntary retirement from his government service, he joined the Surgery department, while she returned as a Professor on September 1, 2004. The circle was complete, but the arc it described had been far longer and richer than anyone could have anticipated when she first drove away from the campus twelve years earlier.
Her second tenure lasted eighteen years. She mentored eighteen postgraduate students through their MDs in Anaesthesiology, guiding crucial research on induction agents, pain management, and airway management. She led the massive expansion of the department's operating theatres, watching her specialty completely transform from clinical intuition and Boyle's machines to advanced electronic monitoring and pulse oximetry.
Of all her monumental achievements, one stood out with particular pride: she fiercely led a government project to train basic MBBS doctors in administering anaesthesia for emergency caesarean sections in highly remote areas where no specialist anaesthesiologist was available. Her own professional association officially resisted the idea. She remained completely resolute. The training went forward anyway. In desperate, rural places where the choice was between an anaesthesiologist who simply wasn't there, and an MBBS doctor who had been trained to act safely in an emergency, her stubborn insistence mattered directly to the survival of countless mothers and infants she would never even meet.
Sagar, Seoni, Sadar, Sevagram, Sawangi: five places that shaped her.
She had started her education sitting on a floor mat in Mandi Bamora. She had been bluntly told that surgery was not for women. She had spent three decades learning that absolutely every constraint could be worked around. And she had ultimately returned to the very institution that had first given her the operating theatres she needed to do the miraculous work she was capable of.
Her daughters inherited that exact same drive: Nidhi became a software engineer in the United States; Dr. Deepshikha Jain became a pediatrician (MGIMS Class of 2004); and Dr. Avantika Jain Patni became a pathologist (MGIMS MD 2024). They inherited a mother who had practiced in high-tech teaching hospitals, district clinics, leprosy wards, rural ICUs, and village doorsteps.
After her official retirement on December 31, 2022, Jawaharlal Nehru Medical College in Sawangi reached out once again—their clinical skills lab desperately needed her expertise. Naturally, she went. She served there for two-and a half years before another call arrived in May 2025, this time from the newly founded Dr Rajendra Gode Medical College in Amravati. The offer was for the highest position in the institution: Dean. She accepted the role, and the immense challenge that came with it. Dr. Sudha Jain simply did not seem to know how to stop being useful.
| 1958 | Born, 20 December, Chandrapur, Maharashtra |
| 1976 | Entered Indira Gandhi Government Medical College, Nagpur — National Merit Talent Scheme scholar |
| 1982 | Completed MBBS |
| 1985 | Completed MD Anaesthesiology, April — thesis on anaesthetic techniques for direct laryngoscopy |
| 1985 | Arrived MGIMS, 8 November — Lecturer in Anaesthesiology |
| 1989 | Promoted Reader, August |
| 1992 | Married Dr. S.C. Jain — Surgical Specialist, Government District Hospital, Seoni |
| 1992 | Left MGIMS — first Professor and Head of Anaesthesiology, JNMC Sawangi |
| 1995 | Moved to Seoni — Leprosy Medical Officer; door-to-door village work |
| 1999 | Managed six-bed ICU, Seoni District Hospital — trained at GMC Nagpur |
| 2000 | Presented leprosy work — World Leprosy Congress, Agra |
| 2001 | Observer training in cardiac anaesthesia — ESCORTS Hospital, Delhi |
| 2004 | Returned to MGIMS, 1 September — Professor; husband joined Surgery department |
| 2022 | Retired, 31 December — after eighteen years in second tenure |
| 2023 | Joined JNMC Sawangi clinical skills lab |
| 2025 | Joined Dr. Rajendra Gode Medical College, May |
Dr. K.K. Hariharan
MDS Dental Radiology, Grant Medical College Mumbai (1970)
Associate Professor of Dental Surgery · Eleven Years at Sevagram · The Man Under the Tamarind Tree
Kalapathi Krishnagiri Hariharan was born on February 10, 1944, in Lahore — delivered by a dai rather than a doctor, a detail that remained a core part of how he understood his own roots. When Partition tore the country apart, the family relocated: first to Mumbai, then Kerala, and finally back to Mumbai, where his father R.K. Giri worked for the Life Insurance Corporation. Young Hari wanted to join the Navy; his father flatly refused. He enrolled in dental school instead, earning his BDS from Grant Medical College in 1967 and his MDS in Dental Radiology from the same institution in 1970.
Unconventionally, he began his career not under a senior dentist, but as a junior to Dr. Rohit Mehta, a well-known homoeopathy practitioner in Mumbai — an early, widening encounter with clinical empathy that he would carry effortlessly because it was simply embedded in his nature. He was a Thalayali by heritage, from the Palghat Brahmin community, speaking Thalayalam — a charming amalgamation of Tamil and Malayalam — alongside Hindi, Marathi, and English, switching between them with the fluency of someone for whom adaptation had become instinct.
He came to Sevagram in October 1971 not because he was chasing a grand Gandhian dream, but because he simply needed a steady job. He packed his bags without much fuss.
Under the old tamarind tree, on slow, heavy afternoons when the bus had not yet come, the young doctors gathered. Dr. Narang, Dr. Dhawan, Dr. Ahuja, and Hariharan would sit for hours — half in easy conversation, half in patient watchfulness — studying the new arrivals as the State Transport bus finally groaned into the campus. A man stepping down with a walking stick meant a patient for Dr. Ahuja. A hand pressed to a swollen cheek, a sudden grimace of toothache? There was no question. That was Hariharan's man, already destined for the old, rickety dental chair.
He had arrived on that same bus in October 1971 with a sharp gaze, restless energy, and a wide, disarming smile that would become his signature across twelve years. He adapted fast — moved into the college quarters, made friends over endless cups of tea, got the bare-bones dental OPD running, and became the local expert not just at painless extractions, but at putting terrified patients at ease with the exact same quick wit he used on his colleagues.
The dental department he arrived at was a department in name only — a creaky chair, a few battered tools, and a waiting room of rural patients who understood dental treatment purely as brute extraction. No wards. No X-ray machine. Though he had specialised in dental radiology, he was forced to work by touch, sight, and raw instinct. He got the OPD running and slowly grew the patient numbers. In a region where roadside tooth-pullers were the standard norm, he became the trusted, educated alternative — the monumental difference between having a tooth blindly yanked and having it treated by a man who understood the anatomy of the jaw.
On November 7, 1973, he married Chella Iyer, a brilliant young gynaecologist from Mumbai. By 1974, he had risen to Reader in Dental Surgery. Research and publications were never where his heart lay — in nearly a decade, he co-authored exactly one case report, and he offered no apologies. His real domain was people: the conversations, the friendships, the small everyday theatre of human life that he inhabited with the full, crackling energy of someone who found other people genuinely fascinating. He was at the absolute centre of faculty theatrical productions, card games, and casual gatherings. He was the man around whom things instantly became livelier.
He could sit across the card table from the formidable Badi Behenji, cracking jokes that made her laugh freely and forget her legendary sternness. He was brilliant, difficult, generous, and entirely consuming — hated and loved in equal measure, the two faces coexisting in the exact same person, sometimes within the exact same afternoon.
On March 28, 1983, he packed up the life he had built in Sevagram and left it for good. He joined Malad Suchak Hospital in Bombay, then came West Africa — six years that his daughter Anuradha would later call the best years of her life. At West End Hospital, he built a stellar reputation quickly, earning wide respect in the medical community. Africa finally gave him a canvas large enough for the many talents that Sevagram's scale had not fully required. After West Africa, he spent years in Riyadh, adapting with characteristic quickness to a radically different healthcare system.
He returned to India in 1992, briefly returning to MGIMS in the hope that his daughter might secure admission under the faculty quota. When that did not materialise, he joined Sharad Pawar Dental College as Professor of Oral Medicine and Radiology. Students admired his diagnostic precision and spoke in hushed, terrified tones of his famous temper. He cycled through Solan, Akola, and Amravati before finally settling in Patiala.
Somewhere along the way, alcohol took hold. The sharp-witted, quick-footed man who had filled rooms with effortless laughter began to fade. By his sixties, he had become a shadow of the man the Sevagram years had known. In 2006, at sixty-two, a massive heart attack struck him down in Patiala.
He had loved dogs and cats with fierce, unapologetic tenderness — a love he passed to his daughters that continues to shape their lives today. His daughter Manisha wrote: "I have never met anyone in my life with so much talent and passion." Sevagram had been a sanctuary — the place where, for a while, his spirit could soar before the heavy burdens of life drew him back down to earth.
He had arrived on a State Transport bus in October 1971 with a sharp gaze, restless energy, and a wide smile that became his signature. The man who could make Badi Behenji laugh at the card table, who claimed his patients by their grimaces from under the tamarind tree, who built a one-man dental department in a village that did not yet understand that dentistry was more than brute extraction — that man deserved a longer and less shadowed ending. What he got was sixty-two years and the honest record of what they contained: the brilliance, the warmth, the talent, the extreme difficulty, and the aching gap between what was, and what could have been.
| 1944 | Born, 10 February, Lahore — delivered by a dai; family relocated to Mumbai via Kerala after Partition |
| 1967 | Completed BDS, Grant Medical College Mumbai |
| 1970 | Completed MDS Dental Radiology, Grant Medical College Mumbai |
| 1971 | Joined MGIMS, 1 October — arrived by State Transport bus; one-man dental department; creaky chair, no X-ray |
| 1973 | Married Dr. Chella Iyer, 7 November — gynaecologist; another of Dr. Nayar’s paired appointments |
| 1974 | Promoted Reader in Dental Surgery |
| 1980 | Applied for Government Dental College, Bombay — did not work out; remained in Sevagram |
| 1983 | Left MGIMS, 28 March — joined Malad Suchak Hospital, Bombay |
| 1983 | West Africa — six years at West End Hospital; built stellar reputation |
| 1989 | Riyadh, Saudi Arabia — years in Middle East healthcare |
| 1992 | Returned to India — briefly returned to MGIMS; then Professor, Sharad Pawar Dental College |
| 1995 | Solan · Akola · Amravati · Patiala — each town receiving some part of him |
| 2006 | Died, Patiala — massive heart attack; aged sixty-two |
Dr. Ashok Pakhan
Postgraduate Diploma in Orthodontics, St. George Hospital Mumbai

He had desperately wanted to study medicine. He missed the admission cutoff by exactly five marks.
Dentistry was not his choice; it was his only remaining option. In the early 1970s, seats in Indian dental colleges often went vacant. Medicine was the coveted, fiercely contested prize; dentistry was simply what remained after the prestigious allocations were made. He enrolled at Government Dental College, Nagpur, with the quiet, heavy reluctance of someone who had been denied the door he wanted and was forced to make the best of the one that had opened. Yet, by the time he finished, what had begun as pure reluctance had transformed into genuine craft. He had mastered the discipline he once actively resisted.
This is not an uncommon story in Indian medicine of that era—the five marks that permanently redirected a career, the second-choice path slowly becoming the right one. What is uniquely characteristic of Ashok Pakhan is the total absence of resentment in the telling, and the profound contentment that accumulated around the work itself, rather than the status it conferred.
He spent twelve years at MGIMS in a tiny department that offered just ten lectures a year to medical students, possessed no postgraduate program, and received minimal institutional recognition. Yet, he built a fiercely loyal patient following among villagers who returned year after year—sometimes arriving by bullock cart—greeting him with folded hands and genuine gratitude. He never once measured himself against the towering physicians and surgeons around him. His deep satisfaction lay purely in the steady, reliable work of healing. That was enough for him. And it is not a small thing for a man to know that his life is enough.
Ashok Pakhan was born on November 14, 1953, in Murha Kh, a remote village sixty kilometers west of Amravati. His father, Jagannath Atmaram Pakhan, farmed the land. His mother, Parvati, kept the home. As their only child, he grew up surrounded by the scent of tilled earth, dry leaves, and cattle at dusk. This specific sensory formation of rural Vidarbha in the 1950s tended to shape two kinds of people: those with a desperate hunger to leave, and those with a profound capacity for rootedness that persisted through whatever came after. Ashok was the latter.
The village had a single primary school. He studied there through the fourth grade, moved away to live with an aunt for middle school, and eventually made his way to Vidarbha Mahavidyalaya in Amravati. In the 1970s, this kind of educational journey—each step negotiated entirely independently, with no parental guidance because none was available, managing admissions and lodging entirely alone—was standard survival for rural boys who wanted to study. There was no one to explain how the system worked. You figured it out, or you did not advance. Ashok advanced.
He enrolled at Government Dental College, Nagpur, after the painful five-mark miss in 1972, earning his BDS in 1976. Though internships were not yet mandatory, he was selected for a grueling, year-long clinical assistantship under seasoned surgeons. He then moved to Mumbai for postgraduate studies in orthodontics at St. George Hospital, writing a thesis on the effects of denture removal.
One day, he spotted a small, unassuming advertisement on a notice board: MGIMS, Sevagram, needed a registrar in dental surgery. Jobs were scarce. He applied, was selected, and in March 1980, he arrived.
The department he arrived at was incredibly small, even by early MGIMS standards. Dr. K.K. Hariharan led it, Ashok was his only colleague, and between the two of them, they handled absolutely everything that came through the door: scaling, extractions, crowns, and bridges. They delivered ten lectures a year to medical students on fractures, tumors, and the intricate, unforgiving mechanics of the human jaw. Dr. Savita Borle joined, followed by Dr. Rajiv Borle, giving the team a few more hands. Then, Dr. Hariharan left in March 1983, and Ashok carried on.
The staff who made the department function were few, but fiercely dependable. Dilip Chinchkhede handled hygiene, Baby Dhole oversaw nursing, and Baba Deshmukh kept the equipment running with the quiet competence of a man who understood that in a resource-starved setting, the equipment’s reliability was just as vital as the surgeon’s skill.
Resources remained severely limited throughout his tenure. There were no resident doctors to supervise and minimal intersection with the elite clinical education happening in the hospital wards and major operating theaters around him. The dental surgery department existed in a state of structural isolation within the medical institution—present, highly necessary, and heavily visited by patients, but not truly integrated into the teaching and research culture that defined the rest of MGIMS.
Dr. Pakhan understood this hierarchy perfectly and made his absolute peace with it. He did not seek recognition he was not positioned to receive. He focused entirely on the patients in his chair, on the precise mechanics of his procedures, and on the trust he was building over years of honest practice. He rose to Reader during his tenure—a promotion earned purely on the sheer strength of his clinical work, rather than the institutional platform that work occupied.
Soft-spoken and deeply unassuming, he moved through his days with quiet confidence. Marathi was his first language; Hindi was available when needed. He listened intently, examined thoroughly, and explained treatments with absolute honesty. He never oversold what Sevagram’s modest dental resources could offer, and he never raised expectations that his limited equipment or fragile supply chain could not meet. Patients always knew exactly where they stood with him.
The devoted following he built was a direct consequence of this transparent quality. Villagers who came once returned with their families. They offered folded hands and simple expressions of gratitude—people who had perhaps never before received from a professional medical institution the specific combination of high competence and deep respect that he offered them without calculation.
Among the clinical highlights of this period was his vital collaboration with Dr. Suhas Jajoo of Surgery. Together with Dr. Savita Borle, they prepared specialized prostheses that helped ENT surgeons manage complex head, neck, and maxillofacial cases directly in the operating theater. It was the kind of cross-departmental contribution that made a tiny, isolated department’s presence felt beyond its own walls.
In 1992, Dr. K.N. Ingley—who had been a professor at MGIMS and was now Dean of the medical college in Sawangi—personally asked Dr. Pakhan to take on the role of Dean at their newly established dental college. He left MGIMS and moved to Sawangi. Because regulations required five years of service as a full Professor before he could formally become Dean, he taught patiently until August 1998.
Then, he held the Deanship for twenty unbroken years.
This staggering two-decade administrative tenure was, in its own way, a perfect expression of the exact same qualities he had displayed in Sevagram: he was steady, reliable, patient, and entirely focused on building something durable rather than accumulating fleeting recognition. He retired at sixty-five in 2018, but stayed on to oversee academic assessments across medicine, dental surgery, Ayurveda, and physiotherapy until 2023, when he finally stepped away from institutional life entirely.
He had married Padma Jhambre in 1983, three years into his Sevagram tenure. Together, they raised three children who grew up in the orbit of institutional medicine: Kulaj (born 1985), Aishwarya (a dermatologist), and Arjavi (a musculoskeletal physiotherapist). The only child of a Murha Kh farmer had successfully produced a family in which clinical practice had become the generational inheritance.
Looking back, he describes his Sevagram years without hesitation as the finest of his life.
The grueling struggle to build a department from nothing had deepened his resolve rather than depleted it. He remembers the patients arriving by bullock cart, greeting the doctors with folded hands. He remembers the slow, purposeful rhythm of a village hospital where the work was the meaning, and the meaning was entirely sufficient. The past lingers, he says, but the work done there remains—standing firm, just like the tilled land he came from.
He had missed the medicine cutoff by five marks, and proceeded to build a magnificent career in the specialty that remained available to him. He arrived in Sevagram without the towering prestige of the physicians and surgeons whose departments filled the hospital’s massive wards. He had understood exactly what his position within the institution was, accepted its structural limits with total grace, and within those narrow limits had done the work with a quality and consistency that produced a reputation in the surrounding villages that no advertisement could ever buy.
Ambition had not driven him. Contentment had. And that contentment was deeply earned—through the tilled earth of Murha Kh, through the five-mark miss and the quiet pivot, and through the twelve years of extractions, crowns, bridges, and lectures on jaw mechanics to medical students who would not become dentists, but who always remembered the soft-spoken Reader who had explained the human jaw to them with honesty, patience, and absolutely no expectation of anything in return.
| 1953 | Born, 14 November, Murha Kh, near Amravati — only child; father a farmer |
| 1972 | Missed medicine cutoff by five marks — enrolled Government Dental College, Nagpur |
| 1976 | Completed BDS, GMC Nagpur — year-long clinical assistantship under seasoned surgeons |
| 1977 | Postgraduate studies in orthodontics, St. George Hospital Mumbai — thesis on effects of denture removal |
| 1980 | Joined MGIMS, 1 March — Registrar in Dental Surgery; saw small advertisement on a notice board |
| 1983 | Dr. Hariharan left — Ashok carried on alone; married Padma Jhambre |
| 1985 | Son Kulaj born |
| 1986 | Promoted Reader in Dental Surgery |
| 1992 | Left MGIMS, 1 June — invited by Dr. K.N. Ingley to join dental college, Sawangi |
| 1998 | Formally appointed Dean, Sawangi Dental College — held for twenty unbroken years |
| 2018 | Retired at sixty-five — continued overseeing academic assessments until 2023 |
Dr. Rajiv Borle
MDS Oral and Maxillofacial Surgery, Government Dental College Nagpur (1984)

Dr. Gupta took the official Army appointment letter from his young student's hand, tore it definitively in two, and said: "The Army is not for you. Your path lies in academics."
Raju never forgot that moment.
The offer had been deeply attractive. Captain Borle. A salary of ₹1,850 a month—nearly three times what a medical college registrar made. It offered total security, immediate status, and a title that had an undeniable ring to it. He had walked into Dr. Gupta’s office with doubt already gnawing at him. The old professor resolved that doubt in a single, violent gesture.
That torn letter was the true beginning of an academic career that would eventually produce a definitive textbook on oral and maxillofacial surgery, hundreds of research papers, an impressive h-index of 20, the Vice-Chancellorship of an entire medical university, and a Lifetime Achievement Award from the Association of Oral and Maxillofacial Surgeons of India.
Sevagram was where this immense foundation was laid. He spent just two and a half years there, effectively running a one-man dental surgery department. Yet, in that incredibly brief span, he published twenty-four papers and violently expanded his surgical repertoire. Through fierce collaborations with surgeons like Dr. Suhas Jajoo and Dr. Ravinder Narang, he pushed into complex reconstructive territory that most dental surgeons in rural institutions would never even attempt to access.
He was chronically overstretched, severely under-supported, and deeply frustrated by the structural constraints of running a tiny dental clinic inside a massive medical hospital. He finally left in September 1987. But the sprawling, magnificent career that followed was built entirely on what the frustration and the relentlessness of Sevagram had required him to become.
Rajiv Borle was born on March 28, 1961, in Parbhani. His father, Mukund Borle, a professor at Punjabrao Krishi Vidyapeeth, was moved constantly by government postings—from Parbhani to Nagpur to Akola. Each move meant a new school, and a blackboard smeared with the half-erased lessons of a previous class. Rajiv adapted. Each time, he stepped into a classroom where absolutely no one knew his name, and left with friends who would never forget it.
This adaptability was not merely social resilience; it was the bedrock of a temperament that would eventually navigate vicious institutional politics, pioneer surgical innovations, command administrative leadership, and ultimately face the particular cruelty of ALS without ever losing its essential forward momentum.
Two things held his heart in those early years: medicine and cricket. Cricket came first. He kept wicket and opened the batting for the Akola Cricket Club, competed fiercely in the Cooch Behar Trophy Under-19 tournaments, and played in Nagpur’s Gazdar League at Reshimbagh Ground. He knew the names of the men who had entered Test cricket through that exact same pathway, and he watched them with the sharp attention of someone measuring the distance to the top. Those who saw him play noted with deep affection that had the IPL existed in his youth, franchises would have competed furiously for his signature.
In 1977, he missed the medical college admission cutoff by a single mark. His father suggested agricultural engineering; Rajiv lasted exactly one month.
Dentistry did not seize him immediately either. For his first two years, his mind drifted back to cricket and the white medical coat he had originally imagined. But in his third year, oral and maxillofacial surgery finally found him, guided by Dr. M.A. Wadkar’s steady surgical hands and Dr. D.S. Gupta’s razor-sharp intellect. His MDS thesis—a complex animal study on the effects of toxins on buccal mucosa—revealed a mind that questioned, probed, and utterly refused to settle for the merely descriptive. He completed his BDS in 1982, his MDS soon followed, and Dr. Gupta tore up the Army letter.
Savita Dawande had been his classmate and closest confidante at Government Dental College, Nagpur. They married on February 7, 1984, in a simple registered ceremony with no fanfare; their lives were moving far too fast for grand celebrations.
Savita was already at MGIMS as a house officer. Rajiv came to Sevagram, taking a registrar’s post simply to follow her. They began their life together in a cramped room at Dharmanda Hostel, moving eventually to Guru Nanak Colony. Their evenings stretched long with intense conversations about medicine, politics, and the future, shared among a tight community of young, ambitious doctors. Life was incredibly simple, and by his own account, incredibly rich.
Dr. K.K. Hariharan’s legendary twelve-year innings at the dental clinic had ended before Raju arrived; their tenures never overlapped. Dr. Ashok Pakhan was the lone lecturer heading the department. A lecturer’s post remained entirely out of Raju’s reach until Dr. Pakhan’s promotion finally opened the position—a bureaucratic frustration he absorbed without ever allowing it to slow his work.
He formally joined as a Lecturer on January 29, 1985. From that point until his departure in September 1987, he effectively ran the dental surgery department as a one-man operation. He managed the patients, performed the surgeries, oversaw the post-operative care, handled the endless paperwork, and still managed to write and publish twenty-four academic papers.
The surgical collaborations that defined his Sevagram tenure were forged in the main operating theaters with Dr. Suhas Jajoo and Dr. Ravinder Narang. Together, they aggressively pushed the boundaries of oral surgery, trauma care, and cancer reconstruction. Rajiv expanded his own surgical repertoire deep into cleft lip and palate repair, severe facial trauma reconstruction, and complex flap techniques for large defects. Precision mattered to him deeply—not just as a surgical technique, but as a defining quality of character.
In 1985, their son Firoz was born in Sevagram. The campus gave the Borles, as it had given so many couples before them, a child alongside a career. Firoz would eventually complete his MBBS and MS from MGIMS, earn his MCh in Plastic Surgery from Tata Memorial Hospital, and join JNMC Sawangi as a plastic surgeon. The rural institution that had formed his parents became the professional foundation of his own surgical training.
The severely limited resources and the structural isolation of a dental clinic within a medical institution eventually chafed beyond what remained sustainable. There were only ten lectures a year, no postgraduate program, and minimal intersection with the institution’s broader research culture—despite his own prolific, unrelenting publishing.
In September 1987, he left Sevagram for the Civil Hospital in Wardha, balancing government service with a booming private practice. His reputation as a maxillofacial surgeon exploded; patients began traveling from considerable distances just to sit in his chair.
By 1993, he left the district hospital. A brief period in Amravati led to a fateful meeting with Dutta Meghe, the founder of what would become the Datta Meghe Institute of Medical Sciences. Meghe instantly recognized in Raju the rare combination of elite surgical excellence, fierce academic drive, and ruthless administrative capability that an expanding institution desperately required.
He joined in 1995. He became an Associate Professor in 1996, a Professor soon after, Vice Dean by 2008, and eventually the Vice-Chancellor and Director General of Administration. It was a staggering administrative arc for a man who had been pushed into academics by a torn Army letter.
His partnership with Dr. S.R. Johrapurkar at Datta Meghe was, utilizing the cricket analogy his profile naturally reaches for, the partnership of Sachin Tendulkar and Virender Sehwag. Johrapurkar’s meticulous, grinding precision perfectly complemented Raju’s audacious, aggressive expansiveness. Together, they rapidly built the institution’s academic reach into nursing, physiotherapy, Ayurveda, and sprawling postgraduate education. The analogy perfectly fit the man who had once opened the batting in the Cooch Behar Trophy.
His academic output never slowed. He published extensively on oral submucous fibrosis, head and neck cancers, and maxillofacial trauma. He authored a definitive textbook on Oral and Maxillofacial Surgery and a Manual of Operating Room Discipline and Protocol. He was a man who had published twenty-four papers in two and a half years at a rural clinic, and he simply never stopped. In December 2021, the Association of Oral and Maxillofacial Surgeons of India recognized his monumental body of work with its Lifetime Achievement Award.
In October 2015, Savita died of metastatic thyroid carcinoma. She had been his absolute anchor since their days at GDC Nagpur—his classmate, his confidante, and the woman who had preceded him to Sevagram and turned a cramped hostel room into a home. She was only fifty-four. The loss was immeasurable.
Music, which had been a long-deferred passion since his youth, finally found its proper moment in his life. In Sawangi, he began rehearsals with a small group, building a collection of karaoke tracks numbered in the hundreds. He acquired a tabla, a harmonium, a guitar, and a dhol, fully inhabiting the rhythm during the enforced stillness of the COVID-19 pandemic. What had once been a purely personal retreat became a source of profound joy shared with others, the music filling the empty, grieving spaces of his life.
Then, Amyotrophic Lateral Sclerosis (ALS) began weakening his muscles. It is a progressive neurological disorder that does not negotiate; it simply takes what it takes on its own brutal schedule. The man who had driven cars with a racing driver’s finesse, who had played vicious square cuts off fast bowlers, who had performed cleft lip surgeries of such microscopic precision that children awoke grinning like Cheshire cats, found himself physically required to slow down.
He slowed. But he did not stop.
Charismatic, strikingly handsome, and possessing the strong, grounded physique of a wicketkeeper, he had always carried himself with a blend of intense poise, confidence, and what those who loved him honestly described as a distinct touch of arrogance. It was just enough to leave people stunned and captivated. He had moved through hospital corridors, administrative offices, and operating theaters with that exact same effortless authority.
The music, the brilliant surgery, the cracking square cut, the complex administrative problem resolved by a flash of sudden insight—these were not different expressions. They were all the exact same person. The restless adaptability that had moved him between schools in Parbhani, Nagpur, and Akola was simply expressed across every single domain his sprawling career required.
The two and a half years in Sevagram—the one-man department, the twenty-four papers, the audacious surgical collaborations that pushed far beyond what the department’s meager resources should have permitted—were the absolute foundation on which everything else was built. Like a beautifully played cricket innings, each difficult delivery was carefully negotiated, and each run was ruthlessly accumulated toward something vastly larger than the moment required.
| 1961 | Born, 28 March, Parbhani — father professor at Punjabrao Krishi Vidyapeeth; frequent government postings |
| 1977 | Missed medical college cutoff by one mark — agricultural engineering lasted one month |
| 1982 | Completed BDS, Government Dental College Nagpur — oral and maxillofacial surgery under Dr. Wadkar and Dr. Gupta |
| 1983 | Army appointment letter — Dr. Gupta tore it in two: “Your path lies in academics” |
| 1984 | Married Savita Dawande, 7 February — registered ceremony; arrived in Sevagram as registrar to follow her |
| 1985 | Joined MGIMS as Lecturer, 29 January — one-man dental surgery department |
| 1985 | Son Firoz born in Sevagram |
| 1985 | Surgical collaborations with Dr. Suhas Jajoo and Dr. Ravinder Narang — cleft lip, facial trauma, complex flap reconstruction |
| 1987 | Left MGIMS, September — 24 papers published in 2.5 years; joined Civil Hospital Wardha |
| 1993 | Left district hospital — private practice; meeting with Dutta Meghe |
| 1995 | Joined Datta Meghe Institute — Associate Professor 1996; Professor; Vice Dean 2008 |
| 2015 | Wife Savita died, October — metastatic thyroid carcinoma; aged fifty-four |
| 2021 | Lifetime Achievement Award — Association of Oral and Maxillofacial Surgeons of India, December |
| 2021 | Vice-Chancellor and Director General of Administration, Datta Meghe Institute |
| 2022 | ALS diagnosis — progressive neurological illness; slowed; did not stop |
Dr. Savita Borle

In the fiercely hierarchical world of academic medicine, titles are the absolute currency of success. To watch the people you trained rise past you, claim those titles, and eventually become your superiors is a bitter pill that very few doctors can swallow.
Dr. Savita Borle swallowed it without a single grimace.
Her juniors—doctors she had personally taught how to run a busy OPD with patience and precision—went on to become Heads of Departments. In a space where egos constantly clashed, she moved effortlessly, simply because she refused to feed one of her own. She bore absolutely no resentment when working under the very people she had mentored. She simply did what she had always done: she showed up, she treated everyone as an equal, and she did the work beautifully.
She left behind no grand academic pronouncements and no frantic pursuit of accolades. Instead, she left something far more enduring: a thirty-five-year lesson to the entire institution on how to live with absolute, unshakeable grace.
Savita Dawande was born on November 21, 1960, in Daryapur. Medicine ran thick in her blood. Her grandfather, Dr. Purushottam Laxman Gawande, had been a doctor. Her father, Dr. Markand Dawande, was a physician of the old school—a man with steady hands, a sharp mind, and an unwavering sense of duty who belonged to the very first batch of GMC Nagpur.
Her childhood moved to the unpredictable rhythm of her father’s government postings. She attended Jubilee High School in Chandrapur before shifting to New English High School in Wardha, where her father took charge as the Resident Medical Officer (RMO) of the district hospital in 1971. The frequent transfers and hostel living disrupted her studies, but they also forged her resilience.
After completing her 11th grade at Jankidevi Bajaj Science College and her B.Sc. at Vidarbha Maha Vidyalaya, she initially secured admission in physiotherapy. She spent a month there and began to like the subject. But fate, and the rigid medical admission system, nudged her elsewhere. Her admission was upgraded, and at her father’s behest, she joined Government Dental College, Nagpur, in 1977.
It was at Dental College that Savita met Rajiv Borle. What began as a natural, easy friendship soon grew into something much deeper. Their bond was unshakeable, but their traditional families were entirely unready to accept the union.
Undeterred, they chose love over convention. Instead of a grand, crowded Indian wedding, they exchanged vows in a strikingly simple registered ceremony on Vasant Panchami in February 1984. Neither Savita’s nor Rajiv’s parents were present. Only a handful of friends attended, including Sitaram, the beloved MGIMS artist, who stood as a quiet, steadfast witness to their commitment.
Acceptance came slowly, but when it finally arrived, it was complete. Over time, their families fully embraced the marriage, showering the couple with a love that eventually bound them all together. For seven years, Savita continued to use her maiden name, Dawande. It wasn’t until August 1991 that she formally changed it to Borle—marking not just a legal transition, but a quiet, loving affirmation of the life she had successfully built with Rajiv.
Savita’s introduction to Sevagram happened years before she ever held a dental drill. When her father served as the RMO at the Wardha District Hospital, Sevagram’s senior doctors—titans like Dr. O.P. Gupta and Dr. Ravindra Narang—frequently visited. She watched them work, listened to their intense clinical conversations, and quietly absorbed the atmosphere of medicine.
After earning her BDS, she returned to Wardha and accompanied her father on a visit to Dr. Gupta. Over a simple cup of tea, the formidable physician casually inquired about her career plans. She admitted she had none set in stone. Without a moment of hesitation, Dr. Gupta made the choice for her. "Join as a house officer in dental surgery at MGIMS," he instructed.
With that simple suggestion, Savita stepped into Sevagram’s medical world. It was a bond that would endure for thirty-five years.
She served as a House Officer from November 1982 to April 1984, then as a Registrar until 1986. She slowly climbed the modest rungs available to her, becoming an Assistant Lecturer a decade later, and finally a Lecturer in August 2004. Unlike most dentists who came to Sevagram, stayed briefly to gain experience, and quickly left for lucrative city practices, Savita remained. She became the quiet anchor witnessing the entire evolution of the dental department firsthand.
The early years were grueling. She lived in the modest, no-frills Dharmananda Nursing Hostel, where duty strictly took precedence over comfort. Working under Dr. K.K. Hariharan, Dr. Shyam Singh, and Dr. Ashok Pakhan, the days were punishingly long, the patients were endless, and the resources were painfully scarce. Savita worked quietly and efficiently. No complaints. No demands.
At one critical juncture, she had an opportunity to pursue postgraduate studies in oral pathology at Nagpur. But by then, Rajiv’s practice had taken deep root, and their young son, Firoze, was still in school. She chose to stay. It was a silent decision, made entirely out of love, and carried without a single ounce of regret.
She was always draped in a sari. Slightly short, moving with an unhurried grace, she never actively sought attention yet was completely impossible to overlook. Her large, expressive eyes carried both warmth and wit. She spoke flawless Marathi to absolutely everyone—the patients in pain, the senior professors, the technicians, and the security guards at the gate. Hierarchy held zero weight with her.
Beyond the sterile walls of the dental clinic, her life was a vibrant, sensory masterpiece.
A voracious reader, she had an uncanny ability to find books wherever she went, raiding the libraries of Sevagram, Sawangi, and Wardha. Marathi literature was her sanctuary. But she didn’t just read; she actively shared. Books flowed constantly from her hands to her friends and children, each gift carefully chosen as a quiet invitation into the stories she cherished.
Her kitchen was a place of equal magic. The sizzle of spices, the rhythmic chopping, the warm aromas curling through the air—she moved through her kitchen with the grace of a conductor leading a silent symphony. Guests never left her home hungry. For Dr. Borle, cooking wasn’t just about food; it was her primary love language, spoken fluently in every carefully prepared dish.
Perhaps the most beautiful irony of her life was her relationship with animals. As a child, she would freeze in pure terror at the sight of a stray dog, instinctively clutching someone's arm for safety. Yet, years later, those exact same hands gently scratched behind floppy ears and stroked wagging tails. Her Sevagram home eventually filled with half a dozen massive dogs—a Labrador, a Golden Retriever, a German Shepherd, a Doberman, a Great Dane. Mornings began with eager paws tapping at her doorstep; evenings closed with a chorus of joyful barks. She welcomed them all, whispering their names like a mother calling her children home.
Illness came quietly, and entirely without warning: metastatic thyroid carcinoma.
The brutal disease took a heavy physical toll, but it never once touched her spirit. She endured the grueling treatments with staggering grace. Her trademark smile remained completely unchanged; her deep kindness was totally undiminished.
On October 30, 2015, at the age of fifty-four, she passed away.
Her son, Firoze, carries her deep medical legacy forward as a plastic surgeon at Jawaharlal Nehru Medical College in Sawangi. But Savita was never just a dentist, just a mother, or just a spouse. She was the steady ground beneath the feet of everyone who knew her. In the bustling corridors of the hospital, in the hushed, affectionate exchanges between her colleagues, and in the gentle confidence of the rural patients who once sat in her creaky dental chair, her spirit lingers.
She never asked for more than she was given. She never wished for what she did not have. She simply lived fully, loved deeply, and showed an entire campus the quiet, staggering power of an ego that never was
| 1960 | Born, 21 November, Daryapur — father Dr. Markand Dawande, GMC Nagpur first batch; grandfather also a doctor |
| 1971 | Family moved to Wardha — father RMO, Wardha District Hospital; first encounters with MGIMS doctors |
| 1977 | Joined Government Dental College, Nagpur — at father’s behest after admission upgraded from physiotherapy |
| 1982 | Joined MGIMS, 1 November — House Officer in Dental Surgery; Dr. O.P. Gupta’s casual suggestion over tea |
| 1984 | Married Rajiv Borle, Vasant Panchami — registered ceremony; only a handful of friends present including artist Sitaram |
| 1986 | Completed Registrar tenure — continued as Assistant Lecturer |
| 1991 | Formally changed name from Dawande to Borle, August |
| 2004 | Promoted Lecturer in Dental Surgery, August |
| 2015 | Died, 30 October — metastatic thyroid carcinoma; aged fifty-four; thirty-three years at MGIMS |
Dr. Subhash Chandra Ahuja
MS Orthopaedics, GSVM Medical College Kanpur (1969)
Professor & Head of Orthopaedics · Deputy Medical Superintendent · Eight Years at Sevagram · The Whim That Was Well-Placed
Subhash Chandra Ahuja was born on March 6, 1943, in Multan — then Punjab, now Pakistan. Multan carries its own associations in the Indian cricketing imagination as the city where Virender Sehwag made his triple century in 2004; it carries a different kind of historical weight in the story of MGIMS, as the city where Dr. Sushila Nayar was present on January 30, 1948, investigating whether Hindus and Sikhs were facing threats in the region — the very day Mahatma Gandhi was assassinated in Delhi. After Partition, the Ahuja family resettled in Kanpur, as many Punjabi families did, beginning again with the particular determination of displacement.
His father, Dr. Suraj Lal Ahuja, was a homoeopath. Subhash attended BNSD College in Kanpur and completed his high school in 1959, then entered G.S.V.M. Medical College, completing his MBBS between 1960 and 1965 with four gold and two silver medals. He completed his MS in Orthopaedics between 1967 and 1969, refined his skills at Willingdon Hospital, Delhi, and then spent nearly two years at Christian Medical College, Vellore — from July 1971 to April 1973 — before the morning newspaper and the Sevagram advertisement changed the trajectory of everything.
He arrived on September 1, 1973, with his wife, a paediatrician — another of Dr. Nayar's paired appointments, two specialists contributing to two departments, each one's presence anchoring the other.
Dr. A.N. Damle had worked in Orthopaedics for two years before Dr. Ahuja's arrival and had left a month earlier, which meant the department was without leadership at the moment of transition. Six months after his arrival, Dr. R. Bhalla joined from Willingdon Hospital, and together they nurtured what they had.
The unit began with thirty beds — twenty in Kasturba Hospital and ten in the Civil Hospital, Wardha. But Dr. Ahuja understood from the beginning that Orthopaedics at a rural teaching hospital serving the villages of Vidarbha was not merely a department that managed fractures and dislocations. He established a weekly Hand Clinic and a Polio Clinic at Kasturba Hospital. He set up a Leprosy Surgical Clinic at the Gandhi Memorial Leprosy Foundation in Wardha. Fortnightly, he travelled to Deoli and Pulgaon to ensure that orthopaedic care reached patients who could not travel to Sevagram. He had come on a whim and was staying with a purpose that had nothing casual about it.
In September 1975, he took up a government-approved deputation to Abadan, Iran. The department he left behind — handed to Dr. R.K. Belsare with only house surgeons and a three-hour weekly visit from Dr. Vikram Marwah — was inadequately covered for the workload it was carrying.
The crisis compounded. Dr. V.N. Chaturvedi left on December 29, 1975. His wife, a Paediatrics lecturer, was also preparing to leave. The departure of both Mrs. Ahuja from Paediatrics and Mrs. Chaturvedi created a specific staffing emergency. Dr. Nayar wrote to Dr. Ahuja in September 1976 urging him not to extend his stay in Iran. Her letter was, at its core, a request to come home and continue what had been started. Dr. Ahuja returned on December 1, 1977.
By the time he was back, Dr. S.A. Farooq had joined as Lecturer. The trio of Dr. Ahuja as Associate Professor, Dr. Belsare as Reader, and Dr. Farooq ran a department whose outpatient numbers had crossed six thousand annually, with major surgeries approaching three hundred per year. In 1980, the department recorded 1,458 admissions — managed by three doctors across thirty inpatient beds.
He became Deputy Medical Superintendent in 1979. Promotions at MGIMS were slow, and teachers remained in the same post for years regardless of performance. Dr. Ahuja applied for a professorship in Maharashtra's government medical colleges, was selected, and received a posting to Ambajogai. He returned to Sevagram with that government order in hand, and the demonstration of external recognition secured his professorship at MGIMS. It was not the most graceful path to a title that should have been his by natural progression, but it was the path available.
On February 6, 1981, after nearly eight years across two tenures, Dr. Ahuja left MGIMS. He joined Christian Medical College, Ludhiana on the Monday following his departure — not a single day's break in service. He rose to become Principal of CMC Ludhiana, serving four years before retirement.
The department he left behind had fewer than ten research publications across its first decade — a modest academic output by the standards of the institutions where he had trained. But the measure of what he built was not in papers. It was in the outpatient numbers that had grown year by year, in the hand clinic and the polio clinic, in the leprosy surgical rehabilitation that brought reconstructive surgery to patients in Wardha who had no other option, in the fortnightly trips to Deoli and Pulgaon in an era when most orthopaedic surgeons with his credentials were in cities.
He had found the advertisement in The Hindu on a morning he might have missed it, applied on a whim, and exchanged a glance worth eight years of building.
| 1943 | Born, 6 March, Multan — family resettled in Kanpur after Partition |
| 1960 | Entered GSVM Medical College, Kanpur |
| 1965 | Completed MBBS — four gold medals, two silver medals |
| 1969 | Completed MS Orthopaedics — refined skills at Willingdon Hospital, Delhi |
| 1971 | Christian Medical College, Vellore — until April 1973 |
| 1973 | Arrived MGIMS, 1 September — spotted advertisement in The Hindu, applied on a whim |
| 1973 | Established Hand Clinic and Polio Clinic, Kasturba Hospital · Leprosy Surgical Clinic, GMLF Wardha · fortnightly outreach Deoli and Pulgaon |
| 1975 | Deputation to Abadan, Iran, September — government-approved |
| 1976 | Dr. Nayar wrote urging return — staffing crisis, vision to be restored |
| 1977 | Returned MGIMS, 1 December — Associate Professor |
| 1979 | Appointed Deputy Medical Superintendent |
| 1980 | Department recorded 1,458 admissions — three doctors, thirty beds |
| 1981 | Left MGIMS, 6 February — joined Christian Medical College, Ludhiana the following Monday |
| 1981 | Rose to Principal, CMC Ludhiana — served four years before retirement |
Dr. Kush Kumar
MS Orthopaedics, Institute of Medical Sciences Varanasi (1976)

Kush Kumar was born on August 8, 1950, in Nainital, his parents Gopal Narayan and Maheshwari Srivastava carrying the gentleness the hills of that city are associated with. He entered King George Medical College, Lucknow, in 1966 — one of India's oldest and most prestigious medical institutions — and graduated MBBS in 1971. Orthopaedics drew him with the particular pull of a specialty that combines mechanical precision with restorative purpose: bones that had broken could be set and healed; deformities that had limited a person's movement and dignity could be corrected. He pursued his MS in Orthopaedics at the Institute of Medical Sciences, Varanasi, under the renowned Dr. Tuli, completing in 1976.
He joined MGIMS on May 8, 1976, as Lecturer in Orthopaedics — his first posting, the ink barely dry on his MS degree. He was twenty-five years old and arrived into a department in flux, Dr. Ahuja away on deputation to Iran, Dr. Belsare managing what he could. His first tenure ended in December 1977 when he left for Iran — following, in reverse sequence, the path Dr. Ahuja had taken.
He returned to MGIMS on November 10, 1982, joining as Reader in Orthopaedics and taking charge as department head following the sequential departures of Dr. Ahuja, Dr. Belsare, and Dr. Farooq. The department he inherited had been through a period of sustained instability — three heads in the space of two years, a workload that had reached 1,458 admissions annually managed by a skeleton team. Stability was the first requirement; expansion was what followed.
In the operating theatre, he brought the exquisite technique that Dr. Chauhan would remember across decades. His photographic memory made him a resource not just in the clinical domain but in the educational one — able to cite the relevant textbook passage, locate the applicable anatomy, recall the published series that informed a particular surgical decision. He emphasised to his postgraduates the primacy of normal anatomy. "You cannot discern the abnormal without a thorough understanding of the normal." On written communication, he was uncompromising: "You can never become a good orthopaedician if you can't write perfect English."
He illustrated his publications by hand — the same hand that manipulated tissues in the operating theatre producing the diagrams that explained what that manipulation had achieved. His research focused on deformities of the hand and spine, fracture repair, and bone plating. In January 1987, having built the department into something substantially more stable than what he had inherited, he left for Karad and the Krishna Institute of Medical Sciences.
From Karad, the trajectory became genuinely extraordinary. He served as consultant to the Ministry of Health in Saudi Arabia, then joined the University of Medical Sciences in Kuwait. He served as Dean at PVNR Medical College in Dehradun, then flew across continents to the University of the West Indies in Trinidad and Tobago for four years. He visited Malawi with Rotary International, worked in Zimbabwe, carrying across all of these the same steady hands and the same commitment to a medicine that respected the dignity of each patient.
In 2000, he and his wife Dr. Vibha Kumar made the most audacious decision of their career together: they migrated to the United States, well into middle age, and began again. "Those years were marked by immense challenges," Dr. Vibha Kumar said. "We went to the USA well beyond middle age. We had to start over — write exams, train again, and prove ourselves in a competitive system. It was perseverance and hard work that carried us through."
He completed three orthopaedic fellowships and then pursued a residency in nuclear medicine at Emory University, where he won the Outstanding Resident Researcher Award. The pivot from orthopaedics to nuclear medicine was not random — his research focus was rooted in orthopaedic applications, particularly the early detection of bone infections and the identification of culprit vertebrae for kyphoplasty. He became Chief of the Radiology Department at the Carl Vinson VA Medical Center in Dublin, Georgia. Eighty publications. Seven book chapters. One book under consideration at the time of his death. Each article illustrated, where appropriate, with his own hand-drawn diagrams.
He had loved cricket, chess, and cards. He had attended kavi sammelans and mushairas, finding in poetry the same elegance and discipline that marked his professional life. In his later years, glioblastoma — aggressive, relentless, ultimately unanswerable — depleted his strength. He underwent chemotherapy and radiation. He died on May 24, 2019, aged sixty-eight.
His former trainee Dr. Vijendra Chauhan, who had watched him operate and called it an art form, had recorded the tribute that now stands as the most complete summary of what he was: extraordinary photographic memory, exquisite dissections, gifted orator, unique illustrator, visionary whose far-sightedness was not always fully appreciated. The institutions that failed to fully appreciate the vision were not the whole of the record. They were the beginning of it.
| 1950 | Born, 8 August, Nainital — parents Gopal Narayan and Maheshwari Srivastava |
| 1966 | Entered King George Medical College, Lucknow |
| 1971 | Completed MBBS |
| 1976 | Completed MS Orthopaedics under Dr. Tuli, IMS Varanasi |
| 1976 | Joined MGIMS, 8 May — Lecturer in Orthopaedics; aged twenty-five |
| 1977 | Left for Iran, December — following the international opportunity that era regularly offered Indian surgeons |
| 1979 | Married Dr. Vibha Kumar, October — Lady Hardinge Medical College graduate |
| 1982 | Returned MGIMS, 10 November — Reader and Head of Orthopaedics |
| 1986 | Wife Dr. Vibha Kumar completed MD Community Medicine, MGIMS |
| 1987 | Left MGIMS, 17 January — joined Krishna Institute of Medical Sciences, Karad |
| 1988 | Completed PhD in Orthopaedics |
| 1990 | Visited Malawi with Rotary International · worked in Zimbabwe |
| 1990 | Consultant, Ministry of Health, Saudi Arabia · University of Medical Sciences, Kuwait |
| 1995 | Dean and Professor, PVNR Medical College, Dehradun |
| 1996 | University of the West Indies, Trinidad and Tobago — St. Augustine and Mount Hope Hospital, four years |
| 2000 | Migrated to USA — sat USMLE, retrained, completed three orthopaedic fellowships |
| 2000 | Residency in Nuclear Medicine, Emory University — Outstanding Resident Researcher Award |
| 2000 | Chief of Radiology, Carl Vinson VA Medical Center, Dublin, Georgia |
| 2019 | Died, 24 May — glioblastoma; aged sixty-eight |
Comparative analysis of tissue effect of dexamethasone and colchicine following intra-articular injection : an experimental study
Histological study of human Intervertebral dice of normal abnormal embryos and fetuses
Evaluation of fibro-osseous tunnel pressure in human beings health diseases
Experimental production of articular tuberculosis in laboratory animals
Medial open wedge high tibial osteotomy
Dr. Kisan Rajaram Patond
MS Orthopaedics, Government Medical College Nagpur (1983)

Kisan Rajaram Patond was born on February 26, 1956, in Sasti, a village thirty-five kilometres south of Akola. His father was a small farmer with four years of schooling. His mother had no formal education. He completed his primary education in Marathi at Shri S.L. Shinde Vidyalaya in Sarsi, moved to RLT College, Akola, and in 1974 secured admission to Government Medical College, Nagpur.
He is not entirely sure, looking back, why he chose medicine. "I chose science on my own, scored well, applied to medical college, and got in. My parents had no clue about the process or what it meant." The honest uncertainty of that answer is more revealing than a polished narrative would be — a village boy who applied the same methodical effort to each step that presented itself, without the guidance or the social capital that shaped the choices of those who came from medical families or urban professional households.
He graduated MBBS in 1978, winning the Shri D.V. Bhiwapurkar Prize for top rank in the Final MBBS Examination at Nagpur University. He pursued his MS in Orthopaedics at GMC Nagpur under Dr. N.K. Saxena — whose dissection techniques he would describe decades later with the reverence of someone describing a formative aesthetic experience: "Precise, detailed, like an artist carefully sculpting a masterpiece." His MS thesis examined how electrical stimulation could accelerate bone healing. He completed the degree in March 1983 and moved progressively through Lecturer and Reader posts at GMC and IGMC Nagpur before Dr. Vikram Marwah's advice at a conference changed the trajectory.
Badi Behenji made up her mind within minutes. Dr. Patond had arrived at Prerna Kutir with a letter of recommendation and a solid track record. He was shy and reserved — not the kind of person who could walk into a room and promote himself with confident ease. The conversation was brief. Dr. Sushila Nayar saw what she needed to see and told him she wanted him to join the next day.
He had to serve a month's notice at IGMC Nagpur or lose a month's salary. He thought about it briefly, then made a decision uncharacteristic for someone usually cautious: he forfeited the month's salary, packed his bags, and came to Sevagram. He arrived on February 19, 1988, into a department that had been without a permanent head since Dr. Kush Kumar's departure the previous year. He was appointed Professor in April 1990 — two years after joining, considerably faster than the government college trajectory would have allowed.
When he arrived, he went through the old departmental records as a way of understanding what he had inherited. Dr. Ahuja's legacy emerged from those records: the hand clinic and polio clinic, the leprosy surgical clinic at the Gandhi Memorial Leprosy Foundation, the fortnightly outreach to Deoli and Pulgaon, the postgraduate programme launched in 1980. "I couldn't help but feel inspired," Dr. Patond said. "I saw the incredible impact Dr. Ahuja had made and felt a surge of motivation to carry the torch forward."
His discipline was expressed most visibly in the OPD, which opened at 8 a.m. without exception. He mentored thirty-eight MS students between 1989 and 2016, and twenty-five diploma students. His first postgraduate student, Dr. Sudhir Srivastava, went on to lead the Orthopaedic Surgery department at KEM, Mumbai.
His clinical focus shifted over time toward joint replacement — hip, knee, shoulder, elbow replacements became his primary work, the particular reward of watching patients who had lived with chronic pain and limited mobility walk out restored. "That feeling of making a difference never fades." His reconstructive surgery expertise in leprosy earned him a fellowship from the National Academy of Medical Sciences of India.
A paper presented at a conference in Hong Kong caught the attention of an expert who would sit years later on an interview panel for a UAE position. The expert remembered the work, remembered the name. "Sometimes," Dr. Patond reflected, "hard work pays off in ways you least expect."
He served as Medical Superintendent from October 2007 to August 2009, and as Dean from August 2009 to June 2014. He was not the figure who strode into a room and commanded it. He was the figure who arrived, watched, understood, and then acted — decoding bureaucratic language, reading what official documents said and what they did not, understanding the unspoken rules before applying the formal ones.
His one non-negotiable was Marathi. In the OPD, the wards, the operating theatre — conversations happened in Marathi. It was not a statement of regional identity. It was a clinical conviction: doctors working in rural Vidarbha needed to speak the language their patients thought in, not the language their degrees were written in. From August 2009 to 2012, he worked at Gulf Medical College in Ajman, UAE — broadening his perspective and putting his work in front of people he had not previously met.
His wife retired as headmistress of New English High School in Wardha. Their son Swapnil, a 2002 MGIMS alumnus, completed his MD in Forensic Medicine from the same institution and serves as Professor and Head of Department at Rajendra Gode Medical College, Amravati — the first doctor from Sasti's son producing the next generation of the medical line.
Dr. Patond continues to see patients, take ward rounds, and perform joint replacements. He cycles through Sevagram each morning with a walking stick in hand to ward off stray dogs — a detail that captures, with the precision of a good X-ray, the quality of a man who combines dedication with pragmatism and has never needed the life to be grander than it is to find it worth living.
He was told by Badi Behenji to come the next day. He forfeited a month's salary to do so. That was 1988. The village boy who did not know why he chose medicine has spent more than thirty-five years demonstrating that the choice was the right one.
| 1956 | Born, 26 February, Sasti, Akola district — father a small farmer with four years of schooling; mother with none |
| 1974 | Admitted to Government Medical College, Nagpur |
| 1978 | Completed MBBS — Shri D.V. Bhiwapurkar Prize for top rank, Final MBBS, Nagpur University 1979 |
| 1983 | Completed MS Orthopaedics under Dr. N.K. Saxena, GMC Nagpur — thesis on electrical stimulation in bone healing |
| 1983 | Lecturer, GMC Nagpur — then Reader and unit head, IGMC Nagpur |
| 1988 | Met Dr. Sushila Nayar at Prerna Kutir — appointed on the spot; forfeited month’s salary; arrived 19 February |
| 1990 | Promoted Professor, April — two years after joining |
| 2007 | Medical Superintendent, October — until August 2009 |
| 2009 | Dean, August — until June 2014 |
| 2009 | Gulf Medical College, Ajman, UAE — until 2012 |
| 2016 | Fellowship, National Academy of Medical Sciences of India — reconstructive surgery in leprosy |
| 2026 | Continues — ward rounds, OPD, joint replacements, bicycle through Sevagram each morning |
Closed intramedullary nailing in displaced fracture shaft of tibia with early weight bearing
Fracture healing under simple external fixator : an experimental study in rabbits
Immunodiagnosis of osteoarticular tuberculosis by ELISA
Clinico radiological evaluation of osteoarthritis of knee intraosseous pressure measurement study in proximal tibial metaphysis
Synovial-fluid analysis in knee disorders
Retrospective study of giant cell tumors of bone
Correlation of arthroscopic clinical diagnosis in disorders of knee joint
Study of post polio residual paralysis around ankle and foot
Fenestration surgery in lumbar disc and canal stenosis
Surgical treatment of flail knee after poliomyelitis
Medial open wedge high tibial osteotomy using bone cement spacer block
Posterior tibial neurovascular decompression in plantar ulcer of leprosy
Ganglion around wrist
Claw hand correction by the lasso procedure in leprosy
Spectrum of orthopedic surgical procedures at MGIMS Sevagram (1990 – 1996)
Thumb deformity correction in leprosy patients
Metaphyseal trabeculectomy of the proximal tibia in early osteoarthritis of the knee
Compartment pressure measurement in closed fractures of leg bones and its correlation and it Z0s correlation with the clinical parameters
Spectrum of congenital Orthopaedics anomalies in the dept. Of Orthopaedics MGIMS Sevagram
Uses of ethylene oxide sterilized allografts in Orthopaedics
Use of pedicle flaps for wound coverage in upper and lower limbs
Arthroscopic lavage in early osteoarthritis of knee joint
Treatment of elbow disorders using sloppy hinge prosthesis
Anterior fusion in Pott’s spine
Closed intramedullary nailing in treatment of displaced diaphyseal fractures of radius and ulna in adults
Acute pyogenic arthritis knee efficacy of open arthrotomy and closed suction irrigation
User of local steroid with 2% xylocaine in tennis elbow
Bipolar arthroplasty in non-infective hip arthritis
Bacteriology of wound contamination in compound fractures at the time of admission
Histopathology of interface tissue retrieved at the time of implant removal
Management of displaced diaphyseal fractures of femur in children with intramedullary kirschner’s wires.
Anterior cervical discectomy and fusion
Intramedullary interlocking in closed tibial fractures
Open door cervical laminoplasty in patients with multilevel cervical spondylotic myeloradiculopathy
Open Door Laminoplasty in Multilevel Cervical Spondylotic Canal Stenosis with Myeloradiculopathy
Primary Plate Fixation of Completely Displaced Midshaft Clavicular Fractures in Active Adults.
Evaluation of intra-articular hyaluronic acid injection in primary osteoarthritis of knee
Bone mineral densitometry in traumatic distal end radius fractures
Epidural steroid injection in managing chronic low back pain
Functional outcome of open reduction and internal fixation of fracture proximal humerus with proximal humerus internal locking osteosynthesis (PHILOS) plate
Epidural steroid in management of chronic low back pain
Epidural steroid in management of chronic low backache
Bone mineral density in traumatic distal end radius fracture
Functional outcome of open reduction and internal fixation of fracture proximal humerus with proximal humeral internal locking osteosynthesis (PHILOS) plate
Open reduction and internal fixation of fracture clavicle treated with pre-contoured clavicle plate
Hospital-based cross-sectional study of osteoporosis in men with proximal femur fracture by peripheral DEXA
Open reduction internal fixation of displaced bicondylar fracture tibia: plating on one side and cannulated CC screws on the other side
Dr. Naresh Kumar Dhaniwala
MS Orthopaedics, Institute of Medical Sciences BHU Varanasi (1987)

Naresh Kumar Dhaniwala was born on November 30, 1957, in Bhagalpur, Bihar — a city of silk and shadows, known for its exquisite tussar silk and bearing the dark legacy of the 1980 Bhagalpur blindings. His father ran a cloth shop and later acquired an agency for Bombay Dyeing. Among seven siblings, Naresh was the third.
His educational journey began at Netarhat Residential School, one of the country's most prestigious institutions, nestled in the forests of what was then Bihar. Admission was fiercely competitive — only sixty students selected annually from across the state. A lawyer customer of his father, whose son attended the school, recommended Naresh. The nearly free education provided at Netarhat broke down financial barriers. Living in an ashram-like setting, wearing simple khadi, embracing Gandhian values — he learned self-reliance, patience, and the quiet strength that would carry him through everything that followed.
Despite his best efforts, Naresh failed to secure medical admission on his first attempt — including to MGIMS. He spent a gap year at BHU, then secured one of twenty-two open-category seats at JIPMER Pondicherry. After a year, he transferred to IMS BHU, where he graduated MBBS with second rank in his final examinations. He chose Orthopaedics — medicine felt too theoretical, surgery too broad, but Orthopaedics combined the best of both. He pursued his MS under Prof. Dr. S.M. Tuli, an internationally recognised expert in bone tuberculosis, writing his thesis on congenital and post-infective dislocation of the hip in children.
With his MS degree, Naresh joined UP Health Services and was posted to Chitbara Gaon, Ghazipur district — a village with no roads, no electricity, and during monsoons, submerged in floodwaters. His first journey there required a five-mile walk from the nearest bus stop through muddy fields and narrow lanes. Snakebites and scorpion stings were common emergencies. Villagers still relied on age-old remedies and prayers.
The isolation wore him down. On a whim, he wrote to the Dean of MGIMS inquiring about vacancies. Around the same time, his mentor Dr. Tuli wrote a recommendation to Dr. Vikram Marwah, a visiting professor at MGIMS. He was called for interview in 1987 — the same interview where Dr. S.P. Kalantri appeared for a Reader's post in Medicine. Two candidates applied for the Orthopaedics post. Naresh was selected. On August 25, 1987, after a gruelling forty-hour journey, he arrived in Sevagram.
What struck him most on arrival was the absence of senior faculty. Dr. Kush Kumar had already left. The department had only one faculty member — Dr. Vijendra Chauhan, an MGIMS alumnus from the 1977 batch. Three postgraduate students were present: Anil Lokhande, Sanjay Marwah, and Sanjay Deshpande. Three months later, Dr. K.R. Patond joined as Professor and Head, bringing much-needed direction.
Orthopaedic care in the late 1980s was undergoing transition. Polio, tuberculosis, and leprosy were still prevalent — he personally corrected many deformed hands and feet caused by leprosy. Fractures were treated with plaster casts and skeletal traction. There were no CT scans, no MRIs, no C-arms, no arthroplasty, no arthroscopy. "We relied on clinical acumen and traditional methods, which, though effective, lacked the technological precision of today."
Years passed, but frustration brewed. Promotions were scarce. He requested an independent unit; the plea was denied. He cleared the MPSC examination and in December 1991 joined Dr. Vaishampayan Memorial Government Medical College. By June 1993, he moved to Nanded, where he dedicated seventeen years to orthopaedic surgery.
In North India, people identify themselves by their first name alone. In Maharashtra, bureaucratic norms require the full name — first, middle, and last. Thus Naresh Kumar, who had never used a surname in Uttar Pradesh and Bihar, became Dr. Dhaniwala in Maharashtra.
In 2015, after nearly three decades in government service, he opted for voluntary retirement and joined Jawaharlal Nehru Medical College, Sawangi, where he has served as orthopaedic surgeon and educator for a decade. His wife Sangeeta — from Shillong, a gifted dancer, singer, and actress — adapted seamlessly to Maharashtra's arid landscapes, learning new languages and acquiring new skills. In March 2023, she published her first story collection, यादों की संदूकची. She now trains children in dance and music in Nanded.
Although Naresh lived in Sevagram for just over four years, he left an enduring imprint. The friendships forged there — with Drs. S.P. Kalantri, Ramji Singh, Mukesh Agrawal, S.K.T. Jain, Naresh Tyagi, and Deepak Mendiratta — remain cherished across the decades. Born in Bihar, educated in Jharkhand, trained in Tamil Nadu and Uttar Pradesh, employed across Maharashtra, married to a woman from Meghalaya — he adapted to each place with remarkable ease. Three times he considered private practice. Each time, fate gently steered him back to institutional service.
| 1957 | Born, 30 November, Bhagalpur, Bihar — third of seven siblings; father in cloth trade |
| 1967 | Admitted to Netarhat Residential School, Bihar — one of sixty students selected statewide annually |
| 1974 | Completed Class 10, Netarhat |
| 1976 | Completed Intermediate, Netarhat — gap year at BHU before medical admission |
| 1977 | Entered JIPMER Pondicherry — transferred to IMS BHU after one year |
| 1983 | Completed MBBS, IMS BHU — second rank in final examinations |
| 1984 | Enrolled MS Orthopaedics, IMS BHU — under Prof. Dr. S.M. Tuli; thesis on congenital and post-infective hip dislocation in children |
| 1985 | Married Sangeeta from Meghalaya |
| 1986 | Son Mrigank Mauli born, November — two months before MS final examinations |
| 1987 | Completed MS · posted UP Health Services, Chitbara Gaon, Ghazipur — no roads, no electricity, monsoon flooding |
| 1987 | Joined MGIMS, 25 August — Lecturer in Orthopaedics; 40-hour journey from Ghazipur |
| 1990 | Son Mukund born |
| 1991 | Left MGIMS, 12 December — joined Dr. Vaishampayan Memorial Government Medical College via MPSC |
| 1993 | Moved to Nanded — served 17 years in orthopaedic surgery |
| 2015 | Voluntary retirement from government service after nearly three decades |
| 2015 | Joined Jawaharlal Nehru Medical College, Sawangi — orthopaedic surgeon and educator |
| 2018 | Son Mukund became orthopaedic surgeon — following his father’s path |
| 2023 | Wife Sangeeta published first story collection — यादों की संदूकची |
Architects of MGIMS
Dr. S. P. Kalantri
MGIMS, Sevagram, Wardha
books.kalantri.co.in