Introduction
T
his is not a book about medicine, though medicine runs through every page. It is not a book about rural India, though Sevagram — Gandhi’s village — is its setting. It is, finally, a book about choices: the small accidents that begin a life and the larger decisions that quietly shape it.
I did not set out to write a memoir. For years, the idea felt unnecessary, even faintly vain. My days were spent inside a rural hospital, looking after patients who would never make headlines. What story could that possibly hold? But colleagues, students, and friends kept telling me to write before the details blurred and the people disappeared. I resisted for a long time. Then, one day, I began.
What follows is the story of a middle-class boy who drifted into medicine, arrived in Sevagram on a salary of ₹650 a month, and never quite left. I came with more enthusiasm than skill. I stayed because the work mattered. Along the way I learned medicine, unlearned certainties, made mistakes, changed my mind, and tried again. I have written about the failures as honestly as the successes.
The book moves through thirteen parts. It begins with my birth, my childhood, my school days, a brief and forgettable year in a science college, and then nine formative years at Government Medical College, Nagpur, where I acquired an MBBS degree, an MD in Medicine, and a lifelong respect for teachers who demanded more than textbook answers.
From there, the story shifts to Sevagram in the summer of 1982. I arrived as a young doctor expecting to stay briefly and somehow never left. The later chapters describe my innings as a teacher, physician, researcher, and administrator at the Mahatma Gandhi Institute of Medical Sciences. They include some of the work that mattered most to me: separating medical education from the influence of the drug industry, helping build a hospital information system long before computers became fashionable, starting a palliative care service, designing hospital spaces, and teaching a style of medicine that valued evidence, restraint, and common sense.
The book is not only about hospitals and institutions. It is also about family. My parents, brothers and sisters, my marriage to Bhavana, our children, their schooling, their marriages, and the ordinary domestic life that unfolded alongside the demands of medicine all find a place here.
There are clinical puzzles, research studies, and ethical knots with no clean answers. There are malaria wards and snakebites, traditional healers and new machines, deaths we could not prevent and the occasional recovery that felt like grace. There are shortages of money, shortages of staff, shortages of common sense. There are bureaucratic tangles and the small absurdities that keep public institutions alive. Above all, there are people — students who arrived eager to change the world, colleagues who became friends, and villagers whose quiet resilience kept us going. Some names are changed, but the stories are true.
This is not a textbook or a policy manual. It offers no grand theory and very little advice. Nor is it a sermon. Poverty here is neither romantic nor picturesque. Rural India can be generous and cruel in the same hour. I have tried to show both.
If you are a young doctor, you may find an honest account of practising medicine where investigations are few and judgement matters most. If you work in public health, you may recognise how policies look on the ground, where a missing drug or a delayed decision can alter a life. If you are simply curious, you may meet a village and its hospital as they are, without embellishment.
Do not expect heroics. Most days in medicine are made of smaller acts: listening carefully, making the best decision with limited tools, admitting uncertainty, learning from errors. Medicine, in the end, is less about drama than about steady work done well.
The chapters move roughly in time, though each stands on its own. You may read them in order or wander. Some pages describe suffering and failure. I have not softened these, because medicine does not. Pain, too, is part of the truth.
Memory is unreliable. Conversations are reconstructed, motives interpreted, events filtered through my own lens. Wherever possible, I checked records and spoke to colleagues. Where I could not, I relied on recollection. I have tried to be fair — to others and to myself. If I appear occasionally foolish or wrong, it is because I often was.
Many stories remain untold: confidences that must stay private, wounds better left unopened. What is here is what could be told honestly.
This book exists because others insisted that it should. I stayed in Sevagram because my family accepted a modest life without complaint. I learned from patients who trusted me and students who challenged me. Whatever I gave this village, it returned more.
That, perhaps, is the only explanation I can offer for these pages — and for a life that began by accident and stayed by choice.
Sevagram, April 2026
SP Kalantri
Wardha, 1957
In February 2026, Bhavana and I travelled to Rajasthan — not as tourists, but as people looking for something older than memory. We were tracing our roots.
Among the things I discovered was the etymology of our surname. The name Kalantri is believed to derive from kalan — rooted in the Sanskrit and Hindi kaal (काल), that most profound of words, which carries within it the entire sweep of human existence. In Hindi, kaal unfolds across all three dimensions of time: bhootkal (भूतकाल) — the past, what has already been; vartamankal (वर्तमानकाल) — the present, this very moment; and bhavisykal (भविष्यकाल) — the future, what is yet to come. The suffix tri denotes a profession. Somewhere in the distant past, our ancestors were the people who kept time for others — who told the farmer when to sow, when to harvest, when the season had turned.
It is a meaning I find quietly fitting for a family that has spent generations in medicine. A physician, too, lives at the intersection of all three dimensions of kaal — reading the past of a patient's history, attending to the present of their suffering, and trying to shape the future of their survival.
Our great-great-grandfathers came from Phalodi, in the Marwad region of Rajasthan. Sometime in the last 150 years — the exact decade unknown, the reason unrecorded — they left the desert and came to Maharashtra. What brought them here, how they survived the journey, what they carried and what they left behind: none of this was ever spoken of at home. My father never told us where we came from. And I, absorbed in the forward motion of my own life, never thought to ask.
That silence is one of the reasons I am writing this memoir.
I have always envied those who can summon their earliest days with cinematic precision — the exact shade of a wall, the scent of a room long gone. My own beginnings resist such clarity. They survive only as a soft haze, stitched together from family hearsay and the occasional unreliable memory that surfaced years later.
I made my entry at 6:26 in the morning on Thursday, August 15, 1957. It was India's tenth Independence Day. While a thirteen-year-old Bobby Fischer was busy unsettling chess masters halfway across the world and the silver screens glowed with Mother India, I arrived quietly in Wardha. I never mistook this coincidence for grand symbolism. It felt simply like a private signal from fate — gently tethering my life to the country's celebration before either of us knew what we were celebrating.
I was the last of six children born to Parvati and Gokuldas. My mother, married at fourteen after only four years of schooling, had filled our home with children by the time she was thirty-two. My father's formal education had ended at the seventh standard. Orphaned at three, he had started with nothing, drifting from his village to Wardha in 1932 in search of a foothold. Through sheer, stubborn duty — the kind that does not announce itself — he eventually rose to lead the local Bajaj group.
When I recently asked my eldest sister Asha — fifteen years my senior and possessed of the inconvenient gift of remembering everything — how exactly I was born, she answered as if she had been waiting decades for the question.
She reminded me of the old way.
The eldest siblings had been born in our grandmother's house in Barshi, amid ancestral walls and women who knew their business. The middle brigade and I, however, were born at home in Wardha. There were no hospital beds, no sterile green curtains, no nurses barking orders in a corridor. I was delivered by the local dai — a woman Asha spoke of with genuine respect. She was a professional without a degree, her authority derived from experience rather than textbooks.
It was a year that cared little for the precision of medicine. A pregnancy was not a project; it was simply a fact of life. There were no blood tests to fret over, no antenatal appointments to schedule, and certainly no ultrasounds to ruin the surprise. Halfway across the world, Virginia Apgar had recently designed her famous scoring system for newborns, but word of this medical revolution had not yet reached our doorstep. No one clipped a monitor to my toe or calculated my score with clinical solemnity.
I was just another cry in a house already full of them, held together by my mother's quiet, unacknowledged strength.
An hour after I arrived, India woke up. It was a morning of unfurled flags, long speeches, and the sticky sweetness of laddoos. My life began in that sliver of time between a personal cry and a national anthem — unscored, unmonitored, and blissfully unaware that a date, like a birthplace, is often just a matter of convenience.
The trouble began in June 1973.
I was desperate to enter Government Medical College, Nagpur, but I was eight months too young. The rule was rigid: you had to be seventeen. To a teenager, losing a whole year to a calendar felt less like a regulation and more like a personal injustice administered by the universe.
Fortunately, this was the pre-digital age. Long before Aadhaar cards and iron-clad databases, reality was negotiable. It was the golden age of administrative fiction, where inconvenient facts were quietly managed with a straight face and a modest fee. Half my generation seemed to have arrived on the first of July — a date neatly packaged for the school inspector. Even today, I notice on Facebook that twenty of my friends share a July 1st birthday. It is a grand collective victory of the pen over the womb.
In my case, a clerk at the Nagar Parishad performed a similar miracle. Fuelled, perhaps, by a few rupees, he backdated my birth to August 15, 1956, with a single stroke. Suddenly, I was eligible for medical school. I had also achieved a biological impossibility: on paper, I was now born three months before I had even been conceived.
That ink-stained lie made me the youngest student in my medical class. Decades later, it forced me into an early official retirement. In August 2021, I received a letter informing me that my regular service was over — because the records showed I was sixty-five, even though I was actually only sixty-four. I had entered medicine a year early, and now the rules insisted I leave a year early.
But I have not gone anywhere. The Institute graciously asked me to stay on as Emeritus Professor. I am still here in Sevagram, still working in the Department of Medicine. My official status in the register may have changed. My work with patients and students has not.
My birth chart was prepared by a well-known astrologer, Mr. Chimniram Shastri. After much mathematical squinting, he announced I was to be Devendra Kumar — a name destined for health, prosperity, and the world's respect. It was an impressive forecast. It lasted exactly until it met my father.
My father was a man unmoved by the stars. He listened to the astrologer politely, then set the horoscope aside the way one might set aside an old newspaper. What mattered to him was not the alignment of planets but the symmetry of sound. My elder brothers were Omprakash and Jaiprakash. It stood to reason that my name should join the family rhythm. He settled on Shriprakash. It pleased his ear, and in our house, that was reason enough.
Like many long Indian names, Shriprakash soon shrank to SP. Everyone used it — my wife, my colleagues, my siblings, eventually my patients. The name suits me: brief, efficient, and intimate. Only my mother softened it to YesPi — a tender twist she alone used, and which I have never heard from anyone else.
Today, Shriprakash exists only on paper — on mark sheets, licences, and tax returns. In the real world, I have always been SP. I sign my notes this way. Whether my father named me after Sri Prakasa, the famous parliamentarian, I never thought to ask him. Perhaps he did. It hardly matters. Two small letters became my identity, and an identity, once worn long enough, becomes the person.
At one, I had so little hair it became a matter of family concern. The few strands I possessed lay flat and silky, earning me the nickname Khrushchev from Professor Ramkrishna Vora, a neighbour with a keen eye for world affairs who saw a resemblance to the Soviet Premier's famous dome. My eyebrows were faint then and have not thickened much since. In short, I was a remarkably under-furnished child.
By four, politics gave way to mythology. My sisters still laugh remembering how I would demand a dhoti and a tilak to lead solemn pujas around the house. I informed my mother, Parvati, that she was merely a substitute — my real mother was the Goddess Parvati in the Himalayas. I devoured the Mahabharata and Ramayana with a passion that would eventually, gradually, and somewhat reluctantly, give way to anatomy textbooks.
Birthdays were quiet affairs in those days — no balloons, no candles, no midnight calls from friends. Yet they carried a weight that modern celebrations, for all their noise, rarely do. My mother followed her own ritual. She would wake me before dawn to rub a paste of turmeric and milk into my skin — a golden guard against ill fortune. She would dress me in a new shirt and shorts, fresh from Hedau Tailor, who ran a shop near Durga Talkies. He had an annual contract with our household. My father would hand him yards of cloth; Hedau would glance at us, estimate our size without a measuring tape, and return with shorts that were invariably oversized — optimistically stitched to fit next year's growth.
Then she would press a single homemade pedha into my hand — shaped with a small iron weight, the kind that sat permanently on the kitchen shelf, sweet and dense and smelling of cardamom. She never remembered her own birthday. No one ever celebrated it. Perhaps that is why she marked mine with such care, investing the day with a tenderness that required no audience and no applause.
My childhood unfolded across three houses, each marking a different chapter of growing up.
The first was a rented home in the Bajaj Electrical premises near Gandhi Chowk. Life there was spartan: no telephone, no scooter, no refrigerator. A flush toilet was a luxury we had only heard about. We lived, as most of Wardha lived, on the honest side of simplicity. That house was eventually flattened by a bulldozer, carrying away the bricks that held my earliest memories. Nothing remains of it now but what I can recall — and memory, as I have learned, is a selective and unreliable archivist.
From Gandhi Chowk, we moved to the Bachhraj Cotton Factory quarters, sandwiched between the bus stand and the railway station near Bajaj Square. The factory provided a constant soundtrack — the steady, mechanical clatter of ginning machines running through the day. The air was thick with the smell of raw cotton, and fine white fibres settled on everything: chairs, clothes, hair, the surface of a glass of water left out too long. Cotton seeds scattered across the floor made every step a minor adventure.
It was a noisy, textured, entirely alive sort of childhood.
In 1965, my father did something that caused a small stir in Wardha's drawing rooms: he bought a girls' school.
The Kesrimal Kanya Shala, built in 1936, had vacated its premises to relocate to a new campus on Nagpur Road near Shivaji Statue Square — where it still stands today. My father purchased the old building for forty-four thousand rupees. In those days, that sum invited raised eyebrows and long pauses.
He renamed it Jaishree Bhavan — an affectionate compound of Jaiprakash and Shriprakash, the two brothers whose names graced the gate. There is a pleasing irony in this: neither of the brothers for whom the house was named ended up owning it. In the family partition, decades later, the house went to our eldest brother, Ashok.
The geography of Jaishree Bhavan defined my adolescence. A simple hedge separated us from Mr. Lulay, the town's leading advocate, who owned a bustling chawl home to twenty-odd people. The open ground near his home served as the venue for the local RSS evening drills. I can still see myself there in ninth grade — standing in regulation khaki shorts and belt, reciting Namaste Sada Vatsale as the evening settled in around us.
To our right lived Dr. M.K. Pawar, whose son Sunil was my classmate. The intersection outside our gate was known as Wanjari Square, named after a humble cycle repair shop owner nearby. It is a small testament to the man's local standing that while the British names on the map have long since faded, his has endured. The square is still called Wanjari Square today.
Turning a school into a home is no simple matter. My father hired a Nagpur-based Padma Shri-winning architect, Mr. Shivdanmal, whose initial advice was blunt: demolish the thirty-three-year-old building entirely and start again. My father found the idea too radical and the cost too large. A compromise was struck. Shivdanmalji agreed to renovate the existing shell — coaxing a home out of a school with a patience that the building rewarded. The real foreman, however, was often my father himself, who was at the site daily, correcting measurements and questioning workers until the school shed its old skin. By the early 1970s, the house, with its generous porch, had become a subject of quiet admiration in the town.
We moved in during 1968. A year later, my brother Ashok brought home his seventeen-year-old bride, Kanta. She had passed her matriculation before the wedding, but my father insisted she continue her education. For the next three years, she attended Yeshwant Arts College, a mile away. On the days my father sent her to class in his Ambassador car, it was an event — a daughter-in-law being chauffeured to college was unusual enough in our town to rarely pass without comment.
My brother Ashok died on Christmas Eve, 2025. The house has outlived him, as it has outlived my parents.
I often think of the Zen tale of the monk who called a king's palace an inn. When the king took offence, the monk asked who had lived there before him. My father, the king replied, and his father before him. And where are they now? They are dead. The monk smiled. A place where people arrive, stay a while, and leave — what is it but an inn?
We call them permanent addresses. But we are all just guests.
In the end, the only address I truly carry is what I remember — and what remembers me.
The Friend I Still Remember
My education began not with a love for books, but with a visceral hatred for school. In the late 1950s, I was enrolled in the Jamnalal Bajaj Bal Mandir—a cluster of huts behind Maganwadi that looked more like a quiet backyard than a temple of learning.
Every morning, a tonga arrived with a clip-clop that sounded to me like a police escort. Other children climbed in with the resignation of the doomed; I treated it like a moving jail. I cried, I protested, and on two memorable occasions, I bit the poor tonga-wallah. Whatever the saintly Mirabai Mundra and Yamunatai Jajoo tried to teach me has long since evaporated. What remains is the memory of the art of refusal.
By age five, I was sent to the Nagar Parishad school. We went barefoot, hauling heavy cotton bags like laborers transporting grain. Inside, there were no benches. We sat on a thin mat—a dari—in neat, cramped rows where our entire world began and ended at the edge of that woven strip. Our teacher, Mr. Champalal Chaubey, ruled from a desk that served as his throne. When the room grew too cheerful, he would crack his palm against the wood, a sound that brought an immediate, clinical silence. On hot afternoons, he would stretch his legs across that same desk for a nap, leaving us to scratch at our slates while the King slept.
I was twelve before I finally mastered the bicycle—a sleek, shining creature I had previously only admired from a distance. My salvation was Sunil Pawar, a neighbor and classmate at Craddock High School. Sunil had mastered the "small push." He would hold the seat firmly as I wobbled like a newborn calf, running beside me until, without warning, he let go.
For a few seconds, I wouldn't realize I was moving on my own. The road would slide under me, the wind would rise, and I would feel a freedom that was both thrilling and terrifying. My landings were less poetic. I had a talent for collapsing in a heap with the machine, a scene Sunil watched with the tolerant amusement of an elder brother. Eventually, the bicycle became a habit. By medical college, I rode with the reckless confidence of the young and unhurt, taking corners with no hands on the bars, believing I was the king of Wardha’s quiet streets.
Sunil’s last decision was a "small push" of a different kind. Like his father and wife before him, he donated his body to the Anatomy department at Sevagram. In the same halls where I once learned the map of the human body, Sunil offered himself as the final lesson. He held the seat steady for the next generation of doctors, and then, at the right moment, he let go.
Years have a way of reversing our roles. I became a physician; Sunil returned to the earth, managing the family farm. Life was not gentle with him. He lost his son to a spinal tumour and his wife to a brain tumour — blows that leave a man quiet, even when he continues to smile.
In 2021, our childhood arrangement turned itself around. The boy who once held my bicycle seat now lay in a hospital bed, and I became his doctor. He was battling laryngeal cancer. A tracheostomy had taken his voice, but we spoke through signs and the steady understanding of a lifetime.
He did receive some radiation and a few cycles of chemotherapy, but decided against interventions that made his life difficult. He bought a new car, drove a thousand kilometres across Maharashtra, and was always smiling — even though he knew his days were numbered. I would often go to his home in Wardha and spend time with him. Having lost his voice, he communicated in sign language. I saw him the day before he passed away and could not meet his eyes. The next morning, the news arrived that he had died in the early hours.
Sunil had already directed that his body be donated to the anatomy department of our medical college, where students could learn human anatomy. He was not the first from his family to make this choice — his wife, who had died of a brain tumour fifteen years earlier, and his father, who had died of old age, had wished the same. When we took Sunil's body to the anatomy department, and it was filled with formalin and returned to its place among the preserved, a tinge of sadness enveloped me.
A part of the childhood memory was deleted.
The Library and the Lantern
My early world was bounded by the smell of old paper and the quiet authority of the Hindi Mandir Pustakalaya. This library sat on the Bajaj Electricals campus, near Durga Talkies. Inside, the librarian Mr. Madanlal Purohit reigned over rows of Hindi classics. At an age when other children were perhaps chasing hoops, I was chasing the prose of Mahadevi Verma, Bachchan, Prasad, and Nirala.
English had not yet invaded my small private world. I became an addict of the Hindi printed word, copying the flourishes of Acharya Chatursen in my school notebooks. The Rashtra Bhasha Prachar Samiti, founded by Jamnalal Bajaj, turned my hobby into a series of hurdles. I climbed the ladder of their examinations: Prathmik, Prarambhik, Pravesh, and Parichay. I remember taking the Kovid exam alongside my bhabhi — a shared family effort under the lamp. I might have reached the heights of Visharad or Sahitya Ratna, but science began to compete for my attention. Science eventually won the battle for my career, but Hindi kept the keys to my heart.
Every month, the arrival of Parag, Champak, and Nandan felt like a national holiday. These were not just magazines; they were windows out of our small town. Nandan brought the scent of Indian mythology, while Champak gave us animal fables that taught morals without the boredom of a sermon.
But the king of the shelf was Chandamama. Its pages were filled with sages, deities, and demons, all rendered in simple, translucent language. I spent hours lost in the Vikram and Vetal stories, fascinated by the king who never gave up and the ghost who never stopped asking riddles. It was a world where imagination was the only currency that mattered.
In middle school, Radhakrishnji Bajaj opened the doors of the Swaraj Bhandar library for me. It stood near the Sabzi Mandi — a place now so crowded you can barely park a scooter, but back then a quiet outpost of knowledge. When Radhakrishnji saw my hunger for books, he gave me an extraordinary open tab. I was told to take any book I liked, and he would foot the bill. I walked away with hundreds of volumes in Hindi and Marathi, reading them cover to cover.
By the time I reached medical college, my literary palate had expanded, but the addiction remained. Like all teenagers and medical students of that era, we developed a desperate interest in Debonair. At the time, it was edited by Vinod Mehta, who would later produce such sophisticated work as The Lucknow Boy. Back then, however, we were not reading it for the political commentary.
Procuring a copy was a feat of high-stakes espionage. None of us had the courage to simply walk up to a magazine vendor and ask for it. Only the bravest among us would volunteer. He would approach the stall, wait until no one was around, and whisper "Debonair" into the vendor's ear, then stand nonchalantly several feet away, keeping a sharp eye out for anyone who knew him.
Once the transaction was done, the magazine was quickly tucked inside a shirt, hidden against the skin until he reached the safety of the hostel. Back in the room, the door would be bolted. A single copy was often shared among three or four friends, hidden under a mattress when not in use. In our curiosity and our clumsiness, we were no different from teenagers anywhere else in the world.
The love for the printed word followed me even into the gruelling years of residency. Buried under the weight of Harrison's Principles of Internal Medicine, I found a secret sanctuary in comic strips.
Chacha Chaudhary was a favourite. He was a sprightly old man in a red turban whose brain was sharper than a needle and faster than a computer. When things got too heavy, his giant friend Sabu from Jupiter would provide the muscle. Even as a busy junior resident, I managed to find time for Pinki, the mischievous five-year-old created by Pran. I still have a vivid memory of being caught red-handed, tucked into a corner at my father-in-law's house, reading a Pinki comic instead of a medical journal.
Despite this vast internal world of stories and grand vocabulary, I remained a remarkably quiet child. By the time I entered medical college, I was too shy to string a single sentence together for my teachers or strangers. I was a tongue-tied boy — a creature of the library who had learned to think in the style of the classics but had not yet learned to speak to the world.
As my training progressed, the glossy pages of Sarika, Kadambini, Dharmyug, and Dinman gradually gave way to the Illustrated Weekly of India and the blunt, scotch-soaked wit of Khushwant Singh. I still remember the specific thrill of buying the inaugural copy of Sunday in May 1976. Edited by a young, sharp M.J. Akbar, it cost just one rupee and felt like the dawn of a new, faster-paced era of journalism. We would pore over his editorials, convinced we were reading the future.
Four decades later, the man behind those editorials would face a different kind of headlines. In 2018, Akbar was accused by Priya Ramani and several other women of predatory conduct. The reputation he had built over years of high-profile editing was dismantled by the testimonies of journalists who accused him of abuse. It was a sobering postscript to the magazine we once admired. Back in the seventies, however, we were oblivious — we just knew that for one rupee, Sunday offered a window into a world far beyond our hospital wards.
These books did more than pass the time. They built the foundation of how I see the world. They taught me that every patient has a story as complex as a Russian novel. I eventually found my voice, but the echoes of those Hindi classics and the silent corridors of the Swaraj Bhandar stay with me — a reminder of a simpler Wardha where the only technology we needed was a well-thumbed book and a bit of imagination.
The Craddock Chronicles
When I was eight years old, my family made a big decision. To them, it was about giving me a better education. to me, it felt like moving to a foreign country. They decided to pull me out of my comfortable Hindi school and plant me in the tougher, stricter soil of a Marathi school. My father found Craddock High School nearby. It had a fierce reputation. It promised not just to teach you to read, but to build your character—usually by putting you through the fire.
Looking back now, from the twenty-first century, I wonder if I was scared. Did I worry about learning a new language? Did I fear making new friends? Honestly, I think I had the blessed ignorance of an eight-year-old. Worries about culture and language belong to adults. As a child, my only real worry was the weight of my school bag and what my mother had packed in my tiffin.
To understand my school, you have to understand the ground it stood on. Wardha is a city that wears its history loosely. Back in the 1850s, it was just a small part of Nagpur. But by the 1860s, the British administrators Sir Bachelor and Sir Reginald Craddock decided to turn it into a proper district headquarters. They designed the city with straight lines and order.
It is a funny twist of history that while we eventually renamed the school, the British ghosts never really left. The school was named after Sir Craddock, and my childhood home was on Bachelor Road. In 1969, to celebrate Mahatma Gandhi’s hundredth birthday, a wave of pride swept the country. Long before Bombay became Mumbai, our school shed its British skin and became Mahatma Gandhi Vidyalaya. But names are tricky things. For those of us who walked its halls in the late sixties, it remained, stubbornly and affectionately, Craddock.
Walking through those gates today feels like stepping into a time machine. The air in Wardha still carries the heavy, rhythmic rumble of passing trains—the background music of our childhood. If the wind blows just right, you can smell the raw, earthy scent of the nearby cotton ginning press. That smell is the scent of memory.
I can still picture my elder sister, Pushpa, walking down these corridors. She walked among future giants. The merit list of 1967 wasn’t just a list of names; it was a prediction. Dr. Abhay Bang, Dr. Ulhas Jajoo, Dr. Prasad Trivedi—men who would go on to define medicine in our region—once roamed these halls, probably worrying about homework just like we did. When I walk through the empty school now, the silence feels heavy with their footsteps.
Typing this on a fast computer feels almost wrong, a betrayal of those days. We lived in a world you could touch. In the late sixties, technology wasn’t a screen; it was wood, glass, and metal. We didn’t have ballpoint pens—teachers looked at them with suspicion. We certainly didn’t have felt pens. And fountain pens? Strictly forbidden. They were considered too fancy, or perhaps too messy, for our clumsy hands.
We wrote like clerks from a hundred years ago. We had wooden desks, glass inkwells, and nibs that you had to dip into the ink every few seconds. My friends Santos Kekre, Ravindra Chawade, and I sat squeezed together at desks with sloping tops. They were terrible for your back, but great for sliding things across. Writing wasn’t smooth; it was a rhythm. Dip, write, dip, write. It taught us patience. Those inkwells were little black lakes waiting to spill, always threatening to ruin a clean white shirt.
If the school buildings were old-fashioned, the teaching was ancient. And the king of this old world was Mr. Dhage, our Mathematics teacher.
Mr. Dhage wasn’t just a teacher; he was a force of nature. He dressed like a man who didn't care about mirrors. He wore an oil-stained cap, a collar that refused to sit flat, and sleeves rolled up as if he were ready for a fistfight rather than algebra. His trousers were a faded grey, held up by an old leather belt. He wore worn-out sandals, but he marched in them like a general.
He didn't wear glasses, but his eyes were terrifying. They swept across the room like searchlights hunting for a prisoner. To Mr. Dhage, math wasn't a subject; it was a religion. He believed in the old rule: "spare the rod and spoil the child." He followed this rule with great enthusiasm. My classmate Vilas Thakur calls it "tough love." I remember it simply as terror.
Mr. Dhage wanted us to memorize everything—the steps, the logic, the ritual. If he saw a mistake in your notebook, his face would twist in genuine pain, as if your bad math physically hurt him. For big mistakes, he would snatch the notebook, tear out the page, crumple it up, and throw it away. "What nonsense is this?" he would shout, his face turning red. "You call this math?"
He had a talent for insults. Abrar Alvi, a student who was a bit slow to answer, was a favorite target. Dhage would sigh, look at the class, and say, "Our train has reached Itarsi junction. We all know the train stops there for thirty minutes to change engines. Abrar is the Itarsi of this class. We must wait." It was cruel, but if you weren't Abrar, it was hard not to laugh.
His punishments were strange. If a boy couldn't solve a problem, Dhage would call on a girl. If she got it right—which they often did—he would order her to lightly slap the boy or twist his ear. The shame was unbearable. The boy would whisper desperately, "Hit me lightly, please!" while the class tried not to giggle. It was a bizarre way to teach, using our awkwardness against us.
Mr. Dhage’s surname means "Cloud" in Marathi. It was ironic because he loved to make students stand on their benches. I had a very tall friend who, when standing on the bench, would almost touch the ceiling. The class would whisper, "He’s gone into the clouds."
Dhage’s power didn't end when the bell rang. Mr. Mankar, our gentle Hindi teacher, had the bad luck of having the class right after Math. Dhage would often keep teaching past his time, lost in a difficult problem or a scolding. We would watch with glee as the two teachers argued at the door—the fierce mathematician refusing to make way for the poet. It was the only time we ever saw Dhage on the defensive.
If Mr. Dhage ruled our minds, Mr. N.D. Kshirsagar—known to everyone as NDS—owned our bodies. He was the Physical Training instructor, built like a rock, with a voice that could shake the walls.
PT class wasn't playtime; it was military drill. NDS would march us to the ground and line us up by height. We weren't children to him; we were numbers stitched onto our shirts. "Number 42, straighten up!" he would bark. Under his watch, not even a bird dared to fly across the school grounds without permission.
He was obsessed with precision. He demanded that the National Anthem be sung in exactly fifty-two seconds. No more, no less. He told us to sing from the "umbilicus"—a medical word that confused us, but ensured we shouted with all our might. "Let your voice show pride!" he would command.
I will never forget one morning assembly. The sun was beating down on us when NDS stepped up to announce a punishment. The student in trouble was Deepak Kalode, a senior. The punishment was a public caning. NDS raised the thin stick and brought it down on Deepak’s legs. Deepak took the first few hits in silence.
Then, in a moment that stopped time, Deepak reached out. He grabbed the stick from the teacher’s hand, broke it over his knee into two pieces, then four, then eight, and threw the splinters on the ground. He walked away without a word.
The whole school stood frozen in shock. Even the terrifying NDS didn't move. It was a rare, electric moment where the wall of discipline cracked, and we saw the fire of youth burning underneath.
The White Gold Mountains
If the classroom was a cage of rules, rulers, and flying inkwells, the world outside the school gates was a wild, open sky.
The geography of my childhood wasn't just defined by the school, but by the Bachhraj Factories. My father was the manager of the cotton ginning press there, which meant I had the golden ticket to an industrial playground. To a modern parent, a factory sounds dangerous. To us, it was a kingdom.
I still remember the cotton season. Trucks would groan under the weight of the "white gold," bringing the harvest in from the fields. The machines would roar to life, separating the seeds from the fibre, a mechanical heartbeat that thumped through the ground. But the real magic happened after the work was done.
The cotton was pressed into massive bales, wrapped in wire, and stacked in towers that seemed to touch the clouds. These stacks were our mountains. My friends—Shekhar Deshkar, Suhas Jajoo, Chandu Fattepuria, and the rest—would climb these soft, white cliffs. We would run and jump across the gaps, sinking into the deep, pillowy cotton. We would emerge looking like snowmen, covered in white lint, standing on top of the world, surveying Wardha from our soft, high throne. We went home dirty, tired, and absolutely happy.
The Box Man
In that group of friends, Santos Kekre was the one you couldn't miss. He was a thin boy with a smile that could light up a dark room. While most of us carried our books in simple cotton bags slung over our shoulders, Santos was different. He arrived every day carrying a distinctive aluminium box.
It was shiny, sturdy, and unlike anything else in the school. Naturally, because schoolboys are cruel geniuses, we named him "Petiwala"—The Box Man.
But Santos was tougher than he looked. In 1958, a terrifying fever called encephalitis swept through our region. Santos caught it. He spent three months in Mayo Hospital, hovering between life and death, enduring painful spinal taps. He was one of only two people in the entire region to survive without brain damage. Maybe that brush with death gave him his courage.
I remember one day in English class. A teacher wrote the word "Seing" on the blackboard. Santos raised his hand. "Madam," he said, "the spelling is wrong. It is S-E-E-I-N-G."
The room went deadly quiet. Correcting a teacher was a crime. She turned on him. "So, you are teaching me now?" she snapped. "How do you spell 'going'? You add 'ing' to 'go'. So 'see' becomes 'seing'. Sit down!"
Most boys would have crumbled. Santos didn't. He marched straight to the Headmaster, Mr. Deshmukh. The Headmaster was horrified by the teacher's mistake and scolded her. It was a small victory for spelling, but a huge victory for Santos. The boy with the aluminium box had a backbone of steel.
Rich Man, Poor Man, Beggar Man, Friend
One of the most beautiful things about growing up in Wardha in the sixties was that money existed, but it didn't matter.
Our class was a strange mix. Chandu Fattepuria came from a wealthy family of cotton traders. Vilas Thakur lived in a massive British bungalow with guards at the gate because his father was the police superintendent. Baban Sonwane’s father was a government minister.
Then there were the rest of us. My father was a manager; others were sons of teachers. But once we crossed the school threshold, or climbed onto those cotton bales, the differences vanished. The rich parents of that era were different. They were humble. They never flaunted their wealth or asked for special treatment. In fact, they told the teachers to be stricter with their sons.
We shared our food, we shared our punishments, and we shared our secrets. There was no VIP section in our childhood. We were just boys.
The Invisible Wall
But if money didn't divide us, gender certainly did. Our school was "co-ed" on paper, but in reality, an invisible wall ran down the center of the hallways.
Shubha Thatte, Lina Wele, and Suhas Jajoo might have been family friends who played together at home on Sundays. But inside the school? They were strangers. Boys spoke to boys. Girls spoke to girls. Crossing that line was social suicide.
If a boy accidentally brushed past a girl in the corridor, the other boys would scream, "Contaminated!" The poor soul would be teased for days. It seems funny now—the idea that talking to a girl was a dangerous act—but those were the rules. We found small ways to show off, of course. During the break, we would rent bicycles for ten paise an hour. We would ride frantically fast, doing tricks, secretly hoping the girls were watching from their side of the invisible wall.
Music and Mayhem
Amidst the noise of school, there was one voice that could stop time. Vikas Kale was our musical prodigy. He had a voice that sounded too mature, too perfect for a schoolboy.
On school picnics, when the chaos settled down, Vikas would sing. I remember him singing songs from the Geet Ramayana. The rowdy boys would stop shouting. The teachers would stop scolding. For a few minutes, the dusty picnic spot felt like a temple. He didn't just sing; he cast a spell. We all knew he would become a star, and he did, becoming a renowned classical singer years later. Vikas lives in Wardha.
But for the rest of us, the real music was the sound of the recess bell.
The twenty-minute break was pure chaos. We would explode onto the field. Footballers claimed one corner, cricketers claimed another, but mostly we just ran. We didn't have teams; we had mobs. A boy might be fielding for a cricket match while standing in the middle of a football game. The ball would fly, bodies would collide, and the noise was deafening. It was glorious. We played with the desperation of prisoners let out into the yard, trying to squeeze a whole day’s worth of fun into twenty minutes.
The Sweetest Memory
I want to end with a memory that smells like chocolate.
In the fifth grade, someone brought a box of chocolates to school. I don’t remember who, and I don’t remember why. But in a moment of pure, innocent generosity, we decided to give them to our teachers.
We tracked down Mrs. Amte, one of our strictest teachers. She was walking towards the staff room. We swarmed around her, a gang of ten-year-olds holding out chocolates like they were gold coins. "For you, Madam!" we chirped.
She stopped. She looked at this group of messy, noisy boys blocking her path. And then, her stern face cracked. She laughed—a warm, genuine laugh that we had never heard before. She took the chocolate.
It was a small thing. But it stays with me. It was the moment we realized that our teachers were not just rule-books with legs. They were people. And just like us, they liked chocolate.
That was the magic of those days. The stinging slaps of the math teacher faded, but the taste of that chocolate, the softness of the cotton bales, and the sound of my friends laughing—those things stayed. We were young, we were equal, and the world was just waiting to be explored.
The Master and the Petiwala
Among the sea of boys at Craddock, Santosh Kekre was an aristocrat of hardware. He was a lean, wiry boy, possessed of an infectious smile that seemed far too large for his modest frame. However, it was his school bag—or rather, the lack of one—that defined him. Every morning, Santosh arrived clutching a distinctive aluminum box. It was a sturdy, rectangular affair that clattered rhythmically against his thigh as he walked. To the rest of us, this was an invitation to mischief, and we promptly christened him "Petiwala." Most boys would have withered under such a title, but Santosh wore the nickname like a medal of office.
There was a quiet gravity to Santosh that we didn't quite understand until we heard of the Great Encephalitis Outbreak of 1958. In a time when medicine was more a matter of prayer than penicillin, Santosh had been one of only two children in all of Vidarbha to survive the brain fever. He had spent three months in the cavernous wards of Mayo Hospital, Nagpur, enduring the terrifying ritual of the lumbar puncture—a needle to the spine that would have broken the spirit of a grown man. The Nagpur newspapers had hailed him as a medical miracle. We looked at him with a new kind of awe; the virus had spared his sharp mind, leaving only his lean frame and that indestructible smile as a testament to his victory.
Our schoolroom was a place where the teacher’s word was Law, even when the Law was wrong. I remember a particularly stifling afternoon when our teacher—a woman of formidable certainties—scrawled the word "Seing" on the blackboard. "Memorize it," she commanded. "S-E-I-N-G." The room was silent, save for the scratching of nibs. Then, from the middle row, the Petiwala’s hand went up. With the reckless honesty of a survivor, Santosh pointed out the missing 'e'.
The teacher froze. She turned from the board, bestowing upon Santosh a look so withering it should have reduced him to ash. "So," she hissed, "the student has become the master? You add 'ing' to 'go' to make 'going,' do you not? Therefore, 'see' becomes 'seing.' Do not try to teach me my own tongue!" Trembling but undeterred, Santosh did not retreat. He took the matter to the Headmaster, Mr. M.J. Deshmukh, a man whose authority was announced by the rhythmic thump-drag of his noticeable limp. The teacher was reprimanded, the 'e' was restored, and Santosh returned to his desk, utterly unaware that he had just committed the ultimate sin of embarrassing a person in power.
In the gallery of masters, Mr. Dhage, our Mathematics teacher, occupied a pedestal all his own. He was a striking figure, dressed in an oil-stained Gandhi topi and sleeves rolled up as if he were about to move a mountain. Mr. Dhage did not merely teach mathematics; he performed it. He poured his heart and soul into the intricate rituals of simple and compound interest, and the mysteries of time, work, and speed.
Whenever he spotted a blunder, his face would undergo a dramatic transformation. His features would contort with a sorrow so deep one might think he had been personally betrayed. If the mistake was particularly egregious, he would snatch the notebook with a sudden movement, tear out the offending pages, and toss the crumpled remains aside with a sigh of absolute frustration. "What nonsense is this?" he would roar. Perhaps the most dreaded of his rituals involved the rare presence of the opposite gender. If a boy failed to solve an equation, Mr. Dhage would turn to one of the girls. If she provided the correct step, he would command her to walk over and strike the boy on the head while he held his own ear in penance. It was an exquisite humiliation.
The Song of the Dug-Dugi
If the aluminum box was Santosh’s trademark, his father’s car was the town’s entertainment. Mr. Kekre senior was a man of unimpeachable honesty who served the Zilla Parishad. His pride and joy was a second-hand Morris Eight, a temperamental beast that seemed to view the streets of Wardha with deep suspicion. It groaned, it wheezed, and it frequently gave up the ghost in the middle of the busiest intersections. We called it "Dug-Dugi" because of the peculiar, rhythmic thumping sound its engine made—a sound that resembled a folk drum more than a combustion engine. Whenever we heard that familiar dug-dug-dug echoing down the road, we knew the Kekre family was approaching. Eventually, the family moved away to Panaji, but in the corridors of Craddock, the ghost of the Petiwala and the missing 'e' remained.
In our class, Chandu Fattepuria came from wealth; Suhas Jajoo had an enviable pedigree; Santosh Kekre’s father was a senior administrator. Three students had politically active fathers: Baban Sonwane’s father was a State Minister; Ashok Gode's father was the President of the Zilla Parishad. Despite the hierarchy of the town, the school was a perfect republic of equals. The sons of Ministers sat on the same splintered benches as the sons of teachers. Wealth provided no shield; our parents gave teachers a simple mandate: "Do not spare the rod if they stumble."
During the break, we found our true freedom. The ultimate luxury was a rented bicycle. For the princely sum of 10 paise per hour, we could hire a heavy, black Hercules cycle. We took turns wobbling across the grounds, the wind in our faces and the rattling of the chain providing the soundtrack to our liberation. For those sixty minutes, we weren't just students—we were masters of the road.
Decades passed, as they inevitably do. I ran into my old bench-mate Shekhar at a Thane railway platform long after our paths had diverged. That night, in a city far from Wardha, Shekhar brewed coffee at two in the morning. We sat and talked until the sun rose. When his wife emerged, she found two middle-aged men chatting with the feverish intensity of those two boys who had once been separated by a math teacher's whim. She wondered who this stranger was who hadn't even attended their wedding, unaware that in the world of Craddock, time and weddings are secondary to the bond of a shared bench.
From Marathi to English, in One Summer
A Leap Across Wardha
By the eighth standard, Craddock High School had become a second skin. The classrooms, the playground, the familiar faces — together they formed a small, reassuring world. I was comfortable there. That was precisely the problem.
I could see, dimly but unmistakably, that the road ahead would demand a command over English and science that Craddock could not give me. Not because the school was poor — it was not. But it was teaching me in Marathi, and I had begun to sense that the world I wanted to enter would not wait for translation.
If I stayed, I would remain safe. I would also remain limited.
What made the decision harder were the friendships I would have to abandon. My days at Craddock were built around people: Suhas Jajoo, Chandrakumar Fattepuria, Chandrashekhar Amte, Narendra Gharpure, Avinash Bhagwat, Kiran Chawade, Vijay Ashtankar, Ravindra Chawade, Namdev Vaidya, Dipak Kalode, Anil Fadnavis, Vishweshwar Mohnapure, and Charudatta Shirpurkar. Among the girls: Asha Fulambarkar, Bharti Deshpande, Lalita Pendsey, Sushma Mondhe, and Mira Pendsey.
Their names were woven into the ordinary fabric of my days — shared lunches, whispered jokes, the easy companionship of adolescence. To leave Craddock was, in a sense, to leave all of them.
Only two came with me to Swavalambi Vidyalaya: Shekhar Deshkar and Sunil Helwatkar. Two doctors in Wardha — Dr. M.K. Pawar and Dr. C.W. Warhadpande — also moved their children, Sunil and Vasanti respectively, to the same school around that time. But the rest stayed behind.
A note on the names: a reader might wonder how a man of sixty-nine recalls them with such precision. The answer is not elephantine memory. My friend Laxminarayan Sonwane — Babya to those who know him, a twist from Baban — gave me a copy of an old Craddock register that carried the names of students from those years. A WhatsApp group of former Craddock friends filled in the rest.
Memory is rarely individual. It survives in groups.
Six years before I arrived, in 1963, Swavalambi Vidyalaya had taken a bold and unusual step: it began teaching science in English. In a town like Wardha, this was not a small decision. It was a declaration.
At thirteen, I understood none of this consciously. I only knew, instinctively, that this was where my future lay.
On 4 June 1969, I joined its sixth batch. I did so quietly, without discussion, and without seeking my parents' permission. It was not courage. It was conviction — which is a quieter thing and, in the end, more reliable.
Six weeks later, Neil Armstrong would step onto the moon. I knew nothing of destiny or metaphor at the time. I only knew that I had crossed the town of Wardha to enter a new school. Yet, in its own modest way, that crossing marked the beginning of everything that followed./
I walked through the big gate of Swavalambi with my eyes forward. To the right stood the Headmaster's office — a room of great quiet and respect. The Biology section opened onto a sprawling, sun-drenched courtyard. The school smelled of possibility, which is a smell you recognise only in retrospect. I did not look back at Craddock. There was nothing to be gained by it.
The Headmaster was Mr. Parshuram Bhajekar. It was a delightful irony that a man named after the fiery, axe-wielding legend of Hindu mythology was, in reality, the most mild-mannered and soft-spoken of souls.
In the ninth grade, I reached a crossroads: Mathematics or Biology. I found the former to be a thorny, unyielding thicket of logic that I simply did not enjoy. I approached Mr. Bhajekar with my desire to switch. He listened with a curious, scholarly patience, and after hearing my plea, he granted me passage into the world of living things. It was a risky choice, perhaps, but that day, standing alone in the corridor, I felt the immense, quiet relief of a boy who had finally chosen his own path.
My school leaving certificate preserves the dates—June 4, 1969, to April 30, 1972—but my memory holds the atmosphere. I remember the scorching May of 1969, oscillating between my old life and the new, just after my elder brother’s wedding. On that first day, I was a stranger among forty-five students. Only four were girls—Kishori Ghirnikar and Rekha Sapkal, who would both go on to join me in the medical profession, and Vasanti Waradpande.
The boys formed a sprawling tribe: Avinash Joshi, Baba Chutke, Bansod, Brijmohan Rathi, Dilip Joshi, Deshpande, Jabbar Khan, Kaushal Mishra, Kuldhariya, Mohan Dubewar, Pandey, Rajendra Phadke, Ravindra Vaidya, Shekhar Deshkar, Sunil Farsole, Sunil Helwatkar, Sunil Pandit, Suresh Singhania, Swarn Singh, Vijay Pawar, Vinod Adalakhiya, Virulkar, and Yeole. We lost Sunil Pawar to throat cancer in 2022, but I still see him clearly at the school’s 25th-anniversary science fair. He was a master of his craft, single-handedly constructing an electric heater on a small brick while I stood by, a mere observer who nevertheless basked in the reflected glory of the prize he won.
Education was a modest expense then; tuition was Rs 7.20 per month. However, because my brother was studying commerce in the same halls, I was granted a "brother’s concession." My parents paid a mere Rs 3.60—exactly the fare for a third-class train ticket from Wardha to Nagpur.
Our mornings began with a prayer by the poet Ramnaresh Tripathi. But the true ritual of the morning involved the white khadi cap. It was mandatory, a symbol of our school’s heritage that we viewed with a mixture of reverence and deep teenage embarrassment. Students from other schools, liberated from such headgear, would mock us. Consequently, we developed a strategic habit: the cap remained stuffed in our pockets until we reached the very threshold of the school gate, at which point it was perched upon our heads with a resigned sense of duty.
That prayer stayed with me for fifty years. Decades later, when my friend Dr. V.K. Gupta visited from Lucknow and gifted me Harivanshray Bachchan’s autobiography, I found a startling echo of my childhood. On page 125, Bachchan writes of reciting that very same prayer at the Mohtashim Ganj Municipal School in Allahabad in 1915. Five decades and a thousand miles could not dim the resonance of those words.
शीघ्र सारे दुर्गुणों को, दूर हमसे कीजिए।
लीजिए हमको शरण में, हम सदाचारी बनें,
ब्रह्मचारी धर्म-रक्षक, वीर व्रत धारी बनें।
॥ हे प्रभु आनंद-दाता, ज्ञान हमको दीजिए…॥
We were guided by a dedicated assembly of masters. Mr. Ramkrishna Pande and Rajendra Singh Thakur oversaw our English; Mr. Shambhusharan Gupta taught Hindi; and Mr. Chintaman Hetre handled Marathi. In the sciences, we had Mr. C.D. Zamvar for Botany, M.J. Gandhi for Zoology, and Mr. Vinayak Zope for Physics. Chemistry was a shared labor between Messrs. Rayalkar, Band, Dattatraya Chitale, and Chaudhary, while Mr. Ambulkar marshaled us for PT.
Mr. Ramkrishna Pande, though our English teacher, possessed a heart that beat for History. We students, ever-opportunistic, discovered that a well-timed question about World War II or Hitler’s tactics would derail the entire lesson. Mr. Pande would forget the English grammar on the board, sit cross-legged on his desk in his dhoti, and lose himself in the ruins of 1940s Europe. By the time the bell rang, he would realize with a start that the German army had advanced, but our English had remained precisely where it started.
Then there was Mr. Chitrakumar Zamvar, a young man in his mid-twenties who brought the microscopic world to life. With models ranging from the humble amoeba to the malarial parasite, he bridged the gap between the textbook and the eye. Even when he was replaced by Mr. Madanlal Tiwari, the fascination remained.
I was a creature of the library. I spent my afternoons at the Rashtra Bhasha Pustakalaya on the Bajaj Electricals campus, where Mr. Purohit would suggest new worlds to explore. I devoured the giants of Hindi literature—Munshi Premchand, Jaishankar Prasad, Mahadevi Verma, and Acharya Chatursen—and eventually the modern prose of Mohan Rakesh and Manu Bhandari.
I even harbored artistic ambitions. In 1969, I sat for the Government Drawing Exam. I was famous among family and friends for my chalk portraits of Shivaji Maharaj and Lord Ram, but the government examiners were less impressed than my aunts; they awarded me a "C" grade.
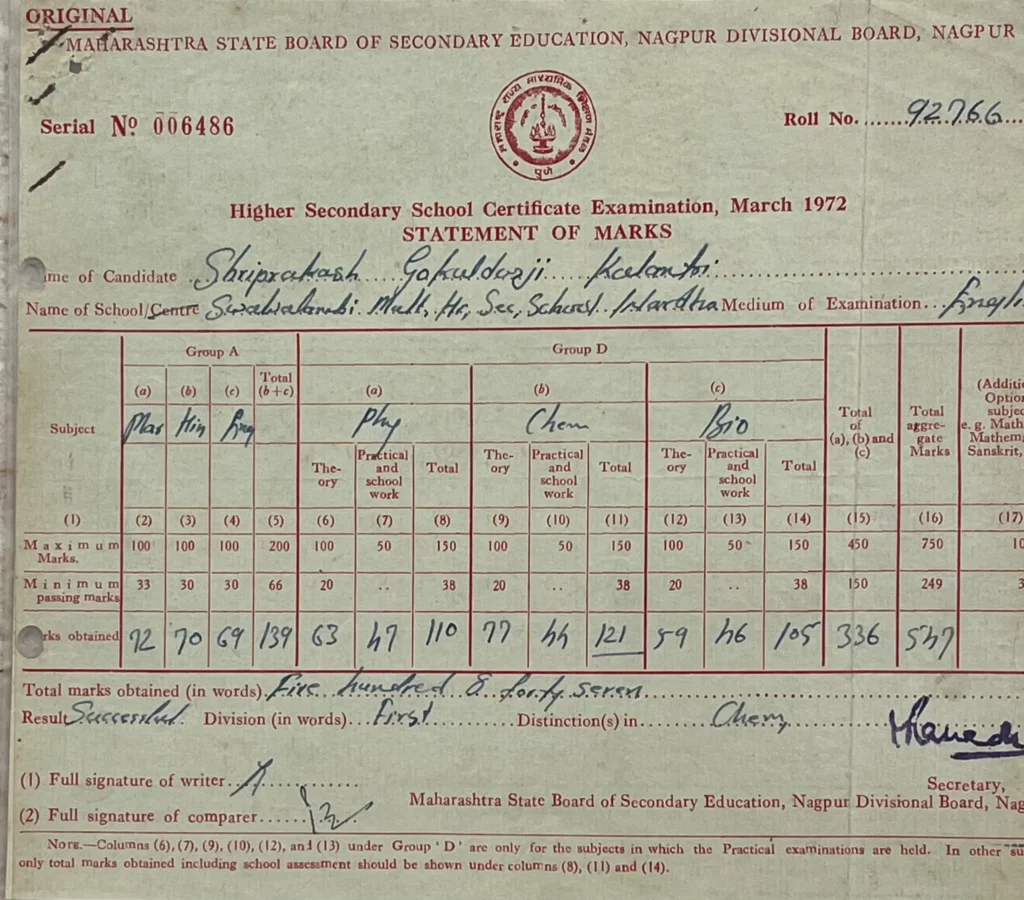
By the summer of 1972, the Board exams arrived. I found my stride, earning a distinction in Chemistry and solid marks across the board: 72 in Marathi, 70 in Hindi, and 69 in English. My confidence was buoyed, though I still hadn't fully grasped that these numbers were the keys to a medical life.
In 1970, when I was in the eighth grade, the domestic peace of our home was shattered by my mother’s illness. At forty-five, she was besieged by the "shadows" of menopause—hot flashes, palpitations, and sleepless nights. Our local physician, Dr. Warhadpande, was stumped.
My father’s concern grew into a quiet desperation until Dr. B.C. Chandak, an intern in Nagpur, arranged for a visit from the renowned Dr. K.L. Jain. The arrival of a Nagpur physician in Wardha was an event of local significance, but what followed was legendary.
Dr. Jain arrived with a bedside ECG machine—a rare, mystical device in those days. As he recorded the electrical signature of my mother’s heart, the news spread through Wardha like wildfire. People spoke in hushed tones of the doctor who could see inside the body with a machine. Whether it was the medicine or the profound "placebo effect" of such a grand investigation, my mother improved almost overnight. For months afterward, my father celebrated her recovery by having fresh fruits delivered from Nagpur, a sweet, seasonal testament to the day the "miracle of the machine" came to our home.
School Was Over
At fifteen, I walked into Jankidevi Bajaj Science College with the singular, heavy-hearted purpose of a boy whose life rested on a single exam. To get into the Government Medical College (GMC) in Nagpur, one had to conquer the BSc Part One. I was assigned Roll Number 562 in Section D.
In the campus hierarchy, Sections A and B were the "good" sections—the academic aristocrats. Section D was a different republic altogether. Many boys came from local business families; they could calculate the profit margins of their fathers’ shops with their eyes closed, but they viewed Zoology with a deep, suspicious apathy. The classroom was a hundred-strong sea of sweating shirts and a low, untamable hum of gossip. Two small wall fans labored heroically against the cruel April heat, but they only succeeded in shuffling the hot air from one side of the room to the other.
That winter, I traded my books for a bicycle and a sudden obsession with fitness. I loved the reckless speed, pedaling across the college grounds with my hands off the handlebars, tasting a freedom that had no syllabus. Along with three classmates, I spent my mornings running in circles, doing squats, and gripping the iron double bars until my fingers went numb in the biting cold.
I might have physically strengthened myself into academic ruin if my friends hadn't shown a rare, selfless clarity. Eight weeks before the finals, one of them looked at me and said, “We are boys with no future, but we won’t spoil yours. You’re the youngest and the brightest. Go home. Study. We don’t want to see you on the ground again.”
I listened. I left the bars and retreated to my desk.
The college was governed by Principal Vasudeo P. Damle, a man of sharp blue eyes and a French beard, topped by a Gandhi cap that sat with geometric precision on his head. When the seven o’clock bell rang, Damle appeared as if the sound itself had materialized him. No one dared to be late.
He and his wife, Mrs. Kamla Damle, turned Botany into a theatrical event. Principal Damle could spend ten lectures on photosynthesis, treating the transformation of light into energy as a miracle. Mrs. Damle taught us Algology with a memory so sharp it seemed to defy time; she lived to be 102, passing away only in 2020.
The department was a microcosm of India. Kamalnayan Bajaj had wanted Wardha to have that intellectual mix. There was Mr. Sathianathan from Chennai, whose booming voice filled the lecture hall when he spoke of mosses and ferns. Mr. R.S. Acharya, another Craddock alumnus, taught Plant Morphology; he was a quiet man who believed the classroom was a sacred space and private tuitions were a sacrilege. In the practical lab, Mr. C.D. Zamvar presided. I could never master the sunflower stem; my blade was always blunt, my sections always slanted. Zamvar Sir would look at my messy diagram and dryly remark, “Kalantri, is this a microscopic stem or a cricket pitch—with a bowler at one end and a batsman at the other?”
Principal Damle’s vigilance extended beyond the morning bell to the very souls of his students. He policed the invisible line between the sexes with the zeal of a frontier guard. During our annual dramas, the stage was a place of strict segregation—there were "All-Boys" plays and "All-Girls" plays, a theatrical apartheid that forced us to find our leading ladies among classmates in wigs and borrowed saris. To Damle, a mixed cast was a script for social ruin.
This rigid code once collided with the cosmopolitan winds of the seventies. A Malaysian girl, perhaps oblivious to Wardha’s unwritten laws, arrived on campus in a skirt. In the sari-clad stillness of the college, it felt like an accidental revolution. Damle did not see a garment; he saw a breach in his cultural fortress. He commanded her to trade the skirt for a "formal dress" at once. In his kingdom, modernity was always expected to bow to tradition.
Our English master, Mr. V.K. Pande, treated the language like a playground. He could take a turgid editorial from The Times of India and make it sing. Once, when I asked for the longest word in English, he beamed and gave me floccinaucinihilipilification—twenty-nine letters signifying the act of treating something as worthless. To a schoolboy, it was a mountain of a word, and I spent days climbing it.
In those days, a teacher earned roughly 633 rupees a month—enough for a new bicycle and little else. Only two professors owned scooters—one being Professor Maheshwari from Zoology. The rest of us, masters and students alike, pedaled the same dusty roads of Wardha under the same unrelenting sun.
I recently sat with my old classmate Dr. Kishor Dubey, who retired from JB Science after teaching Botany there for four decades. He pulled the past back into the present. In our time, the college was the center of the world. Every year, forty students arrived from Sirpur Kagaznagar, and five or six traveled all the way from Malaysia. The hallways were crowded and alive. The Biology division had four sections (A to D) with 100 to 120 students each, while the Mathematics sections (A and B) were packed with 80 to 100 students.
Our monthly afternoons were spent in the "Rescue Debates." We would imagine a burning house with five people trapped inside; the challenge was to argue who should be saved. Murthy and Dubey were the masters of these fierce arguments. Occasionally, Avinash Joshi, Bharti Deshpande, and Sharma would join in, their voices filling the room. When the shouting stopped, Bhagat would sing, his voice so clear it was no surprise he later became a Professor of Music in the Yeshwant Arts College.
On the playground, Shaikh and his partner—both giants at six-and-a-half feet—dominated the kabaddi patch, while Murdiv led the cricket team as captain. Rathod Sir, our Games Incharge, watched us like a hawk. If he saw a student slouching, he would bark: "Why are you standing there like a dead body? Act alive!"
Our laboratories were guided by legends: Ronghe, Supe, Maradwar, and Deshpande in Physics; Galkar, Naigaonkar, Kulkarni, and Sarode in Chemistry; and Maheshwari, Kardar, and Varma in Biology. Mr. Mashankar kept a watchful eye over the library.
“Do you remember the cost?” Dubey asked. “Sixty rupees for the entire year.” Five rupees a month to learn the secrets of the universe.
The university exams in April 1973 were a crucible of heat. I walked out of the hall feeling a rush of confidence, that dangerous certainty that I had cleared every hurdle. But student confidence is a fragile thing; it can vanish in a single morning.
The university exams in April 1973 were a crucible of heat. I walked out of the hall feeling a rush of confidence—that dangerous certainty that I had cleared every hurdle. But student confidence is a fragile thing; it can vanish in a single morning.
In those days, the university didn't send letters; the results simply appeared in the local newspaper. My father was an early riser, a man who treated the morning paper with the devotion of a ritual. He would scan it from the first headline to the last advertisement as soon as it hit the porch. One June morning, at six o’clock, his eyes chanced upon the BSc Part I results. His excited call broke the silence of the house, pulling me from a deep sleep.
I came running from the house, still half-awake, to the front lawn where he sat in his chair. The morning was quiet and the air was still cool. He opened the newspaper, his eyes scanning the tiny columns of print, and asked for my roll number.
"562," I said. My voice was calm; I expected to see my name among the toppers.
We looked once. Then again. The number was not there.
The world seemed to go silent. That cool morning air suddenly felt heavy. I felt a cold, hollow knot tie itself in my stomach. My father stared at the paper with a look of pure bewilderment, as if the ink had betrayed him. He had never imagined I could fail, and seeing that empty space where my number should have been felt like a physical blow. The shame was sudden and sharp.
We searched one last time, our eyes stinging, until we found it at the very bottom under a different heading: “Withheld.” I hadn’t failed, but I hadn’t passed either. I was a ghost in the system. A simple clerical error had trapped my entire future in a dusty university file cabinet, leaving me in a state of agonizing limbo for weeks.
The following weeks were a blur of university counters. When the envelope finally arrived, my hands shook. Seventy-three percent. It was the magic number. I had my seat at GMC Nagpur.
The house erupted in laughter and the scent of sugar. My mother made kilos of pedhas. I was to be the first doctor in the family. As I packed my bags to join Suhas Jajoo, Rekha Sapkal, Avinash Joshi, Rajan Bindu, Narayan Dongre, Pramod Mahajan, Prabhakar Patil, Laxmikant Rathod, Ashok Gambhir, Nandkishor Taori, and Maya Khati, I felt a rush in my chest. We were young, sure of ourselves, and blissfully unaware of the long nights ahead.
The First MBBS
At our class reunion in 2014, we spoke of a classmate who had been a star in school—the kind teachers held up like a warning: Study like him, or suffer like the rest. In First MBBS, he fell short on attendance and the college did not allow him to sit for the exam. That one decision flattened him, and after that something in him seemed to loosen. In internal tests he began scoring seven or eight out of fifty—marks that looked less like failure and more like surrender.
He tried again and again, but the first year would not let him through. After five attempts, the college asked him to leave. He stepped out of medicine and settled somewhere else, carrying a quiet defeat that none of us quite knew how to speak about. That is what First MBBS could do: it was not merely an examination, it was a gate, and once it shut, it did not open easily.
In November 1974, all 204 of us sat for it.
By then my address had changed, as student addresses do—without ceremony, but with the faint sense that life was moving ahead whether you were ready or not. I had spent a year in a cramped room at Bachhraj Factory’s ginning press. In July I moved to Hanuman Nagar, and the new address—484, Hanuman Nagar, Nagpur—felt oddly reassuring, as if the number itself promised stability, at least until the exams were over.
Suhas Jajoo and I shared a modest flat owned by Mr Ishwar Deshmukh. We hired a cook—Pandit Parasnath Sharma Chaturvedi—a short, wiry Brahmin from Uttar Pradesh who ran our kitchen like a temple. His food was simple, clean, and always on time, and he spoke in a nasal twang that made even dal sound like an instruction.
Three seniors from the 1968 batch joined us for lunch and dinner—Ulhas Jajoo, Suresh Chhajed, and Prakash Gupta—and with them entered something we hadn’t known we needed: discipline. Ulhas, especially, had a gift for order. He wasn’t trying to play headmaster; he simply knew what worked, and believed firmly that time, like money, should not be squandered.
Once a month, Suhas and I cycled six kilometres to Itwari market for provisions—wheat, rice, tur dal, moong, groundnuts, oil, salt, spices—everything weighed carefully, tied in brown paper parcels, and loaded onto our bicycles like a travelling ration shop. Ghee arrived from home in steel tins, carrying the smell of kitchens we missed but never spoke about.
Cooking was done on an indigenous cooker Ulhas had brought from Kolkata. It needed only a few glowing coals, and once the lid was shut, the food stayed warm for hours. It was our microwave of the seventies—slow, silent, faithful.
Then came Ulhas’s most decisive reform: he banished newspapers.
Suhas and I read The Indian Express and Tarun Bharat with the seriousness of boys who believed the world would collapse if we missed the morning headlines. Ulhas saw it as a leak in the dam. “Too many distractions,” he said, and spoke to the newspaper vendor. The man stopped coming, just like that, and our day began without news, without politics, without the comfort of printed words that were not medical.
We did not argue. In those days, juniors did not debate orders. We followed them the way soldiers follow a general—quietly, without questions, and with the strange relief that comes when someone else takes charge of your chaos.
Paper was precious, so we drew anatomy diagrams on slates. Chalk squeaked, slate dust clung to our fingers, and muscles and nerves slowly began to sit in the mind where they belonged. We cross-questioned each other like examiners. There was no indulgence, no “later,” no “tomorrow.”
Even bathing became part of the syllabus. On winter mornings, Suhas would leave the bathroom door slightly ajar and I stood outside with a book, reading aloud—biochemistry pathways, physiology definitions, lines that sounded dead on paper but could decide your fate in a viva. He listened between shivers, soap and fear doing their work together. Later, we exchanged roles, as if knowledge could pass through steam.
It sounds absurd now, but at the time it felt normal, even necessary. November arrived, and the exams came like a storm you could see from far away—and still not feel prepared for.
***
We passed in the first attempt, and the relief was physical, sitting in the chest, warm and steady. But the results were harsh: nearly a quarter of the class did not cross the line. I entered the anatomy viva with dread and came out barely intact—107 out of 200.
We held our teachers in awe: Dr P. N. Dubey, Dr Gawhale, Navgirti madam. And then there was Dr P. N. Vaishwanar—the physiology professor with the temperament of a thundercloud. He insisted we read Samson Wright, a book that felt written for boys who spoke English at breakfast, while most of us had grown up on Marathi. If he sensed you had relied on Chandi Charan Chatterjee, his face changed. His anger was not theatrical; it was personal—like a man who had caught you cheating in a matter of faith.
So we learnt to keep our books in pairs: Gray with Cunningham, Kadasne with Gray, Samson Wright with Chatterjee, Harper’s Biochemistry beside whatever simplified text we could afford. We lived with these contradictions the way students always do—trying to look serious while simply trying to survive.
Among us was Abhimanyu Kapgate, the son of a farmer from Khandala, twenty-five kilometres from Bhandara. In anatomy, he did something close to unbelievable: he scored 303 out of 400 and took honours, something that happened once in a hundred cases. The examiners came at him like a fast-bowling attack. They tried everything—obscure arteries, nerve pathways, fetal maturation, insertions no sane person should remember at nineteen—but Kapgate stayed calm and answered as if the body had been drawn inside him.
Years later, on his birthday, I wrote on Facebook that he walked through muddy paddy fields with the same ease with which he once walked through the dissection hall. He went back to village life, practised medicine in Navegaon in Bhandara district, farmed wheat and cotton, and cared for people who had little money but endless need. He was the only one among us to take honours in Anatomy and still stop at MBBS—not out of lack of ability, but out of contentment. For him, that degree was not a stepping stone; it was enough.
Weeks passed before results were declared. When the news finally came, smiles appeared and refused to leave. Jayant Pande stood first in the class, taking honours in both Anatomy and Physiology. Kapgate followed with honours in Anatomy. Sharad Jaitly distinguished himself in Physiology and Biochemistry.
Passing First MBBS did more than move us into second year. It gave us confidence—the quiet belief that we might endure what lay ahead—and for a brief while, before the next syllabus rose like another wall, life felt light again.
Life in the Boys’ hostel
In the spring of 1975, the gates of the GMC hostel finally creaked open, offering us a liberation that felt suspiciously like a coronation. For the top twenty rankers, the rewards were aristocratic: single rooms in the wings, a luxury of privacy that most first-year students could only contemplate with envy. The rest of us, the hoi polloi of the medical meritocracy, were content to share rooms in what we considered the promised land. We sold our rickety chairs and bruised tables, rolled up our mattresses, and marched toward the hostel buildings with the fervor of pilgrims reaching a holy site.
Suddenly, the suffocating oversight of landlords and the nervous scrutiny of electricity meters vanished. I was allotted Room 99 in Hostel No. 4, on the third floor. Whether by some cosmic design or a mere administrative fluke, that number attached itself to me like a second skin. For the next seven years—migrating from Hostel 4 to 3, then 2, and finally the postgraduate quarters—I would inevitably find my trunk parked outside a door marked "99." In the world of cricket, ninety-nine is a state of high anxiety, a "nervous" threshold where batsmen freeze. For me, it was a sanctuary; Room 99 became my personal 10 Downing Street, a fixed point in a shifting world.
Liberty is a dangerous thing in the hands of nineteen-year-olds. We used our newfound freedom to explore the nocturnal geography of the city. We would glide through the sleeping streets on our bicycles, pedaling toward Panchsheel Square for a late-night snack, or marching seven kilometers to Saroj Talkies to catch a midnight show. On one particularly absurd night, ten of us walked the entire distance to watch Ujala—a film nearly two decades old—reveling in the sheer pointlessness of the expedition. The hostel wardens, usually clinical registrars far too exhausted by the day’s rounds to play policeman, simply looked the other way.
However, the hostel had its own internal hierarchy, policed by "permanent residents"—men who had failed their finals so frequently they had become part of the architectural furniture. These veterans felt a pedagogical duty to "educate" us. Every night at nine, we were summoned like fresh recruits to a tawdry cabaret. We were made to parody popular songs, tell jokes, or act out scenes for their bored amusement. It was a tyranny of the mundane. Eventually, as with all autocrats, they grew weary of their own cruelty. The ragging ceased as abruptly as it had begun, leaving us with a strange sense of relief and a repertoire of stories we would polish for years to come.
Inside those walls, life was less about textbooks and more about the art of the distraction. We discovered the seductive, obsessive pull of Teen Patti. It was a game played with a religious intensity that saw us huddling over cards in sessions that bled into the dawn. I too was drawn into the orbit of the bluff, fueled by the irrational hope that luck would eventually recognize my merit and tilt the pile of small coins in my direction. We played until our meager pockets were emptied or sleep finally claimed us; fortunately, this particular flirtation with ruin was short-lived, as the glamour of the gamble eventually faded.
When we weren't losing coins at cards, we were losing our dignity in the Table Tennis hall on the second floor. Most of us possessed the athletic grace of a wounded hippopotamus; we had not so much "acquired skills" as we had developed a rudimentary ability to ensure the ball landed somewhere—anywhere—on the opposite side of the table. It was a game of frantic scurrying and hopeful lunges, played with a seriousness that was entirely inversely proportional to our actual talent. If the ball stayed on the table for more than three seconds, it was considered a sporting miracle.
Yet, the memory that remains most vividly etched in the mind is the sensory assault of the morning bath. In those days, geysers were a decadent fantasy and buckets were non-existent. The bathroom doors had been beaten to death by generations of impatient students and could no longer be closed, meaning one simply learned to abandon modesty. We would sit beneath the cold tap, eyes squeezed shut against the chill, and surrender to the flow. Our relationship with water was one of unthinking trust; we drank directly from the washbasin taps, blissfully ignorant of RO systems or the modern fetish for sterilization. There was no "safe" water then—only water—and aside from the occasional, character-building bout of dysentery, we remained remarkably, perhaps stubbornly, healthy.
The hostel mess provided a different kind of training: an education in endurance. We were served a democratic misery of pale brinjal-potato curries, rotis as dry as ancient parchment, and a dal so watery it could have been used as a laboratory reagent. Sundays, however, were a festival of gluttony. When the news of unlimited gulab jamuns broke, a strange expectancy would settle over the wing. I watched in horrified admiration as boys challenged each other to feats of athletic consumption, swallowing dozens of syrup-soaked balls without a hint of a burp.
Most rooms were a chaotic sprawl of books and film star posters, but I took a pride in my own quarters. Room 99 was an island of order. It was always clean and tidy. Those years shaped us in ways the lecture halls never could. We learned the high art of shared survival, how to tolerate a neighbor’s snoring, and how to forgive the small trespasses of communal life. We were young, we were invincible, and we were perfectly happy to drink from the tap and hope for the best.
Boyd and Barbiturates
Our world was a triangle of the library, the ward, and the hostel. The "scholars" in our batch walked the corridors with thick, heavy copies of Goodman & Gilman’s Pharmacology cradled in their arms like holy relics. They seemed to believe that if they carried the weight long enough, the knowledge would enter through their skin by osmosis. The rest of us, seeking clarity over bulk, found our savior in Dr. R.S. Satoskar. He wrote the way a good teacher speaks—simple, direct, and determined to keep you sane while you memorized the half-life of diuretics.
But it was Pathology that truly stole our hearts, and we had one man to thank for it: William Boyd. To us, Boyd wasn't a dry academic; he was a storyteller who happened to hold a scalpel. He didn't just list symptoms; he painted them. He could describe a diseased gallbladder as if he were writing a Gothic novel: “graceful, fragile gossamer folds of the mucosa… loaded down by dense yellow opaque masses, much as a delicate birch tree might be weighed down by a load of snow.” He wrote that influenza could cross a continent as fast as an express train, and he famously compared the lesions of syphilis to “the list of the ships in the Iliad.” We didn't just read Boyd to pass; we read him to see the poetry in the tragedy of disease.
Life in the hostel was a delicate balance of intense study and high-velocity nonsense. Among us was Abhimanyu Kapgate, a boy from a small village in Bhandara whose English was hesitant but whose memory was a biological miracle. Kapgate knew Gray’s Anatomy with the devotion of a priest. You could point to any obscure nerve or a minor muscle in the palm, and he would recite its origin, insertion, and nerve supply with rhythmic precision.
However, Kapgate’s expertise ended at the human body. Cricket was, to him, a baffling foreign ritual. One humid evening in Room 99, Narayan Dongre decided to test the limits of Kapgate’s literal mind. We were all obsessed with eponymous syndromes—Guillain-Barré, Cushing’s, Conn’s. With a perfectly straight face, Dongre asked Kapgate about the “Greg Chappell and Andy Roberts Syndrome.” He followed it up with the “Tony Greig Syndrome,” discussing them as if they were rare tropical conditions found only in the most advanced textbooks.
Kapgate’s pride was his undoing. He didn't admit ignorance. That night, while we stifled our laughter, he went to the library and searched the medical indexes like a man possessed. He spent hours turning pages, hunting for a pathology that only existed on a cricket pitch. He returned late, looking defeated and weary. When we finally broke the news—that these were cricketers, not diseases—he was furious. He vowed a revenge that, like most hostel threats made before the lights went out, was forgotten by breakfast.
But the mid-seventies in a medical hostel weren't just about Boyd’s prose or locker-room pranks. There was a shadow that lived in the corners, born of a system that was rigid, hierarchical, and often indifferent to the human cost of failure.
The afternoon of April 21, 1975, is a memory that remains frozen in time. Chandrabhan Chattani—Chandar to all of us—was a quiet, reliable boy from a business family in Yavatmal. He was the person you played table tennis with to unwind, or the one you shared a quick, oily breakfast with in the canteen. But the Second MBBS University exams had turned into a monster he couldn't outrun.
Just before the Forensic Medicine paper, while we were all frantically reciting toxicological formulas in the corridors, Chandar retreated to his room in Hostel 4. He had been reading Agatha Christie’s Death Comes as the End—a grim, desert-toned mystery. Perhaps its themes of inevitable endings offered a dark comfort to his own despair. Fearing he could never meet the expectations of his family, he took an overdose and chose a permanent exit.
The hostel let out a collective, ragged gasp as the news spread. The crushing irony arrived a month later when the results were posted: Chandar had passed the paper he feared with a 58. He was qualified to move forward, but he wasn't there to see the notice board.
A year later, the silence returned when we lost Pramila Khapre in the girls’ hostel. She was a girl of impeccable grace and beautiful handwriting, but she, too, found the weight of the white coat too heavy to bear. We moved on because the system demanded it. Classes continued, and the wards beckoned. But the corridors of the GMC hostel never felt quite the same again. Some absences don't leave quietly; they remain as a soft, persistent echo in the back of your mind, reminding you that in medicine, the most fragile thing we ever handle isn't the patient—it’s often ourselves.
The university is indifferent to grief; the machinery grinds on. When the results were finally pinned to the notice board, we crowded around, searching for our names. For some, the marks were a source of relief; for others, they were a heartbreaking reminder of what might have been.
My own marksheet is a yellowing relic now. It isn't the transcript of a genius, but of a student who had finally found his footing in the world of clinical logic.
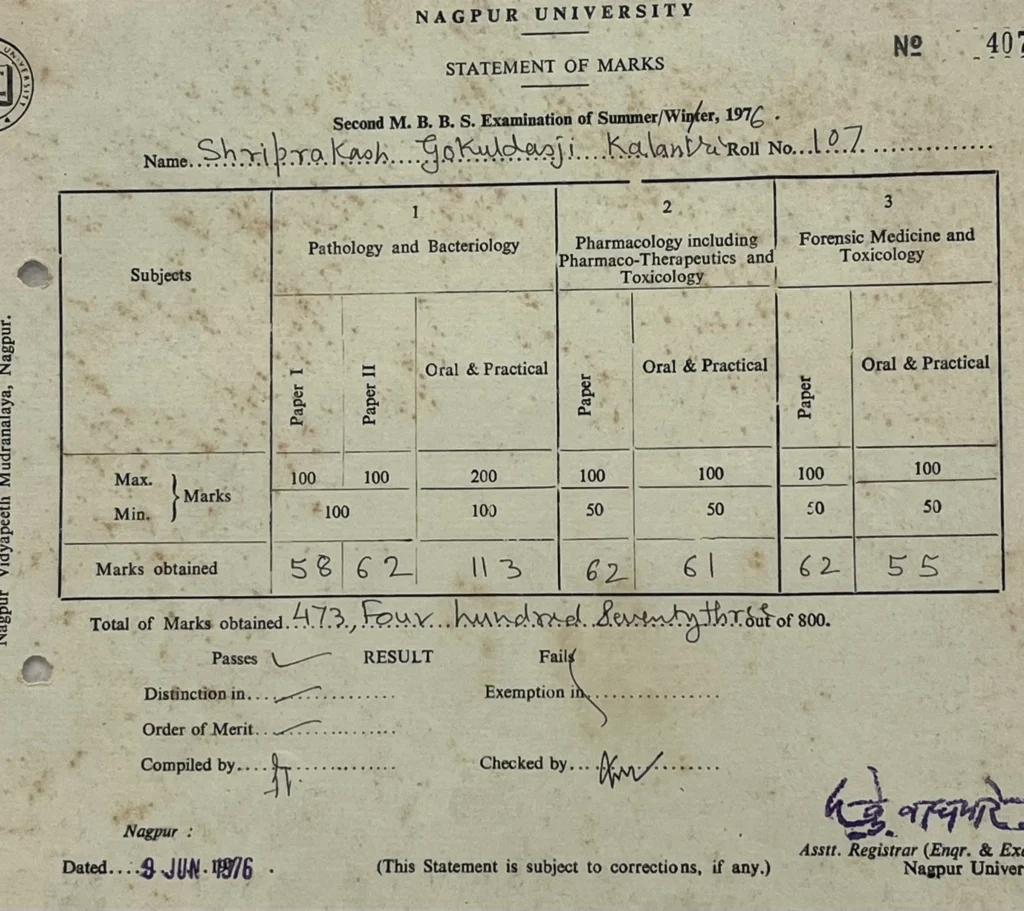
Looking at these numbers decades later, I don't see the marks so much as I see the hours spent under a dim hostel lamp. These figures were our ticket out of the "middle overs" and into the real game. We had survived the grind and the silence. Ahead of us lay the hospital wards and the patients who would eventually teach us more than Boyd ever could.
Summer of the Cooler and the Lambretta
Heat, Harrison, and Hotel thali
The euphoria of the election season faded quickly, as such excitements always do, and the academic calendar resumed its indifferent march. Revolutions could wait; examinations could not.
By the time summer settled over Nagpur in 1977, the city felt less like a place to live and more like something to endure. The sun did not merely shine but pressed down with a steady, exhausting force that softened the tar on the roads and turned the afternoon air into something you pushed aside with your hands. By noon the loo began to blow, hot and gritty, as though someone had opened the door of a furnace.
Most students escaped as soon as they could. Trunks were packed, bicycles loaded, tickets booked. They returned to homes where there were verandas, shade, and mothers who insisted on second helpings of food. Hostel No. 2 emptied within days. Footsteps grew rare. A closing door echoed down the corridor longer than it should have, like a sound reluctant to die.
I stayed back.
The final MBBS examinations were only weeks away, and I told myself that the silence would help me study. Without chatter, card games, or late-night gossip, the days would belong to the books.
Silence, I discovered, has its own weight.
To fight the heat, I bought a second-hand desert cooler from a scrap dealer near the bus stand. It was a dented metal contraption that rattled and coughed when switched on and demanded buckets of water every hour. It cooled nothing with conviction. Mostly it exhaled damp air that clung to the skin. By evening my room felt less like a hostel and more like a cave with a leaking roof.
At night I sprinkled water on the bedsheet and lay down carefully, hoping to borrow a few minutes of coolness before sleep slipped away. The days settled into a routine of reading, sweating, and turning pages. Harrison lay open beside Love and Bailey, their thick spines propped like small walls around me, while a thin line of sweat travelled slowly down my back and gathered at the edge of the chair.
Just when the stillness began to feel oppressive, there was a knock on the door.
I opened it to find Omprakash Singhania standing outside with a small suitcase in one hand and that familiar half-smile on his face, the expression of someone who knows the situation is unpleasant but has decided to endure it anyway.
“You’re here too?” I asked.
He nodded. “Couldn’t study at home.”
That was explanation enough.
We were an unlikely pair. I came from a middle-class household in Wardha where money was counted carefully and nothing was wasted. Singhania belonged to a prosperous family and carried himself with an ease I envied. He owned a Lambretta scooter, which in those days was as good as a badge of privilege.
But the final MBBS examination has a way of flattening such differences. Under that pressure, everyone looks the same—tired, anxious, hopeful.
We settled into a rhythm without discussing it. Through the day we studied in our separate rooms, emerging occasionally to test each other.
“What are the signs of mitral stenosis?”
“How will you manage an acute abdomen?”
“Causes of fever with rash?”
The questions came quickly, like table tennis shots. Somewhere between asking and answering, the fear lost its sharp edges. Speaking things aloud made them manageable.
By early evening the heat softened slightly and the sky turned a dusty orange. That was our signal. Singhania wheeled out the Lambretta, kicked it alive with two firm strokes, and I climbed on behind him. As we rode out of the hostel gates, the wind hit our faces and for a few minutes the day’s fatigue dissolved into that simple, boyish pleasure of movement.
We usually headed to Sitabuldi, to a modest place called Alankar near Anand Talkies. It had metal chairs, scratched Formica tables, and a ceiling fan that squeaked in protest, but to us it felt like a small refuge. For two rupees and fifty paise we could order the special thali—dal, rice, two chapatis, a vegetable, and a little curd served in a steel katori.
The food was ordinary and always the same, yet after a day of heat and revision it tasted generous. We ate slowly and talked about everything except what frightened us most. Families, teachers, rumours from the wards, plans for the future. Sometimes we laughed at nothing in particular. Sometimes we simply sat without speaking, grateful for the company.
I tried to pay my share. He waved it away as if it were a trivial matter, and we settled accounts later in ways that neither of us kept track of. What mattered was not the arithmetic.
Looking back, what I remember most from that summer is not the cooler’s rattle or the weight of Harrison in my hands, but those evening rides through warm air and the quiet comfort of a friend who had chosen, like me, to stay back and face the same anxiety.
Examinations test knowledge, but they also test endurance. And endurance, I learned that summer, becomes easier when it is shared—when someone sits across the table, tears a chapati in half, and asks you one more question before the night begins.
That summer, between the heat, the textbooks, and those evening rides, I learnt a lesson that was not in any syllabus:
Success is rarely a solo journey.
Ambition is heavy. But it becomes bearable—sometimes even enjoyable—when a friend carries it with you, along with a thali.
Teachers, Terrors, and a Quiet Triumph
The Final MBBS curriculum was a hydra-headed beast. Five major subjects, each demanding a different variety of stamina — Medicine with Paediatrics, Dermatology, and Psychiatry trailing in her royal wake; Surgery with Orthopaedics and ENT tucked under its wing; Obstetrics and Gynaecology; Ophthalmology; and the often-neglected stepchild of the whole enterprise, Preventive and Social Medicine, which we called PSM with the casual contempt that only the young and ignorant can manage.
But a medical college is not built on syllabi. It is built on teachers.
In the seventies, Government Medical College, Nagpur was not merely an institution. It was a galaxy of stars — men and women of formidable calibre, frighteningly disciplined, and completely devoted to the hospital in a way that people born into a later era of private clinics and consulting fees will find almost impossible to imagine. They did not treat teaching as a job. They treated it as a duty, and the distinction mattered more than any salary scale could reflect.
They were full-time. No professor rushed through a lecture because an afternoon appointment was waiting across town. Their world began at the college gate and ended in the wards. That single-mindedness gave them a moral authority that we did not question and could not have dismantled even if we had tried. We simply obeyed, learnt, and made every effort not to look foolish.
Government Medical College · Nagpur
The Architects of Our Clinical Conscience
Faculty Roll · The 1970s Era
Medicine
In Medicine, we grew up under the gaze of Dr. B.S. Choubey, who walked the wards like a man who owned not only the department but also the air around it. With him were Dr. Nawaz, Dr. Bhagwat, and the sharp Dr. P.Y. Deshmukh. Dr. Lata Patil and Dr. S.M. Patil taught us the grammar of diagnosis — how to listen, how to look, how to suspect. Dr. H.C. Attal and Dr. G.K. Dubey reminded us, repeatedly, that careful observation almost always beats untested theory. Behind them stood a department of quiet depth: Dr. A. Jeevane, Dr. A. Barua, Dr. V.W. Adbe, Dr. and Mrs. Salkar, Dr. Khurana, Dr. S.R. Tankhiwale, Dr. D.V. Doifode, Dr. B.G. Waghmare, Dr. Jayantibhai Waghela, and Dr. B.R. Maldhure.
Paediatrics & Surgery
Paediatrics had the gentle, unhurried steadiness of Dr. A.M. Sur, Dr. Vibhawari Dani, and Dr. Mrs. Hussain. Surgery belonged to Dr. Vikram Marwah and Dr. M.L. Gandhe, supported by Dr. P.H. Soni, Dr. N.K. Deshmukh, Dr. Johrapurkar, and Dr. R.R. Deshmukh. In the theatres we watched, half-awed and half-terrified, as Dr. R.N. Das, Dr. K.B. Golhar, Dr. Yadkikar, Dr. S.R. Mitra, Dr. Rewale, Dr. Kamble, Dr. B.P. Deshraj, and Dr. M.B. Shende made clean decisions with sharp instruments and an economy of gesture that we envied and could not yet replicate.
Obs & Gynae · Orthopaedics · Ophthalmology · ENT
Obstetrics and Gynaecology was led by Dr. Mrs. Nirmala Mokadam, with Dr. Asha Deshpande, Dr. Venu Shastrakar, Dr. Leela Dubey, Dr. Agrawal, Dr. Survey, Dr. Jawade, Dr. Sarode, Dr. Shobha Gurtu, Dr. Bhattacharya, and Dr. Meena Deshmukh. Orthopaedics was handled by Dr. Saxena, Dr. Wankar, and Dr. Ganeriwal. Ophthalmology had Dr. Ishwarchandra Kamra, Dr. Tehra, Dr. Mala Kamble, Dr. S. Karandikar, Dr. S.U. Joshi, and Dr. Rohidas. ENT was helmed by Dr. M.N. Mahore and Dr. Kumar.
Anaesthesiology & PSM
Anaesthesiology had its quiet guardians — Dr. R.K. Pradhan, Dr. Hema Mankeshwar, Dr. Malti Phadke, and Dr. B.M. Sahay — who taught us, without drama or self-advertisement, the precise value of pain relief and calm hands. And then came PSM — Dr. Ketkar, Dr. Ingole, Dr. N.D. Vasudeo, Dr. M.B. Fulare, Dr. M.C. Pathak, Dr. Prabhu, Dr. P.C. Dubey, and Dr. P.G. Deotale — guardians of public health, doing their best to instruct a roomful of young men and women still entirely intoxicated by the romance of wards and operating theatres.
***
Bhande Plot: Our 'Posting' and Our Picnic
PSM arrived in final year, perhaps to remind us that India did not live only in wards and operation theatres. We were posted to the Urban Health Centre at Bhande Plot, Bapunagar — barely three kilometres from the college. Each student had to 'adopt' five families, monitor their health, understand their living conditions, and function as a kind of primary doctor who was in practice still several examinations away from the right to that title. Usually Dr. Khobragade accompanied us, translating the community into something our ward-trained eyes could understand.
The diseases of the seventies were different, too. Diabetes and hypertension had not yet become the daily background noise of Indian medicine. Instead, we encountered the older enemies — polio, tetanus, rabies, diphtheria, typhoid, tuberculosis, leprosy. Scabies was everywhere, persistent and unglamorous. Jaundice came and went like a seasonal visitor, unremarkable to the families it afflicted.
These visits should have made us humble. They should have taught us that the real India lived not in the teaching hospital's gleaming corridors but in these lanes, in cramped rooms where five people shared a single charpoy and the water supply was a shared tap that ran for two hours a day.
But we were twenty.
For us, Bhande Plot was not a lesson in social medicine. It was a sanctioned escape from the suffocation of college — an excuse to walk in the open air, talking and laughing, with the sun on our faces and no senior registrar to impress. I confess I do not now remember the advice I gave those five families, or whether anything I said made a lasting difference to a single one of them. Public health felt slow and ordinary, while the wards felt urgent and heroic. We preferred heroic. We were twenty.
Only later, much later, did I understand that we had been walking through the very heart of Indian healthcare — and calling it a picnic.
***
The PSM Paper: An Ambush
Our Final MBBS examination opened with PSM, which we had prepared for with the casual confidence of soldiers expecting a small, manageable skirmish.
Then the question paper arrived.
The mood in the hall changed within minutes. The questions were obscure, oddly specific, and designed with what felt like a personal vendetta against anything we had actually studied. They came at angles we had not anticipated. They demanded precision about things we had treated as background reading — the kind of facts one files away under 'probably not important.' We wrote what we could, driven by panic and momentum, filling pages with confident-sounding sentences whose foundations were considerably less confident than their tone suggested.
We walked out stunned. Back at the hostel, the atmosphere was funereal. The usual post-examination chatter — the relief, the post-mortem, the cheerful argument about whether answer B or answer C was correct — had entirely vanished. From the girls' hostel, we heard someone crying. Then more than one. The sound travelled across the campus in the still evening air and sat in our chests like something solid.
That evening, we gathered in the common room in what amounted to a council of war, dressed in pyjamas. We did not study. We consoled. We reassured one another. We made a pact, unspoken but understood: one bad paper cannot ruin five years. And without resorting to any lofty language, we discovered something that no curriculum had formally taught us — that the first duty of a doctor is to offer hope, even when he has none himself to spare.
The remaining papers passed in a blur of nervous energy, fractured sleep, and the peculiar discipline that comes from having no alternative to continuing. Medicine, Surgery, Obstetrics. We wrote, revised, drank too much tea, slept in fragments, woke anxious at four in the morning, and wrote again. When the last bell rang and the last answer book was collected, relief arrived not as a thought but as a physical sensation — something in the muscles, something behind the eyes.
***
Two Practicals and a Small Miracle
Theory tests memory. Practicals test nerve — and the difference, when you are standing at a patient's bedside with two senior examiners watching your hands, is not a small one.
Medicine was my sanctuary. I had loved its logic from the beginning — the detective work of it, the satisfaction when a constellation of signs resolves into a diagnosis that clicks into place like a key in a lock. My long case was Malabsorption Syndrome. My examiners were Dr. S.M. Patil and Dr. Mrs. Lata Patil, both strict, both fair, and both entirely capable of detecting uncertainty at twenty paces.
But at the bedside, something steadied inside me. The history flowed without hesitation. The signs made sense, each one pointing in the same direction. The differential diagnosis lined up in order. Even the viva questions, which can ambush you in unexpected directions, arrived gently that day. I walked out of the examination hall feeling lighter than I had felt in weeks, as though a physical weight had been lifted from somewhere behind my sternum.
I scored 141 out of 200 — a distinction-level score that would later, though I did not know it yet, open the door to my MD.
Obstetrics and Gynaecology was an entirely different story.
I had never been comfortable with the mechanics of labour. The instruments terrified me — the forceps with their confident curves, the entire choreography of a managed delivery that more experienced hands performed with such apparent ease. I still remembered, with a clarity that discomfort preserves better than pleasure, a labour room posting in which I had been asked to conduct a delivery. My hands shook so badly that the slippery newborn almost slid entirely out of my grasp. A nurse caught the baby with reflexes faster than my career had yet managed to develop.
I entered the Obstetrics and Gynaecology practical carrying all of that history, and considerably more dread than I was showing.
And then, as if the gods of examination halls had decided to be merciful for once, I received a case of Placenta Praevia — a textbook diagnosis, heavy on conceptual understanding and blessedly light on the kind of mechanical prowess that had always defeated me. No confusing rotations. No forceps. No instruments to fumble with under the quiet, watchful gaze of a superior.
I spoke with a confidence I did not entirely feel. I explained antepartum haemorrhage, I described the danger signs with appropriate gravity, and I set out clearly why Caesarean section would be the necessary management. The examiners — Dr. Mrs. Dubey and Dr. Sule — listened with the particular attentiveness of people who have heard every version of this explanation and are deciding whether this one is genuinely understood or merely memorised.
When the marks arrived, I looked at the number for rather longer than was strictly necessary.
141 out of 200. Again.
I still call it a miracle, plain and simple, and I see no reason to revise that assessment.
***
The Notice Board
Six weeks after the last paper, the results were pinned to the notice board. A crowd gathered the way crowds always gathered around that board — pushing, craning, some calling out numbers, somebody laughing too loudly, somebody else going very quiet in the particular way that means the news is not good.
I found my roll number.
1031 out of 1600. Sixty-four point four per cent.
In the era of inflated marks and carefully curated academic profiles, it may not look extraordinary. But in those rigorous halls of Government Medical College, Nagpur — where the examiners signed their names to your competence and meant it — it felt like a triumph. I had cleared Medicine theory with 59 and practicals with 62. My examiners — Dr. Mohgaonkar, Dr. Bharaswadkar, Dr. Doifode, Dr. Dekate, and the Patils — had looked at what I knew and decided it was sufficient. That decision, I understood even then, was not a formality.
I looked at the mark sheet for a long time. Not because I needed to read it again. But because I wanted to fix it, to be certain it was real and not some examination-season hallucination born of too little sleep and too much anxiety.
A deep, quiet peace settled somewhere in the chest.
I had done it.
I was no longer a student. I was Dr. S.P. Kalantri.
And in those simpler times — before the feverish race for postgraduate seats began before the finish line was even in sight, before every result became a stepping stone to the next competition rather than an achievement in its own right — we were content. We had climbed the mountain. We had not yet started looking for the next one.
The view, for a moment, was beautiful. And we were young enough to know it.
Internship in Yavatmal
District Hospital, Yavatmal
After passing the final MBBS examination, the next step was a compulsory year-long internship—six months in an urban setting and six in a rural one. At that point, I faced a choice that appeared simple on paper but carried its own weight: should I remain within the familiar walls of Government Medical College, Nagpur, or should I step out into the districts of Vidarbha?
Staying back meant comfort—known corridors, familiar faces, predictable routines. Yet, somewhere within me, a quieter voice suggested otherwise. It urged me to leave what I knew and test myself elsewhere. I listened to it.
And so, I chose the district hospital at Yavatmal, over seventy kilometres from Wardha. I do not recall the precise reasoning that led me there, but I remember the feeling clearly—a pull towards the unknown, and a belief that medicine, if it was to teach me anything lasting, would do so away from convenience.
Yavatmal was not entirely unfamiliar. My elder brother Ashok lived there, which softened the edges of relocation. For meals, we depended on a mess run by a Jain lady, Mrs. Lodha, whose simple vegetarian food sustained us through long days and longer nights. It was not memorable cuisine, but it was dependable, and that mattered.
Each morning, after breakfast, I walked to the district hospital, prepared—though not fully aware—for what awaited me.
Three of my classmates also chose Yavatmal: Atiya Mamdani, Mohan Gupte, and Omprakash Singhania, all of whom had family homes there and were day scholars. Together, we stepped into a hospital that was busy, under-equipped, and relentless in its demands.
We worked under Dr. Phalke, the Civil Surgeon, and alongside a dedicated group of medical officers—Dr. and Mrs. Dharmadhikari, Dr. and Mrs. Ranade, Dr. Bhalme, Dr. Gadekar, Dr. Tayade, Dr. Kedar Rathi, and Dr. Baheti. For a young intern, the pace was unforgiving. Patients arrived continuously, and the hospital never truly rested. Neither did we.
The outpatient department began each day with consultants who were experienced clinicians but far removed from academic medicine. Prescriptions reflected the era: tetracycline, sulfadiazine, and anti-amoebic drugs were commonly used. Quinolones had not yet appeared; cephalosporins were unknown. In the wards, injection procaine penicillin and strepto-penicillin were the mainstay for a wide range of fevers.
Facilities were rudimentary. There were no ECG machines, no ultrasound, no CT or MRI scans. The hospital had no ICU, no NICU, and no dedicated accident unit. Specialists were absent—no cardiologist, no neurologist, no cardiac surgeon. Dr. Belsare, a BAMS physician, doubled as the anaesthesiologist, a role he performed with calm confidence.
The hospital catered to a vast catchment area—Pusad, Darwha, Digras, Umarkhed, Kelapur, Ralegaon, and Wani—places with little or no access to medical care. The flow of patients was constant. We worked almost round the clock, learning quickly that fatigue was a luxury we could not afford.
What the hospital lacked in technology, it compensated for in lessons. Diagnosis depended entirely on history-taking, physical examination, and judgement. There were no investigations to hide behind. We relied on our senses, our reasoning, and sometimes our instincts. It was here that medicine shed its academic polish and revealed its bare essentials.
Over time, my dedication did not go unnoticed. The medical officers grew fond of me. The Dharmadhikari couple often shared their tiffin with me—a gesture that meant more than the food itself. Gradually, I was entrusted with more responsibility.
I learnt to perform lumbar punctures and venesections with growing confidence. I assisted in several surgeries and once came close to performing an appendicectomy on my own—a thought that would alarm me today, but thrilled me then.
Diarrhoea was among the most common—and dangerous—conditions we encountered. Patients arrived dehydrated, with sunken eyes, feeble pulses, and collapsing blood pressure. Renal failure was an ever-present threat. Establishing intravenous access was often impossible. Venesection became the only option.
I performed it repeatedly, so often that my hands learnt the procedure before my mind did. Eventually, I could do it with ease—even in newborns, where precision mattered immensely. With each successful attempt, my confidence deepened, not arrogantly, but steadily.
One skill I took particular pride in acquiring was the writing of patient progress notes. Every morning and evening, I carefully documented vital signs and clinical changes, paying close attention to clarity and handwriting. Slowly, my notes began to stand out. Colleagues noticed. I felt, for the first time, that diligence itself could be a form of competence.
Looking back, the Yavatmal internship was neither comfortable nor glamorous. But it was honest. It taught me how to practise medicine when resources are scarce and expectations immense. It shaped my clinical instincts and my resilience.
More than anything else, it confirmed what I had suspected when I chose to leave Nagpur: real learning often begins when comfort ends.
Learning the Art of Lumbar Puncture
During my internship at the district hospital in Yavatmal in 1978, I encountered a moment that remains sharply etched in memory. A twenty-six-year-old man was admitted with classical features of bacterial meningitis—high fever, altered sensorium, and neck stiffness. A lumbar puncture was essential.
I had never performed one before.
I approached a medical officer for guidance. He was a surgeon, senior to me, and technically responsible for supervising interns. Without even looking up, he refused. There was no explanation, no reassurance, no alternative offered. I was left alone—with the patient, the needle, and my own uncertainty.
I had little choice. I reviewed the steps carefully, positioned the patient, identified the landmark, and paused for a moment. A brief prayer escaped my lips—not out of ritual, but necessity. Then I advanced the needle.
When clear cerebrospinal fluid began to drip, I felt a quiet surge of relief—not triumph, but gratitude. I sent the CSF for cytology and biochemistry and started the patient on penicillin. Over the next several days, I followed him closely, recording his temperature, level of consciousness, and neurological signs with care. Slowly, steadily, he improved. On the tenth day, he walked out of the ward.
Only later did the larger question surface: how does a medical officer entrusted with patients and trainees refuse to teach a life-saving procedure? Such indifference was not unusual in government hospitals of that era, where poverty often dulled expectations and neglect passed quietly as routine.
The incident disturbed me, but it did not deter me. If anything, it reinforced a belief that would guide me throughout my career—that medicine demands responsibility not only to patients, but to those who are still learning its craft.
An April Fool’s Lesson
Memory has a way of softening embarrassment. Over forty years later, I can now recall a foolish prank I played during my Yavatmal internship with a mixture of amusement and unease.
It was April Fool’s Day. In what I believed to be harmless fun, I wrote a short note asking Dr. Dharmadhikari to report to my chamber, signing it with a careful imitation of the civil surgeon’s signature. At the time, the forgery seemed impressive; the consequences did not.
Dr. Dharmadhikari, unsuspecting, presented the note to the civil surgeon himself. The reaction was immediate and bewildered. The civil surgeon denied writing it—but could not deny the signature, which matched his own alarmingly well.
Realisation dawned quickly. Dr. Dharmadhikari traced the mischief back to me and led me quietly to a corner of the hospital. There was no shouting. Only a firm instruction: I was to apologise at once.
As I walked into the civil surgeon’s room, my imagination ran ahead of me. I expected anger, humiliation, perhaps even disciplinary action. Instead, he spoke calmly. He told me, gently but firmly, never to repeat such behaviour.
That was all.
At the time, I felt relieved. With distance, I felt chastened. What I had considered harmless amusement was, in fact, a breach of trust. Medicine leaves little room for frivolity masquerading as wit.
The lesson stayed with me. Professionalism is not learned only from textbooks or wards; sometimes, it arrives quietly, in the aftermath of one’s own foolishness.
Internship in Bhadrawati
Primary Health Centre, Bhadravati
After completing my urban internship, I faced the next decision—choosing a rural Primary Health Centre for the second half of my training. At that time, PHCs were available in four districts: Nagpur, Chandrapur, Bhandara, and Wardha.
Suhas Jajoo and I chose Bhadravati, then known as Bhandak. The village lay nearly a hundred kilometres from Wardha. Reaching it required patience rather than planning. The only mode of transport was a slow passenger train that took over three and a half hours. Buses did not exist, and private cars were beyond imagination.
Bhadravati carried stories older than its name. Local lore spoke of dense forests that once surrounded the town. In the nineteenth century, a Scottish missionary bishop is said to have stumbled upon ancient idols of Chandrika Devi and Parshwanath, half-buried in the jungle east of the village. The district administration fenced the site with barbed wire, and the archaeology department dated the idols to nearly two thousand years.
In 1921, the Kesariya Parasnath idol was reinstalled by Mr. Hiralalji Fattepuria, secretary of the Jain temple and grandfather of my schoolmate Chandra Kumar. He was also a close friend and business associate of my father. The temple maintained a dharamshala, and Mr. Fattepuria ensured that we had accommodation for the entire six months.
Suhas Jajoo from Wardha, Omprakash Singhania from Yavatmal, and I shared a room in the temple premises. Suresh Batra chose to stay with relatives in the village.
Singhania’s inclusion was accidental. He had fallen ill and missed the PHC allotment session at GMC Nagpur. When he arrived two days later, Bhadravati was the only vacancy left. Suhas and Batra did not know him. I intervened, assuring Suhas that Singhania and I had known each other since our hostel days and had worked together during the Yavatmal district hospital internship. That was enough. Singhania joined us.
Life at the temple followed strict customs. Dinner was served before sunset; food after dark was forbidden. By eight in the evening, our stomachs protested loudly. We debated the logic of eating with the sun, but hunger soon found its own reasoning. At nine each night, we slipped out quietly to a roadside stall and restored balance with hot samosas and kachoris.
Work at the PHC was absorbing. We participated fully—in the OPD, vaccination drives, school health surveys, and outreach camps. Dr. Badwaik, the Medical Officer in charge, taught us lessons that textbooks never could—about rural realities, administrative constraints, and clinical decision-making with minimal resources.
Although the Emergency had ended, PHC doctors were still expected to meet targets for tubectomies and vasectomies. Dr. Badwaik led these peripheral camps, and I became his regular assistant. My role was simple but precise—administering antibiotics and analgesics through venipuncture.
I discovered that I enjoyed venipuncture immensely. The moment when the needle entered the vein cleanly and blood appeared felt deeply satisfying. I accompanied Dr. Badwaik to every family-planning camp I could, happy to practise the skill repeatedly.
Despite long hours, we thrived in Bhadravati. Dr. Badwaik noticed our commitment and, one evening, invited us home for dinner. A team from GMC later arrived unannounced to inspect the interns. Dr. S. M. Patil and his colleagues were pleased to find us hard at work in the OPD.
Today, Bhadravati is barely an hour and a half away by road or train. Then, it took three hours by passenger train, followed by a two-kilometre walk from the station to the temple. Roads were rough, trains infrequent, journeys deliberate.
Those evenings, after work had ended and hunger had been temporarily settled, another ritual took over.
During my six months at Bhadravati, I wrote long letters to Narayan Dongre, my GMC Nagpur classmate, who was doing his internship in Wardha. Distance mattered little; letters travelled reliably. There were no mobile phones, no television, no internet to interrupt thought.
Every letter carried only one subject—cricket.
Dongre was passionately devoted to the game. I can still recall his ecstasy when India chased down 403 runs to defeat the West Indies in Port of Spain in April 1976. From Bhadravati, I followed cricket through memory and correspondence. From Wardha, Dongre followed it through statistics.
We debated what ailed Indian cricket, compared Kapil Dev with Ian Botham, and worried about how Anshuman Gaekwad might survive the West Indies’ fearsome fast bowlers. Dongre once wrote, “Prasanna is like a chess player in the guise of an off-spinner—he outthinks his victims before delivering the ball.” He had never played cricket himself, but he knew every score, every wicket, every turning point.
Those letters filled quiet evenings and bridged long distances.
On weekends, I sometimes travelled to Sirpur Kagaznagar, where my elder sister Pushpa lived. Her daughter Tina had just been born. The campus colony felt like another world. Pushpa cooked home food, fussed over me, and gave me the comfort I did not know I missed. We played cards, talked late into the night, and rested.
Looking back, Bhadravati shaped me profoundly. The lessons of rural healthcare, the friendships forged in shared rooms and long clinics, the discipline of work, and the comfort of letters—all stayed with me.
It was a time of learning, not only medicine, but how to live with simplicity, purpose, and companionship.
The House Officer
The first week of my house job left me perpetually alert. Adrenaline carried me from bed to bed—recording vitals, escorting patients, assisting procedures, scribbling notes. We house officers did everything. We clerked patients, accompanied our teachers on rounds, and ran a small side laboratory that was as much a classroom as it was a workplace.
Every patient admitted to the infectious disease wards needed urine sugar estimation. Disposable strips were unheard of. We relied on Benedict’s test—a ritual of sorts. Eight drops of urine, two millilitres of Benedict’s reagent, a flame beneath the test tube, and then the slow watching: green to yellow, yellow to orange, orange to brick red. Colour, we were taught, was diagnosis.
On the third day of my house job, that ritual turned on me.
I was working in the side lab of Wards 37–38 when I lit the Bunsen burner, unaware that spirit had spilled and pooled around it. The flame leapt instantly. I was too close. My face felt the heat before my mind registered danger. Instinctively, I raised my hands to shield myself. My shirt caught fire. There was a brief, terrifying confusion—fire where there should not have been fire.
Ramesh Mundle, Harish Baheti, and Nandu Chandak were nearby. They acted without hesitation—doused the flames with a bucket of water and rushed me to the hospital.
I was admitted to the surgical ward on the second floor. My burns were dressed and bandaged; antibiotics prescribed. News travelled fast. House officers and classmates began to arrive in small groups, filling the ward with familiar voices and quiet concern. They stood by the bed, offered words of reassurance, stayed longer than necessary.
Among them was Archana Srivastava, from my own batch—Batch D. Until then, I had barely interacted with her. Yet she came, sat by the bed, and spoke with a gentleness that surprised me. She told me not to worry, that these days would pass, that I would soon be back on my feet, with no scars worth remembering. There was no formality in her concern, no obligation—only an instinctive warmth. In that moment, I saw in her not a classmate, but a sister.
That bond, formed quietly in a hospital ward, endured. Over time, friendship deepened into kinship. She became my Rakhi sister. Years later, when she married Vinod Srivastava—a neurosurgeon trained at NIMHANS—I attended her wedding in Allahabad. Four decades have slipped by since that visit to the surgical ward, but we remain in constant touch, the connection unbroken by time or distance.
My parents arrived soon after my admission. My mother wept openly. My father stood by the bed for a few moments, pale and shaken, then turned away, unable to stay. My classmates lingered, speaking softly, steadying my parents when I could not.
After two days, I was discharged—with bandaged hands and a temporary dependence I found harder to accept than the pain. An intern helped me record blood pressures, write case sheets, and prepare discharge summaries. Ramesh, Harish, and Nandu took turns filling in the gaps, reassuring my mother that I would be fine. Their quiet loyalty carried me through those weeks.
The burns healed slowly. The scars lingered for years and remain faintly visible even four decades later. In those days, leprosy was common, and my father worried that my scarred hands might be mistaken for something else. Relief came from an unexpected source—a family friend who ran Rambharose Hotel in Wardha prepared a special ointment for burns. My mother applied it daily. She also brought home-cooked meals and, since I could not use my hands, fed me herself for two weeks.
I had entered medicine through fire—quite literally.
***
The infectious disease wards were a daily education in suffering. Cholera, amoebic diarrhoea, and dysentery arrived in a steady stream. Tetanus, rabies, and diphtheria followed with grim regularity. Watching patients with rabies die was especially harrowing—fully conscious, terrified, struggling for breath. Once, I accidentally touched the saliva of a rabies patient. The price of that momentary lapse was fourteen injections of anti-rabies vaccine into my abdominal muscles over a fortnight.
Tetanus was common in the late seventies. Patients arrived with locked jaws and rigid bodies, muscles arching in painful spasms. Convulsions came without warning. Many required tracheostomy just to breathe. Treatment meant tetanus antitoxin, heavy sedation, and weeks of endurance—for the patient and for us. There was little we could offer beyond vigilance and hope.
The ward itself reflected the limitations of the time. Dimly lit, sparsely equipped, it had no monitors, no ventilators, no infusion pumps. We relied on clinical judgment, hands-on care, and constant presence. The air carried the sharp smell of antiseptic, layered over groans of pain. It was medicine stripped of technology, leaving only skill and resolve.
Diphtheria was another feared visitor. The white, leathery membrane over the tonsils was unmistakable. A swab would be sent to microbiology, and the report would return, almost ceremonially: “KLB-like organisms seen.” The membrane could spread rapidly, choking the airway. Isolation was strict, fear pervasive.
Alongside these wards, we spent long hours in the outpatient department of Skin and Venereal Diseases. Our consultant was Dr. B. S. Gowardhan. Scabies dominated the clinic, treated uniformly with benzyl benzoate, applied generously from neck to toe.
What disturbed me more than the diseases was the atmosphere.
Patients with genital ulcers were subjected to comments that crossed the line between humour and humiliation. Privacy was casual, confidentiality fragile. Questions about sexual behaviour were asked openly, sometimes flippantly, without any attempt at education or counselling.
At the time, we did not protest. We did not even recognise the violation clearly. Ethics was not yet a language we spoke. We learned by imitation—absorbing not just clinical skills but also attitudes, with fear and awe mixing freely. A few teachers, brilliant in their medical knowledge, treated patients with condescension, sometimes ridicule. It was accepted as tradition.
Only much later did I understand how deeply such moments shape a young doctor—and how important it is to unlearn them.
Looking back, that posting taught me more than diagnosis and treatment. It taught me about risk, vulnerability, suffering—and about friendship, compassion, and the kind of doctor I did, and did not, wish to become.
Tryst with Dr B.S. Chaubey
Six months passed quickly. By August 1979, I began my second house job—Internal Medicine, Ward 23. The department was headed by Dr. B. S. Chaubey. The thought of working under him made me feel two things at once: thrilled and slightly afraid. His reputation arrived before he did.
Mondays were sacred—and dreaded. OPD began at eight sharp. Dr. Chaubey lived in a palatial bungalow on West High Court Road, a few metres from Shankar Nagar Square, and drove a blue Fiat. My classmate—and then co-registrar—Ramesh Mundle still remembers the registration number: MH 32–8829. We had trained our eyes to spot it the way a sentry watches the road. The moment that Fiat turned into the parking lot, we knew the grace period was over. Dr. Chaubey arrived a few minutes before eight, unhurried and exact. He tolerated many things in life, but not lateness.
So Monday mornings began before dawn. We dressed fast, often skipping tea and breakfast, and rushed to the hospital with one aim: to be inside the OPD before Dr. Chaubey. The waiting area would already be overflowing. Patients came from all over Vidarbha—and even neighbouring Madhya Pradesh—having travelled overnight for a consultation. Many were examined by interns or first-year residents, yet they left satisfied, reassured that their OPD card carried Dr. Chaubey’s stamp. Authority, we learned, could be delivered in ink.
Ward 23 was the male medical ward. The female ward—Ward 25—was on the first floor, with its own house officer, Archana Srivastava, who would later become my Rakhi sister. Admission days were relentless. Forty to fifty patients was routine. We took histories, examined patients, wrote notes, drew blood, estimated haemoglobin, examined peripheral smears, tested urine sugars—then prepared for rounds that moved upward through the hierarchy: registrar, lecturer, reader, professor.
Among the nursing staff, Brother David and Sister Lalamma stood out. They had served in Ward 23 long enough to anticipate Dr. Chaubey’s preferences before he voiced them. Sister Lalamma took a special interest in me. I weighed barely forty kilograms then, and she worried quietly. She brought me lunch or dinner, sometimes even helped with blood samples. Years later, in 1984, I invited her to my wedding. She came.
After rounds—especially the sterner ones—the unit drifted instinctively to the Indian Coffee House on the ground floor, close to our ward. Tea arrived quickly. Masala dosa vanished even faster. Dr. S. M. Patil was the associate professor, and Dr. Viresh Gupta our lecturer. As per GMC tradition, juniors never paid. Seniors insisted on settling the bill. It was an unwritten rule, followed with the seriousness of a posted order.
Once a month, we had a unit party at Hotel Ashoka or Moti Mahal in Sadar. These gatherings marked milestones—completion of house job, submission of thesis, impending weddings. Dr. Chaubey attended without fail. I was usually the only vegetarian and the only one who did not drink. It never seemed to matter.
Around this time, a new two-storey postgraduate hostel was built. Each resident was allotted a single room—girls on one side, boys on the other. I chose Room 99 on the first floor, facing the dental college. I had always liked the number. The room was clean, quiet, and ideal for study.
A telephone stood a few metres away—our lifeline to the wards and to one another. The common mess, however, tested our endurance. Every vegetable seemed to contain potato. The rotis were thick, dry, and cold. By the time we arrived, the dal had lost both heat and hope. One friend summed it up perfectly: “You have to be a yogi to taste hostel food.”
Mornings improved matters slightly. For twenty-five paise, the Indian Coffee House offered salvation—idlis, uttapam, or yet another masala dosa.
And then, almost without warning, the house job ended.
We had lived in a tight loop—sleep, wake, work, eat, sleep again—with little time for reflection. Only later did I realise that Ward 23, with its discipline, fatigue, kindness, and quiet rituals, had taught me not just medicine, but how to endure it.
Residency: The Grind
Entering the Inner Sanctum
In March 1979, the stars aligned. I secured a coveted seat in MD Medicine at the Government Medical College (GMC), Nagpur. In the rigid hierarchy of Indian academia, this wasn't just a degree; it was an elevation to a higher caste. I was no longer merely learning medicine; I was breathing it.
My journey began in Unit 4, servicing Wards 37 and 38. I had barely begun to acquaint myself with the charts—thick, yellowed files held together by rusted iron clips—when the summons arrived. I was to report to Dr. B.S. Chaubey, the formidable Professor and Head of the Department.
A ripple of whispers followed me down the lime-washed corridors. "Why has he called the new boy?" "Is it a test?" I walked to his chamber, heart hammering against my ribs like a trapped bird. The verdict was unexpected: Dr. Chaubey had handpicked me for his own unit. I was to be placed directly under the tutelage of the legend himself.
To work with Dr. Chaubey was a rare privilege; to survive him was a daily miracle.
***
The School of Dr. Chaubey
Between 1979 and 1982, my world shrank to the stone walls of Ward 23 and the Kidney Unit. Dr. Chaubey, a product of the British school of nephrology, wore discipline like a suit of armour.
His routine was a force of nature. Every morning, his blue Fiat would turn into the hospital lot at exactly 7:59 AM. We didn't need watches; the distinctive hum of that engine was our alarm. By 8:00 AM sharp, he would march into the ward, his white coat pristine, his stethoscope draped like a badge of office. We—the registrars and house officers—trailed behind like a nervous retinue, clutching case sheets and praying for invisibility.
In an era before CT scans and automated analysers, Dr. Chaubey was a clinical wizard. He proved daily that a sharp mind, a reflex hammer, and an attentive ear were enough to sketch the inner pathology of a man. But he suffered no fools. His teaching was Socratic, delivered with a razor’s edge.
I remember a post-admission round with agonizing clarity. I was presenting a middle-aged man with paralyzed legs—a textbook case of Acute Transverse Myelitis. I began with the bravado of a resident who had actually read the books. But under the "Grand Old Man’s" gaze, my tongue faltered. When he asked for the diagnosis, I stammered, "Guillain-Barré Syndrome."
The air in the ward froze. Even the overhead fans seemed to stall. Dr. Chaubey’s thick brows furrowed. He didn't shout; he turned to the Associate Professor, Dr. Patil, and pointed a finger at me as if I were a biological specimen.
"Patil," he thundered, the words echoing off the high ceilings, "God save this student. Poverty of thoughts and bankruptcy of ideas."
The verdict hung in the air, heavy and damning. It was a harsh sentence for a slip of the tongue, but in the crucible of Ward 23, there was no room for "loose" logic. That phrase branded my memory. It stung, but it woke me up.
***
The MD thesis is a rite of passage, a scholarly contribution to the ocean of science. Mine, however, was a comedy of errors that would have delighted R.K. Narayan.
Dr. Chaubey had a theory: Pfizer’s new drug, Prazosin, might dilate the peritoneal capillaries during dialysis, washing out more toxins. "Find out if it works," he commanded. "That will be your thesis."
In 1980, haemodialysis machines were science fiction in Nagpur. We relied on peritoneal dialysis—a primitive, messy, and visceral business. We would puncture a patient’s abdomen with a trocar, insert a stiff catheter, and flood the cavity with fluid, waiting for the poisons to seep out into glass bottles.
***
The Kidney Unit, 3:00 AM
The Kidney Unit sat on the ground floor, a place of high science and low plumbing. Dr. Chaubey had been a disciple of Hugh de Wardener at Charing Cross—the man who wrote the book on the kidney. De Wardener was a titan who understood renal physiology but also the human misery of the machine. He had even converted a disused convent into a holiday home for dialysis patients. Dr. Chaubey sought to transplant this British rigor into the humid soil of Vidarbha.
The Unit was the only one of its kind for hundreds of miles. Patients arrived from Raipur and Bhilai, pale, bloated, and literally drowning in their own fluids. I was the junior officer in charge of this precarious kingdom.
Nights were spent in a fugue of exhaustion with Abhichandani, the technician. His pride was a flame photometer—a temperamental contraption that flickered like a moody campfire as it measured sodium and potassium.
At 3:00 AM, the catheter would inevitably clog. The fluid would stop. I would find myself hunched over a gasping patient, manipulating the cannula, praying for a gush of fluid that rarely came. When a patient vomited blood and their pressure cratered, I faced a lonely dilemma. Dr. Chaubey wanted "how" and "why," but the reality was a lottery of leaking tubes and lab errors.
As the July 1981 deadline loomed, the data was a disaster. In several patients, the urea levels actually rose after dialysis. To show these numbers to the Professor was unthinkable—a heresy against the Prazosin hypothesis. Driven by fear, I did what many a desperate scholar has done: I "fixed" the numbers. I massaged the data until it whispered what Dr. Chaubey wanted to hear. The librarian, Mr. Atre, typed the manuscript, and the Dean’s office stamped it into existence.
It lies today in an obscure corner of the GMC library, gathering dust alongside thousands of other academic fictions—untouched, unread, and mercifully uncited.
***
The Remington Machine Gun
The practicalities of research were equally absurd. I had no training in methodology; I didn't know a p-value from a pH value. I hunted for references in the Index Medicus, handwriting abstracts because photocopiers were a luxury for the rich.
The final typing was a manual craft. I took my manuscript to the typist who worked on an ancient Remington typewriter that clacked like a machine gun. Gokhale was a man of leisure. He would type three pages, then disappear to make tea. He would emerge, sip it slowly on his veranda, and suggest editorial changes.
"Doctor, this sentence is too long," he would say, peering over his bifocals. I would nod meekly, hostage to the rhythm of his keys. When the thesis was finally bound—black with gold lettering—I felt only the relief of an escaped prisoner.
***
The Final Hurdle
As the residency drew to a close, the final MD examination loomed like a monsoon storm. To fail was to lose three years of life. Our batch was a "band of brothers" forged in the fires of the wards. We stopped shaving, we barely ate, and we became hypochondriacs by proxy, examining each other's livers and listening to each other's heart sounds in the library.
The practical exam was high theatre. External examiners arrived like visiting royalty. The viva voce was the final interrogation—four professors grilling us on everything from the history of medicine to the mechanics of digitalis. It was a test of nerve. Could you say "I don't know" with dignity?
When the results were posted, six of the ten had passed. The relief was explosive. I was no longer a resident; I was a Physician. I had earned the right to add those two letters—MD—after our names. It was the end of a long, arduous climb, and the view from the top was worth every scolding from Dr. Chaubey and every drop of sweat shed in the wards of GMC Nagpur.
Poverty of Thoughts
Dr. B.S. Chaubey. Even today, the name stirs a familiar cocktail of awe and unease. He could be warm one moment and glacial the next, but his mind always worked like a scalpel—quick, clean, and merciless. He sliced through confusion and exposed the diagnosis we had missed, often in minutes.
For nearly twenty-five years, he ruled the Department of Medicine at GMC Nagpur. Ward 23—his ward—was a crucible. Young doctors were forged there. Some came out tempered; some came out singed; a few came out broken. He had no patience for mediocrity. His temper was famous, his standards unforgiving, and his sarcasm sharp enough to draw blood.
In 1979, I was a Unit 1 House Officer, stretched thin between the chaos of Ward 23 and the Kidney Unit. Mondays were a deluge. Forty new patients would pour in, spilling into the corridors and onto mattresses on the floor. We worked as if time had been outlawed—taking histories, examining patients, chasing reports—fuelled by nothing but adrenaline and fear. Sleep became a rumour.
Then came Tuesday morning. 7:59 a.m.
Dr. Chaubey’s blue Fiat would stop at the porch with a final, impatient squeal. He stepped out as if arriving for a ceremony: red tie perfectly knotted, white apron spotless, shoes polished to a mirror shine. His face carried that thin, unreadable smile, and his eyes moved like a hawk’s—quick, alert, hunting.
The ward stiffened. The Grand Rounds had begun.
A familiar phalanx formed around me—Jalgaonkar, Sarda, Pendsey, Kalamkar, Subhedar, Wasnik, Kane, Mundle, Srivastava. Nurses Bansod and Lalamma stood ready with files. Even our seniors, Dr. G.K. Dubey and Dr. S.M. Patil, looked attentive. Under Chaubey, nobody was truly senior.
He moved fast, dismissing cases briskly—malaria, ulcers, cirrhosis, TB—until he stopped at Bed Number Five, as if something had tugged at his sleeve.
"Present the case," he said.
I had been awake for nearly seventy-two hours. I was unbathed, rumpled, and sticky with fatigue. I knew even my unshaven face would irritate him. I swallowed and began. The patient was sixteen. Both legs paralysed. Numbness below the navel. Bladder distended.
"Kalantri," he cut in, his voice low. "Diagnosis?"
My heart began to thud. My mouth went dry.
"Guillain–Barré syndrome, sir," I said. I tried to pronounce it the way the books wanted—Ghee-yan Ba-ray—hoping a sophisticated French accent could rescue a weak answer.
There was a silence so heavy it felt physical. Then the storm broke.
His nostrils flared. His jaw tightened. With one sharp movement, he pulled the blanket off the boy’s legs and pointed to the abdomen. "Look!" he barked. "No sensory level? Bladder like a drum. Spasticity!"
A small muscle twitched at his temple—his warning signal, the tremor before the thunder.
"Textbook acute transverse myelitis," he said, each word landing like a slap. "And you missed it. Something so obvious!"
My ears burned. The ward seemed to shrink around me. He turned to Dr. S.M. Patil and shook his head, not even pretending to keep it private. "Who sends idiots to Medicine these days?" he asked—loud enough for nurses, students, patients, and even the bedpans to hear.
And then came the line he was famous for. His words were slightly twisted by his facial palsy, yet delivered with perfect aim:
"Poverty of thoughts and bankruptcy of ideas."
Coming from a vernacular school, English had always been my steep climb. His effortless accent made the sentence sting twice—first for what it meant, and then for how beautifully he said it. I stood there wrecked, while he moved on to Bed Six without a backward glance.
Forty-five years have passed since that morning. Dr. Chaubey is gone, but that voice still visits me at odd moments—especially when I am stuck and tempted to settle for the first easy diagnosis.
***
Bankruptcy of ideas.
My colleagues remember it too. Sometimes it comes up as a joke over tea. Sometimes as a warning. Was it brutal? Yes. Did it break me? For a day, it did. But it also shattered my complacency. It taught me to look again, to examine again, to think again.
Ward 23 gave me many things: sleepless nights, aching feet, and a few scars that still smart when I touch them. But it also gave me the habit of thinking straight. And for that—even for that humiliation—I remain grateful.
Residency: The Mastery
Room 99 and making of a Resident
In 1980, the postgraduate residents of GMC Nagpur moved into a new hostel. It was modern, two storeys high, and stood opposite the Dental College—barely a hundred metres from our wards. For boys raised in the crowded barracks of undergraduate hostels, it felt like luxury. Each of us got a single room.
By destiny or design, I landed in Room 99, second floor. The number had followed me through every hostel I had lived in. I accepted it like an old friend.
The room was simple: a table, two chairs, a cot, and a small almirah. From the window I could see the road leading to the Dean’s office, with people moving in and out as if the world ran on files and signatures.
Communication in those days was a physical act. No mobile phones. The hospital PBX worked when it pleased. A single landline sat in the corridor outside my room. It rang with summons—“Bed 4 is gasping”—or, on happier days, news from home.
More often, the call came on foot.
If a patient worsened at night, a ward attendant—almost always a woman in a saree—would walk across, climb the stairs, and knock on the door. In her hand was the call book, a small notebook where the resident had to sign before running back to the ward.
It was a simple system. It was also an accident waiting to happen.
One night, Dr. Pande and Dr. Deshpande were asleep in the dormitory after a brutal 36-hour stretch. The attendant arrived and whispered into the dark, “Deshpande Doctor…”
Dr. Pande, half awake, heard his own name. He grabbed the book and scribbled, in the reflex of a resident who had seen too many arrests: Inject adrenaline and start cardiac massage.
The call, unfortunately, was not for a cardiac arrest. It was for the obstetrician—there was fetal distress.
Even now, I smile at the thought. Then I shudder.
Downstairs, the mess served food that tested both appetite and character. The dal was watery. The chapatis arrived shrivelled. The vegetable was usually potato, sometimes pretending to be something else. We ate because we were young, tired, and hungry.
For breakfast, we escaped to the Indian Coffee House. For twenty-five paise, we could get two fluffy idlis or a crisp uttapam. That was not breakfast. That was survival.
On Being a Donor
In those days, our blood was not only ours. It often became a resource for our patients.
I remember rushing to the blood bank, sleeves rolled up, ready to donate for a patient in my ward who was sinking and needed a transfusion urgently. I would urge the officer to draw quickly so I could run back to work.
And while the paperwork crawled, I would slip into the Sindhi canteen nearby. A hot aloo bonda and a cup of tea—my small reward for a pint of blood.
We were naïve then. We lived in a pre-HIV world. We did not yet respect the silent travellers blood could carry. We saw only the patient in front of us and felt useful, even heroic, for a few minutes.
Later, screening became strict and donation became safer—and rightly so. But I still miss the simplicity of those days, when a young doctor could save a life and feel satisfied with tea and a potato fritter.
A Father’s Love, Delivered in a Box
The MD curriculum is vast, and the list of recommended textbooks can frighten even the brave.
During one visit home, my father asked, “What books do you need?”
I wrote a list: Harrison’s Principles of Internal Medicine, books on the heart, lung, liver, brain, kidney. I handed him the paper, unsure if he would even recognise the titles.
A month later, a heavy cardboard box arrived in Room 99.
Inside were the latest editions of every book I had written down—neatly packed, almost reverently arranged.
I was stunned. In those days, imported textbooks cost close to ₹4,000. My monthly stipend was ₹625. My father was a man of modest means, careful with money, the kind who counted every paisa in his business. And yet he had quietly spent what felt like an impossible sum.
I ran my fingers over the glossy covers and felt something tighten in my throat. It was not just a box of books. It was his faith, sealed with tape.
He never spoke of the cost. He never asked for thanks. He simply wanted his son to learn.
Even today, I cannot recall every chapter I read from those books. But I remember the box.
Slides Before PowerPoint
Before PowerPoint, a seminar was not something you “made.” It was something you crafted.
I was assigned a topic for journal club: Clinical Approach to Coma. I buried myself in Plum and Posner’s Diagnosis of Stupor and Coma, spending weeks trying to understand brainstem reflexes and cortical functions.
Then came the slides.
Somehow, I procured a pack of thick, pure white 8×8 inch cards from FACOR. I followed a strict rule: six lines per slide, not more than eight words per line. With a pencil and ruler, I drew faint guidelines. Then I wrote with a black sketch pen, slowly, carefully, trying to make each letter behave.
On the day of the seminar, I projected those cards with an epidiascope. As I spoke, I watched my teachers’ faces. They did not clap. Teachers rarely do. But I saw it in their eyes—a quiet approval.
That day, I learnt a lesson I have carried ever since: clarity on the slide often reflects clarity in the mind.
A Thousand Names
In 1980, the Department of Medicine at GMC Nagpur hosted the annual conference of the Association of Physicians of India. It felt like a task too big for us.
Nagpur was not a metropolis. Resources were limited. But the department mobilised like an army. Faculty, residents, paramedics—everyone worked day and night.
Dr. Ramesh Mundle and I were given a job that required stamina more than glamour: writing names on certificates for nearly a thousand delegates. We sat for hours, pens in hand, ensuring every spelling was correct.
When the conference began, delegates poured in from across India. The sessions ran smoothly. The hospitality held. The academic content was solid.
At the end, Dr. Chaubey—usually sparing with praise—looked at our handwritten certificates and gave a rare half-smile.
For us, that was more than enough.
The MD Trial
The winter of1980 remains vivid. Ten of us walked out to face that season together—Jayant Pande, Shriram Kane, Aziz Khan, Adesh Gadpayle, Kishore Kedar, Ramesh Mundle, Harish Baheti, Padmakar Somvanshi, Vijay Thakre, and I. We had trained side by side for years, sharing wards, night duties, dog-eared textbooks, and our deepest apprehensions. Now, we were stepping onto the field together, each of us hoping to stay at the crease.
For months, our preparation had been steady and methodical. We practised history-taking until it became muscle memory; we examined patients until our fingertips learnt to see what our eyes might miss. We rehearsed differential diagnoses the way a batsman rehearses strokes in the nets—playing Neurology and Cardiology patiently, defending when unsure, attacking only when the line was clear.
The theory examination went smoothly. We wrote with the calm assurance of men who had judged the pitch correctly. But we knew the real contest—the one that would decide our fate—awaited us at the bedside.
***
The Field Changes
The truth announced itself sharply during the clinicals. Our internal examiners, Dr. B.G. Waghmare and Dr. H.C. Attal, were like familiar umpires. They listened without interruption, allowing us to find our footing and settle into the rhythm of the case. The external examiners, however, changed the field. One was Dr. Mishra from King George’s Medical College—brisk and unsentimental. The other was Dr. V.V. Shanbhag, the Head of Medicine at Topiwala National Medical College. His reputation had arrived long before he did. When he looked up from a case sheet, the room seemed to tighten, as if the bowler had shortened his run-up and the fielders had quietly crept into a catching position.
We reported to Ward 13 at eight in the morning. The beds were occupied by patients brought in specially for the day—men and women from Untkhana, the home for the physically handicapped, whose bodies told complex stories. They carried inherited neurological diseases that moved, spoke, and walked in unfamiliar ways. There was nothing routine about their gaits or their postures. These were our "Long Cases." We did our mental arithmetic: forty minutes for history and examination, twenty to organise notes. It was tight, but we had done it a hundred times.
Then the examiner looked at us and said, evenly, "You have seven minutes to present your case." Seven minutes. We had trained for test matches—unhurried histories, careful examinations, presentations built brick by brick. Overnight, the format had switched to a T-20. Every ball suddenly mattered.
I was allotted a patient with Friedreich’s ataxia. The diagnosis was familiar, the signs waiting to be read. Yet, the time pressure dismantled my rhythm. I tried to play too many strokes at once, fumbling through the history and rushing the signs. Before I knew it, the innings was over. I returned to the hostel with the heavy, sinking feeling of a batsman dismissed for a duck. It wasn't that I didn't know how to bat; it was that I hadn't judged the pace of the bowling. I had read the books and practised the signs, yet I had failed to stay at the crease.
***
The Second Innings
The next day brought the short cases. This time, I took guard more carefully. The patients spoke clearly. Leaky valves murmured their stories; lungs destroyed by tuberculosis told theirs without ambiguity. I listened, examined, and responded without hurry. The bat met the ball. The confidence returned.
Then came the viva voce. The questions arrived steadily, like a probing spell of bowling. I answered what I knew, admitted what I did not, and refused to chase deliveries outside my off-stump. The examiner listened, made notes, and then delivered what felt like the final ball of the over.
"A young man develops syncope each time he urinates. What is the diagnosis?" "Pheochromocytoma," I replied. "And where is the tumour located?" "In the bladder wall, sir."
A pause followed—brief but heavy. Dr. Waghmare’s pen came to rest. Dr. Attal looked up, the severity in his face easing into something quieter. Across the table, the external examiners exchanged a glance over the rims of their thick spectacles. One raised his brows; the other allowed the faintest hint of a smile. It was an expression rarely seen in that room: approval.
The weight of the previous day lifted without ceremony. I knew then, without being told, that I had passed.
Not all of us did. But as I walked out, relief washed over me. I was no longer a resident; I was a physician. Two letters now followed my name—MD—earned through sleepless nights, Dr. Chaubey’s sharp rebukes, and the long, unforgiving hours in the wards of GMC Nagpur.
With distance, I see now that the examination was less a test of brilliance than of temperament. It didn't just ask if you knew medicine; it asked if you could steady yourself after a stumble, adapt to unspoken rules, and think clearly when the clock was ticking. Those seven minutes taught me a lasting lesson: preparation matters, but so does the ability to endure.
Life in the PG Hostel
In 1979, a new postgraduate hostel rose on the GMC campus—freshly built, orderly, and unmistakably modern by the standards of the time. For residents who had spent years adjusting to makeshift arrangements, it felt like a quiet luxury.
Until then, we had lived in a dormitory with sixteen beds, no individual rooms, and zero privacy. It sat on the first floor of the hospital building—convenient, yes, but permanently half-awake. A tired resident would hunt for an empty bed, drop onto it as if shot, and steal whatever sleep he could before the next call dragged him back to the wards.
Communication was primitive. There were no mobile phones, and the PBX failed often. Messages travelled on foot, and confusion travelled with them. A ward attendant—almost always a woman—would walk to the dormitory, locate the resident, and obtain a signature on a call book.
On one memorable night, an attendant called out for "Deshpande." Dr. Pande, half-asleep and thoroughly disoriented, assumed the call was for him. He scribbled an order to "inject adrenaline and start cardiac massage," unaware that the message was actually for the obstetrician managing fetal distress with faint heart sounds. Fatigue was constant, and errors were always waiting.
***
The Move to Order
Against that chaotic backdrop, the new hostel felt like salvation. It stood facing the Dental College, solid and self-assured, with the wards and OPDs barely a hundred metres away. For once, exhaustion did not require a long walk.
The hostel was neatly divided into two wings: ladies on the left, gents on the right. It was perhaps the first time men and women stayed under the same roof in a common hostel, though the demarcation was clear and unquestioned.
I was allotted Room No. 99 on the second floor. I had always liked the number. My window overlooked the busy stretch of road running from the GMC entrance to the Dean’s office. I could watch the campus move through the day—students, nurses, patients, ward boys, and doctors in a hurry, all flowing in the same direction. The room itself was simple: a table, two chairs, a cot, and a compact almirah. Two toilets and bathrooms were shared among ten rooms, and a single telephone at the corner of the wing connected us to the hospital PBX. It was our lifeline—temperamental, unpredictable, but indispensable.
***
The Warden and the Mess
Our warden was Dr. H. C. Attal, then Associate Professor of Medicine—a man who combined discipline with his own unique brand of English. Short, dressed in an untucked bush shirt and chappals, he spoke in a manner that invited more smiles than fear. But a mere lift of his eyebrows was enough to signal that he had no patience for nonsense. He never owned a vehicle, depending entirely on residents to ferry him around as if it were an accepted part of our training. His trusted lieutenant was Mr. Chimurkar, the clerk who knew everyone, everything, and—most importantly—where to find it.
The ground floor housed the mess. The menu displayed a steadfast commitment to brinjal and potato, accompanied by shrivelled chapatis and lukewarm dal. Both disappeared without leaving much of a memory. As a friend put it, you needed spiritual discipline to taste hostel food.
Several of my 1973-batch classmates lived close by—Ramesh Mundle, Harish Baheti, Madhusudan Bagdia, and Shriram Kane. While hostel rooms tended towards disorder, mine was an exception. Driven by an obsession ingrained since childhood, I kept it scrupulously clean, sweeping and swabbing the floor daily—a habit that amused some and baffled others.
I still rode my old undergraduate bicycle. Throughout my MD years, it carried me through the then-quiet streets of Nagpur, faithful and uncomplaining.
The new hostel—with its privacy, its order, and its modest comforts—felt like progress. It did not make residency easy. It simply made it bearable. And at that stage, that was more than enough.
The Things I Didn’t Do at GMC
In the late 1970s, the Government Medical College (GMC) in Nagpur was a place of spectacular, almost exhausting, talent. If you follow Indian cricket today, you understand the modern dilemma known as the "problem of plenty." When you look at the opening slots for the national side, you have the established brilliance of Rohit Sharma and Yashasvi Jaiswal, but then you have KL Rahul, Abhishek Sharma, Ishan Kishan, and even the prodigious young Vaibhav Suryavanshi all waiting in the wings, bats polished, ready to dominate. One feels that even if the top four were to disappear, the replacements would still score centuries.
The GMC Class of 1973 was exactly like that. We had too many "opening batsmen" for life. Had brilliance been a physical substance, the corridors would have needed widening to accommodate us. Everywhere I turned, someone was excelling—singing louder, running faster, or debating with a lethal ease that made the rest of us feel like we were stuck in the pavilion, padded up but indefinitely delayed.
***
The Pavilion View
The auditorium was our sanctuary, a place where the air was heavy with the scent of old wood and the collective sigh of students who had spent ten hours dissecting cadavers or memorizing the Krebs cycle. We would drift there in small groups, smelling of formalin and fatigue, to watch our classmates turn into stars.
Jayant Pande and Vivek Deshpande sang the golden hits of Rafi, Talat Mahmood, and Kishore Kumar with a calm that bordered on the professional. They didn't just sing; they performed "quiet repair work" on our frayed nerves. Sitar strings hummed under the fingers of Shriram Kane and Uday Gupte, while the flutes of Rajendra Sarda and Phadke brought a temporary, pastoral hush to our overworked urban minds. Shashikant Khaire would make the accordion sound like a cheerful conversation, while Jayant Pande—a man who seemed to have a diplomatic treaty with every musical instrument—would jump from the congo to the mandolin without breaking a sweat.
Then there was Vivek Kulkarni—affectionately known as Tillya. He didn't just debate; he held the hall captive. His arguments were sharp, his delivery effortless, and his mind seemed to run a full lap ahead of the judges. He died young, at thirty-three, from cancer of the oesophagus. The news stunned us. Some people belong so naturally to the world of vitality and wit that you never imagine them leaving it early. His absence felt like a clerical error by the heavens—a talent recalled too soon.
***
The Man in the Back Row
And then there was me.
I was a man of spectacular non-achievement. Not out of any grand protest or high-minded principle, you understand—I simply didn’t have the "equipment." I had no gift for music, no appetite for the stage, and certainly no instinct for sport. While my classmates were staking out their legacies on the cricket crease or the basketball court, I was the quiet watcher in the back row. I was the one who clapped the loudest when someone else stole the evening, finding a strange, vicarious joy in their brilliance.
My athletic career was particularly brief. Even our "stadium" was a compromise—a forty-foot terrace at Hostel No. 4, barely the size of a modern living room. The bowler delivered a tennis ball from six yards, not twenty-two, and the batsman was surrounded by close-in fielders waiting like creditors. There was no room for a classic cover drive; one played with tucked-in elbows and a prayer.
My only "proper" boundary came years later, during my internship, in a match between Bhadravati and Ballarpur. I managed a solitary four—a fluke of physics where bat and ball met more by coincidence than intent. I still recall that moment with the disproportionate pride of a man who has very little else to show in the department of physical prowess. Yet, I remained a devoted student of the game, one of those hopeless watchers who can recall scorecards from the 1960s with embarrassing accuracy, despite having no first-hand experience beyond that dusty terrace.
***
The Handwriting "Honour"
In eight long years, my extracurricular record remained gloriously spotless, save for one suspicious certificate: Second Prize for Best Handwriting in a pan-MBBS competition.
I have always regarded this "honour" with deep suspicion. Given the medical profession’s legendary reputation for scrawling like caffeinated spiders, a handwriting competition feels less like a contest and more like an act of misplaced optimism. It is like being named the most sober man in a tavern. I never discovered who walked away with the first prize, or whether their script required a microscope to be deciphered.
Yet, the ghost of that prize haunts me still. Decades later, I wrote a referral note to the cardiac surgeon Dr. Saurabh Varshney. He was so startled by the script—which defied every medical tradition of the "illegible scrawl"—that he posted it on Facebook. My colleagues suspect I am merely being thorough; the truth is that I have quite shamelessly fallen in love with my own calligraphy. In a world of digital fonts and rapid-fire typing, there is a quiet, meditative pleasure in a well-formed "G" or a sweeping "S." It is perhaps the only art form where I wasn't just a spectator.
***
Luxury and Loneliness
I successfully avoided the glamour of the era. Romance was something I observed from a distance, like a naturalist watching a rare species through binoculars. While classmates conducted courtships in the Coffee House or the library—punctuated by stolen glances and meaningful silences—I was… actually, I am not sure what I was doing. I wasn't writing love letters; I was probably re-reading the same chapter of Harrison’s Principles of Internal Medicine for the tenth time. Shyness was my shield, but it was also my cage.
Luxury was equally theoretical. I remember the summer of 1975, when the mess closed and most classmates went home. Om Singhaniya and I stayed back in the sweltering Nagpur heat. We survived on ₹2.50 joint dinners at Hotel Alankar—two people, one plate, no discussion. We ate in a silence that wasn't awkward, just hungry. It was entertainment, nutrition, and social bonding all rolled into one efficient, albeit meager, outing.
***
The Informal Syllabus
I also managed to avoid the informal medical syllabus: smoking and drinking. Medical hostels treat these as compulsory extracurriculars conducted without supervision. You are away from home, surrounded by peers who assume abstinence is merely a temporary condition of childhood.
I still wonder how I stayed away. It was not born of moral resolve or lofty principle. Cigarettes never reached my lips, and liquor never traveled down a throat that remained stubbornly parched. This abstinence survived medical college and, later, even more determined assaults at conference cocktails where generosity was never scarce. In a profession where indulgence is often forgiven and illegibility is expected, my lifelong teetotalism feels less like a virtue and more like a clerical oversight that somehow went uncorrected.
***
The Education of an Observer
I did not stand out. I did not shine. I did not score runs or win debates. Instead, I accumulated something quieter: patience from patients, discipline from seniors, and a peculiar kind of humility that comes from being the least interesting person in a room full of geniuses.
My education arrived through repetition: ward rounds, late-night library sessions, and the slow, grinding understanding of the human body. I was the invisible student, the forgettable classmate, the man who stayed. My legacy from those years is that of a "front-row seat." I got to watch truly gifted people flourish, and perhaps, in the end, being a good witness is as much a vocation as being a good doctor.
It is not a record that would win me a spot in any Hall of Fame. But it is mine, warts and all, and looking back at sixty-nine, I wouldn't trade that back-row seat for all the applause in the world.
The Spectator Who Studied
If my lack of musical or athletic prowess was a public affair, my real education was a private, almost monastic pursuit. While the stars of the Class of 1973 were winning trophies, I was busy building an internal architecture that would eventually support a four-decade career in medicine. At sixty-nine, I realize that what I "did" wasn't flashy; it was simply the relentless application of discipline to the mundane.
***
The Discipline of the Desk
I was a creature of the library. While others possessed the "Socratic spark" that allowed them to shine in spontaneous debates, I relied on the slow, grinding accumulation of knowledge. I discovered early on that I had a high tolerance for the "thick book." I didn't just read Harrison’s Principles of Internal Medicine; I lived in it.
I developed a habit of taking meticulous notes, which brings me back to that second-prize handwriting. It wasn't just about the aesthetics of the script; it was about the discipline of the hand. Writing things down—summarizing a patient's complex history or the specific pathophysiology of a renal lesion—forced me to organize my thoughts. In an era where "Poverty of thoughts and bankruptcy of ideas" was the greatest sin one could commit in front of Dr. Chaubey, my notebook was my shield.
***
The Art of the "Long Round"
While I wasn't on the basketball court, I was on the ward. I became a student of the "Long Round." I realized that if I lacked the natural clinical instinct of some of my peers, I could compensate with sheer volume of observation.
I stayed late. I talked to the ward boys, the dhobis, and the patients' relatives. I learned that a patient's story often changes between the formal morning round and the quiet of the evening. This habit of "lingering"—of being the last person to leave the bedside—taught me more about the human condition than any lecture ever could. It was during these quiet hours that I moved from seeing "cases" to seeing "people." I didn't realize it then, but I was practicing the very "shared moment of silence" I would later write about in my preface.
***
The Teetotaller’s Perspective
My decision to stay away from the "informal syllabus" of cigarettes and alcohol—while social suicide in some hostel circles—gave me an unintended advantage: time and clarity. While my peers were nursing hangovers or navigating the social complexities of the late-night drinking session, I had a clear head.
This wasn't born of a "holier-than-thou" attitude; I was simply too shy to join the fray. But that shyness acted as a filter. It allowed me to stay focused on the rhythm of the Vidarbha roads and the Himalayan treks I would eventually undertake. It taught me that one can be in a culture without being of it. This internal independence would later become crucial when I had to stand my ground as a Medical Superintendent, often making unpopular decisions in the name of ethical medicine.
***
The Habit of Handwriting
My obsession with my own handwriting, which earned me that solitary certificate, became a clinical tool. In a profession where a doctor’s scrawl is a cliché, my legible, sweeping notes became a mark of respect for the next person in the chain—the nurse, the pharmacist, the resident. It was my first lesson in "Systems Thinking." If I wrote clearly, the system worked better.
Even today, when I write a referral, it isn't just a communication; it's a craft. Dr. Saurabh Varshney- the Nagpur based cardiac surgeon- Facebook post about my script was more than just a compliment on my penmanship; it was a recognition of a doctor who took the time to be precise. In medicine, precision is often the difference between a cure and a catastrophe.
***
The Long-Distance Mindset
Finally, I developed the "marathon" mindset. I realized that medicine is not a sprint; it’s a forty-year trek. I didn't need to be the fastest student in 1975; I just needed to be the one who didn't stop walking. This grit—this "spectacular persistence"—is what allowed me to go back to school at forty-seven at UC Berkeley and to start long-distance cycling at sixty.
Looking back, those eight years at GMC Nagpur weren't about the applause I didn't receive. They were about the scaffolding I built when no one was watching. I emerged from GMC as an "invisible student," but I left with a foundation that was deep, solid, and entirely my own.
The Accidental Academic
In the summer of 1982, I had finished my MD at Government Medical College, Nagpur. Like most young doctors, I stood at a familiar crossroads: private practice or hospital life.
My father had already drawn a neat map for me. He had built a modest structure in Wardha, well placed and full of promise. From its windows you could see the bustle of Indira Market and, not far away, the quieter lanes of Maganwadi. It was meant to be my clinic. He could already picture the signboard, the waiting room, the steady income, and our family name taking root in the town.
Only my heart hadn’t signed the papers.
The thought of sitting alone in a clinic all day made me uneasy. I wanted the noise and discipline of a teaching hospital—the ward rounds, the residents, the arguments over diagnosis, the quiet pride of watching a student grow into a doctor. I didn’t have a better plan. I only had a restlessness that refused to leave me.
***
One afternoon, I went to meet my childhood friend, Suhas Jajoo, at his home in Jajoo Wadi, Wardha. As luck would have it, I ran into his elder brother, Dr. Ulhas Jajoo. He was senior to me at GMC Nagpur (Class of 1968) and had known me since I was a boy. Suhas and I had grown up together through school and medical college. Ulhas, meanwhile, was now a Reader in Medicine at the Mahatma Gandhi Institute of Medical Sciences, Sevagram.
He looked at me for a moment—long enough to sense what I wasn’t saying—and asked, almost casually, “Why don’t you join us at Sevagram?”
There was no speech. No persuasion. No “think about it.”
Ulhas did what people of his generation often did when they wanted to help: he acted.
He spoke to Dr. Karunakar Trivedi, the Medical Superintendent of Kasturba Hospital. Things moved with a speed that feels unreal today. I met Dr. Trivedi soon after. He was a man of few words and quick decisions. He glanced at my papers, asked a couple of questions, nodded once, and offered me the post of Senior Registrar.
The salary was ₹650 a month—small on paper, but to me it felt like a king’s ransom.
I said yes, almost before he finished the sentence.
When I told my father, he tried to hide his disappointment, but it slipped out through his eyes. The clinic he had imagined so carefully—the steady, respectable life he had planned for his son—had dissolved in one afternoon.
Yet he didn’t stop me. He never did.
With a grace I understood better only later, he stepped aside and let me choose my own road.
That road led to Sevagram—and then, without my knowing it, to the rest of my life.
***
The Hospital in the Guest House
It was a scorching afternoon on May 4, 1982, when I rode my Bajaj Priya scooter through the gates of MGIMS.
After the imposing stone buildings of GMC Nagpur, Sevagram felt like another country. This was not a purpose-built medical complex. The “hospital” I first saw was an old guest house built by Mr. G.D. Birla in 1940—two storeys, creaking wooden floors, and walls peeling in tired layers. Even the building seemed to carry a memory.
That memory went back to 1969, when Dr. Sushila Nayar began the medical school in this very structure. In those early years, the entire world of MGIMS fit into these two floors. The basic science departments—Anatomy, Physiology, Pharmacology, and Pathology—worked here. So did the library, dissection hall, laboratories, outpatient clinics, pharmacy, X-ray room, wards, an operation theatre, labour rooms, and even a small ICU.
It was cramped, but it was complete.
Over the next decade, the institute grew out of its guest-house skin. By 1982, a new, larger hospital building had come up on the hill, and most departments had moved there. The old Birla guest house, once the whole institution, had become the home of just one department—Medicine. It still housed 140 beds, a small ICU, and, lest I forget, the seminar room where we tried to sound wiser than we were.
Postgraduate training in Medicine had started only two years earlier. Two final-year residents, Hari Om and Ashok Birbal—who would later add “Jain” to his name to be more visible in the local Jain community—were preparing for their MD examinations due in November 1982.
The general wards on the ground floor felt like oversized dormitories. Tube lights glowed dimly, as if they were tired too, and the corners stayed stubbornly dark. The place was spartan—no ventilators, no multipara monitors, no infusion pumps. Central oxygen and suction were still ideas waiting for their turn.
We practised medicine the old way: with a stethoscope, a steady hand, and whatever judgement we could gather at the bedside.
The “ICU” was more a label than a unit. And yet, for all its shortages, this hospital had something Nagpur rarely gave us—stillness. A quiet that softened the day. The air smelled of neem and warm earth, not just spirit and phenyl.
***
Enter “Kissu”
That very first afternoon, I walked into the male medicine ward and saw a resident bent over a patient, doing a pleural tap with the calm ease of someone who had done it a hundred times before. A Littmann stethoscope—rare in those days—hung around his neck, not as a showpiece, but as if it belonged there.
He looked up. Sweat beaded on his forehead, his spectacles sat slightly crooked, and his eyes measured me in a quick scan.
His voice was blunt, but not unfriendly.
“Who are you? And what are you doing here?”
In my crisp new shirt, I suddenly felt like a schoolboy on his first day.
“I’m Dr. S.P. Kalantri,” I said. “I’ve joined as Senior Registrar.”
He paused for a moment. Then his face broke into a wide, sheepish grin. He peeled off his gloves and held out his hand.
“I’m Krishan,” he said. “But you can call me Kissu.”
That handshake steadied me.
I didn’t know it then, but Krishan Kumar Aggarwal—Kissu—would become one of my closest friends in Sevagram. The kind you don’t plan for. The kind life quietly slips into your story. There would be laughter, shared tiffins, long days, longer nights, and the silent understanding that grows between two doctors trying to make sense of rural medicine.
Later, after his MD, Kissu moved to Delhi. He joined Moolchand Hospital, built a formidable career in cardiology, and became a familiar face in the media. Wherever he went, his stethoscope went with him—hospital corridor, home, car, restaurant, even an airport lounge. It hung around his neck like a habit, like a signature.
He was awarded the Padma Shri. And then, in a twist none of us could accept, we lost him during the COVID pandemic—to the very disease he had spent a year explaining, warning against, and fighting every single day.
Even now, when I think of my first day in Sevagram, I see his crooked spectacles and that grin.
***
The Morning Ritual
If the hospital building was the body of the department, the faculty were its soul. In those days, the Department of Medicine had three men at its centre—Dr. O.P. Gupta, Dr. A.P. Jain, and Dr. Ulhas Jajoo.
Dr. O.P. Gupta, the Head of the Department, lived nearby in MLK Colony. This was long before mobile phones and the constant buzzing of “urgent” messages. His life ran on a simple axis: home and hospital. He appeared in the wards without warning, his sharp eyes catching a missing chart or a crumpled bedsheet from what felt like across the ward.
He disliked waste the way some people dislike dishonesty—deeply, almost personally.
“Why are the residents wasting ECG paper?” he would grumble, holding up a long rhythm strip as if it were a luxury item. “I sanctioned two rolls a month ago!”
Every morning at exactly 8:00 AM, a ritual unfolded in his chamber that made residents straighten their backs and swallow hard: ECG correction.
We lined up outside his room with the night’s ECGs clutched like confession letters. Inside, Gupta, Jain, and Jajoo sat shoulder to shoulder, studying each strip with the seriousness of a court hearing. Nothing escaped them—not a missed P wave, not a lazy measurement, not a careless conclusion.
“Why hasn’t this resident calculated the Estes’ score for left ventricular hypertrophy?” Dr. Gupta would ask, peering over his glasses.
“And why can’t they remember the causes of a tall R wave in V1?” Dr. Jain would add, his impatience sharpened by precision.
“They still haven’t mastered vectors,” Dr. Jajoo would sigh, as if our ignorance was a personal tragedy.
It felt like a daily trial by fire. But it was also the finest classroom I ever attended. In that small room—between scolding, silence, and sudden insight—we learned what medicine teaches again and again: the answer is usually hiding in the details.
***
Settling In
Soon my life found a rhythm. Every morning I rode in from Wardha on my scooter, the Vidarbha wind slapping my face like a hot towel. On Tuesdays and Fridays, when I was on emergency duty, I stayed on campus in Kabir Colony—Kabir Niwas, barely three hundred metres from the hospital.
The quarters were modest, even by our standards. Two small rooms squeezed into about 400 square feet, a kavelu roof above, and a farshi floor below that stayed cool under bare feet. The toilets were the old kind—squat only, no commode, no frills, no pretending. Thirteen of these quarters stood in a row, and in our little corner of Kabir Niwas, two of us lived together, making space for ourselves the way young doctors always do—by adjusting without complaint.
I shared the apartment with Dr. Sanjay Shrivastava, an ophthalmologist who somehow managed to look calm even when the rest of us were running on tea, adrenaline, and borrowed sleep. Sanjay stayed for two years, then returned to his hometown, Bhopal, to start private practice. Years later, he would become Joint Secretary of the Medical Council of India. In those days, though, he was simply Sanjay—quiet, steady, and good company on an exhausting night.
One evening in Kabir Niwas, we were doing what young men with little money and big appetites for life often did—huddled around a radio, listening to cricket commentary as if it were a national bulletin. It was 1983, and India was playing Pakistan in Delhi in what people called the first day–night match in India. The lights were new, the excitement was real, and every boundary sounded brighter on the radio.
In the middle of it, I noticed a young man standing quietly outside our door, half in the corridor, half in shadow. He looked hesitant, as if he had walked there and then changed his mind twice.
Dark, shy, self-effaced, and polite to the core—M.V.R. Reddy.
At that time, he wasn’t “Dr. Reddy” yet. He was an MSc from Andhra Pradesh, doing his PhD in Biochemistry. He lived just two quarters away, but we didn’t know him.
He cleared his throat softly and knocked.
“Can I… watch the match?” he asked, almost apologetically.
“Of course,” we said, as if he had asked for a glass of water.
We offered him tea. He sat down without fuss, hands on his knees, eyes fixed on the invisible field inside the radio. For the next two hours, we listened together—four young men in a small quarter, held together by commentary, suspense, and the strange intimacy of sport.
When Kirti Azad began hitting those sixes, our little room came alive. And when India finally won, we celebrated like we had contributed something ourselves—clapping, laughing, speaking all at once, as if the victory had travelled straight from Delhi to Kabir Niwas and stopped at our door.
That was my first real interaction with Reddy.
I had no idea then that this quiet, shy man would become my closest friend, a next-door neighbour for a decade, and almost family. Our children—Ashwini and Amrita—would grow up alongside his boys, Srikant and Sridhar, as contemporaries, as playmates, as if this had been decided that night.
Back home, my mother and my sister-in-law, Kanta Bhabhi, made sure I never went hungry. My tiffin carried the taste of my world—soft parathas, spicy chutneys, and Marwari vegetables cooked the way only home can manage. I often shared it with Hari Om, a warm, easygoing MD resident and an MGIMS alumnus from Etawah. Over those lunches—amid the clatter of steel boxes and the ward’s familiar noise—the feeling of being a stranger began to loosen its grip.
I had come to Sevagram. I had traded the promise of a comfortable private practice for ₹650 a month and a hospital with creaking floors.
And yet, as I walked along the quiet, tree-lined paths of the ashram hospital, I felt something settle inside me.
I was exactly where I needed to be.
The Giants of Medicine
The Men Who Built the Department
A department isn't built only with bricks, beds, and budgets. It is built with people — especially the kind who stay long enough to leave something of themselves behind.
When I joined MGIMS, the Department of Medicine stood on three legs: Dr. O.P. Gupta, Dr. A.P. Jain, and Dr. Ulhas Jajoo. They were different men — different in temperament, style, and the particular way each of them occupied a room. But together, they gave the department something that no infrastructure grant could have provided: a standard worth inheriting.
Every morning at eight, they gathered in the HOD’s chamber for what the medicine residents—Hari Om, Ashok Birbal, Krishan, Kapil Gupta, Vijay Kathuria, the late Ashish Kulkarni, Madhusoodanan, Rakesh Sood, Samir Mewar, and Anil Gombar—quietly called “court.” ECGs were spread out on the table like evidence. A diagnosis was never accepted at face value; it had to be explained, defended, sometimes withdrawn. Mistakes were discussed openly, without embarrassment but without escape. And in that small room, with everyone listening and no one able to hide, learning happened in a way that stayed.
I walked in their shadow first. Later, I had the privilege of walking alongside them. What follows is what I remember — and what I cannot forget.
Dr. O.P. Gupta
Professor of Medicine
Dean, MGIMS (1994–2002)
Dr. A.P. Jain
Professor of Medicine
MGIMS Sevagram

Dr. U.N. Jajoo
Professor of Medicine
MGIMS Sevagram
Dr. Gupta was the anchor.
I joined his unit as a lecturer in June 1983, and my first impression of him was not what I expected. I had braced for the formal distance that senior professors maintain. What I found instead was warmth. Soon after my wedding, he and his wife Geeta invited Bhavana and me for lunch. I was a junior lecturer — barely known, easily overlooked. They treated us like family. That small gesture told me more about the kind of man he was than any ward round ever could.
He had joined MGIMS in 1971, when the department was still finding its feet. In those early years, there were only a handful of physicians. They did everything — OPD, wards, teaching, emergencies, administration — often in the same breath, on the same morning, without complaint. Dr. Gupta carried that habit his entire career. He never seemed to distinguish between what was his job and what simply needed doing.
For years, his unit ran out of the old Birla guest house. The walls peeled. The tube lights flickered weakly. The wards looked more like dormitories than a teaching hospital. But he practised medicine there with the seriousness of a man in the finest metropolitan institution. He never used the building as an excuse for his standards.
He also had a strict streak that kept us alert. Living in MLK Colony, he would sometimes appear in the ward without warning — just to check if the residents were awake and doing what they were supposed to do. It kept us nervous. It also kept us honest. We were better doctors because we never quite knew when he might walk through the door.
As Dean, between 1994 and 2002, he changed how MGIMS examined its students. He pushed for MCQ-based entrance exams, bringing objectivity into a system that could otherwise bend with influence and mood. It was the kind of reform that people resist at first and quietly thank you for later.
Even after a heart attack and bypass surgery, he never stopped learning. When we moved to the new building in 2012, his office sat close to mine. I would often look across and find him bent over a computer screen — reading, searching, figuring things out — like a student who had never quite finished his education.
He retired on 31 July 2023, at the age of eighty. The department didn't just lose a senior professor that day. It lost a habit of discipline.
***
If Dr. Gupta was the steady hand, Dr. Jain was the sharp blade.
He came from Uttar Pradesh and joined MGIMS in 1974. For a time, he had considered Psychiatry. Medicine claimed him instead — and, I think, got the better of the bargain. Dr. Jain believed in the bedside more than the machine. He had no patience for unnecessary tests, unnecessary labels, or the kind of medical theatre that impresses families while helping no one. His consultations were spare and precise, like a well-edited sentence.
He often quoted Osler: "The good physician treats the disease; the great physician treats the patient who has the disease." But with Dr. Jain, this was never merely a quotation. It was a working style, visible in everything he did.
He could be intimidating. His wit could sting. If you tried to cover ignorance with confidence, he could puncture you with a single line. But behind that sharpness lived something solid: a clinician's integrity that patients recognised long before they could articulate it. In 1995, when Dr. Sushila Nayar suffered a massive heart attack, she chose Dr. Jain as her physician — without sending for anyone from Delhi or seeking a more famous name. That choice said more about him than any award could.
He built things too, quietly and without fanfare: the Dialysis Unit, the Geriatric OPD, and the DNB Family Medicine programme, which grew into one of the strongest in the country.
When Parkinson’s disease arrived in 2018, he did not announce it. He simply carried it. His hands trembled. His gait grew unsteady. Yet he continued his ward rounds, his journal clubs, and his teaching. He never dramatised his struggle. He refused to let it define him.
He retired on 31 July 2023, the same day as Dr. Gupta. Two pillars left together on a single afternoon. The hospital felt quieter after that. It still does.
Four days before his fall, Dr. A. P. Jain walked into my office in the Department of Medicine and sat down. We spoke for an hour about the past, the present, and what he still hoped to do. His hands shook. His steps were uncertain. But there was no trace of fear in his voice.
“I take life as it comes,” he said simply.
Then he pushed back his chair with trembling hands and walked away.
On 6 February 2025, he fell in his bathroom and suffered a devastating brain haemorrhage. He spent four weeks moving between critical care units in Nagpur and Sevagram. He died on 15 March 2025, in the very ICU where he had taught, treated, and mentored generations of doctors for nearly fifty years. In the end, he lay connected to the dialysis machines he had introduced to the hospital two decades earlier.
His name, Ajeet, meant unconquerable. For those who knew him, the name could not have been more fitting.
He is gone now. But the way he thought about patients—that precise, unsentimental, deeply humane way of thinking—still lives on in the doctors he trained. Few legacies endure more quietly, or more completely.
***
And then there was Ulhas.
To the world, he is Dr. Ulhas Jajoo. To me, he has always been Ulhas Bhaiyya — and that is the only name I am able to write here without feeling that something essential has been left out.
Our story began long before Sevagram, in Nagpur, when I was still a student and he was the senior who decided newspapers were more dangerous than cigarettes. He cancelled our newspaper subscription to protect two young boys from distraction. At the time, I thought it was strict. Later I understood it was care — the particular, slightly interfering kind that only people who genuinely invest in you will bother to offer.
In 1982, when I stood uncertain at the crossroads between private practice and hospital life, it was Ulhas who looked at me and said, almost without ceremony: "Why don't you join us at Sevagram?"
That one sentence changed the direction of my life. I have thought about it many times since.
He practised medicine like an art, not a transaction. He trusted experience and intuition in ways that kept younger colleagues slightly uneasy — because he was so often right. He would remind us, with a half-smile, that statistics speak in averages while patients arrive one at a time. He never forgot the difference.
His ward rounds had their own unmistakable rhythm. Khadi shirt. Chappals. A crowd of students trailing behind him, notebooks ready. Questions fired like arrows — not to embarrass, but to awaken. He asked about symptoms, yes. But he also asked about money, family, fear, and the long walk to reach us. The patient was never just a case to him. The patient was always a person who had arrived at the hospital carrying more than their illness.
He was a storyteller, and that made his teaching impossible to forget. Students didn't remember only his prescriptions. They remembered his tone, his patience, the particular way he sat beside a bed and listened without glancing at the clock.
Every year on February 14, social media fills with tributes written by people he trained. One student once wrote something that has stayed with me: "I saw Jajoo Sir speaking with patients with compassion, and I wanted to be just like him." That one sentence, I think, is the most complete description of what he gave us.
Ulhas taught us that the most sophisticated instrument in medicine is not the CT scanner. It is the ear. And the willingness to use it without hurrying.
He retired on 28 February 2026, a fortnight after his seventy-fifth birthday. To everyone’s surprise, he soon began private practice, sitting every morning and evening in his younger brother Suhas’s OPD in Wardha.
I still find myself looking at his OPD papers—meticulously written, with careful notes on history, physical signs, diagnosis, and the do’s and don’ts for each patient. Even in retirement, his habits remain unchanged.
He also bought ten acres of agricultural land three kilometres from Sevagram, where he plans to take up organic farming with the help of three local farmers.
I have tried, without much success, to imagine the department without him. I still cannot.
***
Gupta, Jain, and Jajoo built the department I later inherited. They demonstrated, over decades and without ever saying so directly, that serious medicine could be practised in a village. That a hospital need not have the finest equipment to produce the finest doctors. That what a department really runs on is standards, discipline, and a moral spine.
They were, by any measure, giants.
And for many of us — for me, certainly — it was enough that they let us walk beside them.
OP, AP, JP, KP, SP
My relationship with Sevagram did not begin with fanfare or a master plan. It began in the sticky heat of May 1982, when I arrived as a Senior Resident—not quite settled, not quite sure where I was headed.
Dr. Trivedi, the Medical Superintendent then, made it happen. He was a man of few words and quick decisions. He gave me a foothold and moved on. For a year, I worked in the wards, doing what young doctors do best—carry files, chase reports, and stay awake when the body begs for sleep.
Then in June 1983, a post appeared on the notice board: Lecturer in Medicine.
In those days, a government job was not a “career option.” It was security. It was respectability. It was the kind of thing families prayed for.
I applied.
***
The Interview Room
The interview room had an air-conditioner that hummed like a bored mosquito. It didn’t cool the room, but it made the silence feel official.
Across the table sat Dr. B.S. Chaubey.
To Maharashtra’s medical world, he was a titan—Dean of GMC Nagpur, brilliant, feared, and famously short-tempered. To me, he was something else: the man who had watched me closely during residency, the examiner who had seen my strengths and, more painfully, my hesitation.
He didn’t ask me the usual questions. No causes of splenomegaly. No management of DKA. He already knew what I knew.
He leaned back, looked at me for a long second, and asked the only question that mattered.
“So, Kalantri… you want to teach?”
“Yes, sir.”
“It is not the same as passing exams,” he said.
“I know, sir.”
That was it. A few more questions, a nod, and I was sent out.
When the result came, it was in my favour. On 1 July 1983, I signed the register as Lecturer in Medicine. I was twenty-six—barely older than the postgraduates I was supposed to guide.
The title changed overnight. The feeling didn’t. Inside, I still felt like a student who had wandered into the staff room.
***
The Morning I Nearly Failed Punctuality
If the interview tested my nerves, the first few months tested my timing.
Punctuality at MGIMS was not a good habit. It was a religion. And one Monday morning, I nearly became a sinner.
I had spent the weekend in Bhopal with my sister and returned by an overnight passenger train, confident I would make it comfortably for my 7 AM lecture to the 1979 batch.
Indian Railways had other plans.
The train rolled into Wardha East—today’s Sevagram station—at 6:35 AM.
I looked at my watch and felt my stomach drop. Twenty-five minutes. In that time I had to get home, wash up, change, and reach the college—six kilometres away.
I ran.
My mother met me at the door, alarmed by my face.
“Tea? Milk?” she asked.
“No time, Aai,” I said, already pulling off my travel shirt.
I splashed water on my face, threw on a clean khadi shirt and trousers, slipped into my sandals, and kicked my Priya to life. The scooter started on the first kick—one small mercy.
I was flying towards Sevagram when I saw it.
The railway crossing.
Gate down. Red light blinking. A long passenger train crawling through like it had all the time in the world.

I braked hard. Dust rose. My lecture began in ten minutes.
And then I saw a friend on the other side, waiting to go into Wardha. We locked eyes through the iron bars. He understood immediately.
“Swap?” I shouted.
“Swap!” he shouted back.
I left my Priya there, jumped the tracks like a thief, and ran across. His scooter was an old Lambretta—battered, noisy, and stubborn.
It groaned. It smoked. But it moved.
I drove that Lambretta as if my job depended on it. Maybe it did. The speedometer needle shook its way towards eighty. There were no helmets in those days, only youth and poor judgement.
I reached the college, parked, and sprinted to the lecture hall.
As I entered, the clock clicked to 7:00 AM.
The students looked up, mildly surprised, as if I had been dropped from the ceiling. I stood at the podium, caught my breath, picked up the chalk, and wrote the topic on the blackboard.
Only then did my heart slow down.
I had beaten the clock—by a whisker.
***
The Department of “P”s
The Department of Medicine in the early 1980s was not just a workplace. It was a small world with its own rules, its own hierarchy—and its own shorthand.
We called it the department of “P”s.
There was KP—Dr. Kamal Pervez.
There was JP—Dr. J.P. Sharma.
And now there was SP—me.
We were the junior lot. The foot soldiers. The ones who lived in the wards and carried the department on our backs, one admission at a time.
Above us sat the two peaks of the place: OP and AP.
Dr. O.P. Gupta was the sun around which everything revolved. He wore khadi like armour and arrived at 8:00 AM sharp. If you came at 8:05, you didn’t need a watch to know you were late. His eyebrow was enough.
He had an old-fashioned memory. He didn’t need the file to know the patient. He remembered the pulse rate from yesterday and the potassium from the day before.
Dr. A.P. Jain was the counterweight—precise, minimalist, and dangerously sharp. He moved through the ward like a detective, looking for what everyone else had missed: a soft murmur, a faint rash, a line in the history that didn’t fit.
And then there was Dr. Ulhas Jajoo—the conscience of the department. He reminded us, again and again, that illness did not come alone. It came with poverty, fear, and the cost of missing a day’s wage.
Together, they ran the department like a family—loving, demanding, and slightly terrifying.
***
The Tribunal
Every morning began with a ritual that taught us more than any textbook ever did.
ECG correction.
We gathered in the old hospital building—the former Birla guest house. The wooden floors creaked. The walls peeled. The place smelled of phenyl and old paper.
In a small room, the three of them sat together—Gupta, Jain, and Jajoo—like a bench of judges.
A resident would step forward holding a long strip of pink ECG paper, as if it were a confession.
“Read it,” Dr. Gupta would say.
The resident would begin, cautiously. “Sinus rhythm… rate 78…”
Dr. Jain would interrupt softly. “Look at V6 again. Is that a U wave or a P wave?”
And Dr. Jajoo would bring us back to earth. “You are reading a paper. Where is the patient in your thinking?”
There were no digital machines. No automated interpretations. No troponins. No quick CT scans to rescue you from doubt.
We had only our eyes, our ears, our stethoscope—and that strip of paper.
We dreaded that room some mornings. We also grew up in it.
Because in Sevagram, we learnt something simple and lasting: technology helps, but it doesn’t think. The doctor has to do that part.
And in the Department of “P”s, there was no escape from thinking.
The Call from Pavnar
On November 4, 1982, the calm of Pavnar Ashram broke. Acharya Vinoba Bhave had fallen ill. He was eighty-seven, and at that age even a “simple fever” makes everyone sit up a little straighter.
The message reached Sevagram quickly. Dr K.K. Trivedi, Dr O.P. Gupta, and Dr Ulhas Jajoo went across to examine him. They found him feverish and breathless, with a cough that would not settle. He was too weak to walk out of his room. Treatment began at once, but by afternoon it was clear this would not end with a couple of injections and a good night’s sleep.
Dr B.S. Chaubey was called from Nagpur. He examined Vinobaji carefully and said it could be pneumonia—or a pulmonary embolism. The next day, Dr Ashwin Mehta, the cardiologist from Bombay, arrived. Within hours, the ashram had more doctors than devotees, and a small “medical summit” formed almost on its own.
Everyone agreed on one thing: Vinobaji needed hospital care—Sevagram or Nagpur, anywhere with better support.
Vinobaji refused.
He would not leave Pavnar.
So we did the only thing left. If the patient wouldn’t come to the hospital, we took the hospital to the patient.
***
The ICU inside an ashram
A small room in the ashram became our makeshift ICU. Dr Chaubey chose two of us to stay there round the clock. I was one. The other was my colleague, Dr Ramesh Mundle.
We replaced Vinobaji’s simple wooden cot with a Fowler’s bed. We kept an IV stand ready. We arranged a tray with syringes, emergency medicines, and fluids. It looked like a hospital corner squeezed into a space meant for silence and prayer.
There were no monitors. No pulse oximeter. No alarms. We relied on the oldest tools in medicine—our eyes, our hands, and our stethoscopes. For ten days, Mundle and I lived in Pavnar, taking turns, sleeping in short bursts, waking at every change in breathing. We checked pulse, blood pressure, and temperature, and listened to his chest again and again, trying to decide whether the crackles were truly less—or only quieter.
For the first few days, we treated him aggressively. Penicillin for infection. Aminophylline to ease breathing. Heparin because we did not want to miss a clot. We also checked his urine for acetone—one of the simple ways we watched for starvation and metabolic trouble in those days.
Vinobaji lay there frail and bare-chested, ribs showing, beard flowing down like a white stream. His hearing had dulled, but his presence filled the room. Even when he spoke softly, people leaned in.
***
A brief recovery
By November 8, he looked better. His fever came down. His breathing eased. He was awake and attentive in that quiet way of his. That evening he took nourishment—milk, honey, paneer—measured in tolas, because the ashram recorded everything carefully.
It felt reassuring, almost like his body was telling us, I’m not done yet.
We relaxed a little. We stopped the glucose and saline, and told ourselves the worst had passed. That day Dada Dharmadhikari visited. Someone recited shlokas from the Gita and the Gitaai. Later, Rig Veda chants rose and fell in the room, steady as breathing.
For a few hours it felt like we were only doing our job—not standing at the edge of something larger.
***
The moment he chose
That night, something changed.
At 8:15 p.m., Jaidev—Jaisimha Rao, his close associate—brought him his usual glass of milk and honey. Vinobaji lifted his hand. Not in anger, not even in refusal the way we understand refusal. It was more like a man saying, gently, “Enough.”
We tried to persuade him. We told him he was improving, that the medicines were working, that he only needed a little more time. But he refused the milk. Then he refused the medicines. Then he refused water.
As doctors, we are trained to fight for life. That is what our hands are taught to do. That night, our hands had nothing to hold on to.
Vinobaji had decided on Prayopaveshan—a voluntary withdrawal from food and water, a deliberate departure. I had read about such things. I had never seen it up close. I certainly had not imagined I would be posted beside it.
***
Bulletins on a board
Once his decision became known, people began to arrive. Some were anxious, some curious, and some came as if this was a national event—which, in a way, it was.
We were asked to prepare daily health bulletins. Mundle and I wrote them by hand and pinned them outside the room, like school notices.
A few lines still stay with me. On 7 November, we wrote that his condition had improved, that pulse and blood pressure were stable, that he was conscious and taking milk and honey. On 9 November, we noted that he had stopped food, water, and medicines, and that this posed a serious threat. On 12 November, we wrote that he had taken nothing for 80 hours, and yet his condition had not worsened in the past ten hours.
It felt strange to write those sentences—clinical words for something that was not purely clinical.
***
When the body refused to behave
After a point, Vinobaji’s survival stopped obeying our textbooks. Even without intake, his urine output increased. The swelling in his feet disappeared. We kept checking for acetone. We found none.
I remember thinking—half in disbelief and half in irritation at my own ignorance—that this man’s body was not reading the same book as we were.
We were used to simple arithmetic. Three plus three is six. With Vinobaji, it felt like three plus three became eight.
On November 12, he pressed both ears with his hands and signalled pain. We cleaned his ears with glycerine, gave medicines, and waited, but the pain persisted.
I was young then. I had seen death in wards, in emergencies, in the ICU at Sevagram. But this was different. This was not death arriving.
This was death being invited in.
The Prime Minister at Pavnar
The morning after Vinobaji decided to stop food, water, and medicines, Pavnar changed colour. The ashram, usually held together by the soft rhythm of prayer and spinning, began to hum with another kind of energy—the kind that comes when important people arrive and everyone starts walking a little faster.
Mrs Indira Gandhi came that day. With her came Rajiv Gandhi, Babasaheb Bhosle, Vasant Sathe, Sitaram Kesri, and a small army of officials. Walking a respectful step behind was her personal physician, Dr K.P. Mathur. His presence made the situation feel even more serious.
When a Prime Minister brings her own doctor, you know the visit is not only political. It is personal.
Mrs Gandhi entered Vinobaji’s room quietly. She folded her hands, bowed, and touched his feet like a pilgrim. Vinobaji, frail but fully conscious, returned the greeting with a gentle namaskar.
For a moment the room felt strangely normal—an old man on a cot, a visitor on a mat, and a few doctors standing awkwardly at the edge.
“Baba,” she said softly, “at least take some water. Or a little fruit juice.”
Vinobaji lifted his hand. It was a small motion, almost mild, but it carried the finality of a decision that had already been made. No water. No juice. No medicines. No persuasion.
***
A lesson hidden in a breath
As Mrs Gandhi turned to speak to the doctors, Vinobaji called out in a thin voice, “Ram-Hari… Ram-Hari.”
She turned back at once.
He was showing her his breathing—slow, deliberate, almost rhythmic. He pressed his fingers against one nostril, inhaled to “Ram,” and exhaled to “Hari.” Even then, even in weakness, he was teaching. Not with words, but with breath.
Mrs Gandhi watched him closely, as if she had forgotten the crowd outside and the files waiting in Delhi. She nodded once, the way a student nods when something finally makes sense.
“Yes,” she said, “I will.”
I have seen many leaders up close over the years, but I have rarely seen one sit so still, so attentive, and so unprotected by power.
***
Lunch on the floor
She stayed for lunch.
The meal was the kind Pavnar served every day: roti with a little ghee, dal, rice, a boiled vegetable, curd, achar and chutney. There were no special arrangements, no separate plates, no “VIP food.” The ashram did not know how to flatter anyone, and Mrs Gandhi did not demand to be flattered.
When the meal ended, she stood up, picked up her own plate, and walked to the washing area. Then she washed it herself, calmly and thoroughly, as if she had done it all her life.
It was a small act, but it unsettled me. In medical college we were trained to stand up when a professor entered the room. Here was the Prime Minister of India washing her plate like an ashram inmate.
That image has stayed with me for decades, sharper than many speeches.
***
A young doctor speaks too honestly
Later, she asked the doctors to introduce themselves. She listened carefully, not distracted, not impatient. She asked a few questions about Vinobaji’s condition and our plan.
And then, almost inevitably, the conversation returned to the one thing we could not change: Vinobaji’s refusal.
I was young then, and still full of the medical instinct to fight. I had been trained to treat, to push, to rescue. Standing beside a patient who could recover if only he allowed us to help him felt like watching someone walk away from a bridge while you stood holding the rope.
“Madam,” I said, “he can live. But he doesn’t want to. As doctors, we are taught to save life. As a patient, he is choosing to leave it. What is the right thing to do?”
Mrs Gandhi looked at me for a moment. The political mask slipped away, and what remained was a woman who had seen enough of life to understand its limits.
“The patient’s wish comes first,” she said. “We may not agree, but we must respect it. Sometimes dignity matters more than the length of life.”
It was a lesson in ethics, delivered without a textbook and without drama. I remember feeling both relieved and defeated—the way you feel when someone tells you a truth you did not want to hear.
***
When the body stopped following rules
After that, the days tested our certainties.
Vinobaji pressed his ears with both hands, signalling pain. We tried cleaning his ears with glycerine. We tried medicines. We tried whatever little we had. The relief never lasted.
But the rest of his body behaved in ways that confused us. His urine output increased. The swelling in his feet disappeared. We tested his urine for acetone again and again, expecting starvation to show itself. Nothing.
As doctors, we like rules. We like patterns. We like predictable decline. Vinobaji’s body did not cooperate. It was as if the physiology had decided to obey a different master.
Standing by his bedside, I felt I was watching something I could not explain, and could not control.
***
Dr Sushila Nayar’s anger
Two days later, Dr Sushila Nayar came to Pavnar. She belonged to a different school of medicine—firm, fierce, and unwilling to watch a patient slip away if she believed he could be saved.
To her, inaction was almost a moral failure.
“This is not right,” she said, clearly upset. “He is not terminally ill. We cannot let him die of thirst.”
She took a glass of water and brought it to his lips herself. Vinobaji did not argue. He did not raise his voice. He simply brushed her hand away—gently, almost affectionately, but with the same steel we had seen from the first day.
His associates stood around him like silent guards. Not against us, but for him. They were there to protect his decision, even from doctors who meant well.
That day I understood something uncomfortable: a doctor can be helpless not only because the disease is stronger, but because the patient is.
***
A prediction we couldn’t chart
On the evening of November 14, we thought the end was near. His pulse felt like a tired thread. The blood pressure dropped and refused to rise. We looked at our notes, did our mental calculations, and prepared ourselves for the moment we knew was coming.
Then Radhakrishnaji—Gautam Bajaj’s father—walked in. He had been sleeping in a nearby room. He looked at Vinobaji and said, with complete certainty, “He will not go tonight. He will leave after 9:30 tomorrow morning. It will be Somvati Amavasya.”
We had our charts. He had his faith. And in that room, faith sounded strangely confident.
That night none of us slept.
***
9:30 a.m.
Morning came.
At 8 a.m., we gave Vinobaji a sponge bath with warm water. He remained conscious. His eyes followed us. He tried to sit up but could not. There was no panic, no pleading, no last-minute bargaining with the body.
At exactly 9:30 a.m., Vinoba Bhave’s heart stopped.
There was no shouting. No chest compressions. No desperate running around. Just a stillness that felt heavy and clean, the kind you feel after a long storm has passed.
He left the world the way he had lived—quietly, on his own terms.
***
From Moscow to Pavnar
The news reached Mrs Gandhi in Moscow, where she had gone for Leonid Brezhnev’s funeral. She returned immediately. The next morning she landed at Nagpur and flew by helicopter to Pavnar.
To avoid the crowd and the press, she entered from the back, walking past the goshala to the veranda where Vinobaji lay. She sat down near him and cried.
In that moment, the most powerful woman in India looked like a woman who had lost someone she deeply respected.
She did not make a speech. She did not turn it into a public moment. She simply sat there, quiet and human.
***
A funeral without spectacle
There was a suggestion to broadcast the funeral live on television. Vinobaji’s younger brother, Shivaji Bhave, refused. He also opposed covering the body with the tricolour.
“This is not a show,” he said firmly.
Mrs Gandhi accepted it without protest. The procession began, led not by priests or politicians, but by the women of the ashram, with Mahadevi Tai in front.
Vinobaji’s body lay on a simple bamboo stretcher, wrapped in white khadi and decorated with flowers. Mrs Gandhi walked with the ashram inmates to the Dham river. At the cremation ground, Mahadevi Tai lit the pyre.
Before leaving, Mrs Gandhi untied a small knot in the pallu of her sari, took out a piece of sandalwood she had carried, and placed it into the fire.
It was a Prime Minister’s offering, but it felt like something else—a private goodbye.
***
A note on memory (and power)
Years later, Arun Shourie came to Sevagram and asked me about those days. He was writing Preparing for Death. Dr K.P. Mathur wrote his account too. Others disagreed with him. Everyone remembered something different, as people always do.
Mathur’s version carries the view from close to power—security concerns, arrangements, and the small theatre that follows a Prime Minister. But at the bedside, the story felt different. The centre was not comfort or protocol. It was one man’s decision to stop.
I do not claim a monopoly over truth. But I know what I saw: a saint chose to step away, and the rest of us—doctors, politicians, devotees—had to learn how to step back.
In medical training, we are taught to act. That fortnight taught me the harder skill—to respect a patient’s choice, even when it breaks your professional reflex.
And I still remember Mrs Gandhi washing her plate. In that small act, she seemed to understand what we doctors were struggling to accept.
The VIP Trap
Can you imagine the confusion when a “VIP” patient lands in the ward—and the VIP happens to be the father of a doctor from the same department?
I saw it up close in 1983.
My father had been diabetic for nearly ten years. That week, he was admitted to our old medical ward on the ground floor—the building that now houses Community Medicine. He couldn’t swallow properly and wasn’t taking fluids. His blood sugars ran high and kept swinging. In those days we didn’t have fancy bedside glucometers. We adjusted treatment the old-fashioned way—by checking urine sugar again and again, sometimes six times a day.
I was a young lecturer in Medicine then, so I had easy access. After finishing my work, I would sit by his bed and do what sons do when they also happen to be doctors. I checked his urine sugar, wrote it down carefully, measured his blood pressure, looked at his nasogastric tube, and kept an eye on his neurological status. I tried to look calm, but inside I was constantly alert—listening for a change in his breathing, watching his face, waiting for some new trouble to announce itself.
For the first few days, I assumed things were running smoothly. Senior consultants came, spoke kindly, examined him, and moved on. Everyone seemed attentive. My father, too, felt reassured. He had always trusted doctors, and now three of them were hovering over him like guardian angels.
By the seventh day, I realised something odd.
My father had plenty of visitors, but no single doctor in charge.
Dr. O.P. Gupta thought Dr. A.P. Jain was looking after him because I worked closely with Dr. Jain. Dr. Jain assumed Ulhas was the main man because of our family bonds and his natural leadership. Ulhas, in turn, felt my father should technically be in Unit 1 because he had been admitted on Dr. Gupta’s admission day.
So my father was being seen by everyone—and owned by no one.
Every morning and evening, all three would still come. They stood at the bedside, glanced at the monitoring sheet, asked about the urine sugar, offered a few encouraging words, and walked away. Each visit looked like responsibility. In reality, it was shared goodwill floating without a centre.
It was VIP care in its most confusing form: extra attention, but unclear accountability.
I didn’t point it out to them. They were all senior to me, and I was still new enough to choose silence over argument. Besides, I knew how such conversations go—explanations, counter-explanations, and polite insistence that everything is under control. Meanwhile, the patient remains in limbo.
So I did what seemed simplest.
I took charge.
Once I felt my father was stable enough to go home, I discharged him myself. I filled the discharge card, assigned him to a unit on paper, wrote out his medicines, and brought him home.
He did well after that. The episode ended quietly, without drama—thankfully.
But it stayed with me.
It taught me that VIP treatment can be a strange thing. It looks like the best care, but it can create a fog—too many hands, too many good intentions, and no clear line of responsibility. And it reminded me of something basic that hospitals sometimes forget: kindness is important, but clarity is safer.
That week, my father recovered. I did too—though in a different way. I learnt, early in my career, that in medicine, everyone must know who is holding the rope.
The DNB Detour
In 1983, I suffered from a peculiar affliction common to young doctors: the "Alphabet Itch." I already possessed an MD, but I was convinced that unless I could trail a few more capital letters behind my name—like the tail of a stubborn kite—I would remain a medical lightweight. And so, I set my sights on the MNAMS (now known as the DNB). I imagined my future visiting card becoming quite the heavy-hitter in academic circles.
The theory papers in Bhopal went off with the breezy ease of a Sunday brunch. I felt invincible. But then came the practicals at Maulana Azad Medical College in Delhi.
***
Delhi, as any provincial doctor will tell you, is where egos are polished more frequently than stethoscopes. My assigned patient was a textbook case of a cervical cord tumor—or so I thought. I poked, prodded, and questioned the poor man with the precision of a detective. When I faced the external examiner, I was armed with facts and a dangerous amount of youthful certainty.
The examiner, a gentleman whose seniority was matched only by the stiffness of his collar, frowned. "The plantar reflex isn't up-going," he declared, peering over his spectacles as if I’d suggested the earth was flat. "Therefore, no cervical cord lesion."
Now, a sensible man would have nodded. He would have looked thoughtful, perhaps even slightly humbled, and made a strategic retreat. But I was intoxicated by clinical epidemiology. Instead of a graceful exit, I decided to "educate" him. I quoted literature. I stood my ground. I treated the viva like a debating society at Oxford rather than a high-stakes exam in a humid Delhi ward.
The examiner did not appreciate being "educated" by a candidate. He went silent. In a viva, silence isn't golden; it’s the sound of a guillotine being sharpened.
Only four out of thirteen passed that day. I was, quite predictably, left in the cold.
***
A few months later, the very same examiner turned up at Sevagram for our MD exams. He spotted me immediately. "Weren't you at MAMC recently?" he asked with a smile that was dangerously kind. "You were one of the best candidates," he whispered, "but you made one fatal error. Never bruise the examiner’s ego. In an exam room, the examiner is God—even if his theology is a bit rusty."
It was a delightful lesson in humility. I realized that medicine is fifty percent science and fifty percent reading the room. I didn't cry into my tea. I didn't declare it a tragedy. I simply filed the failure away like a misspelled lab report and went back to the wards.
In Sevagram, my patients were remarkably indifferent to my lack of a DNB tag. They didn't care about the alphabets; they cared if I showed up when they couldn't breathe, or if I could explain their heart failure in words that didn't require a Latin dictionary.
***
There is, however, a delicious postscript. My senior, Dr. A.P. Jain—a man twelve years my senior and a formidable unit head—had also secretly sneaked off to Bengaluru to take the same exam. He told no one. He, too, wanted the extra alphabets. It was only when the results came out that the truth emerged: he had failed as well.
Dr. Jain passed away a year ago, and I think he’d enjoy me sharing this now. We both failed. We both lived perfectly distinguished lives without those extra letters. It confirms my long-held suspicion that exams don’t actually select the best doctors; they merely select the best exam-takers. The rest of us are too busy actually practicing medicine.
Madras, October 1984
In October 1984, I travelled to Madras for a conference on Allergy and Immunology at Stanley Medical College. For me, it was a professional outing. For Bhavana, it was our first real trip together after marriage. We had been married barely eight months, and the excitement of travelling with your wife still feels new at that stage.
We took the Grand Trunk Express. It carried us steadily south, as if it had been doing this job for a hundred years and had no reason to hurry. When we reached Madras, the city greeted us with smells I still remember—jasmine in someone’s hair, sea air on the roads, and that unmistakable comfort of filter coffee.
The conference had its lectures and its slides, but my best memory from that trip came from outside the auditorium.
***
Maitreyan’s house, and the chapati struggle
I called my old friend from GMC Nagpur, Vasudevan Maitreyan. In those days he was studying Medical Oncology, fully absorbed in the world of cancer—quiet, serious, and hardworking. Later, he would enter politics and become a familiar name. But in 1984 he was simply Maitreyan—my batchmate, my friend, and someone I trusted.
He invited Bhavana and me home for dinner.
His family was Tamil Brahmin—rice, sambar, rasam, curd rice… the kind of food that arrives with its own rhythm. But they had decided to cook a North Indian meal for us. It was such a sweet idea, and such a difficult one.
In the kitchen, I watched his sisters wrestle with wheat dough. For us, chapatis are muscle memory. For them, it looked like a geometry problem. The dough stuck to their fingers. The circles came out like the map of a new country. They rolled, adjusted, tried again, and refused to give up.
When we finally sat down, they watched us closely—like examiners waiting for a viva answer.
“Is it okay?”
“Does it taste right?”
“Dal is fine?”
We ate with genuine pleasure and told them the truth: it was delicious. Not because it was “perfect North Indian food”, but because it was full of effort and affection. Those chapatis were not just bread. They were hospitality.
That evening, Maitreyan’s mother did something that stayed with us. Before we left, she performed a small aarti. She applied sindoor to Bhavana’s maang and tucked flowers into her hair—blessing her the way mothers do, without asking what language you speak.
We walked back to our hotel feeling strangely at home in a city that was still new to us.
***
October 31: when the city held its breath
The next morning, the mood changed.
We heard the news in fragments first, and then clearly enough to believe it: Indira Gandhi had been assassinated.
Only two years earlier, I had seen her at Pavnar, sitting near Vinobaji with quiet respect. I remembered her stillness, her seriousness, the way she seemed fully present in that room. It felt impossible that she could be gone.
The conference ended abruptly. Madras, usually busy and noisy, turned into a different place. Shops shut. Streets emptied. Even the air felt cautious. It wasn’t panic. It was a kind of stunned silence.
Bhavana and I stayed inside our hotel room. This was long before mobile phones. Trunk calls were a struggle on normal days. In those days, they were nearly impossible. We could not reach Wardha. We could not reassure our families. We sat with the radio and listened, waiting for facts, receiving rumours.
And rumours, as you know, are never gentle.
We heard about violence in the North. About Sikhs being attacked. About trains being stopped. About mobs. We were in the South, far away from the worst of it, but distance doesn’t protect you from fear. It only adds helplessness to it.
On the third day, we stepped out for a short walk, hoping the city had returned to itself. It hadn’t. The roads still looked drained of life. We came back quickly, as if the hotel room was the only safe address we had.
***
The long ride back
After a few days, trains began running again. We got seats on the GT Express back towards Nagpur.
Normally, a long train journey in India has its own comfort—vendors shouting, children running, someone offering you a banana for no reason. This time, the compartments stayed tense. When the train slowed down between stations, people fell quiet and looked out of the windows with suspicion, as if the fields could suddenly produce trouble.
Nothing happened. But the fear travelled with us, sitting quietly in the corner.
When we finally reached Wardha, I felt relief in my bones. We had come back to familiar roads, familiar faces, and the simple comfort of being able to tell our families: we are safe.
That trip gave me two memories that don’t sit easily together—chapatis made with love, and a city going silent overnight. Madras offered both. And somehow, both stayed.
A Research Odyssey
Strange as it may sound, my entry into medical writing did not begin with a grand hypothesis or a randomized trial. It began with a single sheet of paper—and a young boy with an unusual collarbone.
It was 1986. I had finished my MD five years earlier and had just been promoted as Reader in Medicine at MGIMS. A case report we had written—“Cleidocranial Dysostosis with Grand Mal Epilepsy”—was published in the Indian Journal of Radiology and Imaging.
To be honest, the paper was less my brainchild and more an accident of geography and seniority. I happened to be present, reasonably literate, and the youngest man in the room who could be trusted with a typewriter. The real engine was Dr. Sharad Pendsey.
***
Dr. Pendsey was my senior from the 1971 batch at GMC Nagpur. Even back in my house-officer days, he was a man who had quietly carved out a unique reputation. Long before "super-specialist" became a fashionable label for visiting cards, he was perhaps the first physician in Central India to dedicate his practice exclusively to diabetology.
He found his true calling in treating children—young lives that revolved around the relentless cycle of syringes and glucose charts. He stood as a guardian for these families, providing insulin that often cost far more than they could comfortably afford.
While he had a flair for the dramatic and showcased his research at international conferences, he was equally at home in the modern era, remaining active on social media to share his knowledge. Yet, beneath the accolades and the public presence, he was a man of discipline; he simply showed up every day and did the work.
Dr. Pendsey’s presence was as striking as his medical reputation. With his remarkably fair skin and a distinctive tuft of hair, he possessed the charisma of a Bollywood leading man. But it was his eyes that truly defined him—large, expressive, and perpetually dancing with a mischievous glint, as if he were sharing a private joke with the world.
He was a man of two worlds. On the international stage, he was the consummate professional, conducting himself with a polished grace that earned the respect of global peers. Yet, the moment he stepped back into the clinic, that sophistication transformed into a deep, grounded empathy.
For Dr. Pendsey, diabetology was not just about managing numbers; it was a crusade for the quality of life. He fought a tireless battle against the cruelest complications of the disease. He devoted his skill and heart to saving a patient’s limb from amputation, protecting a child's sight from blindness, and guarding fragile kidneys against failure. To his patients, he wasn't just a "super-specialist"—he was the hero who stood between them and a lifetime of disability.
When he passed away from stomach cancer in 2023, the loss felt premature. He was a pioneer who still had much to give, and he left us all a bit too early.
***
My own contribution to the paper was modest: I searched and manged to get the patient's x-ray from the Radiology department, located references, corrected commas, and nodded wisely. In academia, this level of participation is sometimes enough to earn authorship.
When the reprints arrived—ten crisp pairs wrapped in brown paper—they felt absurdly grand, like contraband or a government secret. I slit the packet open with unnecessary ceremony. Inside lay our names in print, black and permanent. I must confess my heart beat faster.
I examined each copy the way a child inspects a new cricket bat, or, more accurately these days, the way people in India open Amazon parcels—with suspicion first, then delight, and finally the quiet calculation of whom to show it to. I smoothed the pages, admired the typesetting, and briefly entertained the dangerous illusion that I had produced something of consequence.
For a few minutes, I was not a junior doctor with ink-stained fingers. I was, unmistakably, an author.
Then the ward bell rang, and reality resumed.
My name sat at the end of a list of six authors. Not exactly the stuff of legends. But holding those reprints in my hands, I felt something shift. The ward work we did every day could live beyond the bedside. It could travel.
And it could stay.
***
Before journals, the bulletin (late 1980s–early 1990s)
For the next decade, my “research output” looked different from what people usually mean by research.
I wrote more for the MFC Bulletin (Medico Friend Circle) and the local press than for indexed journals. The topics were not glamorous—rational use of drugs, the political economy of health, and the everyday unfairness of rural medical care.
These pieces were not peer-reviewed in the strict sense, but they taught me something important: how to look at medicine with my eyes open. They trained me to ask why things happen, not just what happens.
In those years, I did not have sophisticated tools. But I was learning to think.
***
The pivot: McMaster, Berkeley, and a new lens
The real change came in the mid-1990s, when I was exposed to McMaster University and later did my MPH at UC Berkeley.
Until then, like many doctors of my generation, I practised a lot of what can politely be called eminence-based medicine—you trust your teachers, you trust the textbook, and you hope your experience fills the gaps.
McMaster and Berkeley introduced me to evidence-based medicine and clinical epidemiology. It was exciting—and slightly unsettling. Suddenly, “common sense” was not enough. A hunch needed proof. A treatment needed outcomes, not reputation.
I returned to Sevagram with a different kind of confidence. Not the loud kind. The quiet kind that comes from knowing how to ask a question properly—and how to test the answer.
***
A simple rule: give students the credit
Back home, I realised one thing quickly: research in Sevagram could not be a solo hobby. It had to become a habit. A culture.
I began guiding a large number of residents for their MD theses. In many medical colleges, a thesis becomes a heavy file that nobody reads again. I wanted ours to become something else—a piece of work that could stand outside the examination hall.
We chose questions that grew out of daily practice:
Does this clinical sign really predict pneumonia?
How accurate is this rapid test for malaria?
What puts rural Indians at risk for heart attacks?
We did diagnostic accuracy studies, risk factor work, and prognostic studies. But just as important as the methods was the ethics of authorship.
My friend and collaborator Madhukar Pai gave me a rule that stayed with me: the student does the work, the student gets the credit.
So the resident became the first author. I stayed in the background as corresponding author. Watching young doctors see their names in print—often for the first time—gave me a satisfaction that no “impact factor” can match.
***
When Sevagram entered big trials
In the early 2000s, the horizon widened again.
MGIMS became part of major international collaborations led by Dr Salim Yusuf and the Population Health Research Institute, through colleagues like Dr Prem Pais and Dr Denis Xavier at St John’s, Bangalore.
It was a leap of faith. Could a rural hospital in Vidarbha match the discipline and documentation required for multicentric global trials?
We proved we could.
We contributed to studies like INTERHEART, INTERSTROKE, and POISE. What pleased me most was not the prestige. It was the thought that data from our patients—farmers, labourers, housewives—was helping shape global understanding of disease.
Wardha was quietly entering the textbooks.
***
The people behind the papers
No research journey is a one-man show. Mine certainly wasn’t.
Two collaborators shaped my work deeply: Rajnish Joshi and Madhukar Pai.
Rajnish was my student from the 1992 batch. Over time, the teacher-student line faded. He went on to Berkeley for his MPH and later a PhD, and eventually we worked as colleagues. Watching his growth—from Sevagram to global health—felt personal, like seeing your own story rewritten in a sharper script.
With Madhu, I entered the world of tuberculosis research and “clinical operations research”—not only asking does it work? but also can it reach the patient who needs it? Some of that work contributed to questioning—and eventually stopping—the use of inaccurate TB serology tests. That felt like research doing its real job: protecting people from bad medicine.
***
What I see when I look back
Today, if I look at my PubMed list, it looks like a tidy record—titles, journals, years.
But I don’t see it that way.
I see residents collecting data late at night, fighting sleep and ward chaos. I see patients in Kasturba Hospital allowing us to learn from their illness, without ever asking what they would get in return. I see long email threads with co-authors debating one line in a table as if it were a life-and-death decision.
My research journey began with a case report of a boy with a collarbone defect.
It grew into something larger—a way of thinking, a way of teaching, and a way of staying honest in medicine.
And it taught me one lasting lesson: if you listen carefully at the bedside, the paper almost writes itself.
Guten Tag, Sevagram
In 1987, for reasons I can no longer explain with a straight face, I decided to learn German. I had no plans to travel. No professional need. Perhaps I just wanted a small escape from the daily cycle of rounds, case sheets, and prescriptions. Or maybe I wanted to prove to myself that my brain could still do something new.
Learning a foreign language in Wardha in those days was not exactly fashionable. We lived comfortably with Marathi and Hindi, and we managed our medical English as best as we could. Deutsch felt as distant as snowfall. But Wardha has its own way of surprising you.
Mrs. Sunita Kawale, the wife of the District Collector, had moved to Wardha. She was a linguist, fluent in German, and she agreed to teach.
A class of one sounded depressing, so I did what every enthusiastic beginner does—I recruited others. Dr. Sudha Jain and Dr. Anjali Ingle from Anaesthesiology joined in. Monika Ahuja, an intern with a sharp mind, signed up too. So did Parthak Pradhan and Ganesh Srinivasan, two third-year students who were always ready for anything that wasn’t PSM.
***
The J-Y Problem
We committed ourselves to a six-month course. Three evenings a week—Monday, Wednesday, Friday—we gathered in the Medicine seminar room. Outside, Wardha baked. Inside, we tried to sound like people from Berlin.
Grammar was manageable. Pronunciation was the real enemy.
The letter J, we discovered, behaved badly. In German it softened into a Y, which created an identity crisis for half our department. “Jajoo” became “Yayoo.” “Jain” turned into “Yen.” We said these names with great sincerity, and then collapsed laughing.
And then came the dreaded ü. We sat pursing our lips like we were trying to whistle without knowing how. The sounds we produced were somewhere between a groan and a complaint. Mrs. Kawale stayed calm through it all. She corrected us gently, as if she had been trained for this in Germany too.
***
The Exam That Made It Real
Despite the comedy, we took the classes seriously. In May 1987, I appeared for the examination conducted by Max Mueller Bhavan, the Indian arm of the Goethe Institute. I still remember the small thrill of seeing my score.
84 out of 100.
That number made me greedy. I enrolled for the advanced course. This was no longer about memorising words. It was about speaking without panicking.
An external examiner came for the final assessment by the Deutscher Volkshochschul-Verband (DVV). The oral exam was the hardest. I spoke in careful sentences, like a man walking on a freshly mopped floor. Somehow, it worked. I scored 64 out of 90 in theory and 22 out of 30 in the oral. In December 1987, I was officially declared passed.
***
Germany Came to Sevagram
None of us went to Germany after that. We stayed exactly where we were—firmly in central India, with our wards, our patients, and our familiar dust.
Still, the effort wasn’t wasted. Learning a new language opens a window in the mind. It freshens the air. It also gives you the quiet satisfaction of doing something difficult just because you wanted to.
And it gave me a small party trick.
Kasturba Hospital had a few senior nurses who had trained in Germany years earlier—efficient, stern, and impossible to impress. Once in a while, I would walk up to the nursing station and drop a sentence in German.
“Guten Morgen, Schwester. Wie geht es Ihnen?”
The first reaction was always shock. Then came a smile—quick, genuine, almost childlike. For a moment, the usual doctor–nurse distance softened. We became two people connected by a language that had no business being in Sevagram.
We never went to Germany.
But for a few evenings in 1987, Germany came to us.
Sevagram, Permanently
In December 1987—exactly a year after my father passed away—Bhavana and I decided to change the map of our lives. We moved out of the familiar comfort of Jaishree Bhavan in Wardha and into the MGIMS campus at Sevagram. It wasn’t a grand leap. It was a quiet shift. But it changed everything that came after.
We were allotted Flat No. 13, first floor, in the “Type 2” quarters near Kasturba Vidya Mandir. Two bedrooms, a small drawing room, and a kitchen that quickly became the busiest room in the house. We didn’t own much then, so the move was almost embarrassingly easy. One truck, a few steel trunks, and we were done.
To set up our new kitchen, I took my seventeen-year-old niece, Surekha, on my scooter to Sitabuldi in Nagpur. We returned like proud hunters with our trophies: a gas stove, a Sumeet mixer-grinder, and a 165-litre Kelvinator refrigerator. Soon after, a black-and-white Digichrome television arrived. Ulhas Jajoo and Mr. C.B. Taori helped coordinate it, as if buying a TV was a public health programme that needed teamwork and planning.
Once we settled in, colony life took over—quickly and completely. We were surrounded by young lecturers: Dr. Ramji Singh, Dr. Mendiratta, Dr. Ajay Agrawal, and many others whose doors stayed open more often than closed. Privacy existed, but it wasn’t treated as a sacred right. In a two-minute walk you could meet twenty people you knew, and if you looked even slightly troubled, someone would ask, “Kya hua?”
Evenings had their own rhythm. Badminton in the open, cups of coffee that never stayed hot, and snacks that travelled from one house to another without needing permission. Birthdays were not private family affairs. They were community events. One child blew the candles, and the whole block ate cake.
***
The Malgudi of Sevagram
Sevagram was a village, but our colony felt like a little town square. It had its own characters—warm, quirky, and unforgettable—people who could have walked straight out of an R.K. Narayan story.
Dr. K.K. Ghuliani, Head of Community Medicine, became our next-door neighbour when we shifted to Vivekanand Colony in 1989. In the department he looked stern, almost military. Students feared his punctuality more than exams. But at home he was a different man—easy, affectionate, and addicted to Scrabble. Many evenings ended with him grinning over a triple-word score while the rest of us protested like injured parties.
His wife, Mohini, held the colony together in ways no official circular ever could. She taught flower decoration and knitting, organised children’s programmes at the staff club, and somehow made every gathering feel like a family event, even when half the people were meeting for the first time.
Then there was Dr. R.S. Naik from Forensic Medicine—a paradox if there ever was one. He worked with death all day, yet he carried the liveliest spirit on campus. As warden of the boys’ hostel, he followed one simple philosophy: “Boys will be boys.” And since this was the pre-cable-TV era, he started a Cine Club. Every weekend, films were screened, and the hostel boys got their dose of Bollywood, romance, and noise—exactly what young men need when they are stuck in a rural campus with too much study and too little distraction.
***
Lali, Kali, and the Director
But the most eccentric—and most loved—were Dr. Samit Kumar Ghosh and his wife, Laxmi. Dr. Ghosh, our Professor of Anatomy, lived with three passions: dissection, gardening, and dogs. He spoke English in a rich Bengali accent and carried a temperament that could switch from thunder to tenderness without warning.
The Ghosh household didn’t “keep pets.” They had family members who happened to be dogs.
They had adopted two street dogs and named them Lali and Kali, based on their coats. These weren’t dogs who slept outside. They slept on the bed, ate home food, and were spoken to in Bengali like small children who refused to study.
One Sunday morning, the colony woke up to a crisis. Lali and Kali were missing.
Mrs. Ghosh rushed out in panic—hair uncombed, an informal house gown, and a big red bindi that announced she meant business. She stopped a passer-by and demanded, “Excuse me! Have you seen Lali and Kali?”
The man was Dhirubhai—the formidable Director of the institute. He stared at her blankly. Lali and Kali sounded like nieces, or granddaughters, or maybe two important VIPs he was expected to recognise. When she explained they were dogs, his expression shifted from confusion to alarm. He muttered something, shook his head, and escaped before he could be recruited into a search party.
Years later, when Dr. Ghosh moved to Kolkata, their devotion reached another level. They booked a special carriage on the Mumbai–Kolkata Mail for Lali, paying a handsome sum, while Kali travelled by car. They were not dogs, after all. They were Sevagram royalty.
***
A dent in the car, a lump in the throat
Dr. Ghosh could be fiery, but he also surprised you when you least expected it.
In 1999, we bought a second-hand Maruti 800. Bhavana was learning to drive, while managing her job in the IT department, two children, and the daily chaos that runs every Indian home. One Sunday morning, while reversing out of the driveway, she misjudged the angle.
Crunch.
Our car hit Dr. Ghosh’s shiny, well-kept vehicle. A dent appeared—clear, ugly, and impossible to hide.
Bhavana froze. She knew Dr. Ghosh’s temper. She imagined the shouting, the humiliation, the long lecture that would follow. Still, she walked to his door and confessed.
Dr. Ghosh came out, looked at the dent, then looked at Bhavana standing there with her head slightly bowed, waiting for the blast.
Instead, he turned to me.
“Kalantri!” he said sharply. “Why are you not helping her more?”
I stood stunned.
Then his voice softened as he spoke to Bhavana. “It is not your fault. Reversing is difficult. You are doing too much.”
He looked back at me. “She is managing home, children, job. You must share the load. Shoulder her burden.”
And with a casual wave of his hand, he dismissed the dent as if it was a mosquito bite.
Bhavana came back home with tears in her eyes—not from fear, but from relief. The car had a dent. But what stayed was something else: the unexpected kindness of a man who could have shouted, but chose to protect.
***
Amrita arrives—and Ashwini finds a tail
In October 1989, we moved to the first floor of Vivekanand Colony. Soon after, Bhavana went into labour. It was 10 p.m., and the hospital was barely five minutes away on foot. Dr. Chhabra arrived quickly, and within an hour, our daughter Amrita was born.
Ashwini, then three and a half, was thrilled. Outside the labour ward he met Dr. Anuradha Gokarn, a house officer who was engaged to her batchmate, Fali Langdana. In a playful mood, she asked him about a recent staff club party.
“What did you do at the party?” she asked.
“I became Lord Hanuman!” Ashwini announced.
“But you don’t have a tail,” she teased. “How did you become Hanuman without a tail?”
Ashwini looked at her as if the answer was obvious.
“Oh, that was easy,” he said. “I used Phali for the tail.”
He meant the long bean vegetable—phali. But Dr. Anuradha burst out laughing. The thought of her fiancé, Fali, being used as a tail in a toddler’s costume was too funny to resist.
That’s how those years felt: small homes, open doors, shared laughter, and the comforting noise of neighbours who slowly became family.
We moved to Sevagram thinking we were only changing our address.
We didn’t realise we were also choosing our people.
The Kitchen Surgeon
1990 began with a small disaster. In January, only a few months after Amrita was born, I injured my foot. A large, angry wound appeared on the top of it. Walking hurt. Shoes were out of the question.
It got bad enough for me to do something I almost never did—apply for ten days of earned leave.
I stayed home in Vivekanand Colony, sulking a little and limping a lot. The wound needed daily dressing, and I needed antibiotics. My friend, Dr Suhas Jajoo—the surgeon we all trusted—had shifted his practice to Wardha town. It was only a few kilometres away, but with a throbbing foot it might as well have been another district.
Suhas gave me a simple plan over the phone.
“Gentamicin. Ten injections. Twice a day for five days.”
Simple plan. Difficult execution.
***
The Unlikely Nurse
The question was: who would give the injections?
I couldn’t go to the hospital twice a day. Calling a nurse home morning and evening felt excessive—and frankly, embarrassing. I was a doctor. I should have managed my own foot better.
That’s when Bhavana said, quite calmly, “I’ll do it.”
I looked at her as if she had offered to perform a bypass surgery after making tea.
She had no medical training. She had never held a syringe. At home she already had her hands full—Ashwini was three, and Amrita was barely three months old. But she didn’t hesitate. Not once.
In those days we still used glass syringes. She boiled the syringe and needle like she was sterilising kitchen vessels. She snapped open the Gentamicin ampoule, drew the medicine carefully, and walked towards me with a seriousness that made me sit up straight.
I was the patient now, and suddenly very obedient.
***
Kitchen Confidence
I stretched my arm out on the bed, trying to look brave. Inside, I was praying silently: Please don’t miss the vein.
Bhavana tied the tourniquet. She tapped gently. She looked once, then slid the needle in—quick and clean.
I watched her pull back the plunger. A flash of blood appeared in the barrel.
She was in.
She pushed the medicine slowly, withdrew the needle, and pressed cotton over the spot like she had been doing this all her life. I exhaled. Only then did I realise I had been holding my breath.
“How did you do that?” I asked. “You’ve never done it before.”
Bhavana shrugged, as if I was being dramatic.
“Oh, please,” she said. “We women do harder things in the kitchen every day. Finding a vein is easier than making a perfectly round chapati.”
For five days she gave me all ten injections. She didn’t miss once. No swelling. No bruising. No drama.
My foot healed. But what stayed with me was her steady hand—and the quiet confidence behind it. I had married a woman who could run a home, raise two small children, and still teach a doctor a thing or two about courage.
And she did it without asking for a certificate.
The Rhythm and the Record
In the early decades of MGIMS, the Department of Medicine rested not on titles but on temperament. Two men—Kiran Munjewar and Sudhakar Bijewar—carried no MD degrees after their names, yet the wards leaned on them the way an old house leans on its central beams. If they were absent, the place felt slightly unstable, as though a screw had come loose somewhere.
They had arrived when the institute was young and stayed long enough to grow old with it. As a resident, I depended on them without knowing it; as faculty, I depended on them knowingly. They were always present—on Sundays, on Diwali afternoons, during monsoon nights when the power failed and the generator coughed into life. They did not speak of dedication. They simply reported for duty and began work.
In a hospital that loved meetings and memos, they believed in neither. Their loyalty was to the next patient, the next strip of paper, the next slide under the microscope.
***
The ECG Room and the Earthing Ritual
If you mentioned an ECG anywhere in Sevagram, someone would say, “Ask Munjewar.”
The ECG room was small, warm, and faintly metallic in smell, like overheated wiring. In one corner stood the old BPL single-channel machine—cream-coloured, heavy, and stubbornly reliable. It did not forgive carelessness. A clean tracing required patience, good earthing, and a steady hand.
Munjewar treated that machine the way a priest treats an altar.
Before every recording he went through a quiet ritual. The green earthing wire was clipped firmly to a water pipe or sometimes to a copper rod pushed deep into the soil outside the window. The patient’s skin was rubbed with spirit until it shone. The brass electrodes were pressed down carefully, as though he were persuading them, not forcing them.
Then he waited.
If the patient was anxious, the baseline trembled. So he would rest a hand lightly on the patient’s shoulder and talk about something ordinary—how far the village was, whether the crops had survived the rain, whether the bus had been crowded. The heart rate would slow. The line would settle.
Only then would the stylus begin its slow, scratching journey across the thermal paper, burning the rhythm into a grid with a soft skritch-skritch sound.
Today machines interpret and print diagnoses in bold letters. Munjewar interpreted faces first, then hearts.
***
Geometry, Not Waste
Paper, to him, was not expendable.
Where a young resident might waste half a roll waiting for the leads to settle, Munjewar moved through them with quiet precision—I, II, III, then the augmented leads, then the chest leads—each switch timed so perfectly that the entire twelve-lead ECG fit into half the length we would normally use. Watching him was like watching a tailor cut cloth without leaving scraps.
He could spot trouble before the rest of us found our pens. A faint ST depression, a shy heart block, an evolving infarct—he would tap the strip and say, “Something is changing here,” and nine times out of ten he was right.
Over the years he must have recorded hundreds of thousands of ECGs. The P waves and QRS complexes were not abstractions to him; they were old acquaintances.
***
The Side Lab Republic
If the ECG room belonged to Munjewar, the side laboratory belonged to Bijewar.
It was a cramped, dim room that smelt permanently of stain, spirit, and warm glass. No automation, no screens, no reassuring beeps. Just benches, microscopes, slides, bottles with handwritten labels, and residents who learnt quickly or suffered.
Every Medicine resident passed through that room like a rite of passage.
Residents estimated haemoglobin with Sahli’s tubes, squinting to match colours. They made smears by hand and hunted for parasites under oil immersion until their eyes watered. When a patient came in with suspected meningitis, they did not wait for a central lab report. They carried the CSF straight here, counted the cells ourselves, and made decisions on the spot.
Medicine, stripped of glamour, looked like this: stained fingers, bent backs, and the smell of Leishman’s dye.
Bijewar ruled this republic with quiet authority.
***
The Gospel of Frugality
He believed waste was a moral failure.
To ask for an extra slide invited interrogation. “Why two?” his raised eyebrow seemed to ask. “One is enough if you know what you’re doing.” Coverslips were washed and reused. Reagents were measured like precious medicine.
If someone spilled stain or used too much Benedict’s solution, he noticed. He never scolded loudly. The reckoning came later, in a soft voice, with accounts demanded like a shopkeeper balancing a ledger.
At the time we found it excessive. Later, working in resource-poor settings, we understood that he had been teaching us something more important than thrift. He was teaching respect—for material, for labour, for the small economies that keep a rural hospital alive.
Clinical excellence, he seemed to say, begins with not wasting what you have.
***
The Great Purge
Around the year 2000, when we were converting the old ward into an ICU, I decided that the Medicine office needed cleaning. “Cleaning,” I imagined, meant order. To Bijewar, it meant catastrophe.
The office had become a geological site. Files from the 1970s lay under files from the 1980s. Leave applications from doctors who had long retired slept peacefully beside circulars announcing Independence Day celebrations from another century.
One Sunday morning I gathered a group of residents. Sleeves rolled up, we attacked the room with revolutionary enthusiasm. Old forms, yellowed notices, ancient mark sheets—out they went. For three hours we cleared, dusted, rearranged, and admired the sudden space as though we had discovered land.
On Monday at nine, Bijewar walked in.
He stopped at the door.
His eyes scanned the shelves the way a man scans the aftermath of a burglary. “Where are the files?” he asked quietly. To us they had been junk. To him they were history, proof, continuity—the paper memory of the department.
There was a brief protest, a small lament for vanished documents, and then acceptance. But for days he handled the new shelves like a man learning to live in a house rebuilt overnight.
We called it decluttering. He probably called it vandalism.
***
What Remains
Today both men have slowed. Age has done what administrators never could.
Bijewar walks carefully now, Parkinson’s and osteoarthritis negotiating each step, yet the old half-smile survives. Munjewar spends his mornings in his garden, coaxing tomatoes into ripeness with the same patience he once used on anxious patients.
When I meet them, we speak of ordinary things. They never list achievements. But whenever I look at a clean ECG or a neatly prepared slide, I see their handwriting.
Machines today are faster, cleverer, almost arrogant. They announce diagnoses before we think. Yet sometimes, standing in a modern ICU full of screens and algorithms, I miss those two men and their deliberate ways—the careful folding of a strip, the measured drop of stain, the sense that tools deserve respect.
They did not merely record rhythms or count cells. They taught us how to practise medicine without noise, without waste, and without drama.
The department still stands on the foundations they laid, though most of us realised it only after they had quietly stepped aside.
Taking the Helm
By February 1993, I had been an MD for nearly a decade. In medicine, ten years is a long time to remain the fellow who is always “helping” and never quite leading. I was a Reader in Medicine by then—experienced enough to know my way around the wards, yet still functioning as a dependable second-in-command.
The work was steady. The days were full. But somewhere inside, a small restlessness had begun to tap its foot.
The turning point came at a wedding, not in a ward. I was in Pune for the wedding of Sujata Bajaj—Radhakrishnaji Bajaj’s daughter—to Rune Larson. It was February 1993. The hall was buzzing in that familiar Indian way: loud greetings, relatives searching for chairs, photographers shouting instructions, and people eating as if the baraat might snatch away the food.
In the middle of that cheerful chaos, I found a quiet moment with Mr. Dhirubhai Mehta. He had joined the Kasturba Health Society in 1982 and had the rare ability to understand both files and feelings. I decided to be honest with him.
“Dhirubhai,” I said, “I’ve been here for years. I have the degree and the experience. But I’m still working in someone else’s shadow, and it is slowly dampening my zeal. If I don’t get the independence to run a unit, I fear I’ll stop growing.”
He listened without interrupting, the way good administrators sometimes do—silently, but with attention. He didn’t promise anything. He didn’t even say much. But I had a feeling he had heard me properly.
A few weeks later, back in Sevagram, the wheels began to turn.
On March 1, 1993, a notice appeared on the department board: a new unit was being created for me. For a few seconds I felt relieved, almost boyishly pleased. Finally, I thought, a unit of my own.
Then I read the rest.
The administration had divided the department into “Major” and “Minor” units. Units I and II were given two OPD days each. Units III and IV—the newer units—were given only one OPD day each. On paper, it was just a timetable. In real life, it meant something else. In a teaching hospital, patients are our textbooks. Fewer OPD days meant fewer patients, fewer discussions, fewer opportunities for residents to learn by seeing and doing.
A “minor unit” was not a minor thing.
There was another line that made me uncomfortable. The notice said I would share OPD duties with Dr. Ulhas Jajoo—my senior colleague and close friend. To accommodate this new arrangement, Ulhas had been asked to give up one of his OPD days. I stared at the notice for a while, hoping it would rewrite itself out of politeness.
It didn’t.
It felt unfair in two ways. My unit would start with less clinical material, and Ulhas would lose a day despite years of service. I knew the intention was not unkind. It was simply the usual administrative jugglery—three balls in the air and one landing on someone’s head.
I could have accepted it quietly. Many people would have. After all, even a “minor unit” was better than none. But I also knew that if I began my independence by accepting something that didn’t feel right, I would spend the rest of my career adjusting and compromising, and calling it maturity.
That evening, I went home and pulled out my Brother portable typewriter. Its clack-clack-clack filled the room, making my protest sound louder than it actually was. I wrote to our Head of the Department, Dr. O.P. Gupta. I kept the tone respectful and the argument simple. I said the “Major–Minor” divide would breed resentment among junior faculty and create second-class units inside the same department. I also wrote clearly that Ulhas did not deserve to lose an OPD day after serving the institute for so long.
Then I suggested a solution that even a tired resident could understand: distribute OPD and indoor work equally across all four units.
After I signed the letter, I sat for a moment, feeling my heartbeat a little too loud for a man who had only typed a page. In medical colleges, questioning a notice is not considered a hobby. It is treated like a mild infection—people watch it carefully.
To my surprise, Dr. Gupta did not take offence. He did not call me in for a scolding, and he did not make me feel like an overconfident junior. He did something far better. That very day, he withdrew the earlier notice and issued a revised one. The “Major” and “Minor” labels disappeared. The work was redistributed evenly. And I was given full independent charge.
My OPD days were fixed: Monday and Thursday. My emergency duty was set for Thursdays and every fourth and fifth Sunday of the month. I read the new roster twice, as if it might vanish if I blinked too hard. It didn’t.
That evening I felt something loosen inside me. I wasn’t just relieved. I was quietly grateful—first to Dhirubhai for listening, and then to Dr. Gupta for responding with fairness instead of ego.
I also learnt a small professional lesson that has stayed with me: competence is important, but sometimes you must speak up—politely, clearly, and on time. If I hadn’t spoken in Pune, and if I hadn’t typed that letter in Sevagram, I would probably have continued doing my work with a smile on the face and a grumble in the heart.
Instead, I finally had a unit of my own to run—and no reason to keep looking over my shoulder.
The Press Near Rajkala Talkies

My first tryst with printing was in 1986, when I began helping edit the MFC Bulletin. The articles arrived by post — most handwritten in varying degrees of legibility, a few badly typed on manual typewriters with faded ribbons, the letters uneven, the margins ignored. My job was to collect them, mark them up, and take them personally to Samyayog Press in Wardha, near Rajkala Talkies, on my scooter.
Shri Tukaram Chaudhari managed the press. He wore a spotless Gandhi shirt and dhoti, a Gandhi cap placed squarely on his head, and carried himself with the quiet discipline of a man who believed that a clean uniform and a clean proof sheet were equally important. He was unhurried, courteous, and entirely unimpressed by titles. A Professor of Medicine from the hospital up the road was, to him, simply another person who needed a job done correctly.
He had a small team of boys, each one trained in a specific task. One handled the type-setting — picking individual metal letters from the shallow wooden trays and assembling them by hand into words and lines. Another managed the inking — rolling a brayer evenly across the assembled type to coat every raised surface with a thin film of black ink. A third operated the press itself, feeding sheets of paper with a careful precision that came from doing it a thousand times. A fourth handled the proofing — peeling back each freshly printed sheet, holding it to the light, looking for the letter that had shifted, the line that had slipped, the word that had come out faint because the ink had run thin. Together they moved through the room with the practised ease of a surgical team — each knowing his role, each trusting the others to do theirs.
Watching him was like watching a man knit. There was the same repetitive rhythm, the same unhurried confidence, the same quiet that comes from doing one thing so many times it no longer requires thought.
When a line was complete, he transferred it to a flat metal tray, building the page column by column. Thin metal strips between the lines controlled the spacing. There were no fonts to click, no sizes to select from a menu. Every choice was physical — a different tray for a different typeface, fetched and returned by hand. When the page was assembled, it was locked into a frame and placed on the press: a heavy cast-iron machine that had probably been printing things since before Independence. Ink was rolled across the raised type. A sheet of paper was laid over it. A lever came down. The sheet was peeled back and held to the light.
This was the proof. Errors at this stage were painful. A wrong letter meant finding the right metal slug among hundreds, removing the wrong one with a pointed tool, substituting it. There was no undo button.
Often it would take four hours to set a single page. I would sit on a wooden stool beside the compositor, marking corrections on the proof, drinking tea brought in a glass from the stall outside. The ceiling fan turned slowly overhead. The press thudded with a steady, industrial heartbeat. Somewhere outside, Wardha went about its afternoon.
Then computers arrived. The software was PageMaker — a desktop publishing programme that let you design an entire page on screen, adjust the spacing with a keystroke, and send a clean file to the press. What had taken four hours now took forty minutes.
I do not miss the old way. But I understood, after those evenings at Samyayog Press, that every word on a printed page was once placed there by a person — one letter at a time. It made me a more careful editor. Perhaps it made me a more careful physician too. The principle is the same: small errors, in printing as in medicine, have a way of becoming large ones.
The Bulletin Years
In 1990, MGIMS had a problem we didn’t even know how to name. Students graduated, walked out of the gate, and—quite literally—vanished.
There was no Facebook, no WhatsApp, no email. If you wanted to stay in touch, you wrote a letter, posted it, and waited. Sometimes it arrived. Sometimes it didn’t. Professional networks ran on luck: a chance meeting at a conference, or a familiar face spotted across an OPD corridor. Otherwise, silence did the rest.
Today it is hard to explain that kind of quiet. A photograph clicked in Sevagram now reaches New York before the tea cools. Back then, even a change of address could erase a friendship.
Mrs Desikan’s idea
Mrs Kamla Desikan, Secretary of the Kasturba Health Society, understood this loss more sharply than most of us. She had the rare ability to see an institution not as buildings and departments, but as people—especially the ones who had left.
One afternoon she said to me, almost casually, “We need a newsletter.”
Not a circular. Not an annual report. A newsletter—something that would tell our alumni, We remember you. And we still belong to each other.
And before I could ask what that would involve, she added, “You will edit it.”
That is how I became, overnight, the editor of the MGIMS News Bulletin.
A one-man newsroom
The plan sounded harmless: a four-page quarterly bulletin.
In reality, it became a small second job that ran alongside ward rounds, teaching, and the daily chaos of hospital life. In a proper newsroom you have reporters, sub-editors, proofreaders, and designers. At MGIMS in 1990, I had only myself—and a stubborn desire to make it work.
I went from department to department collecting news the way some people collect stamps. A new faculty joining. A seminar. A guest lecture. A promotion. A retirement. Anything that could make an alumnus pause and say, Ah, so the old place is still alive.
But I quickly realised something: buildings and equipment don’t create belonging. People do.
So the most-read part of the bulletin became what we called the “personal columns”—births, deaths, marriages. It was the campus grapevine, made respectable in print.
Cut, paste, and patience
Designing the bulletin was a physical exercise. “Cut and paste” wasn’t a computer command. It meant scissors, glue, and strips of typeset paper.
I sat for hours arranging columns, counting words, trimming edges, and shifting paragraphs by millimetres so the four pages looked balanced. There were days I felt like a junior doctor doing a delicate procedure with no instruments—only patience.
And yet, I enjoyed it. The work had a quiet satisfaction. It felt like stitching together a community that had started to fray.
Our social media, on paper
Looking back, the MGIMS News Bulletin was our social network—just slower and far more polite.
It did what WhatsApp groups do today. It reminded people they still mattered. It gave them a sense of place. When an alumnus posted in a remote district hospital opened the envelope and saw a familiar name, the distance shrank for a moment.
I remember the excitement of the early issues. One line announced the birth of a baby: Shridhar Reddy.
At the time it was just a happy entry in a column. Today, Shridhar is a grown man—a 33-year-old orthopaedic surgeon. That single line, printed on cheap paper, quietly contains three decades of life. No “timeline” can do that so cleanly.
The printing ritual
Every quarter, the bulletin took me back to a familiar place—the printing press of Mr Rajabhau Chawade.
The press had its own smell: ink, paper, and a faint metallic heat. The proofs came out warm, the letters sharp and slightly raised. Photographs were grainy black-and-white headshots, the kind that made everyone look either too serious or slightly guilty.
We checked the layout, fixed the mistakes, argued about fonts, and worried about deadlines. When the final copies arrived in bundles, it felt like a small victory. Not the kind that wins applause, but the kind that makes you breathe easier.
Thousands of bulletins would then go out—little paper ambassadors carrying Sevagram to wherever our alumni had landed.
The dead letter problem
Printing was only half the job. Posting it was the real battle.
Doctors move the way monsoon clouds move—often and without warning. Internship. Rural bond. Residency. Fellowship. Another city. Another hostel. Another address.
In the 1990s, when people moved, they didn’t update a profile. They simply disappeared.
We typed labels, stuck stamps, carried sacks to the post office—and then waited for the heartbreak to return. Weeks later, envelopes came back with red postal stamps:
Addressee left.
Insufficient address.
Door locked.
Each returned copy felt like a small failure. Somewhere, someone who still cared about MGIMS didn’t get the bulletin because life had shifted a few kilometres and we didn’t know.
We tried to keep a database, updating addresses with pencil and hope. It was never complete. It could never be.
What the internet changed—and what it didn’t
I edited the bulletin for six years and then passed it on. The bulletin continued, but the world changed.
With the internet, news stopped waiting for the postman. Retirements, deaths, achievements, celebrations—everything now travels instantly. WhatsApp groups do in minutes what our bulletin did in three months.
In that sense, the bulletin lost its urgency. It became less “news” and more “record.”
But I still feel something for print.
An email is skimmed and forgotten. A notification is swiped away. A printed bulletin is different. You hold it. You turn pages. You sit with it. It asks for your attention without shouting for it. It feels strangely human.
And paper has another strength—it stays.
Hard drives crash. Phones get replaced. Passwords are forgotten. But a booklet can sit quietly in a drawer for thirty years and still open like a memory.
The regret that stayed
This brings me to a regret that still pinches.
Somewhere between office shifts, renovations, changing administrations, and our casual neglect of archives, MGIMS lost most of the News Bulletins from 1990 to 2007.
The irony is painful. We created the record of those years—and failed to keep it.
Sixteen years of campus history: births, obituaries, milestones, faces, names, small announcements that now feel precious. They may still exist in someone’s trunk or attic, saved by an alumnus who couldn’t throw them away. But our own shelves are empty.
That loss taught me something simple: institutions love ceremonies, but they rarely love storage.
And yet, I don’t regret those years.
For a while, we built a paper bridge between Sevagram and the world. It carried more than news. It carried belonging.
Tales from the Typists

The MD thesis is more than a document. It is a visa. Without it, you cannot enter the final examination hall, no matter how good your clinical work is. And as the submission deadline approaches, the same panic returns every year—like a seasonal fever in the hostel.
Postgraduates begin hunting for two people with almost magical powers: a statistician who can rescue a stubborn p-value, and a typist who will stay awake when the rest of the campus has gone to sleep.
As a guide, I usually saw only the final bound volumes—neat, heavy, and deceptively calm. I rarely saw the labour behind them. Recently, I spoke to a few alumni and to the typists who carried generations of residents through those final weeks. Their memories trace a quiet technological revolution—from carbon paper and manual typewriters to laptops, EndNote, and PDF uploads. But one thing has stayed unchanged: the last-minute desperation.
***
The carbon paper years (1980–1990)
When MGIMS started its first MD programme in 1980, a thesis was a physical project. It came in four bound volumes, and each copy had to be typed, checked, corrected, and typed again. Sevagram had a small group of typists who became legends in their own right—Shantanu Dawande, the late Kuljeet Singh, Sanjay Bawse, and Mahendra Chaudhari. In Wardha, the familiar names were Prashant Thakre, the late Sachin Yugaonkar, and Deshpande.
Most residents wrote their drafts by hand. The typists had to decode them—often with more imagination than grammar.
Errors were common, and some were unforgettable. Dr Pradeep Vyavahare (1985) told me his typist repeatedly typed “hydrogen” or “hydrocarbon” instead of “hydrocele.” There was no spell-check, no red underline, no helpful suggestion. Only a tired resident, a tired typist, and a growing pile of corrections.
A note found inside an MD thesis in the MGIMS library. The handwriting at the bottom is Dr. Ravinder Narang's — suggested titles for a thesis not yet written.
Some residents couldn’t afford a typist at all. They borrowed machines and typed on their own.
Kishore Shah (1974) used a Remington Rand manual typewriter with a black ribbon and three sheets of carbon paper. He hit the keys so hard that the fourth copy would not look like a ghost. Arvind Ghongane (1979), a self-declared two-finger typist, survived on bottles of whitener. His thesis probably contained more correction fluid than ink.
***
The first computers arrive
Computers entered Sevagram slowly, and they entered like VIPs—expensive, rare, and slightly intimidating.
Dr Monika Ahuja (1982) was ahead of her time. With no computers available in Sevagram, she travelled to Baroda with her mother as a chaperone. A group of four friends helped her type and print her thesis on a dot-matrix printer. It must have sounded like a tractor starting up, but it worked.
In Sevagram, the real turning point came with Shantanu Dawande. In 1995, at just 24, he opened Excel Computers at Sevagram Square. His first machine was an Intel 386, bought for ₹85,000—a fortune in those days. It had 1 MB RAM, a 20 MB hard drive, and ran on MS-DOS.
Residents were suspicious at first. A thesis typed on a computer felt risky, almost like taking an unfamiliar drug without a trial. But once Dr Pati from Biochemistry took the plunge, others followed. Soon, Shantanu moved from hand-drawn graphs with sketch pens to using SPSS. He also became an expert in reading handwriting—especially the kind that gets worse with every sleepless night. He still remembers trying to decode the drafts of residents like Nandkishore Banait, Manu Kishore, and Chandan Tikku.
Mahendra Chaudhari, another stalwart, bought a Pentium computer in 1994 for ₹42,000, paid in instalments. He became the favourite of Dr V.K. Mehta’s students, known for clean formatting and a patience that never made it into any syllabus.
***
The hardware wars
By the late 1990s, computers began appearing in hostels, but they were still luxury items. Owning a desktop was like owning a small car—people noticed.
Dr Rajnish Joshi (1999) had an assembled desktop running Windows 98, with a floppy drive but no USB port. It cost around ₹30,000. Dr Devashis Barik (1991) had an HP Pentium II with a modem, which made him look like a man who lived in the future. Dr Rahul Narang (1987) managed with the official computer in the Microbiology department, which probably had more users than a hospital stretcher.
Much later, MGIMS itself changed the story by giving laptops and MacBooks to faculty and residents on interest-free loans. That one decision quietly shifted power. Residents no longer depended entirely on typists. They learned Word, Excel, and later EndNote. The typists didn’t disappear—but the relationship changed. The resident now arrived with a file. Not a bundle of scribbled pages.
***
The night shift at Sevagram Square
Even with better machines, the thesis season remained brutal.
In those weeks, Sevagram Square turned into a small nocturnal city. Binding shops stayed open late. Printers ran hot. Residents moved around with dark circles, stapled papers, and the kind of silence that comes only after too much caffeine.
Vishakha Jain (1996) remembers the shops buzzing late into the night. Sheetal Bodakhe (2005) still recalls riding her Scooty from Wardha to Sevagram at 2:30 a.m., clutching fresh printouts like they were blood reports in an emergency.
Some stories were funny. Others were painful.
Ramesh Pande (1989) told me he once rode his scooter to Ramnagar in the dead of night to dictate his thesis to a typist. “Occasionally,” he said, “he would lock the door from inside to sleep. I would stand there in the rain, ringing the bell, knowing he was inside but refusing to open.”
He returned to Sevagram empty-handed, with the kind of heaviness that no medicine can treat.
***
The midwives of academia
Over time I realised the typists were not just typing. They were absorbing panic.
People like Prashant Raut, Yogesh Khond, Prashant Thakre, and others saw residents at their worst—sleep-deprived, anxious, irritable, sometimes close to tears. They didn’t just format tables and correct margins. They offered tea. They offered reassurance. They said, “Ho jayega,” in the same tone a nurse uses in the labour room.
Prashant Raut, who typed nearly a hundred theses, described the process perfectly:
“The drafts changed so many times that the final version often looked like the first. It was like climbing a mountain and coming back to the same rock.”
He wasn’t joking.
Typing a thesis is a kind of labour. The resident is the mother in distress. The thesis is the baby that refuses to come out. And the typist becomes the obstetrician—using whatever tools are available: formatting tricks, last-minute rearrangements, emergency reprints, and sometimes a full “Caesarean section” in the form of massive edits.
By the time the thesis is finally bound and submitted, everyone is exhausted. The resident looks relieved. The typist looks older. And the guide—usually me—receives the final volume like a calm, dignified document.
Only a few people know what it cost to bring it into the world.
The Institute’s Biography
If patient records are the biography of a disease, an Annual Report is the biography of an institution. MGIMS began publishing these reports in 1971, barely two years after opening its doors. For decades, this booklet was our proof of life — a bureaucratic confession of how many students we taught, how many patients we treated, and what research we managed to squeeze out of our limited hours. Important, certainly. But let us be honest: most such reports read like railway timetables from the British Raj, destined to gather dust in the deep recesses of government cupboards.
In 1998, the job of editing this document landed on my desk. I held the post until 2005. I had cut my teeth editing the MFC Bulletin in the late eighties, so I assumed I knew something about deadlines and commas. I was spectacularly wrong. The Annual Report was not about opinion or flair. It was a minefield of numbers, names, and unforgiving details. One wrong digit could turn a year of triumph into a year of negligence.
***
When I took over, I felt the report lacked a spine. It was a chaotic heap of statistics waiting for a narrator. It needed to tell the story of Sevagram in a way that even a distracted bureaucrat in Delhi could follow.
So, I reorganised the chaos into four distinct pillars: Education, Hospital, Research, and Community Work. That simple structural shift changed the tone entirely. ‘Education’ captured our academic soul—the admissions, the results, the theses. ‘Research’ highlighted our intellectual pulse through papers and conferences. ‘Hospital’ revealed the sheer weight we carried—the OPD footfall, the surgeries, the midnight deliveries, the blood transfusions. And ‘Community Work’ brought us back to our roots, documenting the dust and heat of our village camps.
Suddenly, the report felt less like a government file and more like a biography.
***
Writing the report was easy. Finding the data was an exercise in despair.
We must remember the era. There were no Google Forms, no shared drives, no submit buttons. Every March, I sent polite formal letters to Heads of Departments. Then I waited. In April, reminders. In May, desperate pleas. By June, information would arrive — but rarely in usable form.
It came in dribs and drabs: handwritten notes on prescription pads, half-typed sheets from manual typewriters, figures squeezed into margins, tables that looked as if they had been drawn during a blackout. Numbers did not tally. Names were misspelled. Units were mixed up. I learned to suppress my temper and do what internists do best — verify, cross-check, and clean up the mess without creating a scene. It felt less like editing and more like stitching a quilt from scraps that refused to match.
***
The real heart of this story beats not in the corridors of MGIMS but in the noisy centre of Wardha town.
Mr. Rajabhau Chawade ran a small printing press near the R.D. Sinhal shop in the main market. His building defied commercial logic: while most people lived upstairs and worked downstairs, Rajabhau lived on the ground floor and kept his computer shop on the first. He was a gentle, patient man who likely viewed my arrival — with my new format and obsessive lists of corrections — as a divine test of his patience.
He never complained. Not once.
For seven years, my evenings followed an unshakeable ritual. After finishing hospital rounds, I would kick-start my Bajaj scooter and ride into town. It never occurred to me to ask for an official college vehicle, even though I was doing official college work. Perhaps I was too shy. Perhaps I simply did not know the rules. So I drove myself, dodging stray cattle and potholes, arriving at a place that smelled permanently of ink, cheap paper, and machine oil.
The offset machines hummed with a loud rhythmic thud — a steady industrial heartbeat that made conversation difficult. In that cramped noisy room, surrounded by stacks of fresh paper and tins of grease, we sat for hours trying to turn raw data into something readable.
***
Rajabhau did not employ a high-end DTP professional from Nagpur. He had something better. He had his daughter, Pallavi.
In 1998, Pallavi was in the eighth standard — a shy girl from a Marathi-medium school who was suddenly navigating complex English syntax. When she realised I was a senior doctor from the hospital, she froze. Her fingers hovered hesitantly over the keyboard, tongue-tied by the hierarchy that separates a schoolgirl from a Professor of Medicine.
It took time to dismantle that wall. I spent the first few minutes of every session just talking — asking about school, which film she had seen, what she had eaten for breakfast. Small questions. Slowly the tension evaporated. She forgot my title and I became simply the uncle sitting beside her.
Once comfortable, she was formidable. She sat before a bulky HCL computer, wrestling with PageMaker on a screen that flickered with exhaustion. The machine was slow, the software temperamental, and every now and then the computer would freeze like a stubborn patient refusing to answer a question.
Her English was limited, and medical terminology is cruel to the uninitiated. One slipped keystroke and *hypoglycaemia* becomes *hyperglycaemia* — a typo that changes a cure into a cause of death. I would sit beside her on a plastic stool, watching tables jump to the next page and columns shift like unruly schoolchildren, catching the letters that tried to escape.
"Sir, the table is moving again," she would say, panic creeping into her voice.
"Adjust the row height," I would reply, feigning a confidence I did not feel.
One memory still makes me smile. Occasionally she would accidentally delete an entire paragraph and freeze in horror. I taught her Ctrl+Z — the undo button. Her face would light up as if I had been handed her a miracle drug. That simple shortcut saved our sanity, and the report, more than once.
We fought power cuts that plunged the room into sudden darkness. We fought software glitches that ate our files. We fought deadlines that seemed impossible. But every year, we finished.
I had unilaterally changed everything — the cover, the font, the layout — without seeking the Dean's permission. A bold, perhaps reckless, move. Twenty-five years later, I am pleased to see that the annual reports still carry the DNA of the format we designed in that small room in Wardha.
***
When the final report arrived from the press, it was a transformation. A glossy cover with the MGIMS emblem. Crisp paper inside. Legible fonts. Tables that no longer made the eyes water.
I began a small tradition: opening each report with a quotation to give the dry numbers a human voice. In the 1998–99 report, I chose Joseph Pulitzer, and it became my editorial north star:
"Put it to them briefly, so that they will read it Clearly, so that they will appreciate it Picturesquely, so that they will remember it And above all, Accurately, so that they will be guided by its light."
The report travelled to funding agencies, government ministries, and donors. For our alumni scattered across the world, it was a yearly postcard from home — a reminder of where they had come from.
Over time, the Chawade family became more than my printers. They became my patients. And here I must make a confession that punctures my ego.
Rajabhau had come to the hospital hundreds of times over forty years — delivering registers, printing forms, meeting staff. He must have been examined by a dozen physicians. I myself had seen him in the OPD countless times. Yet when he turned seventy-five and complained of breathlessness, we all assumed it was age, or perhaps mild asthma.
We were wrong.
An echocardiogram revealed severe rheumatic mitral valve disease. The murmur of mitral stenosis — that classic rumbling mid-diastolic sound we grill our students about, asking them to find it with the bell of the stethoscope — had escaped us all. It had escaped me.
Had we missed it for another year, his death certificate would likely have read "Bronchial Asthma," obscuring the truth. Fortunately, we caught it in time. I supervised his valve replacement, and he lived a full life until 2022.
It struck me then: the man who had helped me preserve the history of MGIMS had nearly slipped out of it because of our clinical blindness.
***
By 2005, the Annual Report had become a well-oiled machine. Institutions need fresh blood. I passed the baton to Dr. Anshu, a sharp Professor of Pathology who shared my obsession with precision.
For my final report — the thirty-fifth edition — I signed off with George Santayana:
"We must welcome the future, remembering that soon it will be the past; and we must respect the past, knowing that once it was all that was humanly possible."
Some years later, MGIMS launched its own research journal — a biannual publication carrying the work of the institute's faculty. I served as one of several associate editors, helping select manuscripts, reviewing papers, and guiding authors through revision.
Then I began to notice something that bothered me. Papers I had rejected outright as peer reviewer were finding their way into print. The science was not always sound. For months I sat with the discomfort, uncertain whether to raise it or simply continue. Eventually I made my decision.
I wrote to Dr. Anshu, who had just taken over as editor.
Dear Dr Anshu,
I would like to resign both as a member of the editorial team and as a peer reviewer for the Journal of MGIMS.
It has been long since I joined the board, and I feel that those who can critically analyse manuscripts and help the journal separate wheat from chaff should serve it now. The journal needs vision, creativity, leadership, and the courage to call a spade a spade — qualities that younger editors with fresh eyes are better placed to bring.
With too many things on my plate, I can no longer do justice to the post. Hard though it is to give up something you care about, I feel that sharper minds can help the journal carve out the niche it deserves.
May I wish you and your team all the best.
With regards,
SP
***
Editing those reports was labour — pure, unglamorous labour. But years later, when I was tasked with leading the Hospital Information System, I realised those evenings in Wardha had not been wasted. I knew the data. I knew the difference between a real admission and a clerical error. I knew the hospital not just by its patients but by its pulse — its numbers. The report told the truth. In our profession, the truth is the only thing worth printing.
Quiz Day on a Shoestring
1994 was a year of seismic shifts for India, but for us at the Mahatma Gandhi Institute of Medical Sciences (MGIMS), it was simply the year the money ran out.
I was a Reader in Medicine then, managing a ward that never slept and a bank account that was dangerously quiet. I had a lively group of residents, but two stood out: Dr. Prabhat Goel and Dr. Ravi Sautha, both from the Class of 1983. They were a study in contrasts. Prabhat, a Medicine resident, was the cerebral type—the kind who absorbed textbooks by osmosis and could quote Harrison’s Principles of Internal Medicine as if it were poetry. Ravi, an Orthopedics resident, was the pragmatist—hands-on, energetic, and possessed of a sharp, street-smart clinical eye.
Their enthusiasm was abundant. Their money, like most of ours that year, was nonexistent.
It was a strange, anxious summer. The Institute had fallen foul of Mr. B. Shankaranand, the then Union Minister of Health and Family Welfare. In a move designed to teach the management a lesson, he pulled the purse strings tight. The central government withheld our grant. For two months, salaries simply did not arrive.
In a metro city, you have credit cards or anonymity. In Sevagram, you have neither. There were no overdraft facilities to cushion the fall. We lived on borrowed time, patience, and the immense goodwill of the local kirana shopkeepers who quietly noted our debts in their greasy ledgers without asking questions.
***
It was in the middle of this fiscal drought that my phone rang. It was Dr. Sudhir Bhave from Nagpur.
Sudhir was a kindred spirit—an alumnus of GMC Nagpur (Class of 1976), a psychiatrist with a sharp academic streak, and a man who had music in his blood. He was a storyteller and a singer, the kind of person who could make a mundane event feel like a festival. He was organizing the annual medical quiz for the Academy of Medical Sciences (AMS), Nagpur.
“We want a team from MGIMS,” he said, his voice crackling over the landline. “One teacher and two residents. Will you lead it?”
I looked at Prabhat and Ravi. They were drowning in discharge summaries. I was buried under a pile of lecture notes. We were tired, we were broke, and our minds were occupied with the very real problem of how to pay for next week’s groceries. “We can’t,” I started to say. “There is a trophy,” Sudhir added. “And lunch is on us.”
I paused. A free lunch. A day away from the oppressive heat of the wards. I looked at the boys. They nodded. So, we said yes.
***
We travelled the way unpaid doctors travel.
There was no question of hiring a taxi. That was a luxury for consultants with private practices. We pooled whatever crumpled notes and coins we had in our pockets, squeezed our frames into a shared auto-rickshaw to Wardha station, and bought tickets for the unreserved compartment—what we unashamedly called “Third Class.”
The train was a sensory assault. It was packed with the humanity of rural India—farmers with sacks of grain, women with crying babies, students playing cards, and the pervasive smell of sweat, hair oil, and steel. We didn’t find seats. We stood near the door, clinging to the grimy steel rod, swaying with the rhythm of the tracks.
But the mood was electric. Perhaps it was the escape from the hospital, or perhaps it was the absurdity of our situation. We stood there, sweating in our synthetic shirts, grilling each other like schoolboys. “What’s the triad in Felty’s syndrome?” Prabhat shouted over the roar of the wheels. “Rheumatoid arthritis, splenomegaly, neutropenia,” Ravi shot back, dodging an elbow from a fellow passenger. “Don’t ask me triads. Ask me something we actually see!” “Okay, X-ray findings in scurvy?” “White line of Fraenkel!”
We laughed, throwing answers like paper balls, oblivious to the stares of the other passengers who surely wondered why these three men were shouting about spleens and vitamins.
***
We deboarded at Ajni station. It was a strategic decision—partly to save time, and partly because we didn't want to look like lost villagers navigating the chaos of the main Nagpur station. From Ajni, we walked. The venue was the IMA Hall on North Ambazari Road. It was a mile and a half away. Under the merciless Vidarbha sun, that mile felt like a marathon. We walked briskly, clutching our small bags, watching the heat rise in waves off the asphalt. By the time we reached the gates of the IMA Hall, our shirts were clinging to our backs like damp towels. Our shoes were coated in grey dust. We looked less like a team of intellectuals and more like three refugees who had just crossed a border.
We had come with no preparation, no books, and absolutely no expectations. It is, I discovered that day, a very light way to travel.
***
Inside the hall, the atmosphere changed instantly. The air-conditioning hit us like a blessing. But the social temperature was different. Teams from the Government Medical College (GMC) and Indira Gandhi Medical College (IGMC) sat in neat, huddled groups. They looked fresh, crisp, and intimidatingly prepared. They had the calm faces of people who had slept well, eaten a proper breakfast, and revised their notes. We were the rural cousins. The underdogs.
But then, the lights went out. The hall plunged into darkness, save for the single, piercing beam of the carousel slide projector. The hum of the projector fan filled the room. "Question One," the quizmaster’s voice boomed.
Medicine does not care about the starch in your shirt or the money in your pocket. A question is a question—whether you read it in a library in Nagpur or face it in the casualty ward of Sevagram at 2:00 AM. The first slide clicked into place. A blurry image of a retina. The buzzer rounds were brutal. You had seconds to decide.
"Roth Spots," Prabhat whispered instantly. "Hit it," I said. Ravi slammed the buzzer. "Correct."
The questions came fast, a mix of the obscure and the everyday. A chest X-ray showing an odd shadow. An ECG strip with a wandering baseline. A history of a farmer with fever and muscle pain.
This is where the Sevagram grind paid off. Our competitors knew the books. But we knew the patients. We had seen the farmer with Leptospirosis; we had smelled the organophosphorus poisoning; we had held the wrist of the patient with the collapsing pulse. Prabhat was the encyclopedia—he provided the syndrome names. Ravi was the pragmatist—he spotted the fractures and the surgical signs. I played the conductor, keeping us calm, filtering the answers. We worked as a single organism. No ego. No "I think." Just a whispered consensus and a hand on the buzzer.
There was a moment in the visual round that turned the tide. A slide showed a peculiar skin rash. The other teams hesitated. They were looking for textbook descriptions. Ravi leaned in, squinting at the screen. "That’s Pellagra," he muttered. "Look at the necklace distribution. We saw a case last week in the OPD." We buzzed. We scored. By the final round, the "outsiders" label had vanished. The audience was leaning forward. We weren't just participating; we were dominating.
***
When the lights came back on, the scoreboard told the story. We had won.
The organizers called us to the stage. There was applause—polite from the rivals, enthusiastic from Sudhir Bhave. They handed us a gleaming trophy and certificates. Then, they handed us an envelope. Inside was the cash prize: ₹100 each.
To a modern reader, a hundred rupees is barely a tip. It won’t buy you a coffee at an airport. But in 1994, with two months of unpaid wages haunting us, that red note felt like a brick of gold. It wasn't the purchasing power; it was the timing. It felt like an unexpected IV line when the vein has been playing hide-and-seek for hours. It was validation. It was survival money. We stood there, clutching our certificates and our hundred-rupee notes, grinning like we had won the Nobel Prize.
Lunch followed. And what a lunch it was. The Academy of Medical Sciences did not scrimp. There were steaming vessels of rice, rich gravies, paneer that melted in the mouth, and sweets dripping with syrup. We ate like men who had marched across a desert. We went back for seconds. We scraped our plates. The food tasted better not just because of the hunger, but because we had earned it with our wits.
***
The journey back to Sevagram was a blur of exhaustion and euphoria. The trophy sat on my lap like a newborn child that needed guarding. We took a shared auto back to the station and boarded the evening train. This time, we managed to find seats.
The compartment was just as noisy as before, but we were in our own bubble. We replayed the quiz, question by question. "I can't believe they missed the Atrial Myxoma sound!" "I thought we lost points on that Pharmacology question." "Did you see the face of the GMC team when we answered the spleen question?"
There were no smartphones in 1994. No WhatsApp groups to flood with "Winner!" emojis. No Instagram stories to post with a #ProudMoment caption. We couldn't broadcast our victory to the world. We couldn't even tell our wives until we physically walked through our front doors.
Oddly, that digital silence made the win sweeter. The victory stayed strictly between the three of us, sealed in the rocking motion of the train and the smell of coal smoke. We carried the news home the way people once carried love letters—tucked inside a pocket, private and precious.
When we finally reached Sevagram, dusty and dishevelled, we told our families. Their smiles completed the circle. We had left that morning on an unreserved ticket, unpaid, unprepared, and anxious. We returned with a metal cup, three hundred rupees in our pockets, and the lightness that comes from a small victory when the world feels heavy.
For one day, amidst the salary crisis and the politics, three broke doctors felt like kings.
The Art of the EBM
If the 1990s were about digitising hospital records, the early 2000s were about upgrading the software of our minds. In 2000, the Medico Friends Circle (MFC) held its annual meeting at Yatri Niwas in Sevagram—a modest guest house across the road from Gandhi’s Ashram.
MFC meetings had their own distinct flavour: simple arrangements, serious conversations, and a fierce, unvarnished idealism. We sat cross-legged on the floor, arguing about social determinants of health over endless cups of tea, while ceiling fans pushed warm air from one corner to another in a futile attempt at cooling. It was in this sweltering, intellectually charged atmosphere that I met Dr. Madhukar Pai—known to everyone simply as Madhu.
He was a young graduate from Madras Medical College, then pursuing his MD in Community Medicine at CMC Vellore. Madhu spoke with a clarity that was almost startling. He wasn't loud or dramatic; he was simply sharp and well-structured, his thoughts organized like a perfect clinical note. We began talking about medical research, and I confessed my growing fascination with Evidence-Based Medicine (EBM), a concept I had stumbled upon in 1996 through the writings of David Sackett.
Madhu’s eyes lit up. He was already a pioneer in his own right, conducting workshops on epidemiology and statistics. In that small room, with the scent of chai and the low buzz of activists outside, we decided to collaborate. It was a casual decision, made between sips of tea, that quietly shifted the trajectory of my professional life.
***
The Workshop That Woke the Wards
In February 2000, we organized a three-day workshop on Statistics and Study Designs at Sevagram. Thirty residents signed up—a mix from Medicine, Paediatrics, OB-GYN, and Surgery. Most arrived with the expression I knew well from thesis season: a mask of polite interest thinly veiling a deep sense of dread. They expected a dry diet of p-values, t-tests, and academic boredom.
Madhu had other plans. He didn’t teach statistics as a punishment; he taught it as a torch. He showed the residents how bias can bend the truth, why randomisation is simply fairness written into a study design, and how to read a medical paper without being seduced by confident conclusions. He made confidence intervals feel like common sense rather than a mathematical hurdle.
For eight hours a day, the residents stayed awake—fully, vibrantly awake. In Sevagram, that was a minor miracle. By the end of the third day, the fear had softened. They began to see research not as dry mathematics, but as curiosity armed with discipline. Many pleaded for Madhu to join MGIMS full-time. I realized then that we were no longer just treating patients; we were learning to interrogate our own habits.
***
McMaster: My First Flight, My First Mistake
Three years later, the pull of this new world took me to its birthplace—McMaster University in Hamilton, Ontario. This was where EBM had been shaped into a global movement.
In June 2003, I was accepted for the prestigious workshop, How to Teach Evidence-Based Clinical Practice. The Kasturba Health Society funded part of the cost, and Mr. Dhirubhai Mehta helped bridge the rest. I booked an Air Canada ticket—my first international flight. My route was Mumbai to London, then Toronto, with a ninety-minute layover.
I landed at Heathrow and did exactly what a novice international traveller does: I wandered. I stared at the luxury shops. I walked slowly, as if the terminal itself were a museum. I forgot that ninety minutes in a giant terminal is not a window of time; it is a countdown. When I finally reached the transfer desk, the staff looked at me with a mix of sympathy and disbelief.
“Sir, your flight has already departed.”
I felt small, foolish, and suddenly very far from home. My luggage was on its way to Canada, and I had neither the money nor the courage for a new ticket. I went to the Air Canada desk and told the truth: I was a doctor from rural India on a grant, trying to learn how to teach better medicine. The lady at the counter listened, her fingers dancing across the keys. She paused, then said, “Okay. We can put you on the next flight. It leaves in an hour.”
I didn’t celebrate. I simply ran. That day, I learned a vital clinical rule for travel: never underestimate the distance between two gates.
Nafisa Kapadiya-Aptekar, an MGIMS alumna from the Class of 1975, was waiting at the airport with her husband to rescue me. They listened to my travel travails with a mix of laughter and sympathy, fed me a proper meal, and coached me on the tips and tricks of fighting jet lag. I stayed with them overnight—a small, welcoming island of Sevagram in the middle of Ontario—before shifting to the Hamilton hostel the next morning.
***
Hamilton: Among the Masters
Hamilton in 2003 felt like a city built on a different logic. The McMaster campus was a sprawling blend of limestone and glass, nestled near the Royal Botanical Gardens. The air was crisp, a sharp contrast to the humid heat of Wardha, and the university felt like a cathedral of thought.
There were ninety of us from across the globe, but we didn't sit in a lecture hall. We sat in circles. The method was role-play—slightly uncomfortable, deeply effective. One person played the sceptical student, another the arrogant consultant, and a third the EBM advocate trying to introduce evidence without bruising a senior's ego. It was funny, but it was also a mirror. I realized that knowing the evidence is useless if you cannot navigate the hierarchies of human pride.
Then there were the masters themselves. In those days, we in India were still easily fascinated by international celebrities, and here they were, in the flesh. I found myself sitting across from Gordon Guyatt, the man who had actually coined the term "Evidence-Based Medicine" in 1992. Seeing a giant like Gordon—casual, accessible, and intensely focused—teaching us was a thrill I can still feel.
Beside him was Deborah Cook, a powerhouse who co-authored the definitive Users' Guides to the Medical Literature. Watching Deborah explain diagnostic accuracy tests, likelihood ratios, and how to apply them at a patient's bedside was like watching a master artist at work. She turned abstract numbers into tools for survival.
A librarian sat with each group, teaching us how to navigate PubMed and Cochrane. Watching her find answers in minutes that would have taken me days was a humbling experience. It made me uneasy. How much of my earlier practice had been built on "expert opinion," and how little on hard, verifiable evidence? This workshop changed everything. It influenced the thirty-two MD theses I would go on to supervise and shaped my later time at UC Berkeley. I returned home as a better physician, now knowing when—and more importantly, why—not to order a test or write a prescription.
***
An Alumni Trail and a Suitcase of Books
On the way back, I stopped in the UK to visit the MGIMS diaspora. I stayed with Monica Ahuja in London—once a resident, now a mother juggling medicine in a new world. In Edinburgh, I visited Bhavana’s cousin, Vipin Zamvar, a cardiac surgeon who showed me his theatre with a quiet, practiced pride. In Aberdeen, I spent time with Muthu Kumar and Sonali, and bought the Harry Potter audio series for my daughter, Ashwini, carrying the tapes home like precious contraband.
In Oxford, I met Dr. Sadhana Bose and her husband, through whom I was introduced to Dr. David Warrell, the editor of the Oxford Textbook of Medicine. We spoke for two hours about snakebites—a global expert and a rural doctor discussing a problem that slithers into our Sevagram wards every monsoon.
I returned to India with a suitcase full of books and a new lens. The evidence revolution had begun in Sevagram, but for me, it was merely the prelude to an even bigger adventure: a year at UC Berkeley.
Bapu Ki Beti, Hamari Behenji
On January 3, 2001, a silence fell over Sevagram. Dr. Sushila Nayar — our Badi Behenji — was gone.
She had passed away in Prerna Kutir, a residence stubbornly modest for a woman of her stature. Visitors did not sit on sofas; they sat on a thick cotton mattress covered with stark white khadi sheets. On that mattress, the hierarchy of India dissolved. A Union Minister would sit cross-legged beside a ward attendant, both held in the same steady gaze. To the nation, she was Mahatma Gandhi's physician and a freedom fighter. To us, she was simply the gravitational force that kept MGIMS from floating away.
With her passing, the baton moved to Mr. Dhirubhai Mehta. He took charge quietly, aware of the giant shadow he was stepping into.
***
By August 2001, I was finally exhaling. For six months I had been obsessed with renovating the Medicine ICU — a project that had turned me into what I jokingly called an "intellectual decorator." Alongside Dr. Rajnish Joshi and a nocturnal architect named Anil Pandit — who prowled the construction debris at midnight with a cheek full of paan — we had turned a pile of rubble into a functioning place of healing.
Then the phone rang. It was Dhirubhai.
"SP," he said, using the initials that only close friends used. "We need to bring out a book. A tribute to Behenji. I want you to edit it."
A surge of honour. Then a cold wave of alarm.
"When is the release?"
"Her first death anniversary. January 3, 2002."
I did the arithmetic. Four months. In the Sevagram of the early 2000s — where communication still moved at the speed of the post — four months was effectively yesterday. The intellectual decorator hung up his hard hat and picked up a red pen.
***
I knew my limitations. I needed a partner who handled the English language with surgical precision. I called Dr. Prabha Desikan, Class of 1984. Prabha had Sevagram in her marrow — her father was the legendary leprosy researcher Dr. K.V. Desikan. She possessed an editor's eye: sharp, patient, and entirely unsentimental.
We were joined by Dr. Rajnish Joshi and Dr. Ashish Goel, both from the MGIMS classes of 1992 and 1993, then in the middle of their MD residency in the department. Today both are Professors of Medicine — Rajnish at AIIMS Bhopal, where until recently he also headed the department, and Ashish at AIMS Chandigarh, where he currently heads it.
They were a perfect counterbalance. Rajnish possessed a restless, fertile mind—quick to innovate and uniquely capable of wrestling fleeting ideas into finished realities. Ashish, on the other hand, wore the quiet, measured look of a man who weighs his words. He anchored the project with exactly what it required: precise writing, meticulous proofing, and an intuitive sense of how text should rest on the eye. We would need all of it. Together, we faced a staggering mandate: forty-five contributors, a three-month deadline, and the grueling, everyday demands of our hospital work—the packed OPDs, the wards, the ICUs, and the unpredictable rush of medical emergencies. And, lest I forget, Rajnish and Ashish were simultaneously writing their own MD theses.
Yet, despite the exhaustion of the wards and the weight of their theses, we were driven by a singular vision. We wanted the volume to be what Prabha Deikan and I called in the introduction a "prism of affection." To build it, we reached out to MGIMS faculty, administrators, politicians, Gandhian scholars, social workers, and alumni, leaving the content entirely to the contributors. We weren't trying to create a perfect, saintly portrait that hid her flaws. We were after something much more difficult: a small, honest tribute to a woman who refused to give up, told through the raw and real stories of the people whose lives she had changed.
***
For the printing, I turned to Vinod Sinhal. He was thirty-five then, a man quietly carving out his own path. His father ran R.D. Sinhal Stores, a well-known shop in Wardha Market that sold everything from stationery to guns and bullets—a combination only small-town India could produce without irony. The elder Sinhal was a man of firm principles; if a child returned too soon for more pencils, he would conclude they had been careless and refuse to sell them any. Schoolchildren approached his counter with the same caution they reserved for difficult teachers.
Vinod, however, had moved out from under that stern shadow. By 1996, he had set up his own small press in the industrial area, four kilometers from the college. He had never produced a book before, and when I approached him, he accepted the commission with a visible, nervous hesitation. What he could not have known then was that this project would go on to define the rest of his professional life.
Since Vinod was new to books, we had to assemble a makeshift team across two cities. We worked with Prashant Thakre, who ran a small typesetting center in Wardha, but for the heavy lifting, we had to look toward Nagpur. The project was a massive technical undertaking for its time. We had piles of black-and-white images from the 1940s that required high-resolution scanning—a luxury in 2001. We took them to a specialist near the Gandhi statue in the Mahal area of Nagpur, paying nearly ₹18,000 for scanning alone.
For the visual design, we found Vijay Farkase. He was a talented man who had designed the iconic Haldiram's snack pouches but, like the rest of us, had never worked on a book. We were all learning on the fly, a team of amateurs fueled by enthusiasm.
This inexperience led to one serious setback: after the first few copies were printed, we discovered a layout error. We had to reprint the entire run. It was a costly, demoralizing blow, but in the spirit of the woman we were writing about, we absorbed the loss and moved on.
***
As the deadline approached, the cover remained our biggest hurdle. The sketches looked amateur, and the photographs felt generic. We wanted something that was unmistakably "Behenji"—plain, firm, and without ornament.
We were sitting in my office, staring at a succession of failed proofs, when Rajnish Joshi suddenly pointed at my chest.
"Sir," he said. "Why don't we use that texture?"
I was wearing a yellow khadi shirt. In Sevagram, khadi was the code. I had made my own compromise with the institute's dress culture: I wore crisp khadi shirts rather than trousers, which usually crumple so badly by late afternoon that you end up looking like an unmade bed.
"The fabric," Rajnish insisted. "That’s her."
We took the shirt off my back right then and there and placed it on the glass bed of a flatbed scanner. The machine whirred, capturing the rough, uneven weave of the hand-spun cloth. That scan became the soul of the cover. Over that yellow texture, we superimposed a sepia photograph of Behenji sitting beside Bapu. The title followed naturally: Bapu Ki Beti, Hamari Behenji.
The photographs inside presented their own challenge. We didn't want the book to look like a modern documentary; we wanted it to feel like a memory. Today, you can achieve this with a simple Instagram filter, but in 2001, it required a kind of darkroom alchemy. We drove to Nagpur yet again to find a specialist who could convert the sharp blacks and whites into warm sepia tones.
We didn't want the book to look glossy; we wanted it to look timeless. When the first proof finally came off Vinod’s machine, we knew we had achieved it. Gandhi. Behenji. Khadi. Nothing extra.
***
Tribute books suffer from a predictable disease: they become hagiographies — garlands of sugary praise in which the subject ceases to be human. We were determined to avoid this.
Everyone in Sevagram knew Behenji's famous temper. It was not the petty irritation of a bureaucrat. It was the terrifying wrath of a matriarch who could not tolerate laziness, excuses, or indifference to patients. We included a detailed interview from the National Medical Journal of India where she spoke in her own unvarnished voice. We ensured the essays we selected reflected both her immense compassion and her steel. A Behenji without her temper would not have been Behenji.
Prabha Desikan worked through the drafts with a disciplinarian's eye — smoothing language, fussing over margins, obsessing over font sizes and spacing. The invisible details that decide whether a volume looks like a serious work or a rushed souvenir.
***
When the final copy was bound, I took it to Dhirubhai. He held the book in both hands, running his fingers over the cover — perhaps recognising the texture of the ideology he was now sworn to protect. He praised the work at length. Then the practical man surfaced.
"How much did it cost?"
"The printer's bill is ₹1,40,000."
He nodded, pulled out his pen, and authorised a payment of ₹1,50,000. It was a gesture of class — his acknowledgment that Vinod Sinhal had gone beyond what was asked.
On January 3, 2002, exactly one year after she left us, the book was released at a ceremony in the open ground behind the Microbiology department. The chief guest was Shri Krishan Kant, the Vice President of India. Security was tight, speeches were long, and the stage was crowded.
I was not on it. I do not recall being invited even to the front row. In the theatre of official functions, the workers are rarely the actors. The flashbulbs popped, the Vice President held up the yellow cover, and the applause moved through the crowd.
It did not matter. Standing at the back, I felt a quiet, private satisfaction that had nothing to do with the stage. I knew the one-minute glory of a public function fades before the car reaches the gate. But the book was real. We had taken the rough weave of a khadi shirt and turned it into a testament. We had preserved the spine of Sevagram.
For Vinod Sinhal, that single project changed everything. He mastered the trade, went on to publish the MGIMS News, police annual reports, and nearly every publication the institute required. A partnership that continues to this day — built, at its beginning, on a nervous young man's willingness to say yes to something he had never done before.
The Belgaum Bond
Workshops like these are useful, of course. But what stays with you is often what happens after the sessions—over tea, in corridors, and sometimes in the room you are allotted.
That is where my luck worked quietly.
AIIMS paired me with Dr. Premnath Kotur, a senior Professor of Anaesthesiology from JN Medical College, Belgaum. He had already spent close to two decades in academics. On paper, we had little in common. He was from the south, I was from central India. He worked in anaesthesia, I worked in medicine.
But once the lights went out and the Delhi winter began pressing against the windows, we started talking.
We didn’t waste time on small talk. No cricket. No politics. We went straight to the things that kept bothering both of us—medical ethics, evidence, and the quiet power an editor holds. We spoke about what gets published, what gets ignored, and how easily medicine can drift when nobody asks hard questions.
By the end of those two nights, I felt I had found a fellow traveller.
When we checked out, Dr. Kotur said, “Kalantri, you must write for my journal.”
***
An invitation that became a platform
He wasn’t being polite. Dr. Kotur edited the Indian Journal of Anaesthesiology, and he actually meant it.
Over the next few years, I wrote a series of articles for his journal—pieces that had little to do with anaesthesia drugs and everything to do with the practice of medicine. I wrote about informed consent, not as a form to be signed, but as a human contract. I wrote about medical errors, a subject most doctors preferred to keep locked away. I wrote about the drug industry and conferences, and about the uneasy space where ethics and evidence collide.
Dr. Kotur published them without flinching. In those days, that itself was an act of courage. He gave these ideas a home when many journals would have found them “uncomfortable.”
***
Belgaum, and a workshop years later
Our connection deepened in May 2009. By then, evidence-based medicine was no longer a fancy phrase—it was becoming a way of thinking.
Along with my younger colleagues, Dr. Rajnish Joshi and Dr. Saranya Sridhar, I travelled to Belgaum to conduct a two-day workshop on Evidence-Based Medicine at KLE University. Dr. Kotur, now the Registrar, was our host.
It felt oddly satisfying. Six years earlier, we had whispered these ideas in a room at AIIMS. Now we were teaching them from a podium in his institution, to a hall full of young doctors.
Some friendships grow slowly. Ours grew through shared work.
***
When the roles reversed
In 2016, Dr. Kotur decided to do something that surprised me—not because he lacked ability, but because he already had stature. Despite seniority and administrative responsibilities, he enrolled for a PhD in Evidence-Based Medicine.
When his viva came up, he asked me to be the external examiner.
A PhD defence has its own atmosphere. The candidate stands alone at the front, years of effort condensed into slides and answers, while the examiners watch like hawks. The room is always tense. Even confident people suddenly forget their own names.
But as Dr. Kotur presented his work, I saw the same man I had met at AIIMS—careful, serious, and quietly stubborn about getting things right. I asked him difficult questions, because that is what the role demands. He answered calmly, without shortcuts. He knew his subject, and he had earned his conclusions.
When it ended, I didn’t feel like I had examined a candidate.
I felt I had witnessed a friend complete a long, honest climb.
***
The best connections are of the mind
When I think of Dr. Kotur now, I don’t remember a formal conference or a big stage. I remember a shared room at AIIMS, the Delhi cold outside, and two doctors talking late into the night about the grey zones of medicine.
That room gave me more than a workshop certificate.
It gave me a colleague for life.
The McMaster Calling
By 2003, Evidence-Based Medicine had begun to take root in Sevagram, and much of that credit belonged to my collaboration with Madhukar Pai. But Madhu, as always, thought one step ahead.
“You have to go to McMaster,” he said. “That’s where it all began.”
McMaster University in Hamilton, Canada, was the birthplace of this movement. It was where Gordon Guyatt—who coined the term “Evidence-Based Medicine”—taught and trained people to question their own certainty. Madhu had attended a workshop there and returned with a new kind of confidence: not the loud kind, but the quiet confidence of someone who knows how to check the facts. He wanted me to feel that shift too.
***
On April 10, 2003, I wrote to the President of the Kasturba Health Society. I had been accepted for a workshop titled How to Teach Evidence-Based Clinical Practice, scheduled from June 22 to 27. The organisers had waived the tuition fee—$2,700—which felt like a small miracle. But travel was still expensive. I worked out the cost of the round trip—Sevagram to Mumbai, then London, Toronto, and back—at around ₹65,000, a serious amount in those days.
I also added a second reason for the trip. Dr. Mike Galvin had invited me to stop in the UK on my way back and speak in Leeds and London about MGIMS—our work, our rural focus, our stubborn belief that good medicine is possible even in a village. I hoped it might open doors for exchange programmes.
To my relief, the Society agreed to fund half the cost. For the remaining amount, Mr. Dhirubhai Mehta arranged ₹30,000 from a private trust in Mumbai. That settled the only question that mattered.
I booked an Air Canada ticket.
It would be my first international flight.
***
I left India with a suitcase of clothes and a head full of nervousness. My itinerary looked simple on paper: Mumbai to London Heathrow, a 90-minute layover, then onward to Toronto.
Heathrow, however, was not an airport. It was a small universe.
I landed, looked around, and immediately felt out of place. Everything was enormous—corridors that never ended, signboards that seemed to multiply, people walking as if they were late for something important. I did what a small-town traveller does when he wants to appear calm and “international”: I slowed down. I wandered past duty-free shops. I tried not to look rushed.
I didn’t realise that in aviation, a 90-minute layover is not a relaxed stroll. It is a test.
When I finally reached the transfer desk for the Toronto flight, the staff member looked at my ticket and shook her head.
“Sir, your flight has already departed.”
For a second, I couldn’t even respond. The sentence landed like a slap. I was alone in London. I had limited foreign currency. My luggage—most likely—was already flying to Canada without me. I stood there feeling ridiculous and helpless, like a child who has lost his mother in a crowded market.
Then I did the only thing left. I walked back to the airline desk and pleaded.
“I’m a doctor from rural India,” I said. “I’m going to learn how to treat patients better. I don’t have money for a new ticket. Please help me.”
The woman behind the counter studied my face for a moment. Then she softened. She typed quickly, printed a boarding pass, and handed it to me.
“There’s a seat on the next flight,” she said. “It leaves in an hour. Run.”
I ran.
I reached the gate breathless and humbled, with a new rule stamped into my mind: never treat a transit lounge like a picnic spot.
***
By the time I landed in Toronto, the panic had drained out of me. And then I saw a familiar face.
Dr. Nafisa Kapadiya, an MGIMS alumna, was waiting at the airport. She had graduated from Sevagram, done her MD in Radiology at Tata Memorial Hospital, and was now settled in Toronto. Despite my delay, she and her husband had waited patiently.
“Welcome to Canada, Sir,” she said, smiling.
That one sentence brought me back to earth. That evening, sitting in their warm home, we spoke about Sevagram—teachers, wards, old friends, and the strange way a small rural institute stays inside you even when you move continents. MGIMS alumni carry that bond quietly. You recognise it instantly.
I stayed with them for a night. The next day, I travelled to Hamilton and checked into the university hostel.
***
The McMaster workshop felt nothing like the conferences I was used to in India. There were no long speeches and no ceremonial lectures. It was serious work from the first hour.
The programme was led by giants—Dr. Deborah Cook and Dr. Gordon Guyatt. There were around ninety participants, mostly from North America. I was one of the few from a developing country, and for the first day or two, I felt that difference keenly.
We were divided into small groups by specialty—eight participants, two tutors, and one person who surprised me the most: a librarian.
At MGIMS, librarians were caretakers of shelves. At McMaster, the librarian sat with the clinical group like a key team member. She taught us how to search PubMed and Cochrane properly, how to frame a clinical question, how to separate a good paper from a confident paper.
That was a new idea for me: that finding the right answer is a skill, not an accident.
***
A large part of the teaching happened through role-play. It sounded childish when I first heard it. It turned out to be brilliant.
One person played the senior consultant—confident, experienced, and allergic to new evidence. Another played the eager junior doctor trying to introduce a guideline without insulting the boss. We acted out the conversations we all know too well, the ones that happen in wards and ICUs when “experience” and “evidence” collide.
McMaster taught me something I wish we taught residents early: being right is not enough. You have to communicate without bruising egos.
Before applying any new research, we were trained to ask three questions:
Is the study valid?
What are the results?
Will it help my patient?
For five days, from morning to evening, we lived inside those questions. We argued over P-values. We dissected confidence intervals. We learned to say, without shame, “I don’t know.”
By the end, I understood what Madhu meant. I wasn’t returning with just notes and handouts.
I was returning with a new operating system in my head.
Sevagram in the UK
After the intensity of McMaster, I crossed the Atlantic. My old friend Dr. Mike Galvin—a long-standing ally of MGIMS—had choreographed the visit with meticulous care. The itinerary was split into two distinct halves: the professional, involving lectures in Leeds and London, and the personal, a quiet pilgrimage through the MGIMS family scattered across Britain.
I landed in a country that felt oddly familiar. It wasn't the weather or the food; it was the people. Everywhere I turned, I ran into someone who spoke my language—not English, but Sevagram.
My base was Wakefield in West Yorkshire. I stayed with Agam Jang and her husband Suresh Kumar, both Class of 1985. They were living in on-campus accommodation, navigating the grueling process of retraining for the UK system. Agam was a Senior House Officer then, moving with that breathless, early-career velocity I knew so well.
One morning, as she rushed to the hospital, I found myself standing in their living room, ironing the school dress of their five-year-old daughter, Alakh. It was a domestic scene that would have looked perfectly ordinary in Wardha, yet here it was unfolding in Yorkshire. Two decades later, Agam and I still laugh about it over the phone. Alakh is a doctor now, having stepped into the very shoes I saw her parents lace up that morning. In that small act of ironing a child's dress, the formal label of "Visiting Faculty" evaporated. I was simply a family friend trying to be useful.
***
Mike lived in Ackworth, a village of old, solid stone houses that seemed to have grown directly out of the landscape. Mike was a man of firm routines and fierce loyalties. His children often nudged him to move closer to them, but he refused. He liked his village. He liked his house. End of discussion.
His wife, Hazel, was warmth personified. She ensured that this vegetarian doctor from rural India was never once made to feel like a culinary burden. Mike hosted a dinner for me—easy hospitality, gentle laughter, and the kind of conversation that makes you forget the thousand miles of ocean between you and home. Between the soup and the dessert, we compared the NHS with our Indian system. The logistics differed, but the heartbeat was identical: too many patients, too little time, and doctors trying to bridge the gap with nothing but their wits.
Hazel passed away a few years ago, after a brave battle with lymphoma. Mike’s connection to Sevagram, however, remained unbroken. As recently as 2023, he returned to participate in the Medico Friends Circle (MFC) meeting. Watching him engage in our heated, four-decade-long debate on public health ethics, I realized that some friendships aren't just personal; they are philosophical.
***
The professional peak of the trip was a talk at Pinderfields Hospital. I was charmed to learn the name came from the "Pinder"—an old town official tasked with impounding stray animals. It sounded like a detail from an English storybook.
I spoke about MGIMS—the village camps, our pro-poor philosophy, and the daily, gritty compromises of practicing medicine far from the luxuries of a metropolis. I explained how we kept care affordable without cutting corners on quality.
Midway through, I felt a jolt of genuine nervousness. Sitting in the audience was Dr. Maurice King.

To anyone in public health, Maurice King is a giant. His seminal work, Medical Care in Developing Countries, shaped our entire worldview. For a fleeting second, I wondered what a doctor from Wardha could possibly teach the man who wrote the bible of resource-limited medicine. But he was the definition of grace. His questions were not tests; they were genuine inquiries into how we managed critical care in Sevagram. It was the highest form of compliment: serious attention from a master who did not give it lightly.
***
The rest of the journey was a moving reel of old students. MGIMS had travelled much further than we ever imagined back in the 1980s.
In Leeds, I found Vandan and Veena Zamvar in a modest hospital apartment. In Edinburgh, I visited Vipin Zamvar (Bhavana’s cousin), now a Consultant Cardiothoracic Surgeon. He showed me the Royal Infirmary—gleaming, modern, and efficient. Yet, when he spoke of his patients, the tone was familiar: serious, involved, and quietly proud. What struck me most wasn't his surgical theatre, but the community centre where he volunteered his time for cardiac patients. No spotlight, no fanfare. Just a surgeon giving back.
In Aberdeen, I stayed with Muthu Kumar and Sonali (Class of 1985). Scotland was a landscape of grey stone and biting cold. It was there that I performed the ultimate ritual of the Indian father abroad: I bought the Harry Potter audio series for my daughter, Ashwini. In 2003, those tapes felt like carrying back a suitcase of gold.
In London, I stayed with Monica Ahuja (Class of 1982), an outstanding student who had done her MD under my wing. She was then a Registrar in Oncology, newly a mother to her son, Rahul. Seeing her so calm and capable in a high-pressure North London ward gave me a deep, quiet happiness. (Monica has since moved to Perth, Australia, continuing the diaspora's reach.)
***
My final stop was Oxford, staying with Sadhana Bose (Class of 1985), who had built a formidable career in public health. Through her husband, I secured a meeting with Dr. David Warrell, the editor of the Oxford Textbook of Medicine and the world's leading authority on snakebites.
We spent two hours discussing a problem that was a daily terror in Vidarbha but a clinical curiosity in Oxford: antivenoms, transport delays, and the subtle clinical signs that distinguish a lethal bite from a terrified patient.
It was surreal—sitting in the shadow of Oxford’s spires, talking about Indian cobras with the man who wrote the definitive text. Yet, it felt right. Medicine has a way of shrinking the globe until the most unlikely rooms are connected.
***
I returned to Mumbai on British Airways with a suitcase of gifts and a head full of memories. But the real weight I carried was pride.
The students we had taught in the dusty wards of Sevagram were now healing hearts in Edinburgh, fighting cancer in London, and shaping health policy in Oxford. Our little institute had quietly gone global. For those ten days, it felt as though Sevagram hadn't stayed behind in Wardha; it had come along with me.
Labours of Love
When I look back at three decades in Sevagram, my mind does not wander to the sterile hum of the lecture hall or the polite boredom of committee meetings. It goes to a smaller, messier place: my office desk.
I see faces. I see young MD residents, eyes rimmed with the specific, heavy fatigue of thirty-six-hour duties, sitting across from me and clutching sheaves of paper they hoped would eventually become a thesis. To the outside world, and perhaps even to the National Medical Commission, an MD thesis is a mere formality—a black-and-gold bound volume destined to gather dust on a library shelf, sandwiched between years of forgotten data.
For me, it was never a formality. It was a rite of passage. It was a shared struggle to wring a single drop of truth from a sea of noisy clinical data.
I was not an easy guide. I confess this now with the safety of retirement. In my younger days, I was viewed not just as strict, but as a terror. I demanded a discipline that many found unreasonable. I lost my temper when p-values were misunderstood. I sent exhausted residents back to the wards to collect data again or threw drafts into the bin because the grammar was sloppy. I can see now how that must have felt to a twenty-five-year-old doctor. But my intention was never to harass; it was to instill a singular, terrifying standard: if a document carried the Sevagram name, it had to be bulletproof.
***
This archive records the lives and labors of thirty-two residents in Sevagram. I suspect—indeed, I am certain—that few enjoyed the work. During the frantic years of residency, a thesis is rarely a pursuit of truth. It is a hurdle; a bulky ghost let loose by the university to haunt a doctor through three years of training.
I have yet to find a student who claimed to love the task. None genuinely thanked destiny or their guide for the chance to master the mechanics of research. One should never trust the "Acknowledgements." Fifteen years ago, the university removed that section to keep the manuscripts anonymous. Before then, it portrayed guides as patient demigods of wisdom—the sole reason the work ever saw the light of day. The reality was often the opposite.
The thesis is a forced march through a desert. The traveler hates every step and finds no joy in the sand, yet he knows he must reach the other side if he is ever to be called a physician.
A young doctor’s priority is the bedside. He wants to master clinical skills and ICU procedures. He needs time to digest the two voluminous editions of Harrison's Principles of Internal Medicine. Without that, he cannot clear the MD hurdle or find the confidence to practice medicine. I do not blame them for viewing the thesis as a nuisance; I was in the same boat in 1980, treating my own manuscript with the same weary resentment.
Furthermore, a medical degree does not grant the gift of data management. Most residents arrived with little idea of how to collect evidence, let alone how to clean, analyze, or reference it. In the early years, they wrung out manuscripts by hand. They suffered the labor of physical rewriting and the whims of professional typists. Only when the computer became universal were residents freed from the caprice of the stenographer to type their own thoughts.
Be that as it may, here is the record of those thirty-two journeys.
It began with the rhythmic clack-clack of the typewriter. Those were the days of carbon paper and the sharp, chemical scent of correction fluid—the era where a single typo on page 80 could induce a minor nervous breakdown.
Monica Ahuja was the first to break the mold. A Mumbai girl from Borivali, she was studying the prognostic value of stress tests after a heart attack. While the rest of the department was drowning in handwritten drafts, Monica quietly rebelled. She carried her manuscript to Baroda because a friend there had access to a computer—a machine then as rare as a unicorn in Sevagram. She returned with a manuscript that looked like it had fallen from the future: crisp, laser-printed, and devoid of the smudge marks that defined our era. That thesis didn’t just impress me; it frightened me. It signaled that the world was moving, and we had to move with it.
Not everyone had the stomach for the long haul. Vijay Subbarao lasted exactly fifteen days. He took one look at the rigor I required, realized that Sevagram—and perhaps the particular brand of academic penance I practiced—was not the canvas for his life, and left. He was right to do so. Some people change continents, but they rarely change their nature. Vijay moved to the United States and became an accomplished cardiologist in Denver, the city where Madhuri Dixit also lives. Today, when he isn't fixing broken hearts in his cath lab, he spends his time riding his bike, reading, and practicing photography.
***
Then there was Anju Gupta, Class of 1982. She had fallen in love with Irfan, a junior, transformed into Anjum Amreliwala, and brought a fierce, quiet determination to her work. Anjum was my partner in a new craft I had just brought back from Mumbai: fiber-optic bronchoscopy.
We were threading thin, lit tubes into the lungs of patients to see if "bronchial washing" could catch tuberculosis bacilli that routine samples missed. Anjum was allotted this topic—a top-down decree from guide to student that remains a stubborn tradition in Indian medical colleges today. We hand out topics like inheritance, and students accept them like fate.
May 1991 was a month of heavy air. Rajiv Gandhi had just been assassinated; I recall hearing the news on the platform at Itarsi station, feeling the specific chill that ripples through a nation when a leader falls. While the country mourned, Anjum was in the final phase of her thesis. She was also full-term pregnant.
In those days, the postal service was our only "shared drive." I was in Bhopal; Anjum was in Jalgaon. Every few days, a thick brown envelope would arrive. I would bleed red ink all over her drafts and post them back. On June 18, 1991, the race ended in a tie. Anjum delivered her first baby girl, and she delivered her thesis. We never published it—a mix of laziness and the relentless pace of the wards—but it remains a quiet biography of a summer of red ink and a June baby.
***
Parimal Sarkar, Class of 1985, arrived from the far reaches of Tripura. He survived on the unadvertised kindness of peers who pooled money for his food. He was a brilliant, silent boy who navigated Hindi and English with a thick, melodic Bengali accent. He was too poor to afford the trip home to Agartala, so he stayed in the hostel, a permanent fixture of the campus.
His thesis was pure Sevagram: The diagnostic value of percussion in assessing heart size.
We were born and brought up on the holy trinity of eyes, ears, and hands. Parimal spent two years tapping on chests, listening for the transition from the resonant thud of the lungs to the flat dullness of the heart. He was trying to prove that a doctor’s touch could still compete with the machine.
Alas, even Hutchison’s Clinical Methods has now quietly amputated percussion from its chapters on the heart. It is a discarded skill. But Parimal’s journey did not end there. The boy who once relied on classmates for a meal is now a Professor of Medicine in Agartala. He is no longer the silent student; he is the mentor, likely teaching a new generation that there is still truth to be found in the tips of one’s fingers.
***
Others followed, each taking a slice of the human condition. Dhanraj Singh spent his residency palpating spleens, asking the oldest question in medicine: Is it really enlarged? Manoj Singh explored the mystery of fever, trying to quantify how accurately a patient knows their own body temperature before the thermometer touches them. Priya Badam and Vaishali Solao walked the wards looking at stroke patients, trying to predict subtypes by clinical presentation alone, while Ravindra Indra hunted for the hidden signs of hypothyroidism in those who simply looked "tired."
These were not abstract inquiries. They were battles against death. Amandeep spent his nights in the ICU, asking why patients with venomous snake bites were dying despite our best efforts. Sumedh cataloged the grim spectrum of pesticide poisoning, a tragedy that haunts the cotton fields of Vidarbha. Madhuri Meena looked at diagnosing malaria with rapid tests, while Swati Waghdahare dusted off century-old textbooks to see if the classic signs of meningitis were science or merely medical folklore.
***
I had one odd habit: I did not just supervise; I infiltrated. I would sit with residents until midnight, typing their drafts and obsessing over the font size of their references. I was the ghostwriter who couldn’t help himself. If a sentence was clumsy, I physically couldn't leave it alone. I wanted the English to be as precise as the science.
This once led to a moment of supreme comedy. A resident—now a successful oncologist—walked into my office, saw the pristine, finished manuscript I had largely polished, and asked with total innocence:
"Sir, since you have done so much... can you also write the Acknowledgement section for me?"
I laughed so loud I startled the pigeons on the windowsill. "My dear friend," I asked, "How do I thank myself? Do I write a paragraph about how wonderful Dr. Kalantri is and sign your name to it?" That was the limit. I stopped writing Acknowledgements.
The real work, however, happened at my dining table. Residents would arrive after rounds, hungry and hollowed out. This is where Bhavana, my wife, became the silent partner in all thirty-two theses. She never understood the p-values, but she understood the hunger. She served endless tea, cooked late-night dinners, and turned our home into a sanctuary. When these doctors meet me today in the UK or Australia, they rarely talk about statistics. They talk about Bhavana’s dal. They remember the warmth of the kitchen more than the chill of the library.
***
I eventually forced the department into the digital age—Word, Excel, EndNote—treating software as a weapon against error. But one rule was absolute: the resident was always the first author. The sweat was theirs. The glory had to be theirs.
Most of these thirty-two did not become career researchers. They became practitioners and teachers. For a long time, I felt a pang of failure about that. I wanted to build an army of scientists. But I see it differently now. The thesis was never really about the book; it was about the mind.
It was meant to teach a doctor how to think. How to spot the lie in a glossy pharmaceutical brochure. How to respect the uncertainty of biology. How to understand that a "significant P-value" is not the same thing as the truth.
Those black-and-gold books sit in the MGIMS library now. The paper is yellowing. The protocols are outdated. But to me, they are a ledger of our lives together—a record of the nights we spent trying to stop death with nothing but a stethoscope, a question, and a typewriter.
***
The Double-Blind Trial
My career as a postgraduate guide began in 1988 with Monica Ahuja. She was an MGIMS student from the 1982 batch, and her task was to decipher the prognostic significance of treadmill tests in patients who had recently survived the wreckage of a myocardial infarction. At the time, I was what one might call a "raw" guide. I possessed the title and the white coat, but I was entirely untrained in the formal architecture of a thesis. I knew little of statistics and even less of epidemiology. Like many of my contemporaries, I was a bush-pilot flying by sight, learning the process through a messy series of trials and errors.
The early years were defined by technical frustration. I harbored a long-cherished desire to master the tools of modern research, but they remained just out of reach. That changed when Madhukar Pai entered my life. It was through our association that I finally developed a firm grip on biostatistics and the digital instruments that make sense of clinical chaos. I learned to navigate the sharp corners of Stata, to organize a sprawling EndNote library, and to coerce Microsoft Word and Excel into doing my bidding. This newfound fluency allowed me to direct my students toward clinical questions that actually mattered in the wards of Sevagram.
The topics we tackled were as diverse as the patients in our waiting rooms. We interrogated the human body and the systems we use to measure it. P. Sarkar looked at the utility of palpation in assessing cardiomegaly, while M. Singh tested the simple validity of a hand on a forehead to screen for fever. We explored the grim realities of rural life through the clinical profiles of snake bites and pesticide poisoning—work carried out by residents like Pranay Taori and Abhay Kelkar. Later, we moved into the realm of neurological scoring, where Priya Badam and Vaishali Solao evaluated the Siriraj and Guy’s hospital stroke scores to see if they held water in a rural Indian setting.
Yet, as I look back on these thirty-two residents, regret colors the memory. The workflow followed a predictable, flawed pattern. My postgraduates would type their drafts and send them to me via email. I would then sit at my desk, delete their clunky phrasing, retype their observations, and polish the prose until it shone. I would deliver them a final, pristine copy. In doing so, I committed a pedagogical sin. I robbed them of the freedom to stumble. By smoothing over their mistakes, I prevented them from developing the very skills I had worked so hard to acquire. Most of my postgraduates wrote their theses passively; they emerged as degree-holders, but few emerged as confident researchers.
The Integrity of the Byline
In the competitive world of Indian medical academia, there is an unwritten rule: the names of heads of departments or senior guides must occupy the prestigious first or second authorship slots. I found this practice a quiet form of intellectual theft. If a student spends two years laboring over a project, their name should lead the charge in the journals.
I took a different path. It is a matter of quiet satisfaction that many of my MD residents saw their thesis work transition from a bound volume to high-impact medical journals as first authors. Monica Ahuja led the way with her work on treadmill tests. Parimal Sarkar and Dhanraj Singh Chongtham published rigorous interrogations of the physical exam—Sarkar on the utility of palpation in cardiomegaly and Singh on the clinical signs of splenomegaly and ascites. These were not mere student exercises; they were contributions to the global understanding of bedside medicine.
Others followed. Manoj Singh published on the screening of fever, while Priya Badam and Vaishali Solao saw their evaluations of stroke scores reach a wider audience. Ravindra Indra contributed to the diagnosis of hypothyroidism, and Samir Patil documented risk factors for myocardial infarction in our rural setting. Even complex cross-sectional studies reached publication under the primary authorship of the residents: Geetha Devi on brain lesions, Amandeep Singh on snake bite mortality, and Trunal Lokhande and Swati Waghdhare on the accuracy of physical signs in pleural effusion and meningitis. Madhuri Meena rounded out this tradition with her work on undifferentiated fever.
By stepping back and taking the final slot, I hoped to teach them that the true reward of research is not the hierarchy of the byline, but the integrity of the evidence. My Google Scholar profile serves as a ledger of these shared successes—a record of what happens when a guide acts as a steward rather than a master.
The Evidence of the Wards
My research has never been about the vanity of citation counts; it has been a systematic attempt to turn the daily observations of a rural hospital into data that could help others. The research was born from the dilemmas we faced at the bedside. We looked at the prevalence of tuberculosis infection among our own healthcare workers in a study published in JAMA, and we interrogated simple tools, such as using pallor to detect anaemia, finding that our eyes are rarely as precise as the laboratory. We didn't just look at the high-tech; we also documented the "diagnostic uncertainty" of non-malarial fevers to reduce the irrational use of antimalarial drugs in rural OPDs.
In the mid-2000s, I began a collaboration with Madhukar Pai that eventually yielded some three dozen papers, including systematic reviews on phage-based tests and line probe assays for rapid drug resistance.
The education of a researcher is often a spectator sport. In August 2004, before I moved into a studio in Berkeley, Madhu graciously hosted me for a fortnight. I would watch him work, his eyes fixed on every line of a manuscript, revising and refining until the prose passed his own particular acid test. He was a man of extreme meticulousness; he labored to ensure the final draft was flawless, aiming for the exacting standards of journals like JAMA.
It was this rigor that saw his PhD thesis on tuberculosis—work actually performed in the wards of Sevagram—find its home in the pages of JAMA with Madhu as the first author. When the news arrived, the joy in his eyes was impossible to describe. It was the look of a debutant test cricketer who had just struck a century in his first innings.
My work has also been a tool for advocacy—from exploring the crisis in access to essential medicines to campaigning against industry sponsorship of medical conferences. During the pandemic, we insisted on the rigor of well-designed trials for Hydroxychloroquine and Inhaled budesonide over the noise of anecdotal "cures." This body of work is the "paper trail" of my life in Sevagram—evidence that we tried to leave the science a little clearer than we found it.
The Fall of the Bound Volume
This realization eventually grew into a public critique. I have argued that we must stop the mandatory PG thesis. In its current form, it has devolved into a "Double-Blind Trial": the student is blind to the methodology, and the guide is often blind to the science. And both have no idea what is going on until the thesis is submitted to the university. You can read my full indictment in The Double-Blind MD Thesis.
The tragedy of the modern thesis is that instead of teaching ethics, we are inadvertently instilling the habits of data manipulation and plagiarism. It is a system running toward a cliff, as I noted in The Fall of the MD Thesis. We force students to "cook" data to satisfy a disinterested examiner, teaching intellectual dishonesty before the career has even begun.
We would serve our students better if we abandoned this bound volume of fiction. Instead, we should teach them to critically appraise a paper on diagnostics or clinical trials. If we taught them how to read a study and apply its truth to the patient in front of them, we would produce physicians who practice with wisdom. A doctor who can interpret a likelihood ratio at two in the morning is far more valuable than one who has spent three years assembling a thesis that will never be read again.
Amar Jesani and the IJME
Amar Jesani was the kind of man you didn’t forget after meeting once. If the Medico Friend Circle (MFC) was the soul of public health activism in India, Amar was its restless, unrelenting conscience. I had known him since the early 1980s, and his annual visits to Sevagram were events we looked forward to—with a mix of intellectual excitement and a little nervous respect.
He was physically striking. Behind thick, scholarly glasses sat large, searching eyes that always seemed to be reading between the lines of your soul. When Amar spoke, he didn’t just fill a room; he commanded it. His voice was a unique instrument that could pivot from profound empathy for the marginalized to a searing, white-hot anger at the medical establishment’s indifference.
In the breaks between sessions, he would step outside to smoke—a lean, quintessential leftist figure wrapped in a cloud of tobacco. Amar specialized in calling a spade a spade, and he had a particular talent for cutting people down to their proper size if he sensed a hint of pretension. I often sat in the audience, fascinated and slightly terrified, wondering: How does he say these things so openly? I was careful by temperament; Amar was a storm.
Decades later, that bond remained. During the height of the pandemic, he invited me to deliver a talk on the Ethical Challenges of Research in a Pandemic and to co-author a critical editorial with Sahaj Rathi on the ethics of clinical research and practice in India during Covid-19.
***
The Birth of a Rebel Journal
In the early 1990s, Amar and a group of like-minded colleagues in Mumbai founded the Forum for Medical Ethics. By 1993, they had birthed a newsletter called Medical Ethics, which evolved into Issues in Medical Ethics (1996), and finally took the name it is known by today—the Indian Journal of Medical Ethics (IJME)—in 2004.
The journal was a rebel from the start. It refused to behave like a typical medical publication. It didn't charge authors a paisa to publish. It made its content freely available online in an era of expensive paywalls. Most radically, it refused a single rupee of advertisement money from drug companies or medical device manufacturers. In a world where journals often survive on the patronage of Big Pharma, IJME chose a precarious independence. It ran on a shoestring budget: a few donations, two underpaid staff members, and a mountain of volunteer hours.
***
The Reluctant Editor
Sometime around the turn of the millennium, Amar approached me with an offer that felt more like a summons.
“We want you to join as an Associate Editor,” he said.
The Editor-in-Chief then was Dr. Samiran Nundy—the former head of GI Surgery at AIIMS and a towering figure in Indian medicine. I felt completely out of place. I was a physician from a rural medical college, a man of the wards, not of the printing press. I had never edited a national journal. I had only recently acquired an email account and was still learning how to navigate the digital world without embarrassing myself.
“I don’t think I can do this,” I told Amar.
He didn’t accept my refusal. Sandhya Srinivasan, the journal’s executive editor, didn’t accept it either. Between the two of them, they pushed me—gently but firmly—into the role.
***
Learning the Craft
Those three years were a steep, sometimes grueling tutorial. Sandhya became my guide. She was sharp, quick-witted, and possessed a mind that often moved faster than I could follow. She taught me the invisible craft of editing: how to tighten a paragraph without strangling the author’s voice, and how to remove clutter without removing meaning.
My job was to solicit manuscripts and support Dr. Nundy. In the beginning, I felt like a clumsy intruder. I was plagued by the sense that I had been "prematurely recruited"—that they wanted a voice from the public sector and a teaching hospital who shared their philosophy, even if that voice lacked the technical polish of an experienced editor.
I often felt I wasn't doing enough. I wasn't a "natural" at the blue-penciling and the back-and-forth of peer review. When I eventually stepped down in 2003 to leave for my sabbatical at UC Berkeley, I did so with a lingering sense of embarrassment. I felt I hadn't quite lived up to the towering expectations Amar and his colleagues had for the role. Looking back, I realize I was perhaps too hard on myself; I was learning a new language in the middle of a crowded room.
***
Keeping Medicine Human
Despite my self-doubt, those years were transformative. I found colleagues who became lifelong friends—people like Dr. Sanjay Nagral and Dr. Sanjay Pai. Our connection went beyond the exchange of emails; we were all trying, in our fragmented ways, to keep medicine human.
I started writing, too. I co-authored pieces on the ethical quagmire of government-funded antiretroviral therapy for HIV/AIDS and explored the uneasy culture of medical consumerism in an article titled, “When is enough, enough?”
When I look back, those three years with IJME feel like a vital turning point. If Evidence-Based Medicine taught me how to treat, IJME taught me why we treat—and, more importantly, who gets left behind when the system is rigged. By the time I boarded the flight for California, I felt quietly prepared. Bhavana had dragged me into the digital world; Madhukar Pai had sharpened my clinical lens; and Amar Jesani had made sure my moral compass stayed wide awake.
The Awards Paradox
Recognition is a strange thing; it feels good for about five minutes before it starts asking questions you didn’t plan to answer. In May 2008, the institute nominated me for the Best Teacher Award of the Maharashtra University of Health Sciences (MUHS), Nashik. It was a significant honour. In a state crowded with medical colleges, being singled out as the "best teacher" is no small compliment.
But my satisfaction was short-lived. I soon learned that my close friend and colleague, Dr. M.V.R. Reddy, the Head of Biochemistry, had also been considered. The rules were simple and rigid: one institute, one nomination. I could immediately see the awkwardness this would create—two friends vying for one title, leading to forced smiles, careful conversations, and that invisible comparison in the staff room that no one admits but everyone feels.
Reddy wasn’t just "good at teaching." He made biochemistry—a subject most students flee from—feel alive. He possessed that rare gift of making enzymes and pathways sound like a story rather than a syllabus. So, I wrote to the Dean and asked him to withdraw my name, stating plainly that Reddy should be the nominee. An award is never worth disturbing a friendship that had quietly become family.
On July 30, 2008, MUHS announced the winner: Dr. M.V.R. Reddy. I felt genuinely happy. I wrote a congratulatory email to the faculty and meant every word. Watching him receive the award, I didn’t feel I had "lost" anything; if anything, I felt lighter.
Bureaucracy, however, has stamina. The Dean tried again the next year, and then again. Finally, on February 22, 2009, I sent a direct email declining the nomination permanently. I explained that I did not consider myself an exceptional teacher—only an average one—and that singling out one person often obscures the quiet, collective work of a faculty. It wasn’t false modesty; I have simply always believed that teaching is a team sport.
***
Fourteen years later, in September 2022, I was in Chandigarh visiting my daughter Amrita when I received a call from Dr. R.B. Kalamkar. He was my senior from the 1971 batch in Nagpur, someone I had worked alongside during my residency.
"The Association of Physicians of India (API), Vidarbha Chapter, wants to honour you," he said.
My reflex was ready. No, no… please don’t… I had practised this refusal for years. But then he added a line that stopped me cold.
"It is the Dr. B.S. Chaubey Award."
Dr. Chaubey’s name has a way of straightening your spine, even decades later. He was my mentor, my examiner, and—on some days—my nightmare. He shaped the way I think as a physician. His standards were brutal, but they were never casual. Over the next few days, calls poured in from friends and colleagues—Dr. Viresh Gupta, Dr. Nikhil Balankhe, Dr. Deshpande—all urging me to accept. This was not a distant university selecting names from a file; this was my own fraternity. These were people who had watched me grow older, slower, and greyer, yet still turn up to work.
So, I said yes.
***
The ceremony took place in Chandrapur. My former teacher, Dr. S.M. Patil, handed me the citation while the audience applauded. The words were generous—too generous, if you ask me. When my turn came to speak, I had no desire to list achievements or sound like my own obituary. Instead, I took them back to Ward 23 of GMC Nagpur, circa 1980.
I was a first-year resident then. I had admitted a young patient with leg weakness and a distended bladder—a classic case of acute transverse myelitis. But standing in front of Dr. Chaubey, my brain went blank, the way it does when fear hijacks reason. When he demanded the diagnosis, I blurted out, "Guillain-Barré syndrome, sir."
He didn’t shout immediately, which would have been easier. He went quiet first—the dangerous kind of quiet. Then he pulled back the sheet, pointed out the signs I had missed, and turned to Dr. Patil.
"Patil," he said, his voice cutting through the ward, "God save this student. Poverty of thoughts and bankruptcy of ideas."
The audience in Chandrapur laughed when I narrated this. I smiled too, but inside, I remembered exactly how it felt that morning: the hot flush of shame, the dry mouth, and the desperate wish to disappear behind the case sheet. That sentence stayed with me for years—not as an insult, but as a warning. That day I learned a simple truth: in medicine, ignorance is not harmless. It can hurt people. The fact that it embarrasses you in public is merely the smaller problem.
***
When I looked at the award later, I didn’t see a trophy. I saw a long road. I saw myself refusing a nomination in 2008 because I didn’t want an award to stand between friends. And I saw myself accepting one in 2022 because it carried the name of the teacher who once scared the nonsense out of me.
The MUHS award would have been just a certificate. The API award felt like something else entirely. It was a full stop. And, in a quiet way, a return to Ward 23.
The California Dream
I first noticed Madhukar Pai at an annual meeting of the Medico Friend Circle — one of those gatherings where idealism and exhaustion arrive in equal measure, and where the conversations that matter happen not in the sessions but over tea.

He was younger than me by thirteen years, but he carried himself with the quiet certainty of someone who had already decided what kind of doctor he wanted to be. A Madras Medical College graduate from the 1987 batch, he had chosen Community Medicine at CMC Vellore over the safer, shinier clinical specialties — a choice that, in Indian medicine, requires either courage or indifference to peer opinion. Madhu had both.
He spoke about public health, epidemiology, and biostatistics with the ease of a man discussing the weather. Most clinicians treat these subjects the way they treat difficult relatives: greeted politely at family functions and avoided thereafter. Madhu treated them as the most interesting problems in medicine. Slowly, over several such meetings, his enthusiasm began to do what enthusiasm sometimes does — it became contagious.
Around 2000, between sessions at one of those MFC meetings, Madhu turned to me and said: "Why don't we do a workshop on epidemiology at MGIMS?"
I said yes before he could change his mind.
What followed became a small legend in Sevagram. For three days, thirty residents from Medicine, Paediatrics, and OBGYN sat through eight-hour sessions and — remarkably — did not attempt to escape. Madhu had a gift I have rarely seen in academic medicine: he could make a P-value feel like a story. He explained how bias enters a study the way a draught enters a room — quietly, through gaps you did not know existed. He turned confidence intervals from a source of examination anxiety into something you could actually use at a bedside.
For residents drowning in their MD theses, he was not simply a visiting faculty member from Canada. He was a lifeline.
I watched him work. I watched how he held a room — not through authority, but through clarity. I noticed how he nudged my younger colleagues, Rajnish Joshi, Kaustubh Gokhale, and Anurag Bhargava, not with instructions but with questions. Have you thought about this? Have you read that? Have you considered why the study was designed this way? He was building researchers the way a good gardener builds a garden — by improving the soil, not by pulling at the plants.
Somewhere between the tea breaks and the chalkboard scribbles, a friendship formed. I did not fully understand, at the time, where it would lead.
The internet arrived at Sevagram around 2003 — late, unreliable, and rationed like electricity during the monsoon.
I remember the day I opened a Rediffmail account for the first time. I typed the address into the browser with the concentration of a man attempting a procedure he had never tried before. Then I wrote to Madhu in Canada and pressed send. The screen flickered. Somewhere across the world, a server received what I had written. I sat back and waited, not entirely sure I believed it had worked.
I had held a USA.net account before that, but rarely used it, and whatever was exchanged there is lost now — Rediffmail offers to retrieve old messages for a fee, but two decades have defeated even that. What I do have is the memory of what came back.
Madhu's reply arrived like a small celebration.
He wrote,"When I received your email, I almost fell off my chair! I know downloading a 10 MB PDF takes ages at your end, but it is worth the wait. I am so happy MGIMS has joined the World Wide Web."
It was through this thin, fragile thread — dial-up connection, flickering screen, the occasional power cut mid-sentence — that he planted the idea that would alter the course of my professional life.
It did not arrive as a grand proposal. It came as a single line, almost casual, tucked at the end of a message:
Apply for an MPH at Berkeley.
Six words. I read them twice, then a third time. I was not sure if he was serious
I sat with that suggestion for longer than I should have.
I was a full professor with a ward full of patients, a department that depended on its routines, and a family in Sevagram. My daughter was young. Bhavana was managing a career and a household simultaneously, as she always had. Leaving for a year felt selfish in the specific way that only physicians understand — the guilt of abandoning the people who need you, compounded by the knowledge that someone else will manage, and the uncomfortable suspicion that they might manage perfectly well.
But something had begun to shift in me. I had spent two decades practising medicine with skill and sincerity, but I had not always known why some things worked and others did not. I wanted to understand research from the inside — not just read papers but know how to interrogate them. I wanted to ask better questions. I wanted to know how to answer them honestly, with the right tools, in the right sequence.
Madhu understood this before I had fully articulated it to myself. He did not lecture me or send a prospectus. He simply kept the door open — a question here, a paper there, a gentle nudge at the right moment. He had received support from the Fogarty AIDS International Training Program, which had taken him first to UC Berkeley for an MPH and later a PhD. He knew what the year could give a person. He wanted me to find out for myself.
In the winter of 2003, I finally wrote back.
"I'm ready."
The application process was not romantic. It was paperwork, queues, and the small humiliations that Indian bureaucracy reserves for its most motivated citizens.
First came IELTS. I scored 8 out of 9 and felt absurdly pleased — the particular satisfaction of a man in his late forties who has just proved something to no one in particular.
Then came the real test: transcripts.
I needed validated mark sheets from Nagpur University and Government Medical College, Nagpur. The records were a tangle. At one counter, a clerk informed me with complete administrative serenity that I had not completed a mandatory rural posting and owed a fine of several lakhs. I stood there for a moment, genuinely trying to remember a rural posting I had apparently skipped without noticing, in the middle of a career spent almost entirely in rural Maharashtra.
It was a clerical error. The rule did not apply to my batch.
My classmate Dr. Abhimanyu Niswade, then Professor of Paediatrics at GMC Nagpur, stepped in and quietly untangled the knots. Without him, my Berkeley dream might have ended its life in a dusty government file, stamped and shelved and forgotten.
While I chased signatures in Nagpur, Madhu was doing his own quiet work in California. He spoke to Dr. Art Reingold, Dr. Warren Lee, and Dr. Jack Colford Jr. about me — mentioning my name in rooms I would never enter, building a small argument on my behalf with people whose opinion mattered. I did not know this at the time. I learnt it later, gradually, the way you learn most of the important things people have done for you.
On 5 November 2003, I sat down to write my Statement of Purpose.
It was not simply an application form. It was, as these things sometimes become when you take them seriously, an argument with myself — written neatly, in the hope that someone in California would find it convincing.
I wrote that MGIMS had a tradition of service but that clinical research remained thin because we lacked trained mentors. That in India, for too many doctors, the MD thesis was the first paper and the last. That I wanted to return from Berkeley with the tools of evidence-based medicine and build, in Sevagram, a culture of inquiry — the habit of asking not just what but why, and then finding a rigorous way to answer.
It sounded ambitious on paper. But it was honest. And honesty, as I have learnt, is the one quality that a good Statement of Purpose cannot disguise.
On 12 February 2004, the letter arrived.
I had been accepted.
The School of Public Health at UC Berkeley had opened its doors. The Fogarty programme offered a stipend of $2,519 per month for living expenses and $200 per semester for books. I read those numbers again and again, half expecting them to rearrange themselves into something more modest.
The final hurdle was the US Consulate in Mumbai. I had heard enough horror stories about visa interviews to lose sleep over them. On 2 July 2004, I walked into the embassy with my heart doing something that felt less like beating and more like insisting.
The officer looked at my papers. He looked at me.
"Where are you going?"
"UC Berkeley," I said.
He smiled — the particular smile of a man who likes the answer he has just heard — and handed everything back.
"Good luck. You are going to a great university."
That was it. No drama. No interrogation. A simple sentence that unlocked a door.
News travels fast in Wardha. Pride travels faster.
The Maheshwari Mandal insisted on a felicitation. I tried to protest — I had achieved nothing yet, I told them; I had only secured admission — but they were not interested in my logic. A function was arranged. Dr. Ved Prakash Mishra was the Chief Guest, and Shri Narayandasji Jajoo presided. Dr. Mishra spoke for forty-five minutes in his grand, rolling Urdu-Hindi, turning my scholarship into a victory for the entire city. I sat in my chair, shrinking by degrees, embarrassed by the praise yet genuinely warmed by the affection behind it.
When my turn came, I spoke for three minutes. I thanked them. I promised to do my best. And I understood something clearly that evening, in the way you sometimes understand things not when you think about them but when you are forced to speak about them in public: Berkeley might give me wings, but Sevagram would always be my roots.
In the first week of August 2004, I boarded a British Airways flight from Mumbai to San Francisco. I left behind my hospital, my ward rounds, my routines, and my family. I flew, at forty-seven, towards a new identity.
Somewhere in Canada, I imagine, Madhukar Pai already knew I would be fine

I met Madhu at the annual meetings of the Medico Friend Circle. He was younger than me, but he carried himself like someone who already knew where he was headed. A Madras Medical College graduate from the 1987 batch, he had chosen Community Medicine at CMC Vellore over the safer, shinier clinical specialties. He spoke with ease about public health, epidemiology, and biostatistics, subjects most clinicians treated like distant relatives: greeted politely and avoided thereafter.
Around 2000, at one of those MFC meetings, Madhu said, “Why don’t we do a workshop on epidemiology at MGIMS?”
I said yes before he could change his mind.
That three-day workshop became a small legend in Sevagram. Thirty residents from Medicine, Pediatrics, and OBGYN sat through eight-hour days and, surprisingly, did not try to escape. Madhu made P-values less frightening, explained how bias creeps in quietly, and turned confidence intervals into something you could actually trust. For residents drowning in their MD theses, he wasn’t just a visiting faculty member. He was a lifeline.
Somewhere between tea breaks and chalkboard scribbles, a friendship grew. Madhu had wit, stamina, and a stubborn desire to pull others up with him. He became a mentor to my younger colleagues, Rajnish Joshi, Kaustubh Gokhale, and Anurag Bhargava, nudging them towards good questions, good methods, and the right people. He himself had received support from the Fogarty AIDS International Training Program, which took him to UC Berkeley for an MPH and later a PhD.
***
The Sweet Box at the Airport
My transition from a settled life to a student life began not on a plane, but on a rain-soaked platform in Wardha. On the evening of 9 August 2004, Bhavana and I boarded the train to Mumbai. As the train picked up speed and the familiar yellow signboard of Wardha station disappeared into the monsoon mist, the weight of my decision finally sank in.
I was forty-five. A Professor of Medicine. A father. And yet I was leaving everything I had built, my home, my hospital, my family, to study across the ocean. A lump rose in my throat. I turned to the window and watched the green fields of Vidarbha slide past, hoping the year ahead would be worth this separation.
***
Mumbai, in August, was doing what Mumbai does best. It was raining as if the city had offended the clouds. The sky was a stubborn grey sheet and the roads looked like shallow rivers.
We went to see Mr PL Tapadiya’s cousin, Mr Kamal Gandhi, who had come from Kolkata for an emergency angioplasty at Jaslok Hospital. Even getting back to Thane after that visit felt like a small exam. We boarded a Mumbai local in peak hour. The compartment was packed with wet clothes, damp hair, and people pressed so close that you stopped trying to find space and simply surrendered.
It was chaotic, uncomfortable, and strangely familiar. The kind of energy you only notice when you are about to leave it behind.
***
My flight to San Francisco was scheduled for 2:00 AM. At the airport, Bhavana and my cousin Surendra stood with me near the departure gate. My niece Jyoti could not come. She had just delivered her son, Daksh.
I was preparing myself for a proper goodbye, when the check-in counter produced a small disaster. The staff told me my luggage was overweight.
For a moment I felt my stomach drop. I did not have the money for excess baggage. I did not have the patience to argue. I simply unzipped my suitcase right there on the polished airport floor and began pulling things out like a man searching for his own common sense.
Clothes. Books. Files.
Then my hand touched a large box. Bhavana had packed a kilogram of homemade sweets for me. A piece of home, carefully wrapped.
I held it for a second and then handed it back to her. “Keep this,” I said.
It was a small decision, but it felt symbolic. I walked towards immigration a little lighter, and not only in kilograms.
***
San Francisco greeted me with jet lag and a strange kind of silence. Then I saw Madhu.
He was there at the arrivals, smiling, solid, familiar. I did not realise how much I needed that one known face until I saw him. He drove me to his apartment at 1040 Jackson Street in Albany, a quiet leafy neighbourhood about three miles from the UC Berkeley campus.

Nikita was waiting at home. She was doing her MPH too. She had cooked an Indian meal and the smell of dal and rice felt like a welcome that went deeper than words. That first evening, sitting in their living room, eating warm food after a long journey, my anxiety eased.
Madhu and Nikki were my first anchors in America. Their kindness told me something simple: you are not alone.
***
A week later, it was time to stand on my own feet. I moved into Studio MN 244 at the Manville Apartments, at the corner of Shattuck Avenue and Channing Way. The building buzzed with student life. My room was on the second floor.
When I opened the door for the first time, I noticed two things: light and silence.
It was a 260-square-foot studio, tiny compared to my bungalow in Sevagram, but neat and efficient. There were light-coloured cabinets, a clean countertop, and big windows that poured in California sunshine as if it came free with the rent.
The flat was unfurnished, but it had a built-in desk, a bookcase, and internet ports that worked without coaxing. For someone who had lived all his life surrounded by family or colleagues, the solitude felt odd. There was no one to talk to when I woke up. No one to share tea with.
But there was a novelty that fascinated me: a coin-operated washer and dryer in the unit. I felt ridiculously proud the first time I managed laundry without ruining anything.
***
Soon my days fell into a rhythm shaped by geography. I had Haste Street on one side, Durant Avenue on the other. The AC Transit stop was close, but I mostly walked.
Every morning I slung my backpack over my shoulder and walked to the School of Public Health. The air was crisp and smelled of eucalyptus, roasted coffee, and something faintly salty from the ocean. I passed bookstores, cafés full of students hunched over laptops, and the mix of street performers and homeless people that gave Berkeley its strange, restless character.
In Wardha, I needed a scooter. In Berkeley, I needed only good shoes.
“Call Me Art”
The academic culture was another shock.
In India, hierarchy is built into the air. You say “Sir” and “Madam” before you even learn the person’s name. At Berkeley, I met people whose papers I had cited, and they wanted to be addressed like neighbours.
One of the first was Dr Arthur Reingold, Head of Epidemiology. I approached him with the respectful stiffness of a junior doctor. He extended his hand and said, “Call me Art.”
I froze.
For days, “Art” would get stuck in my throat. “Sir” tried to escape on its own. But Art was firm, and also gentle. He invited our entire MPH cohort to his home for dinner. I expected a formal evening. Instead, I walked into his kitchen and found him wearing an apron, cooking Indian food with a Tarla Dalal recipe book open on the counter.
That evening, I learnt a lesson I still carry: real authority does not need distance.

***
My coursework was demanding and exhilarating. I chose Epidemiology and enrolled for twelve units. The syllabus read like a wish list I had carried in my head for years: outbreak investigation, trial design, meta-analysis.
The faculty list was equally intimidating.
But the class that truly tested me was PH 250B, Epidemiologic Methods, taught by Jack Colford Jr. Jack was brilliant and fast. His slides appeared and vanished before your brain could finish reading the first line.

Madhu had the perfect description. “Jack is the Shoaib Akhtar of Epidemiology,” he said. “Before you see the ball, it has hit the stumps.”
I began typing notes like a man chasing a runaway train. The School gave me a Dell laptop and a Stata license. At night, in my small studio, I sat with that laptop and wrestled with command lines, regressions, and my own self-doubt. Some evenings I felt too old for this. Then the code would run, the output would appear, and the joy returned.
***
Living alone brought another challenge: hunger.
Back home, the kitchen had never been my department. In Berkeley, if I didn’t cook, I didn’t eat. My kitchenette became my laboratory. I began visiting the farmers’ market and saw vegetables I had only read about: artichokes, Brussels sprouts, kale. I tasted strawberries that felt like sunshine and bread that crackled properly when you tore it.
I learnt to chop onions without injuring myself. I learnt to make a basic dal. My meals were not masterpieces. They were survival food. But there was a quiet satisfaction in eating something made by my own hands.
And on days my experiments failed, Berkeley fed me kindly. Thai curries on Telegraph Avenue. Burritos that could feed two people. Pasta near Shattuck that reminded me, faintly, of home and not at all of home.
Life on Shattuck Avenue was a solitude I wasn’t used to. But it was a productive solitude. Stripped of my title, my ward rounds, and the daily noise of Sevagram, I was free to do one thing properly.
I was a student again.
The Seat on the Edge
The fall of 2004 changed the direction of my life. I was packing for UC Berkeley, telling myself I was taking a mid-career break to learn research properly. But even as my mind drifted towards California, my heart stayed in Sevagram.
Ashwini had just finished his 12th standard and was preparing for the MGIMS entrance test. For a faculty member’s child, that exam carries a special kind of pressure. You grow up on campus. The hospital corridors feel familiar. Teachers are not distant names, they are people you have greeted for years. And yet, if you don’t make it, the disappointment feels public. The whispers travel faster than the result.
That summer, our house in Vivekanand Colony felt like a pressure cooker. Biology notes lay open on the dining table. Physics formulas stared from the walls. Everyone walked softly, as if noise itself might spoil his concentration. We decided to send him to Nagpur for coaching. It was not easy, but it was necessary.
We were fortunate. Mr Raja Khapre opened his home to Ashwini and gave him a quiet corner in a busy city. My elder sister Pushpa, in Giripeth, became his refuge. Whenever the coaching centre exhausted him, he would go to her for a meal and a little comfort. A plate of her food did what no motivational talk could.
The Gandhi paper
The MGIMS entrance test is unlike any other. It has the usual three-hour paper of Physics, Chemistry, and Biology. But it also has a second paper that catches most students off guard: an essay-based test on the life and times of Mahatma Gandhi.
You cannot cram for it. You have to understand what Gandhi stood for, and why Sevagram still carries his shadow.
Before I left for Berkeley, I became Ashwini’s weekend tutor for that paper. Our Saturdays were spent with My Experiments with Truth, not with cricket or movies. We spoke about satyagraha, the Dandi March, khadi, and what it meant to live simply in a complicated world. I was teaching him for an exam, yes, but I was also trying to pass on something deeper.
***
When the results came, the news hit us hard. Ashwini had done well, but not well enough.
The staff quota had only two seats. Ashwini stood third.
In admissions, being third when there are only two seats is its own kind of torture. Close enough to taste it, far enough to lose sleep. He had also missed the cut in the open category. The house fell quiet. Nobody said much, because there was nothing sensible to say.
We did not have the luxury of grieving for long. We needed a Plan B. Fergusson College in Pune offered him admission in BSc Biotechnology. It was a good course, a good college, and a respectable path. But for a boy who had grown up watching ward rounds and treating a stethoscope like a toy, it felt like a detour.
He left for Pune, trying to look brave. We pretended to be cheerful. Inside, we were all waiting.
***
I flew to the US with a guilt that sat stubbornly in my chest. I kept asking myself the same question: was I chasing my own growth while my son’s future hung in the balance?
A few weeks into the term, a seat in the open category fell vacant. Someone withdrew. The waitlist shifted. Ashwini was next.
The call came from home. It was Bhavana. Her voice was trembling, not with worry this time, but with relief.
“He got in,” she said. “The seat opened up. Ashwini is coming back from Pune.”
I sat down. I don’t remember what I was doing before that call, but I remember the moment after it. The relief was physical. Across oceans and poor phone lines, we held on to that one sentence like a blessing.
Our son was coming home.
***
The happiness lasted a few minutes. Then reality returned.
To secure the seat, the fees had to be paid immediately. In 2004, money could not be moved with a click. There was no NEFT from a phone, no instant transfer. We were not sitting on spare cash either. Most of our savings were in mutual funds.
And I was 13,000 kilometres away.
Bhavana had to do everything. She arranged the redemption, hunted down the agent, searched for the physical papers, filled forms, signed, re-signed, and then travelled to Amravati to submit documents at the main branch. The waiting was the worst part. Every day mattered. Every delay threatened the admission.
The cheque came in time. She deposited the draft with a day to spare.
Only then did we breathe.
***
Looking back, Ashwini fought the exam. But Bhavana fought the year.
Amrita was still small then, in third standard, needing homework help, routine, and reassurance. Ashwini had gone through the full emotional cycle of hope, disappointment, hostel life in Pune, and sudden return. And Bhavana was holding the home steady through all of it.
At the hospital, she was also dealing with the chaos of launching the Hospital Information System. Anyone who has introduced a new HIS knows what it means: software glitches, angry staff, resistance, delays, and daily firefighting. Her workdays stretched to ten or twelve hours, and even after she returned home, the problems followed her like a shadow.
On top of that, she was preparing her own passport and visa so she could visit me in Berkeley. One more queue, one more form, one more deadline.
People talk about work-life balance as if it is a neat solution. That year taught us something else. For a working woman, balance is not a pose you achieve. It is a constant act of holding, adjusting, and not letting anything fall.
When Ashwini finally wore his white coat and walked into the anatomy hall of MGIMS, it was his victory. But the foundation had been laid by Bhavana’s quiet resilience. She kept the roof in place, even when everything felt unsteady.
Friends Without Borders
Friendship in adulthood is rare. Friendship in a foreign land is a lifeline.
At forty-seven, I was a professor in India and a student again in Berkeley. I lived alone, studied hard, and tried to look calm. But loneliness has a way of showing up quietly, usually when you return from a long day and the room is too silent.
About two weeks after I arrived, I was walking back from a heavy epidemiology lecture when I fell into step with three classmates. We began with the usual student talk: the syllabus, the assignments, the fear of exams, and the strange feeling of being back on the bench after years on the dais. By the time we reached the crossing where our paths split, something had already clicked.
Christine Ho, Maureen Morgan, Joseph Ezoua, and I became a small unit. An unlikely quartet: an Indian doctor, an American woman who was changing direction midstream, a physician-mother from Marin County, and a cheerful health worker from Côte d’Ivoire. We studied together, worried together, laughed together, and slowly began to feel less alone. In Berkeley, they were not just classmates. They were the family I hadn’t planned for.
***
Christine was the gentle intellect of our group. She had studied at Berkeley, gone to medical school at UCSF, and trained in internal medicine. But she wore her achievements lightly, almost as if they belonged to someone else. She was also a mother to Lee and Mika, and she carried that double load with a calm that I still admire.
In class, Christine was sharp. She saw patterns quickly and asked questions that made the rest of us sit up. She had worked at Asian Health Services in Oakland, caring for patients who did not speak English. She had seen the early tremors of SARS even before it became a headline. In 2003, she had travelled to Bihar to work on polio prevention. And when I got stuck in statistics, she became my patient teacher. She would explain again and again, without a trace of impatience, until the fog cleared.
Christine lived in San Anselmo, about twenty miles from my apartment. Visiting her became a small ritual. I would take the BART, cross the Richmond Bridge, and then a bus to her quiet home. The journey felt long, but it always ended with good food, warm conversation, and the comfort of being treated like family.
Our friendship did not end with Berkeley. Christine later worked with the California Department of Public Health and then the CDC. In 2011 she moved to Atlanta. In 2017 she came to India as a TB advisor with CDC, and life brought her back into our orbit in the loveliest way. She visited Sevagram three times. She did not arrive like a dignitary. She came like someone returning to her own people.
My granddaughter Diti took to her instantly. They spoke about books, exchanged reading recommendations, and treated each other like old friends. During Christine’s visit in May 2019, I noticed she was wearing a white and turquoise kurta. It was the same one Bhavana had gifted her in Berkeley in 2004. Years later, in January 2023, Christine visited again. As she left for Nagpur airport, she messaged me: “Hi SP… I just looked in the bag and saw that Bhavana gave me a beautiful dark blue silk shirt! It is really beautiful and she really should not have. I still remember the white and turquoise kurta she brought to Berkeley for me. Really so thoughtful.”
Some friendships do not fade. They simply travel.
***
Joseph Ezoua was the heart of our group. He came from Côte d’Ivoire, and he brought with him the warmth of West Africa. He would tell us about his country, the music, the rainforests, the beaches, and the kind of life that feels colourful even in memory.

Joseph also carried a burden we did not. His first language was French. His English was good enough for daily life, but Berkeley was not daily life. It was fast, technical, and unforgiving. He had to work twice as hard just to keep pace. He never complained. We helped him with language and phrasing, and he repaid us with laughter and morale. When Joseph was around, the room felt lighter.
When Bhavana visited me in December 2004, we had a small welcome party in my apartment. Joseph arrived with gifts from his country, including a beautiful frame that we still have. At one point, he turned serious, pointed to himself, and told Bhavana, “Bhavana, I am your big brother now. If anyone here hurts you, you come to me.”
He said it with a smile, but the feeling behind it was real. In a place far from her own brothers, Joseph offered her the protection of family.
Joseph eventually returned home and later worked with UNDP in Côte d’Ivoire. But to us, he remains the big brother who stood guard in Berkeley.
***
Maureen Morgan became my guide to American life. She was local to the Bay Area, and she understood things I was still trying to decode. She became my study buddy. Many evenings were spent at my place, going over assignments, making sense of readings, and trying not to panic.
Maureen also showed me the real Berkeley. She introduced me to the Farmers’ Market and the idea of organic food. I had grown up respecting farmers, but this was a different kind of admiration: for people who grew food while trying to protect the soil and the future.

When Bhavana came to Berkeley in December, it was Maureen who drove me to the San Francisco airport to pick her up. She did not just come as a driver. She came with roses and a box of homemade cakes. That was Maureen: practical, thoughtful, and quietly generous.
Driving in San Francisco frightened Bhavana and me. The roads climbed like walls. At every steep turn, we held the door handle as if it could save our lives. Maureen would laugh and drive on, as if gravity had signed a peace treaty with her.
When Bhavana left a month later, I was low. Maureen drove us to the airport again. After the goodbye, she did not drop me back to an empty room. She took me out for dinner, talked to me, and made sure I ate something. She knew what silence can do to a person.

Over the years, I watched Maureen’s journey with pride. She went from being an Emergency Room Technician to becoming a physician. She trained, specialised, and eventually became a gastroenterologist in Richmond, California.

Before I left Berkeley, we spoke about books. I mentioned I wanted to read The Tennis Partners by Abraham Verghese. On my last day, Maureen handed me a gift-wrapped package. It was the book. She had remembered. Inside was a card with words I still keep close: “Your name fits you exquisitely well, for you have a brilliant light shining from deep within… I can only imagine what a tremendous amount of courage it took to leave India… to come and study at UC Berkeley… I consider you part of my family, and I will miss you terribly.”
How do you not carry a line like that for life?
***
The most joyful part of our friendship was the exchange that happened over food. When Bhavana visited, she decided to cook for my Berkeley family. Our small apartment on Channing Way became a miniature banquet hall.

She made a proper Indian meal: curries, rice, and desserts like shrikhand and kheer. I still remember Joseph, Maureen, and Christine sitting in my studio, unsure at first what to do with so much food and so much spice. Then they followed our lead and began eating with their hands. They did not stop. They asked for seconds. They licked their fingers without shame. The next day, they told anyone who would listen that Bhavana was the best cook they had ever met.
Bhavana smiled when she heard that. I think she felt, for the first time in weeks, that Berkeley had become kinder.
***
Looking back, I realise the MPH degree was only half of what I gained that year. The other half was simpler, and perhaps more important.
Kindness travels. Friendship crosses borders. And if you keep your heart open, even a foreign city can begin to feel like home.
The California Family
If Christine, Maureen, and Joseph were my bridge to American life, my Indian circle became my anchor to home. Before leaving Sevagram, I had pictured Berkeley as a year of quiet weekends and lonely meals — Saturdays in the library, speaking more to books than to people.
I could not have been more wrong.
Once I settled in, I discovered what every Indian abroad eventually discovers: we are never truly alone. The Bay Area was full of familiar names, familiar accents, and familiar warmth. California stopped being a place of campuses and freeways. It became a map of living rooms, dining tables, and cups of tea that appeared before you could even ask. I called it our Desi GPS — an invisible navigation system that always knew where the next home-cooked meal was.
It began, naturally, with Madhu and Nikita Pai. They were not just the reason I was in Berkeley. They were my translators — helping me understand everything from bus routes to the American grading system, from what to buy at the supermarket to what to ignore entirely.
One Sunday morning, soon after I moved into Manville Apartment, Madhu called.
"Come for tea and breakfast," he said.
"I can't," I replied, sounding important. "I'm going to San Jose to meet Bhavana's cousin."
I pronounced it exactly as it looks: San-Joes.
Madhu paused. Then, very gently, he rescued me. "SP," he said, "here it's San Ho-say. The J becomes H. Spanish."
I felt foolish for a moment — a full professor who could not pronounce the name of the next city. But I was grateful. That small correction saved me from a great many future embarrassments.
Madhu and I also bonded over cricket, which in America is as rare as a decent cup of cutting chai. He knew where to find it. We would drive to an Indian cinema in Fremont and watch India play on a large screen, surrounded by hundreds of shouting expatriates, returning late, sleepy and satisfied, like boys who had stolen an extra hour of childhood.
On quieter Sundays, we played cricket in Madhu's backyard. After the match, Niki would feed us a breakfast that felt like a reward for simply showing up. For a few hours, Albany became Sevagram.
My most frequent refuge was the home of Raju and Uma Zamvar in Sunnyvale, about fifty miles from Berkeley. Their house was my weekend reset button — the place I went when the week had been long and the studio apartment had begun to feel small.

They had a black Honda Civic that became our little chariot across the Bay Area. Raju had just joined Visa. Uma was working as an internist at Kaiser Permanente Santa Clara. They were young, busy, building their lives in a new country — and yet they made space for us with the ease of people who understand, instinctively, what it means to be far from home.
We celebrated Diwali 2004 with them. Their son Rohan was a toddler then, wobbling around the house with that proud seriousness that toddlers carry. Uma was pregnant with their second child, Rishi, who would arrive in February 2005. Even with a demanding job and a growing belly, she hosted us as if it cost her nothing.
Our weekends found their rhythm. Raju would take us to Fry's Electronics — a vast store that felt like a museum of the future, aisle after aisle of gadgets and cables and things that had no name yet. We wandered through it, amazed that Silicon Valley seemed to run on small shiny objects.
And then came the real medicine: Indian food.
We would go to Chaat House on El Camino Real. After a week of sandwiches and salads, a plate of pani puri and pav bhaji tasted like homecoming — not metaphorically, but physically, in the chest. In January 2005, when Bhavana visited, we celebrated Rohan's birthday at Mayuri Restaurant in Santa Clara. There was a bird show for the children. It was loud, cheerful, and slightly chaotic — exactly the way birthdays should be.
Today, Raju is a senior professional at Visa and Uma is Chief of Medicine at Kaiser, leading a large team. But in my mind, they remain the young couple in the black Civic who made sure a lonely student did not stay lonely for long.
The circle kept expanding in the way that Indian networks do — each connection leading to another, each home opening a door to the next.
Bhavana's aunt, Nilu Masiji, lived in Palo Alto. Visiting her gave us a glimpse of an older Indian community, settled and steady, that had made California genuinely its own. We went trekking in the Palo Alto hills and were surprised, as one always is, by how green California could be.

In Fremont, Rahul Asawe and his wife Heena fed us as if we had been away for years rather than weeks. And then there was Sanket Khemuka — a Wardha connection, vivid and unexpected in the middle of Silicon Valley. Seeing a Wardha boy working in Sunnyvale, confident and settled, filled me with a quiet pride. Wardha, it turned out, had travelled farther than any of us had imagined.

When graduation day arrived in May 2005, Raju and Uma drove all the way from Sunnyvale to Berkeley to be there. Later, they came to the apartment for lunch with my friends. It was a simple meal. It felt like a celebration with family.
During Bhavana's December visit, we took a trip to Los Angeles. It was not sightseeing — or not primarily. It was a tour of people.
We met Subhash Mantri, Deodas Rathi, and Chandrakala Rathi. We stayed with Shilpa Fattepuria, the daughter of our family friend from Wardha, Ramesh Fattepuria. Sitting in her living room in California, talking about Wardha names and Wardha stories, the distance between the Bay Area and Vidarbha shrank to nothing. That is the peculiar alchemy of the Indian diaspora — you travel ten thousand kilometres and find yourself talking about the same street corner you left behind.
Before flying home in May 2005, I made one final stop — a flight from Oakland to Denver, to visit Ravi Kachaliya and his wife Shyamala.
Ravi came from a Wardha family that everyone knew. His father Bhupatbhai had run Panchsheel Store, a cloth shop that had dressed half the town for decades. Ravi had built a life in America, earned two Master's degrees, and established himself in finance. He lived in a large home in Denver, but he carried Wardha inside him the way we all do — in his references, his humour, and the particular ease he had with people from home.
For four days, Shyamala fed me Gujarati food that tasted as if it had made the journey directly from our kitchens: dhokla, thepla, undhiyu. Ravi and I were both night owls. We sat up late, watching India versus Pakistan on his large television, cheering and complaining like seasoned selectors. We talked about books — swapping authors, arguing gently over sentences. Those nights were the perfect winding down. After months of deadlines and lectures, Denver felt like a long, unhurried exhale.
And then I found, recently, a letter I had written to Bhavana from Denver — dated 20 March 2005. Gmail had been born barely a year before, and I was still discovering that letters could travel instantly. Reading it now, twenty years later, I find it captures those days more precisely than memory alone can manage.
In fact, I had written to her the day before as well — on 19 March, the evening I arrived in Denver. That letter, too, survived in my inbox.
Denver, 20 March 2005
Hi Bhavana,
I am writing this mail from Denver, where I landed last night. Berkeley was a bit cold and wet all Friday. I took BART from Berkeley to Oakland airport and got into a bus that took 15 minutes to take me to the airport. I already had a boarding pass, so all I had to do was check my luggage and wait for an hour at the gate. Later I found that my bag had been opened officially by the airport authorities as part of a routine random check. It is always better not to lock the bags — if the authorities have to break the locks, they can damage the zip. Two and a half hours later, I found myself at Denver airport.
Ravi had already hinted — and I am glad that he did — that Denver is a really huge airport. Much bigger than San Francisco. And certainly more beautiful. I came five floors down, took a train, collected my luggage, went one floor down, and then waited about 15 minutes for Ravi and his wife to arrive. A 25-minute drive took us to their home at about 9:30 pm — Denver is one hour ahead of Berkeley time. Their home is really beautiful. I am taking a few snaps of their artfully decorated rooms. What caught my eye was the open-plan concept — drawing room, living area, kitchen, and dining room all flowing into one, with the master bedroom overlooking the drawing room. Like California homes, all homes in Denver are made of wood, which makes them easy to remodel every few years. You do not have to live in the same old house year after year.
I had a lovely Indian-style lunch, which I ate to my heart's content. And then a surprise was waiting for me. Ravi has a large, wall-mounted television, which was showing the India-Pakistan match live. And like me, this couple is also cricket-mad. We ended up enjoying Rahul Dravid's century and watching Dinesh Karthik narrowly miss his, until almost 2:00 am. The post-tea session of the match was recorded on video so that we could watch it the next day. Then I retired for a well-deserved sleep.
I am sure the next three days are going to be exciting. Both Ravi and Shyamala work from home and seem to be doing very well. They told me stories of how their parents visited last year and, much against their original plan, ended up staying for a couple of months. And now Bhupatbhai has liked the US so much — particularly its work ethic and professional honesty — that he is planning to visit again.
I will keep you posted on the day's developments in the evening. I do hope everything is fine in Sevagram. Have a nice time.
With all my love, SP
Dear Bhavana, my love,
March 20th — my second day in Denver. We stayed up late the day before — till 1:45 am. The India-Pakistan cricket match, shown live on cable, was too tempting to go to sleep for. I woke up early the next morning, though. I did write you a mail, but because I could not access the net, the mail is still sitting in the draft section of my Outlook. The Sevagram map that you sent me looks indeed very nice. I also received a mail from Rahul Narang and replied to him yesterday.
In the afternoon, Ravi drove us for about two hours to a small town called Georgetown. These small towns around Denver have their own innate 18th-century charm, with most of them built in the old French style, and even today they have carefully retained that same old touch. I saw snow there, capping the mountain tips, dressing the green trees, and clothing the houses.
Next we drove for about 45 minutes to reach another small town called Vail. This town showcases the spectacularly beautiful Rocky Mountains that stretch from coast to coast. Eyes refuse to believe that nature could be so picturesquely pure and spectacularly serene. No wonder that this town houses some of the most expensive homes in the USA: celebrities have invested close to 100 crore rupees to acquire small one- or two-bedroom apartments, to get away from the maddening, crowded cities and their hustle and bustle. These homes take you straight to the Rocky Mountains — clothed in pristine white snow — and bring a much-needed solace and stillness to the average ambition-driven American. Even Europeans come here in winter to spend their vacations.
We then strolled through the town. Ravi took me to several shops that sell antique showpieces and watches to connoisseurs. Some watches, exquisitely beautiful, cost 20 lakh rupees. And the shop owner was generous enough — as most Americans are — to allow us to try these watches on our wrists. For a few seconds, our wrists were the proud owners of the most expensive Swiss watches in the world! Collectors interested in unique cut-glass pieces also frequent an adjoining shop that showcases sculptures and pieces whose prices range from 10 to 50 lakhs.
The stomachs were hungry by now and badly needed food. A Chinese restaurant looked a bit shady, and we chose to eat pizza at an Italian restaurant instead. After a wait of about 50 minutes in a queue, a waitress ushered us into a busy — and noisy — dining hall whose walls were painted black and red. The pizza tasted really good, more so because our palates were quite hungry. It was 11:30 at night when we came back. And then curiosity got the better of us again. Ravi and I watched the final session of the India-Pakistan match until our eyes literally dropped and we found it extremely difficult to stay awake.
Today an Indian couple has invited us for lunch. We will go there and then probably to a famous Hindu temple here.
I spoke to Bhupat bhai yesterday night. He was very happy to know that I was with Ravi. He had already called him, asking that he make my stay as comfortable as possible. He also said that it was my home and I should stay as long as I wanted. He again instructed Ravi to take special care of me. He regretted that he had visited the US too late in his life, and that had he come here about ten years earlier, he would have settled down in the US. He was deeply impressed with their work ethic and professionalism, and also with the dignity of human labour and the equality of people.
That is it. I will write to you again.
With all my love, SP
***
On the flight back to India, I understood something simple that I had not known how to articulate before.
I had gone to America to study public health. I learned epidemiology and statistics, of course — and I am grateful for both. But the deeper education was quieter. Home, I learned, is not a building. Home is people.
It was Madhu saving me from saying San-Joes for the rest of my year. It was Uma making tea even when she was tired. It was Raju driving us around the Bay Area as if we had always belonged there. It was Ravi watching cricket with me at midnight in Denver, talking about Wardha as if we had never left.
They took a foreign country and wrapped it in familiarity.
And because of them, even when I was far from India, I never once felt far from home.
The Golden Gown
The climax of any Master’s program is the thesis. For me, it was more than an academic requirement. It was the moment the rubber met the road. After months of theory, I had to apply it.
I worked with Madhu Pai, Lee Riley, and Art Reingold on a systematic review and meta-analysis. We chose a topic that mattered deeply to India: how accurate bacteriophage tests were in diagnosing tuberculosis.
As a clinician, I was used to things I could see and touch, a patient’s breathlessness, a murmur, a swollen ankle. Research felt different. It lived on paper, inside tables, behind confidence intervals. Madhu taught me that good research is not magic. It is discipline. He pushed me through the hard work of data extraction. We read hundreds of papers, separated the good from the sloppy, and entered numbers into large sheets, one study at a time. Every digit was checked and rechecked.
He introduced me to Stata and EndNote. To me, they felt like a new set of instruments. But more than the software, I learned something that stayed with me: respect for data. You don’t twist numbers to say what you want. You listen carefully, even when the answer is inconvenient.
Even today, I still have those old yellow data sheets. They remind me of the year I stopped being only a reader of medical literature and became, in a small way, a creator of it.
The work paid off. I defended my thesis before Art Reingold and Allan Smith. And before I had even packed my bags, our paper was accepted: Bacteriophage-based tests for the detection of Mycobacterium tuberculosis in clinical specimens. For me, it felt like a certificate with weight.
***
Paul Farmer and the $30 Gown
On May 17, 2005, the sun shone brightly over the Berkeley campus. Graduation day. We rented golden gowns for thirty dollars.
When I pulled the heavy cloth over my shoulders and adjusted the cap, I felt a surge of emotion I had not expected. I was in my mid-forties, a professor back home, yet standing in a line of twenty-somethings, I felt a boyish pride. That gown was not just ceremony. It was proof. I had stepped out of my comfort zone, survived a demanding year, and earned a new identity: student again.
The School of Public Health had invited Dr. Paul Farmer to give the commencement address. Farmer was already a legend. He had worked among the poorest in Haiti, Rwanda, and Peru. He did not only treat disease. He fought the injustice that produced it.
He spoke without drama, but every sentence landed. One line stayed with me: “Passion and indignation have a place in public health.” In a world of numbers and models, he reminded us that behind every statistic there is a human life.
Paul Farmer died suddenly in February 2022. But on that day in 2005, he made us feel that public health could be both science and conscience.
***
The Lunch Disaster
After the ceremony, I hosted lunch at my apartment. Bhavana had returned to India by then, so I was on my own. I ordered vegetarian Indian food from Vick’s Chaat.

My calculations were based on Indian habits. I assumed people would eat politely. I was wrong.
The moment the boxes opened, the smell of samosas and curry filled the room. My guests included professors, classmates, and friends who had become family. And the Americans, it turned out, loved Indian food with a seriousness I had not predicted. Within minutes, the trays were scraped clean. People were still looking for seconds. I stood there, embarrassed, amused, and oddly happy.
It was a classic desi planning error. But it became a memory I still smile at.
***
The Visa Cliffhanger
A week before my flight back, I discovered something that made my stomach drop. I needed a transit visa for London Heathrow.
By then I had vacated my apartment. I had sold my furniture. I was living out of a suitcase. The British Consulate required me to send my passport to Los Angeles by post. They promised a five-day turnaround. I had six days.
I mailed it and spent the next week checking the mailbox like a man waiting for a lab report that could change his life. Without the passport, I was stuck. Homeless in Berkeley, unable to fly, trapped in paperwork.
On the sixth day, less than twenty-four hours before my flight, a courier envelope arrived. I tore it open. The passport was inside, visa stamped.
Only then did I breathe properly.
***
The Farewell Letter
In the last quiet days, sitting in my empty apartment, I felt I could not leave without saying goodbye. I wrote an email to my friends and colleagues.
Dear Friends,
It was the best of times; it was not the worst of times. I'm about to finish my time in Berkeley soon! A year at Berkeley—educating, entertaining, exciting, and at times exasperating—would come to an end!
When I arrived in Berkeley last fall, I was in my mid-forties and struggling with mid-career blues. I knew I had some gaps in my knowledge... So, I decided to come to Berkeley to learn more. But, I'm usually a shy and introverted person... The idea of being in a foreign land and living on my own for a year without knowing how to cook was a bit overwhelming.
Despite the initial challenges, I managed to adapt and thrive... I learned how to become self-sufficient and even managed to make perfectly round rotis - a significant accomplishment for me! What did I learn in Berkeley? I learned the fundamentals of statistics, epidemiology, and evidence-based medicine... But most importantly, I learned that to find answers, one must ask the right questions.
I won't fall into the familiar trap of comparing the US with India. Berkeley has filled my heart with a sense of achievement and fulfillment. I loved Berkeley, and my eyes may tear up when I say goodbye.
***
The Return to Reality
The flight back was long, across time zones and moods.
Somewhere over the Atlantic, I read an email from my friend Dr. MVR Reddy in Sevagram. It pulled me back to earth. He wrote about the usual chaos: inspections, entrance exams, confusion over admissions. He even wrote about Amrita’s future schooling and said, gently, that after what I had seen in America, I might have a different perspective.
He was right.
I was returning to the same Sevagram, with its heat, its constraints, and its daily pressures. But I was not returning as the same man. I was coming back with tools: Stata for my data, epidemiology for my questions, and Paul Farmer’s words sitting quietly in my conscience.
The Berkeley year had ended.
The mid-career blues had not just lifted. They had disappeared.
I was ready to go home.
My Berkeley Days

I landed in San Francisco with two suitcases and a mind full of apprehension. I was in my forties, uprooting myself from the familiar soil of Sevagram to become a student again.
My soft landing in this new world was arranged by Madhu.
Madhu was not just a host. He was my friend, philosopher, and guide. He picked me up from the airport and, for the first ten days, opened his home to me. He drove me through the hilly streets of Berkeley, taught me the small survival codes of California, and fed me warm meals when I was too disoriented to even think of cooking.
One night he drove me to Fremont for an experience I had not expected in America. A local cinema was screening an India–Pakistan one-day match. We sat in the dark from 10 at night to 5 in the morning, surrounded by a loud, excited diaspora crowd. When Sachin Tendulkar got out, the hall erupted in celebration. I looked at Madhu, startled. Only then did I realise that half the audience was Pakistani. In that dark theatre in Fremont, thousands of miles from the subcontinent, the rivalry was alive and noisy, and strangely comforting.
***
It sounds unbelievable now, but I spent my entire Berkeley year without a mobile phone.
I lived like an analog man in a world that was turning digital by the month. My only lifeline to India was a landline provided by the program. Every Sunday, without fail, I called home.
Bhavana was on the other end. While I was learning statistics and epidemiology, she was fighting battles on multiple fronts. She managed the house, her job, and the chaos of the hospital’s newly launched Information System, which was going through painful teething troubles. And she was carrying the biggest worry of all, Ashwini’s admission. She ran from pillar to post collecting documents, filing affidavits, and arranging fees. At one point she even had to liquidate our mutual funds. I listened from thousands of miles away, helpless, and full of gratitude.
And yet, while I did not have a phone, I watched a digital revolution unfold in front of my eyes.

When I arrived in Berkeley, my email was still Rediffmail, the faithful companion of many Indian academics of that era. Then Google announced Gmail. It offered a full 1 GB of storage. Most of us thought it was a joke. Rediff and Hotmail gave you a few megabytes, barely enough for a couple of attachments.
It was not a joke. By early 2005, I had switched. I like to say I went to Berkeley as a Rediff man and returned to Sevagram as a Gmail user. It sounds small now, but it marked a turning point. The world was changing, quietly but decisively.
***
My days in Berkeley soon fell into a quiet rhythm. I did not own a car, which in California felt like a mild disability. But Berkeley was kind to walkers. I managed with public transport and my own feet, and I began to enjoy the anonymity of it.
Warren Hall became my work-home. I had a designated table and a computer in the program office. I spent long hours there working on my MPH thesis, a systematic review of a diagnostic test for tuberculosis. The work was slow and demanding, but it later got published, which made those hours feel worthwhile.
When I wasn’t in Warren Hall, I was often at the Berkeley Public Library. I still remember the day I asked the librarian, a little timidly, “How many books am I allowed to borrow at one time?”
She laughed, a big American laugh. “The entire library, if you can carry it!”
That one line captured Berkeley. It was a place of open doors and generous rules. Most people were warm and large-hearted. Once in a while, I met a teacher or two who made me feel small, as if I did not fully belong. The condescension was subtle, but it stung. Thankfully, those moments were rare. The larger experience was welcoming.
***
Berkeley was an intellectual crossroads. I sat in lecture halls listening to giants like Amartya Sen, who had recently won the Nobel Prize, speak with dazzling clarity.
But the students were no less impressive. I met an American PhD scholar who was writing his thesis on the last year of Bhagat Singh’s life. He had travelled through India, Pakistan, and Nepal. He had learnt Hindi, Urdu, and Punjabi. He had spent years digging out details about an Indian revolutionary that even I did not know. It was humbling. It reminded me what real scholarship looks like when it is done with patience and respect.
***
The best part of that year came between the two semesters, when Bhavana visited for a month.
Her arrival showed me the depth of the friendships I had made. Maureen insisted on coming with me to the airport. When we reached my small studio apartment on Channing Way, we found that she had quietly left behind a bunch of fresh roses, dry fruits, and a handwritten welcome note. It was such a simple gesture, and yet it moved us both.
Bhavana’s presence changed everything. My lonely student meals turned into proper food again. We invited my Berkeley friends, Christine, Maureen, and Joseph, for dinner. In that small studio, with limited utensils and even less space, Bhavana cooked a full Indian vegetarian feast. The three of them were so delighted that the news travelled fast through the department: SP’s wife makes vegetarian dishes that nobody can match.

We also spent time with my teachers, Art, Jack, and Lee. Lee is no longer with us now, but the memory remains warm. Bhavana and I travelled down the coast to Los Angeles and San Diego to visit her relatives.
For that one month, the loneliness of being a long-distance student disappeared. The Sunday phone calls were replaced by shared meals, shared walks, and shared sunsets over the Pacific. For a brief while, my two worlds, Sevagram and Berkeley, sat together in the same room.
Goodbye, Berkeley. I Love You.
Some letters are written to inform. This one was written to feel — to hold, for a moment longer, something that was already slipping away. In the spring of 2005, with two weeks left before my flight back to India, I sat down and wrote to everyone I knew: family, colleagues, friends, people who had watched me leave and were waiting for me to return. I did not know, at the time, that I was writing a piece of memoir. I thought I was simply saying goodbye to a city. But letters have a way of becoming more than their occasion. Reading it now, nearly two decades later, I find in it a man I recognise but can no longer fully inhabit — uncertain, grateful, quietly astonished that he had survived a year of solitude and emerged, somehow, more himself. I offer it here unchanged, exactly as it was written: unpolished, unhurried, and still, I think, true
It was the best of times; it was—fortunately—not the worst of times. But now, my Berkeley season is drawing to a close. On May 24, I will touch the soil of Sevagram once again. A year that was educating, entertaining, exciting, and at times exasperating, has come full circle.
Last fall, when I arrived at the University of California, Berkeley—a vibrant town barely twenty miles from San Francisco—I was a man in his mid-forties grappling with the restlessness of the middle years. I had come conscious of the vast gaps in my knowledge. Statistics, epidemiology, and evidence-based medicine were languages I struggled to speak. I had tapped the portals of Berkeley hoping to fill those voids.
Berkeley accepted me with open arms.
By nature, I am shy, inhibited, and often tongue-tied around strangers. Moreover, I had never lived away from my family for so long. The fear of a foreign land, and the daunting prospect of surviving independently without even the most basic cooking skills, weighed heavily on my mind.
But survive, I did.
I found Berkeley to be warm, compassionate, and deeply tolerant—a place that celebrated diversity rather than just tolerating it. It is a small town where, of the 102,000 residents, nearly half are students. Slowly, I began to decipher the American accent, just as they began to absorb my Indian cadence. I learned their culture, and they went out of their way to understand what rural India meant. I grew comfortable with the informality of first-name relationships. Within days, the senior doctor from Sevagram had transformed into a student walking the campus with a backpack and a lunchbox.
Berkeley took me back to my undergraduate days. I returned to classrooms, home assignments, unit tests, and midterms. I spent nights preparing for seminars, writing a thesis, and dreading the finals. All my life I had been math-challenged—perhaps the sole reason I became a doctor—and initially, I struggled to figure out exponentials, logs, and coefficients. I will never forget the professors and friends who helped me navigate those complexities. I acquired outstanding friends as I travelled hopefully, and I value their camaraderie in more ways than one.
My teething troubles over, I began to settle. The days rolled by, and eventually, so did the dough—I finally learned to roll a perfect round roti, perhaps my greatest achievement of the year! I learned how to thrive without asking for help, embracing the fierce independence that Americans cherish.
I learned how to count, how to measure, and how to associate A with B. I discovered the rows and columns that make a table, and the bars, pies, dots, and lines that breathe life into a graph. I learned to read, write, analyze, and interpret. I realized with some shame that three-quarters of the medical articles I used to read in Sevagram had never truly made sense to me. Berkeley decoded the anatomy of a research paper and showed me what it takes to publish in JAMA. It taught me that medical research is serious science, and that India needs it—perhaps even more than the developed world—to solve its own unique problems. Indeed, I learned that to find the right solution, one must first learn to ask the right question.
I won't fall into the familiar trap of comparing the US with India. Berkeley has simply filled my heart with a sense of fulfillment. It opened a massive canvas for me, and my amazement at discovering its colorful kaleidoscope never ceased. I loved Berkeley, and my eyes might well tear up when I say goodbye.
And yet, as spring replaces the fall, a gentle homesickness is enveloping me. I miss Sevagram. My dreams these past few days have been woven around my family, friends, colleagues, and patients. The countdown has begun—I am excited to return home in exactly two weeks.
Words fail me when I try to thank those who coaxed, cajoled, and literally pushed me into accepting this fellowship. I value their support more than I can say. I won't name them, for I can never repay the debt I owe them. I remain ever conscious of the love and affection that my friends and the MGIMS family have showered upon me.
So, it is time to turn from San Francisco back to Sevagram.
Berkeley Comes to Sevagram
When I wrote my Statement of Purpose for the MPH program in 2003, I made a bold promise: I would return to India and help build a culture of inquiry. In January 2006, less than eight months after I graduated, that promise came home in the most unexpected way. Three of my teachers from the UC Berkeley School of Public Health, Art Reingold, Jack Colford, and Lee Riley, travelled nearly 8,000 miles to Sevagram to conduct a workshop on Applied Infectious Disease Epidemiology.
For a medical college in rural Maharashtra, hosting even one international expert is an event. Hosting three, at the same time, felt almost unreal. Madhu Pai, my mentor and friend, had quietly worked behind the scenes to make it happen. Their visit was more than a workshop. It was a signal, to us and to the campus, that what we were trying to build at MGIMS mattered.
***
The Maruti chariot
Art Reingold’s arrival is still one of my favourite memories. I had decided to pick him up not from an airport, but from Aarti Talkies on the Nagpur road, a familiar meeting point for travellers arriving by taxi. I reached there in my second-hand Maruti 800, a small rattling tin box that looked nothing like the cars in California.
When Art stepped out, I felt a brief, foolish self-consciousness. Here was the Head of Epidemiology at Berkeley, a man who advised the CDC and the WHO, and I was offering him the front seat of my Maruti.
Art didn’t blink. He smiled, put his bag inside, and climbed in as if this was the most natural thing in the world.
He had always been an Indophile. In Berkeley, he once surprised all of us by cooking Indian food from a Tarla Dalal recipe book, measuring spices with the seriousness of a lab experiment. As we drove towards Sevagram, bumping over Vidarbha’s uneven roads, he looked out of the window with curiosity and affection, not judgement. He seemed less like a visiting professor and more like an old friend returning.
***
Traffic, stray dogs, and Jack
Jack Colford’s relationship with India began differently. For him, this was his first encounter with our glorious sensory overload.
One evening, after the day’s lectures, Art and I decided to walk Jack back to our home. The route took us down the hospital slope and into Sevagram Square. In 2006, the square was a theatre of chaos. There were no traffic lights, no lanes, and no visible rules. Vehicles flowed like water, except water does not honk.
As we walked, India introduced itself properly. A pack of stray dogs erupted into loud barking. A motorcyclist cut past us, missing my elbow by inches. An auto-rickshaw appeared from the wrong side, swerved, and disappeared again. A pedestrian slipped on loose gravel and recovered without complaint.
Jack looked genuinely shaken. His eyes kept searching for a crosswalk, a walk signal, anything that promised order. Nothing did.
Art watched him for a moment and chuckled. Then he put a hand on Jack’s shoulder and said, “Jack, this isn’t San Francisco. You have to flow with it.”
It was a perfect Berkeley moment transplanted into Sevagram. Art, the seasoned traveller, was calm and amused. Jack, the brilliant methodologist, looked as if he was trying to calculate the probability of survival at a road crossing.
I knew he would adjust. India overwhelms you first. Then, slowly, it wins you over.
***
The workshop of giants
The workshop itself was a treat. For four days, the classroom buzzed with serious, joyful learning. We had about thirty participants, and the quality was as remarkable as the faculty.
Dr Saranya Sridhar, an MGIMS alumnus from the 1997 batch and a Rhodes Scholar, flew in from London, where he was pursuing his PhD, just to attend. Dr Anurag Bhargava, a dear friend from Jan Swasthya Sahyog in Ganiari, joined us too, bringing with him the sharpness of rural practice and the impatience of someone who wants ideas to matter on the ground.
Art, Jack, and Lee covered the full sweep of modern epidemiology. There was the detective work of outbreak investigations, the discipline of trial design, the logic of randomised controlled trials, and the newer language of molecular epidemiology. They taught with energy, but also with humility. They didn’t speak down to anyone. They listened. They asked questions. They used examples that made sense in Sevagram, not only in textbooks.
I sat in the back of the room and watched my Berkeley professors teach in my own backyard. It felt like two parts of my life had finally shaken hands.
***
Culinary diplomacy
But the best part of the visit did not happen in the lecture hall. It happened at our dining table.
We were living then in a rented flat in Vivekanand Colony, close to the Dean’s office. I invited Art, Jack, Lee, and Saranya for dinner. Bhavana had been preparing all day. The house smelled of ghee, roasted cumin, and cardamom, the kind of smell that makes you feel safe even before you sit down.
She began with soup. Jack, still recovering from Sevagram traffic, took a cautious sip. Then his face changed.
“Wow,” he said. “This is amazing.”
For the main course, Bhavana laid out a full vegetarian feast: basmati rice, hot parathas, curries, and dry vegetables cooked the way we like them. For dessert, she served gulab jamun and ras malai.
Art and Lee had eaten Indian food in the US. They were still stunned.
“We’ve had Indian food,” Art said, wiping his plate clean, “but nothing like this.”
That evening, the labels fell away. There was no professor and student. No visiting faculty and host. We were just friends talking, laughing, eating slowly, and staying longer than planned.
***
The aftermath
After they left, I wrote to Madhu.
“Dear Madhu, the workshop really went well… I gave the Berkeley faculty a tour of the institute… Art spent three hours with us cutting jokes… But for you, I would not have been able to get the Berkeley faculty to Sevagram. I am conscious of your support all these years… Needless to say, of all people, I really missed you!”
A little later, I received a letter from Jack. He wrote generously about our first meeting at Art’s party and about my participation in his course. His words were kind, but they also carried a quiet message: I was no longer only a learner sitting in the back row.
By bringing Berkeley to Sevagram, I had become a bridge.
The hospital’s digital revolution was still ahead. But that week, I felt the intellectual revolution had already arrived.
The 3 A.M. Train
n the mid-1980s, India began a cautious, suspicious courtship with a machine it had long mistrusted. Until then, computers belonged to a distant, air-conditioned world of big cities and men who spoke in a cryptic language of acronyms. In small towns like Wardha, the word "computer" still carried a faint, technophobic chill; it was viewed as a clever toy destined for obsolescence, or worse, a threat designed to replace human labor.
Then, the Indian Railways introduced the computerized reservation system, and the national mood shifted. If you had lived through the old era, you understood that booking a ticket was not a transaction but a bureaucratic ordeal—a test of stamina involving serpentine queues and the thud of a clerk’s stamp that sounded like a judge’s gavel. When the glowing screens arrived, the sweat and the queues remained, but they were joined by a new kind of certainty. The machine did not argue; it simply worked. Slowly, the public stopped seeing computers as threats and began to see them as tools. Bhavana was among the first in our circle to notice this shift, and she viewed it with a seriousness that caught me off guard.
***
In Wardha, technology still meant a sturdy typewriter and the reliability of a carbon copy. If a file vanished, you didn't query a database; you interrogated human memory. Yet, Bhavana was drawn to this new digital world with a focus that was neither a passing whim nor a hobby. She wanted skills—the kind that would allow her to sit before a screen and make things happen.
The problem was geographical: Wardha offered no place to learn. NIIT in Nagpur was the only reputable name, but it required a staggering eighteen-month commitment and a fee that was significant for a middle-class family. We weren't wealthy, but we did what families of our station do when they believe in a door worth opening: we adjusted our expectations and dug deep. The only workable schedule for a mother of two small children was a 7 a.m. class in Nagpur. It was a logistical nightmare that turned our home into a place that ran on a timetable set while the rest of the town was in deep sleep.
***
For a year and a half, the 3 a.m. alarm became the silent conductor of our lives. Bhavana would rise in the stillness of the house—the ceiling fan turning lazily, the children breathing in rhythm—and the kitchen would flicker to life before the first hint of dawn. There was no romance in this routine; it was not heroic, it was simply necessary.
By 3:30 a.m., we would step into the biting air for the seven-kilometre ride to Sevagram station, then known as Wardha (East). The scooter’s headlight cut a narrow tunnel through a deserted landscape where the only other inhabitants were startled stray dogs. I would drop her at the dimly lit platform—a lone figure moving toward a train that promised a different life. At 4:00 a.m., she boarded the Dadar–Nagpur Express, often the only passenger in the compartment, traveling through a landscape that was steady and indifferent.
The part that concerned me most was the arrival at Ajni station before dawn. In those years, the walk through Dhantoli or Ramdaspeth was not a casual stroll for a woman alone. Bhavana dealt with the risk the way a programmer deals with a bug: she planned around it. She waited at the station for an hour, watching the city wake, and only when the light became steady did she walk to her class for two hours of logic, flowcharts, and practice code.
***
The return trip was a mirror of the morning: the 11 a.m. Maharashtra Express, a shared auto-rickshaw, and a return to Sevagram by 1 p.m. There was no pause for recovery. She slipped immediately back into the roles of mother and homemaker—roles that do not halt simply because one has spent the morning mastering COBOL or C++.
She endured the summer heat that turned train compartments into furnaces and the monsoons that soaked her to the bone. She seldom missed a class. It wasn't stubbornness for its own sake, but a quiet, steady belief that if she allowed the routine to slip even once, the entire future she was building would collapse. Our neighbors watched this with a mix of admiration and disbelief, as if she were fulfilling a strange personal vow. They recognized that such commitment is expensive; it costs sleep, it costs ease, and it costs the luxury of being ordinary.
Years later, when people ask how we managed to build complex digital systems in a rural hospital like MGIMS, they assume it began with government grants or high-level policy meetings. They are wrong. It began with a woman waking at 3 a.m., making sure her children were tucked in, and riding through the dark toward a railway platform. The first chapter of our technology story was not written in code; it was written in the relentless, unglamorous language of routine.
FoxPro on a Blue Screen
In March 1995, I went to Dhirubhai Mehta with a request that mattered to our family more than it may have sounded on paper.
Bhavana had finished her training. She had learned FoxPro—an old database language now, but powerful then. She had done the hard part. Now she needed a place to use it. Learning a skill is one thing; finding a space to practise it is another. In a town like ours, the second part is often harder.
Dhirubhai listened, and he did what he often did when he saw sincerity: he helped without drama. He spoke to Dr. Sushila Nayar, who agreed to appoint Bhavana in the hospital. There were no grand speeches about women empowerment, no declarations. It was simply a practical decision made by people who could recognize ability.
In April 1995, Bhavana joined MGIMS hospital as a junior clerk.
Our children, Ashwini and Amrita, were nine and six.
Her “office” was not impressive. It was a small room near the registration OPD, close to the daily noise of patients, relatives, clerks, and confusion. Anyone who has spent time near an OPD registration counter knows the particular kind of chaos it produces—questions flying, tempers fraying, papers being pushed, someone always trying to jump the queue.
But for Bhavana, that room held something rare.
A computer.
***
In those days, discharge summaries were often handwritten scrawls. Some were detailed, some careless. Many were barely readable. For doctors, the discharge summary is a routine document, something you finish quickly at the end of an admission. For patients, that one sheet of paper is the story of their illness, the only evidence of what happened to them inside the hospital walls.
When handwriting is unclear, the patient suffers. The next doctor suffers. Even the same hospital suffers when the patient returns months later and nobody can decipher what was written earlier.
Bhavana began by computerising discharge summaries for the Medicine department. It was a small change, but it had a visible effect. Typed text looks honest. It looks accountable. It forces you to think in complete sentences. It also reduces the temptation to write vague phrases that mean everything and nothing.
Faculty members would dictate. Bhavana would type. A structured summary would emerge—clearer, cleaner, and easier to follow. People noticed. Not because it was glamorous, but because it was useful.
The hospital, like any institution, is full of people who don’t resist change itself. They resist inconvenience. When something saves time, reduces errors, and prevents embarrassment, it begins to earn its place quietly.
***
After discharge summaries came the medical store. Inventory in hospitals has its own kind of confusion: missing stock, delayed supplies, expired medicines, manual registers that nobody trusts fully. In a paper system, the truth is always slightly negotiable. A number can be adjusted. A page can go missing. A shortage can be blamed on someone else.
Bhavana wrote small programs that brought some order to this. She did not “transform” the store overnight. She did not eliminate problems with a magical piece of software. But she introduced something important: a record that did not depend entirely on memory and handwriting.
She also developed software for Kasturba Vidya Mandir. That might seem like a side project, but it reflected her nature. Once she learned a tool, she wanted to apply it wherever it could reduce friction and confusion.
By October 1996, she was promoted to Computer Operator.
It wasn’t a dramatic rise. There were no ceremonies. But in a hospital that still ran on paper and carbon copies, Bhavana had become something uncommon: a person who could translate work into code.
***
FoxPro had a particular look that people of that era will remember: a blue screen, a blinking cursor, and the feeling that you were speaking to a machine in a language only a few understood. Bhavana’s screen became a small window into a different way of working.
It also changed the way people looked at her. A junior clerk is invisible in most institutions. A computer operator, even in a small room near OPD, begins to attract attention. People come to you with problems, not because they respect your designation, but because you can fix something they cannot.
And Bhavana fixed things patiently.
Not just the programs. She fixed small human anxieties too—the fear of touching the keyboard, the hesitation of pressing the wrong key, the embarrassment of not knowing what “Enter” meant. In a hospital, technology is never just technology. It is also psychology.
***
In retrospect, those FoxPro years did more than computerise a few tasks.
They trained Bhavana in something that would later decide the fate of the Hospital Information System. Not programming. Patience.
Because hospitals don’t change when you give them software. Hospitals change when people trust the person who brings it.
Bhavana learned how to listen to complaints without becoming defensive. She learned how to teach without humiliating. She learned how to persuade without preaching. She learned that the smallest staff member at the counter often understands workflow better than the senior faculty member who only signs the file.
Those were not “IT skills.” They were human skills.
And they would matter far more when the hospital tried to digitise not one room, but its entire bloodstream.
The Lucknow Epiphany
In 1999, I travelled to Lucknow to see the Hospital Information System at SGPGI — designed by C-DAC.
I went as a curious doctor and returned as a restless one.
SGPGI was not just bigger than MGIMS. It operated with a different rhythm. It felt as if the hospital had a spine, an internal structure that held information in place. In Sevagram, we were used to files that moved like wandering cattle—sometimes present, sometimes missing, often found only after a long search and a few raised voices.
In Lucknow, information sat quietly where it belonged.
A doctor could pull up patient history on a screen without calling for a file. Lab reports appeared without someone running across the campus with bundles of paper. The system reduced the shouting, the searching, and the daily small humiliations that a paper-based hospital forces on both staff and patients.
I watched doctors order investigations, view results, and retrieve records with a calm efficiency that felt almost luxurious. It wasn’t luxury, of course. It was simply good design.
For someone used to Sevagram’s daily struggles, it looked like tomorrow had arrived early in Lucknow.
***
I came back with a question that refused to leave me. If Lucknow can do it, why not Sevagram?
It wasn’t a question of pride. I wasn’t trying to prove that we could match a big institute. The question came from something simpler: fairness. Our patients were poor, but that did not mean they deserved a chaotic system. In fact, it meant they deserved a system that wasted less of their time and money.
We had patients. We had volume. We had work ethic. We had clinical seriousness. What we lacked was infrastructure, expertise, and money. And perhaps the courage to attempt something that sounded too ambitious for a rural teaching hospital.
In a place like Sevagram, ambition is often treated as arrogance. People tolerate big dreams only if they come with guaranteed success, and no dream comes with that guarantee.
Still, the question remained.
***
Big projects don’t survive on enthusiasm alone. They survive on backing—especially when things go wrong.
In Sevagram, two men mattered deeply to this story: Mr. S.R. Halbe and Mr. Dhirubhai Mehta.
Halbe arrived in the mid-1990s and quickly became a presence you couldn’t ignore. Tall, broad, and blunt, he had the air of a man who had seen too much inefficiency to tolerate it quietly. A chartered accountant by training, he carried the discipline of corporate India but wore khadi like it belonged to him.
He was not sentimental about systems. He wanted results. He also had a sharp sense of what institutions hide behind routine. He could smell delay the way a doctor smells infection.
When I spoke about the HIS dream, I expected questions about cost.
Instead, he asked about impact.
Would it reduce waiting time? Would it cut leakage? Would it bring transparency? Would it stop patients from being pushed around for files and reports? Would it stop a villager from being told to repeat a test simply because a report had been misplaced?
He saw the moral side of technology. Not the glamour.
He didn’t promise ease. He promised support. And in a project like this, that difference matters.
Dhirubhai, in his own style, provided the quieter kind of strength. He was less dramatic than Halbe, but steady in the way good institutions need. Dreams require energy, but they also require people who keep showing up when the dream becomes inconvenient.
I began to understand that if we were to attempt something like an HIS, we would need more than software. We would need protection—from cynicism, from fatigue, and from the inevitable chorus of “this will never work here.”
***
By the time the idea matured, it had stopped being about computers and started being about the hospital’s nervous system.
Registration, billing, laboratory reports, pharmacy inventory, ward notes, discharge summaries—these were not separate islands. They were one organism. In a paper system, the organism survives by improvisation. In a digital system, it survives by structure.
I could also sense, even then, that the greatest challenge would not be the code. It would be the culture.
Hospitals have muscle memory. They run on habits that have been reinforced for decades. Paper has its own comfort. You can hold it. You can hide it. You can blame it. A computer record is unforgiving. It exposes delays. It exposes errors. It exposes leakage.
And nothing frightens an institution more than exposure.
Still, I could not let the idea go.
Lucknow had shown me what was possible. Sevagram demanded that we try.
The Delhi Library
In the winter of 2003, Mr. Shripad Halbe summoned me to Delhi. As Vice President of the Kasturba Health Society and a long-time confidant of the Dhirubhai Mehta family, Halbe was a man who moved in significant orbits, yet he harbored a dream for MGIMS that had not been whispered, let alone attempted. He wanted to dismantle our paper-driven world and replace it, entirely and unapologetically, with a digital one. Halbe knew everyone who mattered—the politicians, the bureaucrats, and the captains of industry—and among them was Arun Shourie, then the Minister for Information Technology.
Halbe’s invitation was characteristic of the man: short, definite, and leaving no room for debate: “We are meeting Arun Shourie.”
Shourie was no ordinary minister. In my mind, he was already a legend—the fearless intellectual and journalist who had rattled the establishment with his pen before becoming a key figure in Vajpayee’s cabinet. The prospect of meeting him felt slightly surreal, as if I had been invited to step inside the morning newspaper to strike up a conversation with the lead editorial. I travelled to Delhi with a folder of notes and a mind crowded with doubts. I wondered if he would truly listen, or if this would be another of those perfunctory meetings where one speaks for five minutes only to be dismissed with a polite, vacant smile. I feared he might treat Sevagram as a quaint rural project, useful for a photograph but unworthy of serious investment.
Halbe, however, did not allow such doubts to take root. He carried certainty the way some men carry authority—naturally and without effort. We reached Shourie’s office on a cold evening to find a space that felt entirely un-bureaucratic, filled with more books than files and possessing the quiet dignity of a place where thinking is taken seriously. We were ushered into his library, a vast room lined with volumes that looked used rather than displayed, appearing almost as a structural argument against noise. Though Shourie was in the middle of a meeting, he paused, greeted us, and listened with a rare, focused intensity. It was a small but significant sign; while busy men often rely on the pretense of listening, Shourie listened with the genuine article.
***
I had rehearsed a formal pitch, but once I began speaking, the artifice vanished and it started to feel like a confession. I told him about MGIMS—its Gandhian roots, its rural mandate, and its stubborn refusal to chase money. I explained that we didn't seek computers for the sake of status; we sought them because paper was failing us. Paper delays care, hides leakage, and forces the poor to pay for administrative inefficiency. It forces relatives to run between counters like refugees, holding files like passports and begging for the mercy of a stamp or signature.
I spoke of what I had seen in Lucknow and expressed our desire for that same clarity in Sevagram—not to compete with urban giants, but because our patients deserved better than a chaotic trail of lost reports. I expected interruptions, feasibility questions, or a lecture on the lack of rural infrastructure. Instead, there was only silence and attention. There were no glances at the clock and no signs of impatience. When I finished, he simply said he would support the project. I walked out feeling something rare in public life: a door had opened without the need for a bargain.
***
On 12 February 2004, the machinery of the state began to turn. Mr. P. Soreng, a Deputy Director in the Ministry, tasked C-DAC Noida with designing and implementing a Hospital Information System for MGIMS. On paper, it looked like a routine administrative order, but in reality, it was the beginning of a profound upheaval. We did not fully grasp it then, but we were about to ask a rural hospital to change its entire muscle memory—registration, billing, labs, and pharmacy.
We were asking clerks who had lived inside paper registers for twenty years to suddenly trust a flickering screen. We were asking residents, already exhausted by clinical duties, to shoulder the extra burden of "testing" a new system. Most significantly, we were asking departments to surrender their private silos for a shared, transparent digital ecosystem. The technology would come later; first would come the resistance, the fatigue, and the slow, stubborn work of persuasion.
As is always the case in Sevagram, the weight of this work would fall not on those of us who sat in meetings, but on the people who stood at the counters. Somewhere inside me, the excitement was tempered by a quiet awareness: we had invited a storm into the hospital, and once it arrived, we would simply have to live through it. The file had moved; now, the real work would begin.
How Sevagram Went Digital
In late 2003, when the idea of a Hospital Information System (HIS) first landed in Sevagram, it did not arrive with the fanfare of a revolution. It arrived as a stack of official letters, a collection of unfamiliar names, and a promise that sounded dangerously ambitious for our setting. At the time, MGIMS was a rural teaching hospital fueled by paper, collective memory, and raw human stamina. Our wards were perennially full, the OPDs overflowed with the desperate, and every department was its own sovereign state with its own secret language. Files moved between counters like tired, fraying messengers; lab reports traveled in envelopes like clandestine notes; and billing depended on slips of paper that could vanish into a pocket as easily as a forgotten coin. We weren’t dreaming of "digital transformation." We were simply trying to survive the daily load without losing our minds.
The Center for Development of Advanced Computing (C-DAC) was the chosen architect. They had built systems for SGPGI Lucknow and stumbled through mixed results in Delhi, but the government decided that Sevagram would be the testing ground for their next great effort. The project was titled, with bureaucratic grandiosity, “Design and Development of Advanced Hospital Management System and Prototype Implementation for MGIMS.” That word—prototype—was the most honest thing about the document. It meant we were to be the place where the system would learn to walk, likely by falling on its face several times first.
On 30 December 2003, Mr. R.K. Verma of C-DAC Noida identified the men who would lead us into this new era: Naveen Kumar Jain, Pradip Parida, and Praveen Srivastava. By February 2004, the Ministry formally tasked them with the implementation. The budget was ₹100 lakhs—a king’s ransom in 2004—and the timeline was a optimistic twelve months. In reality, the project ignored "file time" and ran on "human time." It would take four years, eventually reaching completion in June 2008.
***
On a PowerPoint slide, the C-DAC plan was a masterpiece of order. Phase 1 would build the clinical spine—the very skeleton of the hospital. Phase 2 would handle the unglamorous machinery of laundry and security. Phase 3 was pure science fiction: digital radiology.
But in a hospital corridor, this neatness looked like impending chaos. Our staff hadn't grown up with computers; many were nervous even touching a mouse. We didn’t have a culture of "data entry"; we had a culture of "somehow manage."
Then came the first heavy blow: the initial project manager left before the requirements were even gathered. It was the editorial equivalent of losing your star opening batsman for a duck. All the time spent by staff explaining registers and walking engineers through wards was evaporated. The document—the very DNA of our workflow—was lost. When the new team arrived, the energy had soured. People were polite, but the enthusiasm had been replaced by a quiet, cynical wait for the inevitable failure.
This is where Praveen Srivastava saved us. He stepped in as project manager with the calm of a mathematician who knew that progress rarely moves in a straight line. He didn't offer speeches; he offered structure. He regrouped the team and began the grueling work of collecting requirements all over again. None of us knew then that this struggle would birth e-Sushrut, a system now used across India. We were only thinking about how to survive the next morning’s OPD.
***
A system is built by code, but it is implemented by people who take abuse with a smile. Sevagram became a colony for a steady stream of C-DAC engineers—men like Rajeev Yadav, Ajay Gupta, Devendra Rao, and Ravi Sinha—who sweated through our summers and learned our hospital’s dialect.
There were the "House Officers" of the server room: Ashish Singh, Mantosh Kumar, and Amit Kumar Digaliya. Each left a mark. Ravikumar built the insurance module in a cramped pharmacy room; Ajay Gupta mastered the stores. Amit Kumar, however, became family. He was taken into local homes, tasted Maharashtrian meals with the curiosity of a student, and spent his weekends exploring Bordharan. These small human connections were the "grease" that allowed the digital gears to turn.
I remember Holi in 2005. Two young female engineers were warned to stay inside. They didn’t listen. Sevagram Square on Holi does not deal in pastels; it deals in total immersion. They were drenched and startled, finding themselves in a crowd that meant no harm but looked like a riot. Our staff member Hemant had to rush out and rescue them, a small act of chivalry that reminded us that while technology is modern, implementation still rests on old-fashioned human decency.
***
In August 2004, I left for Berkeley for my MPH. I handed the HIS reins to Dr. Rajnish Joshi. He was thirty, a young lecturer in Medicine with a temperament for complexity. My brief to him was brutal: Get HIS on the desktops by August 2005. Rajnish built a team of quiet revolutionaries. First was Bhavana, who had already been secretly writing FoxPro programs for discharge summaries in the Medicine department. Her work was "emotional labour"—maintaining her composure while training staff who were terrified of the screen, all while managing a young family.
Then there was Yogesh Khond. Every great project has a hero who doesn't appear in the official letterhead. Yogesh had endured more than his share of life's cruelty—losing his father to cancer, dropping out of his BSc to survive—but he had a stubborn, innate love for machines. He became the "man who could fix anything." When the system broke—which was nearly every hour—Yogesh was the one who answered the call. He wasn't trained as an IT professional; he became one by necessity, learning faster than the system could fail.
***
The physical spine of the system was miles of cable. In 2004, networking felt like surgery on the earth itself. Digging up the campus roads to lay fiber optics was a bureaucratic nightmare, so the contractor did it "village heist" style—quietly, overnight, while the campus slept. By dawn, the roads looked innocent again, but the cables beneath them were already carrying the future.
Training was a comedy of errors. Nearly 300 staff members were dragged to the computers. Some came with the fear of a child in a dark room; others came with a quiet, fierce pride.
But the "insurance module" launch in late 2004 nearly broke us. It went live under immense pressure, and it was a disaster. Mismatched cash, duplicate cards, and a discrepancy of ₹2 lakhs. Worst of all, the source code was accidentally overwritten on a PC. It sounds farcical now, but we were learning the hard way that computerization doesn't create discipline; it only shines a light on the lack of it.
***
By 2005, the Oracle servers had arrived, but they struggled. A busy teaching hospital is not a demo unit; it is a high-traffic monster. Transactions crawled. On 11 August 2006, I wrote to C-DAC with a line that came from the soul: “We look forward to a server that would run, not crawl.” It took years of upgrades—more RAM, better processors, and the move to Tomcat in 2012—to find stability. The HIS survived not because it was perfect, but because we were too stubborn to let it die.
When people ask me for the "hero" of the Sevagram HIS, I don't give them a single name. I tell them about the engineers who took the heat, the clerks who overcame their fear, and the cables laid under the cover of darkness. It wasn't a visionary moment; it was a thousand small persistences. The first time a patient’s name appeared on a screen without a frantic search for a paper file, I didn't feel pride. I felt relief—the kind you feel when a long-standing headache finally eases. We didn't become digital because we were advanced; we became digital because we were willing to learn, one mistake at a time.
The System Learns to Breathe
A presidential visit is a peak moment in the life of an institution, offering a photograph for the archives, a fleeting surge of pride, and a brief memory of grandeur. But the next morning, the hospital invariably returns to its old, unvarnished truths. The patients still crowd the OPD in their silent, patient thousands; the wards still overflow with the weight of rural illness; and the emergencies continue to arrive with their characteristic lack of warning. If the Hospital Information System had to prove its worth, it would not be under the gaze of the President, but during those ordinary days when nobody clapped, when nobody cared for the word "innovation," and when the only thing that mattered was whether a specific report could be retrieved in time to save a life.
In those unremarkable hours, the system began to mature. It didn’t happen through a dramatic miracle, but rather through the slow, grinding process of repetition, irritation, small technical fixes, and eventual, reluctant acceptance. One of the earliest moments I realized the HIS had truly begun to weave itself into the fabric of the hospital occurred not during the busy office hours, but in the dead of night.
When a patient arrives with chest pain at midnight, the resident is often working in a state of high-octane anxiety. In the era of paper, the resident's decisions were hostage to memory, luck, or a relative who happened to be carrying a frayed discharge card. With the HIS, that same resident could search by a name or a village, and within minutes, the past record would surface—a digital ghost rising to offer clarity. It wasn't always a perfect record, but it was enough to cut through the old fog of guesswork, giving young doctors a newfound confidence and making the entire hospital feel inherently safer.
***
Our patients are mostly villagers who have lived lives requiring immense endurance, and they understand how systems fail far better than we do. What surprised me most was how quickly rural women grasped the logic of the HIS. Often, when we asked for old paper reports, they would point not to their bags, but to the monitor near the nursing station with a gesture that seemed almost teasingly to say, “Why are you asking me? It is all there.”
Many of these women had never written a full sentence in English, yet they trusted the screen because it offered a security that paper never could. Paper gets wet, it tears, and it disappears in the chaos of a life lived in a small hut; the screen, however, stayed. The HIS did more than just digitize data; it changed patient behavior and created a new kind of confidence—the belief that the hospital would remember them.
None of this progress came without a heavy human cost, for change in a hospital is never a neutral act. Every new system steals time from someone, and in our case, it was the juniors who paid the price. It was the interns filling out both paper slips and digital orders; the nurses learning to type when their hands were already full of syringes and dressings; and the lab technicians asked to trust machine-to-server transfers when their entire professional lives had been validated by the stroke of a pen in a register.
This era also demanded significant emotional labor, particularly from Bhavana while I was away at Berkeley. Without the "Kalantri name" to act as a shield, she had to face department heads who were often frustrated and cynical. If a bug caused a report to be wrongly mapped, it wasn't dismissed as a software glitch; it was treated as a personal insult to a department’s competence. Bhavana absorbed these blows, and when she called me at the end of a long day, she wasn't looking for sympathy—she was seeking a partnership in the struggle.
***
The HIS eventually won people over through small, practical reliefs rather than grand speeches. We saw the end of the "daily marathon" for biochemistry attendants who used to spend three hours a day acting as human couriers for bundles of sugar and creatinine reports. We saw Pathology residents, who previously stayed up until 2:00 a.m. manually copying parameters, finally finishing their work earlier as the mindless parts of their labor disappeared. These weren't the kind of victories that required a ribbon-cutting ceremony, but they returned the most expensive currency in healthcare back to the hospital: time.
Perhaps the most powerful change, however, was not clinical but moral. In many hospitals, the bill is a dark mystery that families pay out of fear. With the HIS, our patients began receiving itemized, system-generated bills that brought fairness into the light. Even if a patient couldn't read every line, the very structure of the printed bill created trust. It allowed us to demonstrate what we had always claimed but could never prove: that MGIMS charged procurement costs plus a modest margin, not the inflated market prices seen elsewhere.
Before the HIS, the hospital functioned as a collection of isolated islands, each department unaware of the other's real-time reality. The system began to connect these islands, allowing nurses to check for X-rays and residents to verify blood cross-matching without a dozen phone calls or messengers. It didn't make the hospital quiet—hospitals are never quiet—but it organized the chaos. Slowly, the HIS stopped being a project and started becoming an atmosphere, a shared digital breath that the institution took every single day
Building the System
In 1999, I travelled to Lucknow to see a health informatics system developed by C-DAC at Sanjay Gandhi Post-Graduate Institute of Medical Sciences (SGPGI). Until then, I had read about hospital information systems, but seeing one in action was different. The speed, the order, the clarity of information, and the way it reduced confusion in the hospital impressed me deeply.
When I returned to Sevagram, the idea stayed with me. MGIMS was not a large metropolitan institute, and we did not have the luxury of unlimited resources. Yet I kept wondering why efficiency and accuracy should remain the privilege of big cities. If a hospital runs on discipline, then information should run on discipline too.
Mr. S.R. Halbe played a pivotal role in turning this idea into something real. He arrived in Sevagram in the mid-1990s and quickly became someone who understood not only accounts and systems, but also people. In the winter of 2003, he called me to Delhi and took me to meet Arun Shourie, then the minister responsible for information technology.
We met him in his library, a room that looked as if it had been built for long conversations and difficult decisions. Although he was in the middle of a meeting, he gave us time. I spoke about MGIMS, about our hospital, and about our plan to implement a Hospital Information System. He listened with interest and promised support.
On 12 February 2004, Mr. P. Soreng from the ministry formally tasked C-DAC Noida with designing and implementing an HIS for MGIMS.
The paperwork moved quickly. The hospital did not.
In August 2004, I left for Berkeley for my MPH. Before leaving, I handed over responsibility to Dr. Rajnish Joshi with a brief that sounded simple when spoken aloud: get HIS on hospital desktops by August 2005.
Bhavana was at the centre of this work. She also brought in Yogesh Khond, a young man who had lost his father to oral cancer and had started as an attendant in the Dean’s office. He had talent and hunger, and Bhavana recognised it early. In a project like HIS, the most valuable people are often not those with impressive degrees, but those who can learn quickly and stay steady when the system collapses.
C-DAC selected a Java-based server that was said to be used by top banks. On paper, it sounded reassuring. On our campus, it behaved like an exhausted creature. It froze, slowed down, and sometimes refused to respond. Transactions failed. Screens hung. Printers jammed. The network crawled.
For interns and residents, ordering a test began to feel like waiting for a slow train that never arrives. In a busy hospital, delays are not just irritating. They become dangerous, because every delay adds pressure to a system already running at full capacity.
We were learning this the hard way.
On 11 August 2006, I wrote to C-DAC in frustration:
“We at MGIMS look forward to the server that would run, not crawl. Indeed, if the speed issue is set right, we will heave a huge sigh of relief!”
It was not a clever line. It was an exhausted one.
In the early days, residents had to do double work. They filled the paper requisition forms as usual and also entered the same orders digitally, because the system needed testing. This meant extra time, extra fatigue, and extra resentment, especially during night duties.
C-DAC sent system analysts who stayed in Sevagram for two months. Our team took them to department after department, nearly fifteen of them, and patiently explained workflows. Some heads of departments were supportive. Some were cynical. Some became defensive and found faults in every screen. A few simply pushed the job onto the junior-most person, who did not fully understand how the department actually functioned.
After three months, a blow arrived that felt almost absurd. C-DAC informed us that the system analysts had resigned and left without submitting their report. The entire system analysis had to be repeated.
Bhavana had to face this at a time when I was away in Berkeley. She was not only dealing with software and servers. She was dealing with disappointment, anger, and the tiredness of repeating work that should never have been lost.
The bugs were many, and some were frightening. Once, the same lab report appeared in multiple patient records. In one ward, ten consecutive patients were shown as positive for malaria. The Pathology head wrote an angry letter. It was embarrassing, but more than that, it was alarming. A hospital information system cannot afford to be casually wrong. It has to be boringly reliable.
At that stage, we did not have a trained in-house technology expert. The C-DAC engineers were learning too. We were all learning while the hospital kept running, and that is what made it exhausting.
The strongest resistance came from Pathology. They felt the system was a waste of time and energy. They demanded data entry operators, arguing that doctors and technicians should not waste time entering data. The institute refused, because the truth was simple: if a system is built on outsourced data entry, it never becomes part of hospital culture. It remains someone else’s burden.
Not everyone resisted. Dr. MVR Reddy in Biochemistry supported the system fully. Dr. Deepak Kumar Mendiratta, the Microbiology head, also stood by it and tolerated the teething troubles. The surgical departments were mostly indifferent. They did not fight the system, but they did not champion it either.
For Bhavana, the resistance was emotionally taxing. The system was slow and error-prone, and she had to face senior colleagues who were cynical and impatient. She was managing the home and the children, while carrying a project that had begun to feel like a test of endurance.
C-DAC began with registration and insurance. For many clerks, it was their first encounter with a computer. They were nervous, curious, and eager.
During training, someone asked Prem Das, one of the clerks, to “click an icon.” He lifted the mouse and held it against the screen. For a second, everyone froze. Then the room erupted in laughter, Prem Das included. He laughed, then he learned. Within a week, the staff were comfortable with the keyboard and mouse.
And something quietly remarkable happened. Registering 1,500 patients took no more than three hours. In a hospital that had lived on paper, this felt like a new kind of order.
The cost of the HIS was not only financial. It was time, fatigue, and the strain of change in a hospital that was already stretched. Yet the hospital’s lowest rung, the people who actually do the work, stood by the system. Residents, technicians, pharmacists, nurses, ward staff, OPD staff, lab staff, kitchen staff, accounts staff, and administrative staff kept going, even when many wondered if the project was worth it.
We involved them because they understood how the hospital really functioned. When they felt included, the system slowly became theirs, not ours. That sense of belonging saved the project more than any server upgrade ever could.
Over the years, the HIS entered our lives in an intimate way. It followed us home, entered our conversations, and occupied our weekends. Like the film Chalti Ka Naam Gaadi, it began to feel like a family enterprise, full of teamwork, breakdowns, repairs, arguments, and strange humour.
Even today, when our Honda Jazz approaches the blind turn at the railway underpass between Sevagram and Pavnar, my granddaughters shout, “Baaju!” They are warning the car.
In our lives, the HIS was also a sharp turn. Once we took it, there was no going back.
From Memory to Mouse
When I first joined MGIMS, our “medical store” was really just a humble dispensary. It sat quietly in a corner of the hospital, functional but unassuming. The wooden shelves held loose tablets—aspirin, chlorpheniramine, Nilpyrine—and a few familiar glass bottles: cough sedatives, expectorants, throat paints, ear drops, glycerine magsulf, and zinc oxide ointment. If a doctor wanted something unusual, they had to write a prescription for an outside shop.
The dispensary didn’t run on software; it ran on experience and memory. It was anchored by two dependable compounders, Sudhakar Mitkar and Ambulkar. They knew every bottle, every drawer, and every patient’s face by heart. When both of them retired in 2006, the dispensary lost its soul. Within two years, it shut down for good.
What replaced it was not just a bigger room. It was a completely different way of thinking—about medicines, money, and the dignity of the patients who had to buy them.
***
In those early years, we stocked what we could and managed shortages the way small hospitals always do: by improvising. The concepts of an organized inventory, batch tracking, expiry alerts, and systematic procurement felt like science fiction. Most of us could not even imagine that a rural teaching hospital could run a modern pharmacy with the discipline of a corporate chain. We were too busy treating patients and making do with what we had.
The change began slowly in 2004, when C-DAC arrived with the ambitious plan of computerising hospital services. A year later, Ajay Gupta built a small part of the pharmacy module. At first, the system hobbled along on two legs—paper and computer—because no one trusted the new method completely. The old registers stayed open, and the new screens flickered beside them, waiting to be believed.
***
The medical store staff had every reason to feel anxious. For years, their competence had been measured by manual speed—how fast they could decipher a scrawled prescription, find the medicine, and keep accounts in thick registers. Suddenly, a machine arrived and demanded a new, alien vocabulary: clicking, typing, saving, searching.
Mr. Chhagani—who later became our Chief Pharmacist—would often remember those early days with a smile. He confessed he was initially so intimidated that he didn’t even have the courage to touch the mouse. It looked harmless, but to him, it represented the terror of making mistakes in public, of slowing down the queue, of being judged by younger people who seemed to learn faster.
Tragically, Chhagani’s story was cut short. In 2025, just two years before his retirement, he was killed in a road accident when his car collided with a truck. But before he left us, he had transformed from the man who feared the mouse into the man who mastered the machine.
***
Ritesh, who joined the medical store as a clerk in 2007, remembers the old procurement system as a relic of a slower age. It functioned like a dusty file in a government office. Doctors recommended branded drugs. The medical store had to type letters to companies and send them by post. Companies forwarded lists to distributors. Distributors took their own sweet time. Supplies arrived late—or not at all. Stock-outs were common, and as always, the patients paid the price.
When C-DAC began computerising hospital services, the medical store saw a chance to upgrade properly. We decided to migrate from the old FoxPro program to the newer Oracle-based system. That shift happened on a day I still remember clearly—not because it was dramatic, but because it was symbolic.
It was Maha Shivratri—Monday, February 23, 2009. While the rest of the town was celebrating, the pharmacy staff stayed behind, working through the holiday to migrate every single item of inventory from FoxPro into Oracle. The next morning, the store opened with the new software. It was not just a technical switch. It was a declaration that we were done with half-measures.
Bhavana’s role in this transition remains one of my favourite ironies. She had helped create and run the FoxPro system earlier. Yet she was the one who insisted we replace it with the C-DAC module and integrate it fully with the hospital’s electronic ecosystem. She approached it the way a good cook approaches change: she was willing to retire her own signature dish if she found a better recipe.
***
Technology improved tracking, but the real revolution came from a deeper question: What medicines should we stock—and at what price?
Between 2007 and 2011, we had a Drug and Therapeutic Committee meant to recommend rational drugs. On paper, it sounded ideal. In practice, it faltered. Opinions clashed, and decisions often remained stuck in the safe middle ground between “what is best” and “what is familiar.”
So we changed the approach. We formed a new drug committee chaired by Dr. Poonam Varma Shivkumar, bringing together department heads, the administrative officer, the chief accountant, and the chief pharmacist. It met annually, but it worked with a seriousness that matched the stakes.
In 2009, the medical store got a adrenaline shot in the form of Dr. Rajnish Joshi. Then an assistant professor of Medicine, Rajnish came armed with an MPH and PhD from UC Berkeley and was asked to look after the ailing store. Rajnish was quick, decisive, and impatient with inefficiency. He knew how to rally a team and get work done. Having already played a key role in building our Hospital Information System (HIS), he brought that same clarity to the pharmacy.
Under his watch, procurement became systematic. Tenders and quotations brought prices crashing down. Although Rajnish left Sevagram a year later—moving to AIIMS Patna, Sikkim, and finally AIIMS Bhopal, where he became the Medcine department head and also a Dean—he laid the foundation. Later, Dr. Ramesh Pande took the baton and has carried the work forward for over a decade, improving the system year after year.
In February 2010, we made a decisive shift: we focused on generic and branded-generic medicines, and we digitised the tender process end-to-end. We also revolutionized the pricing. Earlier, like many hospitals, we deducted a percentage from the MRP. But MRP is often a fantasy number, designed for marketing rather than honesty. We moved to a transparent model: Procurement Cost + 20%.
I often think of the ordinary patient with multiple chronic diseases—heart disease, diabetes, hypertension—who needs a cocktail of tablets every day. Earlier, such a patient would bleed money slowly, month after month. With the new system, many could buy their daily medicines for around five rupees a day. In India, that is less than what people spend on a cup of tea without thinking twice.
Even auditors were stunned. Some would stare at the price list and ask, half-suspiciously, “How can you sell this for ₹24 when the MRP is ₹100?” A few were so impressed they bought medicines for their own parents. That was not part of our plan, but I took it as an unintended certificate of credibility.
***
Heena joined the medical store as a pharmacist in 2010, taking to the work like a duck to water. “I still remember those days,” she told me. “We prepared purchase orders by hand, and it would take forever to make even one.”
By 2011, that manual labor was history. The team began using the digital system to procure everything—from tablets and syrups to injections, sutures, mesh, staples, stents, balloons, and implants. The entire lifecycle of a medicine—from the moment we needed it to the moment a patient paid for it—became digital, transparent, and trackable.
***
Over the years, the medical store moved around like a restless tenant. It started near the Obstetrics wards, moved to the old Surgery OPD, and finally, in 2020, found a proper home: a spacious, newly built complex inside the hospital building.
Today, the new store runs like a small airport. There are separate counters for outpatients, inpatients, senior citizens, emergency cases, and dialysis patients. On an average day, it serves around 1,500 patients and generates nearly two lakh rupees in sales.
Not everyone welcomed the change initially. Some doctors worried that "generic" meant "inferior." We listened, we discussed, and we tightened our quality checks. But we did not abandon our central philosophy: patients must not be punished for being poor.
The fall in prices has been dramatic. A Paclitaxel injection (260 mg), which cost ₹13,500 in 2015, now costs around ₹550. When you see a reduction like that, it doesn't look like "policy." It looks like survival.
The most convincing evidence is not in a spreadsheet. It is at the counter. Patients arrive tired, clutching prescriptions, mentally calculating if they have enough cash. Then they hear the amount. Their faces change—first disbelief, then relief, and sometimes, a smile. They look at the pharmacist as if a small miracle has just occurred.
In those moments, I don’t see a pharmacy module or an inventory system. I see what a hospital is supposed to do: make treatment possible.
Five Minutes with President Kalam
By 2007, the Hospital Information System had graduated from a fragile experiment into a stubborn reality. It had survived the sceptics, the slow servers, and the endless, exhausting phone calls that accompany any attempt to drag a traditional institution into the digital age. It was still imperfect—temperamental on bad days and sluggish on others—but it had achieved the most important quality of all: inevitability. People no longer asked, “Why are we doing this?” They merely asked, “Why is it not working faster?”
Then came the news that made the entire campus sit up straight. Dr. A.P.J. Abdul Kalam, the President of India, was coming to Sevagram on June 15, 2007.
For a rural teaching hospital, a presidential visit is not merely an honour; it is a logistical storm warning. The Special Protection Group arrived first, with their walkie-talkies and faces that revealed nothing. Routes were mapped, corridors sterilized, doors sealed, and the forgiving, fluid routine of the institute was suddenly placed in a corset. Every movement was planned; every minute had a price.
In the middle of this tightening grid, I was handed a task that sounded simple but felt terrifying. I had to demonstrate the HIS to the President.
I had five minutes.
***
Five minutes is a breath. It is nothing when you are trying to explain the nervous system of a hospital to a rocket scientist.
In those days, the HIS was a work in progress. It was registering patients, generating bills, and beginning to knit the laboratories into the wards. It allowed residents to order tests without chasing peons, but on bad days, it would freeze mid-transaction, provoking the specific, helpless rage that only a tired doctor at 2 a.m. can feel. I knew Dr. Kalam would not be seduced by PowerPoint slides or jargon. He was not a politician who smiled politely at buzzwords; he was a man who understood how machines failed. He would want to see if the logic held.
Security decided that the demonstration could not happen in the crowded OPD. Instead, we were banished to the corridor of the Radiotherapy department—a narrow, controllable space. A corridor is an odd place to showcase a digital revolution. A laptop screen was too small for a delegation, and a projector would wash out under the harsh tube lights. We needed something bold.
So, the hospital bought a 36-inch high-resolution colour screen for ₹85,000.
Writing that figure today makes me pause. In 2007, that amount could run a village household for a year. It was the kind of money that made you question your own sanity. But the decision was made instantly, because when the President is coming, hesitation is a luxury you cannot afford.
***
In the days leading up to the visit, my mind ran on two parallel tracks. One was clinical: patients would not stop falling ill just because a VIP convoy was approaching. The other was digital: we had to make the software behave.
I rehearsed my script until I could say it in my sleep. I stripped away the adjectives and the self-congratulation. The HIS was not a trophy to be polished; it was a tool to be used. I wanted to show the journey of a patient—Registration, Insurance, OPD, Lab, Discharge—without a single wasted word.
Mr. S.R. Halbe and Mr. Dhirubhai Mehta watched these preparations with the quiet intensity of men who had gambled on this project. Mr. Halbe, practical as ever, asked the only question that mattered: “What if it crashes?”
It was not a threat. It was the question of a man who respected the law of averages.
“We will keep backups,” I said, sounding more confident than I felt. “And we will pray.” Technology, I had learned, is much like medicine. You can prepare, anticipate, and mitigate, but you can never guarantee the outcome. There is always a small, silent space where fate sits.
What the President would not see, however, was the invisible labour that made the screen light up. For months, our residents—specifically the postgraduate batch of 1998—had served as unwilling test pilots. Residents like Udit Narang and Namita Jajoo did what residents always do: they complained about the extra work, they rolled their eyes at the "green button" that loaded too slowly, and then they did the work anyway. The system survived not because the code was perfect, but because the juniors absorbed the pain of the transition.
***
On the evening of June 15, Sevagram felt scrubbed and held its breath. The humidity was heavy, but the usual chaos of the hospital had been hushed.
When Dr. Kalam walked into the corridor, the space suddenly felt smaller. He moved with that famous, springy energy that belied his age, his eyes darting around with genuine curiosity rather than ceremonial boredom. He didn't look like he was inspecting a guard of honour; he looked like he was about to debug a circuit.
I stood by the expensive screen, my mouth dry. I began.
I walked him through the registration, the unique ID that prevented duplication, the lab orders, the retrieval of reports. I showed him how a system-generated report was valid without a signature because the integrity came from the process, not the ink.
The moment I feared—the spinning hourglass, the frozen screen—never came. The server behaved beautifully. The pages loaded with a snap. The data appeared cleanly.
Dr. Kalam did not just watch; he engaged. He asked questions about the logic and the utility, treating the software not as a magic trick but as a working model. When I finished, he smiled. It was not the practiced smile of a dignitary on a schedule. It was the smile of a teacher who has just seen a student solve a difficult problem.
That smile travelled down the corridor like a quiet blessing. I felt my shoulders loosen for the first time in a week.
***
After the convoy left and the security detail packed up their radios, the campus exhaled. People began speaking at normal volumes again. The tension dissolved into the familiar, comforting noise of a working hospital.
But for me, the victory wasn't the successful demo. It was what that success signalled to the people who kept the hospital running. Somewhere that night, a clerk at the registration desk might have felt a little more important. A cynical resident might have felt the system was worth the trouble. And Bhavana, who had poured her life into the code, must have felt that the long nights were not in vain.
In a hospital, the most fragile thing is not a server or a patient’s pulse. It is morale. And that evening, without speeches or slogans, the morale rose.
Building Virtual Sevagram
The Hospital Information System was a story about the inside of the hospital—the nervous system of counters, wards, labs, and bills. It was about the patient’s journey from the village to the bedside. But around the same time, a quieter, equally transformative dream was taking shape. We had begun to ask a different question: What should MGIMS look like to the outside world?
In the year 2000, the internet was still a novelty in India. In a place like Sevagram, built on Gandhian simplicity and situated miles from the nearest tech hub, the "web" felt almost mythical. Most people here had never sent an email; fewer still had seen a website. The word “online” belonged to Bangalore or Mumbai, not to a rural medical college where the electricity still flickered during the monsoons.
Yet, the need was real. Students applying for admission were hungry for information. Alumni scattered across the globe wanted a way to look back at home. Parents wanted exam results without the crushing anxiety of waiting for the post. We needed a public face, but we had no IT department to build one.
***
The first bridge was built not by a contractor, but by an alumnus.
Dr. Avita Pereira, from the 1990 batch, had moved to Bengaluru after her internship. She and her husband, Dr. Johnson, shared a fascination with technology that was rare for doctors in those days. While most of us saw computers as glorified typewriters, they saw them as tools of connection.
One day, Avita reached out with an offer that felt both generous and improbable: “We want to build a website for MGIMS.”
There was no contract, no consultancy fee, and no corporate pitch. It was simply an act of gratitude. For months, Avita and Johnson worked on the code and design, trying to translate the lived, messy reality of Sevagram into something that could sit neatly on a screen. It was a difficult task; a hospital is a chaotic, breathing organism, and capturing it in static HTML pages required immense patience.
On October 2, 2000—Gandhi Jayanti—the MGIMS website went live. By today’s standards, it would look primitive, perhaps even quaint. But for us, it was a door opening to the world.
***
The website’s impact was immediate, and its greatest gift was practical: it killed the anxiety of the entrance exam results.
Until then, the weeks following the exams were a time of torture. Students waited for letters that might get lost; parents travelled long distances just to scan a notice board. The stress spread like a fever through towns and villages. Putting the results online changed that overnight. Suddenly, a student could check their fate from a cyber-café in Nagpur or a dial-up connection in Delhi.
Within six months, the website recorded nearly 25,000 visitors. That number may seem trivial in the age of viral videos, but for a rural medical college in 2000, it was a stampede. It meant that Sevagram had become searchable. We had created a “Virtual Sevagram,” accessible to people who had never set foot in Wardha.
***
Launching a website is the easy part; sustaining it is the penance.
Over time, the original site began to show its age. Technology moved faster than our capacity to update it. Pages became stale, links broke, and new needs emerged—online applications, alumni databases, research archives. We tried several times to revive it. Ashwini, then a medical student, created a preliminary site for the Department of Medicine. We collaborated with his colleagues—Ramashish Bhutada, Nikhilesh Ghushe, and Akhilesh Mritunjai—to patch things up. Ramashish, who later founded Deusco Technologies, exchanged countless emails with me between 2006 and 2010, trying to build a comprehensive portal. We even paid for a system audit in 2007, hoping an expert view would force a leap forward.
But these initiatives often stalled. The relentless demand of hospital life has a way of swallowing side projects. The website began to feel like a half-built house: the address existed, but the rooms were empty.
In November 2008, however, we took a small but crucial step. We purchased the official academic domain from ERNET India: mgims.ac.in. We finally had the right name. Now, we just needed to build the right home.
***
The true revival finally arrived in 2015, and it came from within the family.
By then, Ashwini had grown from a curious student into a professional who understood systems architecture. He decided to rebuild the website from scratch—not as a hobby, but as a serious institutional project. He was joined by my daughter-in-law, Shaily.
Their partnership gave the project its balance. Ashwini brought the structure, the logic, and the technical backbone. Shaily brought the design sense, the content clarity, and the human touch that prevents a website from becoming a cold directory.
At home, our conversations shifted. Dinner table talk drifted from clinical cases and ward politics to navigation menus, subdomains, and the eternal question of good design: How does a user find what they need in two clicks? They studied medical school websites from Harvard to Johns Hopkins, not to imitate them blindly, but to understand the grammar of elegance.
They settled on a simple philosophy: Information, Design, Simplicity.
In February 2015, the new MGIMS website went live. It was clean, functional, and modern. It told the institute’s story without clutter and made essential information accessible without drama. Watching them work was strangely moving for me. It was not just a technical project; it was a continuation of a larger family habit—building systems that reduce friction for others.
***
While the website became our public face, another digital shift was brewing quietly inside the campus—one that would end the tyranny of paper.
In 2008, Ashwini—still an intern—noticed something that the rest of us had accepted as a law of nature: the inefficiency of the paper circular. Notices were printed, pinned, photocopied, distributed, misplaced, ignored, and then rediscovered when it was too late. He realized that Google Apps for Education offered free institutional email services. He applied, verified MGIMS as an educational institute, and secured the license.
It was a masterstroke that saved the institute money, but more importantly, it changed the culture. On October 7, 2009, Ashwini wrote to me, brimming with the impatience of youth:
“I am testing the MGIMS intramail on Google apps, and it is working flawlessly! The familiar and simple Gmail UI makes it even better… Please start the official process of obtaining the leased line as soon as possible (now!).”
He also pushed for a larger vision, urging us to think beyond just email: “With 2.0, we must think big… A system that’s unimaginable and clearly the best internationally.”
I replied instantly, because such enthusiasm is contagious: “Fantastic ideas! Go ahead – I will talk to the KHS management.”
In May 2009, Intramail began rolling out. It started slowly—some faculty were indifferent, others tech-phobic—but once the Medical Superintendent began emailing circulars instead of printing them, the shift became irreversible. A student could now email the Dean. A resident could message a consultant. The campus became lighter, faster, and less wasteful.
Today, when I log into an official MGIMS email address, I often remember that intern urging his father to act “now.” It reminds me that in Sevagram, innovation rarely comes from expensive consultants. It comes from the people who live here, who see the cracks in the wall, and care enough to fix them.
***
Looking back, the HIS, the website, and the Intramail were not separate stories. They were two arms of the same instinct. One was about making the hospital safer and faster for patients; the other was about making the institute visible and connected to the world.
iPads at the Bedside
In 2011, we decided to attempt something that felt, in equal measure, obvious and audacious: we wanted to make our hospital data mobile. While our Hospital Information System had matured impressively on desktops, the reality of medicine is that patient care is rarely a desk job. It happens at the bedside, during the chaotic rhythm of ward rounds, in the corridors, and in those critical, fleeting minutes when a junior doctor must make a decision that is both quick and correct. The question we faced was simple: Could we carry the hospital’s brain in our hands?
We began the search for a technology partner capable of translating our complex, desktop-based HIS into an iPad application that was fast, clean, and devoid of clutter. Ashwini introduced me to Sourcebits, a Bengaluru-based company whose portfolio had caught his eye. One of their applications, Night Stand HD, had reportedly crossed four million downloads in four months—a figure that sounded almost fictitious to me at the time. Yet, it signaled that they understood the three things we needed most: design, usability, and scale.
Sourcebits was founded in 2006 by Dr. Rohit Singal, a radiologist who possessed the restless instincts of an entrepreneur. He had ridden the early wave of the iPhone ecosystem, building hundreds of apps across various platforms. Their reputation was robust enough for us to take the gamble; we walked them through our workflow, explained the intricacies of the HIS, and awarded a contract of ₹30 lakh to build an interface for MGIMS.
Two individuals became the backbone of this project: Amit Pandey, a partner at Sourcebits, and Farzan Siddiqui, a dedicated software engineer. Over the next nine months, they worked with a steady, quiet persistence, supported by colleagues like Giridhar Krishnamurthy, Girish Karudi, Shashank Lagvankar, and Vivek Menon. My own role was less glamorous but perhaps more relentless; I became the bridge between the doctors who demanded perfection and the developers who dealt in code.
Our weeks were consumed by Webex sessions, long email chains, and repeated face-to-face discussions where we dissected the user experience. We agonized over hundreds of granular decisions—what data should appear instantly, what could afford to be one click away, and what must never be buried under a menu. Naturally, we faced the predictable friction of digital transformation: server breakdowns, connectivity drops, database glitches, and the stubborn, technical challenge of importing high-resolution radiology images smoothly onto a handheld screen. We did not solve these issues in one dramatic stroke of genius; we solved them the way hospitals solve complex cases—step by step, with stubborn patience.
In January 2013, I met the Sourcebits team in Bengaluru. By then, the project had acquired both momentum and shape — and we were ready to build.
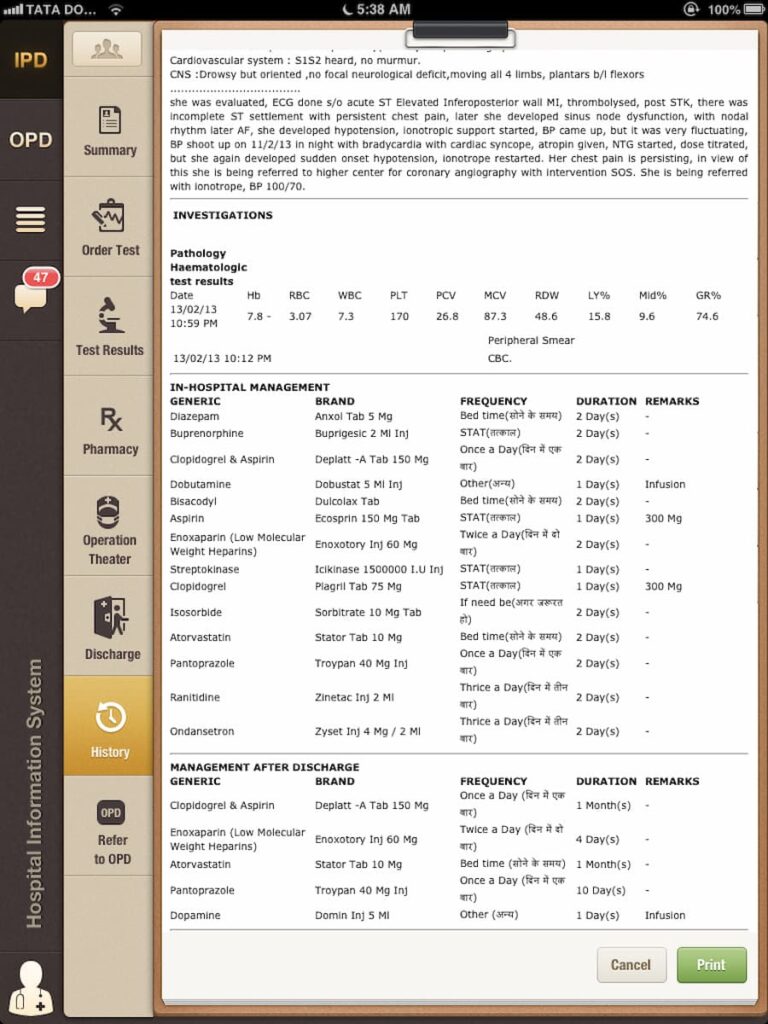
I still remember the distinct professional thrill of seeing radiology images on an iPad for the first time. The CT and MRI scans appeared with a clarity that felt almost indulgent; we could scroll, zoom, and review complex anatomy without having to huddle around a single shared desktop in a crowded nursing station. Even routine lab values began to look smarter, as blood glucose and creatinine transformed from scattered numbers into coherent graphs. Trends became visible, and consequently, decisions became quicker.
The app also allowed doctors to place orders electronically—tests, medications, procedures—without the inefficiency of running back and forth between wards and terminals. The interface was clean, responsive, and surprisingly intuitive. For the first time, our HIS felt less like a passive record-keeping tool and more like an active clinical partner.
Once the iPads arrived, they didn't just sit in boxes; they went into the pockets of our residents, and the change in culture was immediate. The old habit of "I’ll check and get back to you" began to wither. Instead of chasing paper slips through corridors, doctors stayed at the bedside because the data followed the doctor, not the other way around. Information, once trapped in the heat and hum of a computer room, was suddenly portable, living in corridors and on call-duty. It was no longer a static record; it was alive.
I recall a specific morning in the OPD when I showed a patient his blood glucose trends on the iPad screen. In our villages, people often speak with their eyes rather than their tongues. He didn't say much, but as he looked at the graph, I saw a shift in his understanding. He wasn't looking at a mysterious medical verdict; he was looking at his own life mapped out in front of him, finally understanding why the medicine mattered.
Demonstrating the iPad interface in the Sevagram OPD, 2013
I couldn’t help but marvel that a device often dismissed as a luxury toy was behaving as a powerful instrument of change in a rural ward. It was not just a repository of data; it was an instrument of engagement.
Encouraged by the success of the iPad application, the hospital administration decided to expand the ecosystem significantly. In September 2012, we distributed 100 iPads and MacBooks to residents and faculty, adding to the 300 laptops that had been issued in previous years. It was a significant institutional decision, especially for a public teaching hospital, signaling that technology was no longer a side project—it had become infrastructure.
Two major upgrades strengthened the system further: the installation of PACS and the Radiology Information System, coupled with the arrival of campus-wide Wi-Fi. Together, these tools improved imaging workflows, mobility, and access to patient data, ensuring the hospital moved faster and made fewer decisions in the dark. In a small way, this is what we had wanted from the beginning—not computers for their own sake, but information that reached the bedside on time. That, after all, is where it belongs.
Sourcebits was founded in 2006 by Dr. Rohit Singal, a radiologist who traded X-rays for code and rode the early wave of the iPhone ecosystem to build one of India's more interesting technology companies. In 2014, Sourcebits was acquired by Globo, a UK-based firm. Dr. Singal subsequently moved to the United States, shifting his attention to gaming startups and angel investing in Silicon Valley — a trajectory that says something about where ambition leads when the first frontier has been conquered.
Amit Pandey, who was the backbone of our project at Sourcebits, left to found Synclovis, a company focusing on mobile and web solutions that he continues to lead today. Farzan Siddiqui, the software engineer who worked with quiet persistence through nine months of Webex calls and server glitches, deserves more credit than project footnotes usually allow.
Twenty Years of HIS
By now, I am the last person who can claim to be “neutral” about our Hospital Information System. I lived with it for two decades—sometimes like a proud parent, sometimes like an exhausted mechanic. Still, if I step back and look at it the way a visiting outsider might, a simple question comes to mind: Did we actually build something useful, or did we merely replace paper with screens?
In April 2009, the New England Journal of Medicine published a survey on health information technology in American hospitals. Its opening line stayed with me: less than 2% of acute care hospitals had a comprehensive electronic records system, and only 8–12% had even a basic one. When I first read that, I smiled—partly in disbelief, partly in relief. If wealthy hospitals in the United States were struggling, what were we trying to do in Sevagram, a village that often didn’t have stable electricity for half the day? No reliable internet. No smartphones. Not even the habit of using a mouse. And yet, we had decided to digitise a 1,000-bed teaching hospital as if it was the most natural thing to do.
We began in 2004, not with grand promises, but with a practical irritation: paper was failing us. Handwritten notes went missing. Files grew fat and unreadable. Lab reports got tucked into the wrong folder. Discharge cards looked like they had survived a cyclone. With nearly 50,000 admissions a year, the system was cracking under its own weight. We needed something that could hold information without tearing, fading, or walking away in someone’s pocket.
***
The first visible change was not dramatic. It was almost boring—registration became faster, test orders became cleaner, reports became retrievable. But in a hospital, “boring” is a compliment. Automation took over the repetitive work: registering patients, printing slips, generating reports, tracking bills, and sending information across departments without a messenger boy sprinting down corridors. Slowly, the hospital began to breathe a little easier.
The discharge summary, in particular, changed shape. Earlier, it was a daily embarrassment. Residents wrote them in haste, handwriting collapsed into hieroglyphics, and crucial details slipped through the cracks. With HIS, the patient’s demographic details pulled in automatically. Investigations came in neatly—date-wise and lab-wise. Operation notes and in-hospital medications got recorded without anyone having to “remember” them later. The resident still had to write the clinical story, but the skeleton was ready. For the first time, discharge summaries looked like something you could actually read without a magnifying glass and a prayer.
The pharmacy felt the impact even more. Every day, about 1,500 patients queued up for medicines. In the old days, a crowded counter and a hurried handwriting were an invitation to error. HIS didn’t eliminate mistakes—nothing does—but it reduced the chaos. Billing became cleaner. Stock tracking became smarter. Pharmacists spent less time deciphering prescriptions and more time dispensing safely. That, to me, was progress.
***
This is the part where I must resist the temptation to sound triumphant. Did electronic records improve clinical decisions? Did they reduce complications? Did patients live longer because of our software?
I don’t know. And I cannot pretend I do.
We never ran a proper before-and-after evaluation. We didn’t measure errors systematically. We didn’t compare outcomes across years. Like many hospitals, we were so busy building the system that we forgot to study the system. If I were advising my younger self today, I would say: Do the research while you do the work.
What I can say, with honesty, is simpler. The hospital ran more smoothly. Information became easier to find. The number of “missing” things—files, reports, bills—reduced. And when you reduce friction in a hospital, you reduce suffering, even if you cannot calculate it neatly in percentages.
***
One day, much later, I saw residents doing rounds with iPads. Radiology images looked startlingly clear. Blood sugars and creatinine values appeared as graphs instead of scattered numbers. Orders could be placed without running back to a desktop computer like a schoolboy sent on errands. That sight gave me a quiet happiness—not because it looked modern, but because it looked useful. The screen was finally at the bedside, where it belonged.
***
If technology was the engine, adoption was the fuel. And fuel doesn’t come easily in a hierarchical hospital.
Many senior doctors trained in the 1960s and 70s disliked the idea of a computer between them and the patient. Some felt data entry was beneath them. Some worried it would slow them down. Others simply didn’t trust a system that had been designed outside Sevagram. A few saw it as an administrative obsession, not a clinical need.
So we took a “bottom-up” route. We leaned on residents, clerks, pharmacists, technicians—the people who actually carried the hospital on their shoulders. We sought the passive support of department heads. We tolerated the year of double work—paper plus digital—because that was the only way to build confidence. There were days when the server crawled, transactions failed, and the hospital staff looked at us as if we had personally invented suffering. We absorbed complaints, fixed what we could, and returned the next morning to try again.
The gap between engineers and doctors is real. At times it felt like two different alphabets trying to form one sentence. But over time, we learned each other’s language—slowly, clumsily, and with plenty of irritation. What kept it alive was not brilliance. It was persistence.
***
Even today, I can list what we lack without hesitation.
We never built strong clinical decision support into the system. Drug–drug interactions and allergy alerts didn’t become routine in critical areas. Vital signs were not captured reliably across all wards. Problem lists and active medication lists remained incomplete. Some departments stayed stubbornly paper-based. CPOE excited a few units but failed to capture the whole hospital’s imagination. Patients still didn’t have easy electronic access to their own records. Data privacy and security needed deeper attention. And in many ways, we digitised old workflows instead of redesigning them.
In other words, we improved the container, but we didn’t always improve the contents.
***
When I think of those years, I often remember the old Hindi film Chalti Ka Naam Gaadi—a story held together by family, humour, breakdowns, and stubborn forward movement. HIS also became like that. We didn’t work on it only in office hours. It entered our dinner conversations. It sat beside us like a silent guest. Bhavana, Ashwini, and later Shaily were part of that long, unglamorous labour.
But this was never a “family achievement.” The real credit belongs to the people who kept showing up: the pharmacists who learned computers despite fear, the technicians who entered results patiently, the clerks who corrected errors without drama, the residents who used the system even when it slowed them down, and the engineers who tolerated our endless demands and clinical tantrums. The system worked because it became everyone’s system.
We rarely celebrated milestones. We just moved from one problem to the next, like doctors on night duty. Perhaps that is why, even now, the most satisfying part of this story is not the technology itself. It is the memory of a hospital learning—slowly, awkwardly, and with a lot of resistance—to trust a new way of working.
And every time our car approaches that blind turn near the railway underpass between Sevagram and Pavnar, my granddaughters shout, “Baaju!”—making way, making noise, making us laugh. The hospital, too, learned to make way. From paper to pixels, it kept moving.
The Reluctant Administrator
In September 2009, the trajectory of my career shifted without warning. I was a Professor of Medicine, content in my familiar world of wards, rounds, students, and research, when a letter arrived from Dr. (Mrs.) P. Narang, Secretary of the Kasturba Health Society. It was brief, formal, and decisive. I had been appointed Medical Superintendent of Kasturba Hospital.
I read it twice, as if a second reading might change the meaning. It did not. I felt two things at once — apprehension, and a faint, helpless amusement. The management had sanctioned a special allowance of ₹500 per month for the post. Even in 2009, it was a token amount, almost ceremonial. I smiled for a moment. Then the smile vanished. The sum felt inversely proportional to the headaches the job would bring.
The vacancy had opened because of a regulatory technicality — the kind that looks harmless on paper but rearranges lives. Dr. K.R. Patond, our Orthopaedic Surgeon, had been running the hospital with calm efficiency. But the Maharashtra University of Health Sciences enforced a strict rule: one person could not hold two administrative positions simultaneously. Dr. Patond had to choose between being Head of Orthopaedics and Medical Superintendent. He chose his department — understandably — and the superintendency landed, with quiet inevitability, on my table.
I had not applied for the post. I had not lobbied for it. In truth, I had spent most of my career avoiding it.
My hesitation was not only about workload. It was about legacy.
To sit in the Medical Superintendent's chair in Sevagram was to step into a long shadow. Kasturba Hospital had been run by men whose names were spoken with a particular kind of respect in corridors and committee rooms: Dr. P. Nayar, Dr. Karunakar Trivedi, Dr. O.P. Gupta, Dr. R. Narang, Dr. V.N. Chaturvedi, Dr. A.P. Jain, Dr. S. Chhabra, Dr. K.R. Patond. They were administrators of a different era — firm, authoritative, and entirely comfortable with power. They could still a room with a glance. They could resolve a crisis with one sentence.
I was not cut from that cloth. I was a physician who preferred the bedside to the boardroom, the patient's story to the committee's agenda. I had always believed that the best decisions in medicine are made close to the patient — where breathlessness can be seen, not merely described; where pain is not a complaint but a face.
I had done nothing to prepare for this role. I had not enrolled in any of the hospital administration courses that some doctors pursue, and occasionally mention on social media. I had no idea what I was getting into. Honestly, I am not sure I wanted to know.
Consider what I knew of Medical Superintendents before I became one. Back in the 1970s, when I was a registrar in Medicine at GMC Nagpur, I had only the vaguest sense of who ran that hospital. We walked past his office almost every day — it sat beside the Indian Coffee House, where we gathered before ward rounds or after — and I cannot recall a single occasion when I had reason to go in. The Medical Superintendent was a creature who existed, presumably, behind a closed door. We did not need him. He did not need us. The arrangement suited everyone.
Sevagram was different. Dr. Karunakar Trivedi had, through force of personality and institutional will, made the Medical Superintendent's office as consequential as the Dean's. That tradition held. In Sevagram, the post carried real weight — a fact that surprised me further when I later discovered the position had no formal standing in the university's own statutes. It was, in effect, an office that derived its authority entirely from the person who occupied it. Some found that liberating. I found it unsettling.
Administration, to me, was a foreign country: files, permissions, budgets, politics, and meetings that began late and ended later. It was not that I looked down on it. I simply knew I did not belong there — the way a man who has spent forty years reading fiction knows, without embarrassment, that he cannot write a balance sheet.
I accepted the chair. I never quite got comfortable in it.
The letter gave me little time. In Sevagram, decisions like this are rarely made slowly. The hospital runs on urgency; even leadership changes must not interrupt the rhythm of admissions, deliveries, emergencies, and ICU alarms.
In that narrow window, I did what many people do when they are unsure: I called someone who would tell me the truth without softening it. I rang Dr. Rajnish Joshi, a close colleague whose intelligence I trusted and whose humour I had learned to respect.
He listened quietly. Then he said, "My condolences."
I laughed, because it was funny. I also laughed because it was accurate.
Rajnish assumed — perhaps correctly — that a man shaped by academic medicine would not survive the friction of administration. I assumed the same. In my mind, I would do my duty for a few months, endure the chaos, make some improvements if I could, and retreat gratefully to my ward rounds and postgraduate teaching.
I could not have been more wrong. I remained in that chair for twelve years.
I learned early that the Medical Superintendent's job in a teaching hospital is a paradox dressed as a title.
You are expected to lead, yet you are constantly negotiating. You must speak for the faculty, the residents, the nurses, the technicians, the clerks, the patients — and remain answerable to the Society, the Board, the auditors, and the budget. In one hour you might be discussing ventilators and ICU mortality. In the next you might be arguing about a broken autoclave, missing linen, or a water tank that refuses to fill. A superintendent must be a visionary one moment and a plumber the next.
Unlike the President of the United States, who is granted the luxury of a first hundred days, a Medical Superintendent gets no honeymoon period. The judgment begins on day one, often before you have learned where the keys are kept. The emergency does not wait. The OPD does not shrink. The wards do not become quieter out of sympathy.
Success in administration is a peculiar thing. In clinical medicine, you can measure improvement — blood pressure, oxygen saturation, fever chart, appetite, sleep. In administration, you measure success by the absence of catastrophe. The day goes well if nothing collapses. It is like financial planning: wealth is built not by spectacular gains but by avoiding ruinous losses. In a hospital, you are constantly trying to prevent the one mistake that can undo years of goodwill.
Once I accepted the role, reluctance could not be my personality. If I was going to sit in that chair, I needed to set a tone — at least for myself. I did not want to become a caretaker who signed files and attended meetings. I wanted the post to remain anchored to what mattered most: patients.
On September 4, 2009, I wrote to Mr. Dhirubhai Mehta, President of the Kasturba Health Society. It was not a formal acceptance letter. It was closer to a manifesto.
From: Dr. S.P. Kalantri
To: Mr. Dhirubhai Mehta
Subject: On taking charge
Date: September 4, 2009
Dear Dhirubhai,
May I thank you for the wonderful letter you wrote asking me to look after our hospital.
Managing a hospital is a challenging task. It gives one a unique opportunity to introduce changes that could positively influence the way health professionals function. Incidentally, the word "hospital" comes from an old French root which originally meant shelter for the needy. Curiously, the words hospital, hostel, hotel, and hospice owe their origin to the same root — each indicating a place that offers succour.
And yet, if public perception is anything to go by, given a choice, nobody likes to stay — let alone visit — a hospital. Hospitals evoke pain, stress, fear, uncertainty, and insecurity. A good hospital is one which responds not only to the explicit concerns of patients, but also to the unvoiced ones, and tries to make their visit a little more pleasant.
Today's New York Times reports that Johns Hopkins Hospital was ranked as the best hospital in the US because it received the highest scores for quality and efficiency. Of the 100 hospitals judged, compared with the poorest performers, the best-performing quintile had 25% lower death rates, 19% fewer medical complications, and 13% fewer patient safety incidents — even though their patients were sicker and their average hospital stays were significantly shorter.
Not an easy task to achieve these standards in our setting. But that should not deter us from trying. I am on a learning curve right now and hope to learn quickly the tips and tricks that good managers use to make hospitals more professional and patient-friendly.
With regards,
SP
When I read that email now, years later, I can see my nervousness hiding behind formality. I can also see something else: a stubborn hope. I was telling Dhirubhai — and perhaps telling myself — that even in a rural hospital with limited resources, we could still aim for quality, dignity, and trust.
I did not know then how many times that hope would be tested.
What I did know — and what I have never forgotten — is a passage from Vinod Mehta's memoir, Editor Unplugged. He wrote that as long as you do not let success go to your head, as long as vanity is kept in check, as long as you treat fame as an impostor and remember that those who applaud your fluency will not recall a word of it five minutes after the television programme ends — you will retain your sanity.
I kept that close.
And I was helped, more than I can say, by Bhavana. Whenever she sensed that I was growing proud of the post — the chair, the title, the small privileges that come with it — she would quietly, firmly, cut me to size. No speeches. No arguments. Just a look, or a word, that brought me back to the ground. It is an occupational hazard of anyone who occupies a position of institutional authority: the gradual, almost invisible inflation of the self. Bhavana was my corrective. She still is.
The chair was mine. The hospital was waiting. And I had, by some fortunate accident of marriage, exactly the right person to keep me honest.
The Colossus of Prena Kutir
Although I joined MGIMS in the summer of 1982 and Dr. Sushila Nayar remained the Director until her death in January 2001, our paths rarely crossed in any formal sense. For those two decades, I had almost no interaction with her. I do not recall ever meeting her face-to-face in her office. To the world, she was a colossus: Mahatma Gandhi’s personal physician, a freedom fighter, a former Union Health Minister, and the builder of institutions. To us in Sevagram, she was “Badi Behenji”—a name that carried affection, reverence, and a quiet warning.
She was the institution’s conscience and its compass. She had a rare presence that did not require a microphone; she could walk into a ward and make everyone straighten their backs without saying a syllable. She was fiercely pro-poor, allergic to pretense, and possessed a famous, purposeful temper that she used like a surgical instrument against laziness. Many of us found her difficult in our younger years, but we eventually realized she was difficult for the same reason a good teacher is: she refused to let us remain mediocre.
***
My limited personal interactions with her occurred only in the final decade of her life, when her heart began to falter. Dr. A.P. Jain, her physician, looked after her with a devotion that saw him visiting her residence, Prena Kutir, every single day for ten years. Prena Kutir was a small, modest, one-bedroom dwelling—frugal and austere, reflecting the Gandhian simplicity she lived by. Day after day, year after year, Dr. Jain would go there to record her blood pressure and exchange pleasantries. Whenever he was on leave, he would ask me to cover for him.
I might have gone no more than a dozen times. Even as a faculty member, I was shy and in awe of her, hardly daring to speak. By contrast, she was an unnervingly warm host. She would welcome me as "Doctor Saab," despite being four decades my senior. She would generously extend her arm for the sphygmomanometer—those were the days before digital instruments—and keep her eyes fixed on the rising mercury column. Then, with a polite smile, she would ask, "Theek Hai?" (Is it okay?)
If I told her the reading was high, she would laugh heartily and offer a human excuse: "I didn't sleep well," or "I am constipated," or jokingly, "These days, even the blood pressure does not listen to me!"
***
As a perfect host, she would insist I sit. She would take slices of bread, smear them with butter, sprinkle them with salt, and command me to eat. "Don't look at the butter," she would say, "and don't be afraid of heart disease!" During the summers, she would slice fresh mangoes and arrange them on a plate with motherly care.
When it was time to leave, she would insist on escorting me to the door, regardless of my protests. She would stand there, thanking me profusely, and wait until I had kicked my scooter to life and sped past her residence. In those moments, I never saw the administrator, the former Member of Parliament, or the woman who had stood beside Gandhi from the late 1930s until his end. I only saw a woman of immense kindness.
***
In her later years, I began writing "Sevagram Stories," attempting to chronicle how MGIMS was conceived and how Behenji had drawn the best minds from Delhi, Chandigarh, and Nagpur to this rural outpost. To my frustration, there was no written record of this history. I had to rely on the fading memories of the elders still among us: Mr. P.L. Tapdiya, the current President who had been here since 1968; teachers like the Narangs, Dr. O.P. Gupta, A.P. Jain, Karunakar Trivedi, Dr. Ingely, Dr. Chhabra and Dr. Ulhas Jajoo.
Behenji had compiled the unfinished work of her brother, Pyarelal, on Gandhi’s biography, but she never dictated her own memoirs. A few months ago, I met Prabha Desikan (MGIMS Class of 1984) and lamented this void. I told her how much I wished I had gone to Behenji and requested her to tell me the stories while I sat at her feet and documented them. I never did, for two reasons: the thought never occurred to me then, and even if it had, I was too introverted—too afraid of her aura.
I watched other professors go daily for tea, to play cards, or to recite the Hanuman Chalisa or Sundar Kand with her. I never did that. Today, I wish I had shed my inhibitions and possessed that "Punjabi boldness." I should have looked her in the eye and, like a journalist, extracted those pearls of history. I blame myself for that silence.
***
There is one memory that still stings—a testament to my own social awkwardness. In February 1984, I got married. I desperately wanted to invite Behenji to the reception at Jaishree Bhavan, but I couldn't muster the courage to face her. I walked to her doorstep once or twice and retreated. Finally, I committed a grave social blunder: I asked the Medicine OPD attendant, Ramu Chavan, to hand her the invitation card.
For a woman of her stature—a Punjabi, a politician, and the head of the institute—to receive a wedding card from a faculty member via a hospital orderly was unthinkable. Predictably, she did not attend, nor did she write a letter. After the wedding, I failed to take my wife, Bhavana, to seek her blessings—a routine campus tradition. My shyness must have appeared to her as the rudeness of a mannerless lecturer who lacked social grace. I could not help it then; I can only regret it now.
***
The clock turned full circle in 2001. Six months after she passed away, Mr. Dhirubhai Mehta asked me to compile and edit a commemorative book on her: Bapu ki Beti, Hamari Beti. I spent days and nights with Prabha Desikan, collecting old photographs and inviting people to write their tributes.
This was my delayed homage. It was the respect I should have paid her while she was still with us. When she died, Sevagram felt as if it had lost its protective roof. The OPDs continued and the ward rounds happened, but a certain gravity disappeared. We realized then that the hospital could no longer rely on one towering personality to keep it aligned.
Modern administrators love their charts and their "systems." Behenji had no use for them. Her system was a mixture of Gandhian discipline and a fierce, often terrifying, personal loyalty to the poor. She wasn't an "administrator" in the corporate sense; she was a guardian. And like any guardian of a large, unruly family, she kept us in line not through files, but through the sheer impossibility of saying 'no' to her.
Dhirubhai Mehta
After the iron discipline of Dr. Sushila Nayar came the warm, chaotic heartbeat of Mr. Dhirubhai Mehta. If Behenji was the soul of MGIMS—severe, principled, and formidable—Dhirubhai was its life force. A Chartered Accountant by training, he understood finance the way a tabla player understands rhythm: not by calculation alone, but by a deep, percussive instinct. He walked away from the high-stakes corporate corridors of Bajaj Auto and stepped into the dust of Sevagram, trading Mumbai’s polish for the daily, unglamorous mess of a rural hospital. He brought with him a Mumbaikar’s quick wit, a Gujarati’s unapologetic love for food, and an administrator’s rarest gift—the ability to trust a person’s character before trusting their paperwork.
When he first arrived in 1982, he never bothered with the stiff stereotype of a hospital president. He would laugh at his own lack of medical vocabulary, joking that he couldn’t spell half the departments he was supposed to run. Yet he possessed a Nehruvian eye for talent; he drew academic giants like Manu Kothari, Ashok Vaidya, B. S. Chaubey, and G. M. Taori into our orbit, lending intellectual weight to an institution that city-dwellers often dismissed as peripheral.
***
Tea at Six and Decisions by Seven
Our relationship did not begin in a boardroom or across a mahogany desk. It began in my home in Vivekanand Colony at six in the morning. He would walk in unannounced and unpretentious, asking after Bhavana and the children before moving seamlessly into hospital matters as if the two belonged to the same breath. To Dhirubhai, the institute was not a "system" to be managed, but a family enterprise to be nurtured.
He possessed a profound distrust for thick files and an almost mystical reliance on gut feelings. "Don’t confuse me with data," he would say, a mischievous glint in his eye as he waved away a bundle of statistics. "I’ve already made up my mind." It wasn't that he lacked rigor; it was that he believed hesitation in a hospital was a form of cruelty. He preferred to make a decision at speed, own it fully, and deal with the consequences later. It was this very instinct that shaped my own career, for it was under his watch that I became the "Reluctant Medical Superintendent." He found my total lack of ambition an amusing oddity in a world where titles are chased with the fervor of religious pilgrims.
***
The 7 O’Clock Darbar
Dhirubhai’s true genius was his accessibility. Every evening, his office transformed into what we called the "7 O’clock Darbar." It was a daily open court where the hierarchy of the hospital dissolved. Anyone could walk in: a senior surgeon, a junior resident, a clerk from accounts, or a ward attendant. Ideas, complaints, and gossip flowed in a single stream, and quite often, solutions emerged with stunning speed.
A single phone call from that room could unlock fifty lakhs for a new ICU or a palliative care ward. He did not always demand elaborate proposals; he gambled on men rather than systems. While that trust carried risks, the results were visible in the brick and mortar of an expanding MGIMS. Under his leadership, we took ethical stands that were inconvenient and unpopular—unlinking academic activities from pharmaceutical sponsorship and banning medical representatives from campus. He pushed us into the malnourished heartland of Melghat, visiting remote centers not for a photograph, but to remind us, and perhaps himself, why Sevagram existed.
***
The "I" Specialist and the Dhokla Diplomacy
Dhirubhai was never a saint carved in marble. He was wonderfully, maddeningly human. He had a predictable weakness for flattery and suffered from what we affectionately called the "I, Me, and Myself Syndrome." We joked that he was an "I Specialist" because of his penchant for name-dropping ministers and governors as if he were reciting a grocery list. He enjoyed being the sun around which the room orbited.
His love for food was equally legendary. Faculty members learned quickly that the most efficient route to a new grant ran through a home-cooked Gujarati breakfast. He could discuss a multi-crore budget with a straight face while keeping a predatory eye on the last piece of dhokla. Yet, beneath the showmanship was a deep sincerity; he wasn't performing kindness, he was living it.
***
The Slow Fading and the Last Call
Time, however, eventually begins to edit the most vibrant of men. As the years passed, the sharp accountant’s mind began to soften. His memory faltered, and the decisiveness that once defined him became a wandering narrative. He would sit for long hours in his office, drifting into anecdotes, unable to reach the conclusions that once came in a heartbeat. It was a painful transformation to witness—not because he was weak, but because he was a builder who could not bear to step away from what he had built.
Every day in Sevagram, he would stand before the idol of Goddess Durga for fifteen minutes, head bowed in unhurried surrender. "I owe everything to Amba Mata," he would say. It was a startling contrast—the man who commanded destiny in the boardroom bowing like a child in the temple. He knew that institutions survive on grace as much as they do on intelligence.
On April 22, 2022, Dhirubhai passed away at Bombay Hospital. Even on his deathbed, surrounded by city specialists, he bypassed them all to call me. "Is the treatment right?" he whispered. It was the quintessential Dhirubhai question—half anxious, half practical, and entirely human. When the news reached Sevagram, the sky felt a little lower. I had not just lost a President; I had lost a father figure who taught me that sometimes, you don’t need a file to make a decision. You only need a heart, a gut feeling—and a good cup of tea.
The Custodian of the Ledger
When Dhirubhai Mehta passed away, a heavy hush settled over Sevagram. For nearly a quarter of a century, his voice — booming, teasing, impulsively decisive — had been the soundtrack of the administrative corridors. Suddenly that rhythm was gone. The institute needed a hand that could steady the ship without requiring a spectacle. The mantle fell, almost by gravitational pull, on Mr. Parmanand Tapdiya.
To the casual observer, Tapdiya is the quintessential Chartered Accountant who climbed the Kasturba Health Society ladder the old-fashioned way: rung by rung, from member to trustee, to Vice-President, and finally President. A man of numbers, meticulous, cautious, and deliberate. That description is accurate as far as it goes. It does not go far enough.
***
The Man Who Called My Father Mamaji
To me, the professional title is secondary to a much older, more personal history. He is the man who called my father Mamaji. That single word contains half a century of shared struggle and unspoken debt. Our bond was not forged in committee rooms or over boardroom minutes. It was built on a foundation of gratitude that has remained unshaken since the days when my father mentored him.
In a world where people repay debts with flowery speeches, Tapdiya chose the harder currency of constancy. Since 1986, he has filed my income tax returns every single year — quietly, efficiently, and with a stubborn refusal to accept a single paisa. It is a small act on paper. In the context of a life, it is not small at all. Whether it was my daughter's wedding or my departure for Berkeley, he was always somewhere in the background — not demanding the spotlight, but ensuring the stage did not collapse. In Sevagram, such loyalty is rarer than brilliance. Brilliance merely shines. Loyalty sustains.
***
What a CA Brings to a Hospital
I have worked in medicine long enough to know that the most dangerous threat to a public hospital is rarely clinical. It is financial. A missed payment stalls a project. A delayed tender creates a drug shortage. A casual signature triggers an audit query that haunts an institution for years. The hospital that runs out of money cannot run at all — no matter how skilled its surgeons or how dedicated its nurses.
This is where Tapdiya's particular discipline matters. He treats institutional finances the way a good clinician treats a patient: with close attention, early intervention, and a healthy suspicion of assumptions. Under his watch, the accounts are not merely kept — they are interrogated. He understands that in a thousand-bed teaching hospital serving one of the poorest districts in Maharashtra, the difference between a balanced ledger and a deficit is often the difference between a ward that functions and a ward that does not.
He moved beyond the balance sheets during Dhirubhai's fading years, taking on the gritty labour of construction oversight, procurement, and the endless negotiations required to keep a large institution from stalling. These are unglamorous tasks. They require patience, attention to detail, and the willingness to sit through meetings that produce nothing visible. Tapdiya does them without complaint and without credit.
His approach to financial management reflects a principle I have come to believe deeply: that a pro-poor institution must also be a financially disciplined one. Generosity without solvency is not generosity — it is a postponed crisis. The poor patients who walk miles to reach Kasturba Hospital are not served by noble intentions. They are served by a hospital that has oxygen in its cylinders, drugs in its pharmacy, and staff who have been paid on time.
***
Discipline in the Time of AIIMS
Tapdiya has inherited a storm that would have exhausted his predecessors. The loss of institutional autonomy after NEET and the disappearance of the staff quota have fundamentally altered the Gandhian DNA of our admissions. Simultaneously, the shadow of AIIMS Nagpur — less than an hour away — has changed the local medical map forever. Faculty retention has become a battle. The new generation of doctors often prioritises urban postings and specialisation over the slow, patient art of rural bedside medicine.
His leadership style is a deliberate departure from the giants who preceded him. Dr. Sushila Nayar led with a terrifying moral authority. Dhirubhai led with a Mumbaikar's instinct and theatrical generosity. Tapdiya leads with dry methodical discipline. He does not trade in slogans or poetry. He calls a spade a spade, sometimes with a bluntness that can feel abrasive to those accustomed to softer diplomacy.
In a storm, however, you do not need a poet. You need a firm hand on the tiller.
***
The Mike Brearley of Sevagram
The question whispered in the corridors is whether a man of numbers can steer an institution of ideals. I find myself leaning toward optimism.
Tapdiya reminds me of Mike Brearley — the England cricket captain who was not the most flamboyant batsman but who read the game with a clinical intelligence that transformed an ordinary side into a formidable one. His value was never in the scorebook. It was in the dressing room, in the field placements, in the quiet conversation with a bowler who had lost his rhythm. MGIMS does not need theatrics right now. It needs clarity, financial prudence, and the discipline to remain pro-poor without becoming professionally obsolete.
Watching him lead feels less like a corporate succession and more like the next page of a family chronicle — written in quieter ink, but with a remarkably steady hand.
The balance sheet of Sevagram, for the moment, rests in safe custody.
Three Rooms, One Hospital
During my tenure as Medical Superintendent, I worked out of three different offices. Each one marked a distinct phase of my administrative life—almost like three addresses for the same responsibility.
I began in September 2009 in the original MS Office in the old hospital building, and stayed there until 2015. From March 2015 to November 2020, we functioned out of a temporary space in the Medicine Department building. Finally, in December 2020, we moved into a newly constructed MS Office—ironically, a space that had served as the hospital library for more than four decades.
Over these years, I worked closely with three office heads—Mrs. Vinaya Dabir, Mr. Dave, and Mr. Girish Dev—and three matrons—Pushpa Biswas, Aruna Janaikar, and Neeta Shetye. Together, they formed the administrative spine of the hospital. In a teaching hospital, the MS may sit in the chair, but the office runs on teamwork, memory, and quiet coordination.
The responsibilities were vast and never neatly boxed. The MS Office oversaw outpatient departments, wards, ICUs, ICCU, the cath lab, dialysis unit, emergency services, registration OPD, health insurance schemes (including MJPJAY), the hospital information system, medical records, linen and laundry services, kitchen, medical store, CSSD, and radiology. Kasturba Hospital functioned like a living organism—busy, noisy, relentless. Every day, nearly 2,500 outpatients walked through its doors, around 125 patients were admitted, about 15 babies were delivered, roughly 30 major surgeries were performed, and close to 1,500 prescriptions were written or refilled. Even on “quiet” days, the hospital did not truly slow down.
Over time, the hospital’s catchment area also changed. Most patients now came from Wardha district. Earlier, nearly a fifth had travelled from Telangana. The emergence of another medical college in the district, the government’s policy of opening medical colleges in every district, and the growth of private and public healthcare facilities in the region inevitably diluted MGIMS’s earlier dominance. The hospital remained busy, but the geography of its patients slowly shifted.
Being equally comfortable in Hindi, Marathi, and English helped me enormously. In administration, language is not just a tool of communication—it is often the difference between authority and accessibility. It helped me speak to staff and patients, attendants and journalists, clerks and senior administrators, without sounding distant or performative.
***
The original MS Office sat behind the Radiology Department in the old hospital building. It was a sprawling space—two large halls connected to a maze of small rooms, always bustling with clerks and administrative staff. The moment one walked in, the place felt alive. I spent most of my time in the first hall, which had an old table, a chair, a sofa, and walls lined with trophies and photographs. I liked the hum of activity around me. I also enjoyed typing, and I preferred working there, in the middle of the noise, rather than in a silent cabin that made me feel detached from the hospital’s pulse.
In 2015, space constraints forced us to shift to the Medicine Department building. My room there served a dual purpose—it became both my departmental office and the MS Office. The administrative officer, matron, and public relations officer occupied adjoining cabins, while the clerks squeezed into a small shared cubicle. It was far from ideal, but hospitals are experts at improvisation. We adjusted, and we made it work. That arrangement lasted five long years.
In December 2020, we finally moved into a permanent MS Office, created by repurposing the old hospital library. The irony was not lost on me. For decades, that room had been a sanctuary for students—a quiet place of books, notes, and late-night study. Now it would become the nerve centre of hospital administration, where the day’s crises arrived in files instead of textbooks.
***
When I took charge, Mrs. Vinaya Dabir was the administrative officer. She retired on 28 February 2014 and was succeeded by Mr. Girish Dev, who had joined a month earlier. His family had migrated from Guntur to Betul nearly a century ago, and their surname had evolved from Devraya to Deo. Before joining MGIMS, he had worked at M–Two–S, an academic institute in Nagpur. Mr. Dave was also part of our team for about a year, before he resigned voluntarily in May 2014.
Our office staff included Kuljeet Singh, the stenographer, who sadly passed away in 2019; senior clerks Jyotsna Chaturvedi and Ganesh Trivedi; Mahendra Chaudhary, the computer operator; and clerks Maya Kakade, Mahadev Pisudde, Vijay Pattewar, and Om Pariyal. Chandrakant Wadhekar managed the linen section, while attendants such as Laxman Bele, Rama Jagtap, Dilip Ambulkar, Maruti Ghonge, and Mangesh Jamunkar kept the office running smoothly, often unnoticed. Hospitals celebrate consultants, but they survive on people whose names rarely appear in speeches.
Mrs. Parihar served as Public Relations Officer until 2012. Tireless and principled, she played a crucial role in resisting the influence of the pharmaceutical industry on prescriptions and in shielding the institution from unethical practices. Her contribution during the 2011 NAAC inspection was pivotal to MGIMS securing an A grade. Though she left in 2012, her imprint on the institution remained long after.
The matrons were the other pillar. Pushpa Biswas served from 2001 to 2010. Aruna Janaikar joined as assistant matron in 2002 and continued until retirement. In December 2015, Neeta Shetye replaced her. With an M.Sc. in Nursing and prior experience at Kasturba Nursing College, she was a natural leader and a strong candidate for higher administrative responsibility. Assistant matrons Rajani Mishra and Kanchan Wandile provided steady supervision, drawing on their deep familiarity with the hospital and its staff.
And then there was Manish Hazari. Officially, he was an attendant. In reality, he was indispensable. He carried the institutional memory of MGIMS in his head, knew everyone who mattered, and handled every task with cheerful efficiency. We called him “our Man Friday,” and the name stuck—not as a joke, but as recognition.
Our biomedical engineers, Alpesh Raut and Suresh, quietly transformed the way we maintained equipment. By developing in-house expertise, they spared us the burden of expensive annual maintenance contracts and saved the hospital substantial sums. Their work rarely made headlines, but it prevented breakdowns that would have hurt patients.
In the final phase of my tenure, five clerks—Umesh, Nilesh, Priti, Ashish, and Vinod—joined the MS Office, bringing fresh energy to a seasoned team that had already learnt how to function under pressure.
***
I had learned typing at the age of twelve, and by the time I became MS, I could type at about fifty words per minute. Gradually, my home became an extension of my office. Late into the night, I drafted letters and emails, often finishing what the day had left undone. Administration, I discovered, does not end when you leave the building. It follows you home, sits beside you at dinner, and waits quietly on your laptop screen after the house falls asleep.
I made it a habit to leave no files on my desk after 5 p.m. My table was always clean—sometimes deceptively so. Dr. K. V. Desikan once joked that he could never tell whether the MS was working because my desk was invariably bare.
It was meant as a compliment. I took it as one.
The Deans of Sevagram
In four decades at MGIMS, I worked under eleven leaders. Some I admired. Some I merely respected. A few I disagreed with loudly and publicly. All of them, in ways they probably did not intend, shaped the physician and administrator I became. This is not their official record — that exists in the files of the Kasturba Health Society. This is what I remember of them as people: their habits, their contradictions, their moments of grace and occasional failure.
When I arrived in Sevagram in 1982, MGIMS did not yet have a Dean. It had a Principal. The difference was not merely titular.
***
Dr. M.L. Sharma was part of the original contingent from Nagpur that arrived when MGIMS was barely a year old. He joined in 1970, became Vice Principal in the same year, and Principal in 1974 when Dr. I.D. Singh departed. For the next decade, he was the trusted right hand of Dr. Sushila Nayar — attending her card sessions in the evenings, reciting the Sunderkand at her request, and walking with her in the evenings to keep her spirits steady.
He was not merely her administrator. He was her companion in the long project of building an institution from nothing. And he was her confidant — a man who sat close to power for twenty years and never once reached for it. In an institution where proximity to the founder was a currency many coveted, Sharma spent it on none of his own purposes. That, in my experience, is rarer than it sounds.
For twenty years, Sharma was my neighbour in Vivekanand Colony. A deeply religious Marwadi Brahmin, he performed puja every morning and made prasad with his own hands every fortnight — never failing to bring kheer for my family.
One Sunday, my mother was visiting from Wardha. We were talking in the backyard, in Marwadi, when Sharma overheard us from his kitchen window. He rushed out, his large eyes magnified behind thick spectacles. "Kalantri!" he exclaimed. "I thought you were Maharashtrian. But you are a Marwadi! And you speak it so well!" I laughed. "Sir, Marwadi is in my blood. How could I not?" He remained wide-eyed — shocked that he had mistaken a Marwadi for a Maharashtrian for so long.
He lived simply and without apology. Rented quarters all his life, no car, no scooter, no airplane journey. "I've never built a bungalow or boarded a plane," he would say, with a quiet pride that was entirely genuine. "My students are my wealth." In the lecture hall, he was a king — his pharmacology classes punctuated by perfectly timed jokes that students remembered decades later. His office was always open, grievances met with humour and empathy, mischief handled with the lightest possible hand.
He walked always a step behind Dr. Sushila Nayar, arms folded behind his back, matching her deliberate pace. It was not subservience. It was the most eloquent form of respect I have seen in an institution full of people performing respect.
***
In 1983, Dr. Kharak Singh Sachdeva arrived in Sevagram not at the beginning of a career but well past its peak — fifty-eight years old, recently retired as Director of Medical Education and Research for Punjab, and expecting, one imagines, a quiet advisory role as Professor of Physiology. Sevagram had other plans.
Within months of his arrival, the management committee created the post of Dean — a position MGIMS had functioned without for fifteen years. On February 14, 1984, after appearing before a selection board that included Dr. Sushila Nayar and the Director General of Health Services, Sachdeva became the first Dean of MGIMS. He was the only candidate. Whether this was destiny or institutional convenience, I cannot say. Probably both.
He was a striking figure — tall, turbaned, salt-and-pepper beard, eyes large and piercing behind thick glasses. Anyone who entered his office would first meet that unwavering gaze, scanning them from head to toe. Then, in a quiet but firm voice: "Why have you come?" That question alone was enough to unsettle most visitors.
Where Sharma's office had been warm and conversational, Sachdeva's was formal and deliberate. He spoke little, kept his distance, and never indulged in gossip. He walked slowly, always alone, acknowledging those he passed with a graceful nod. Discipline was his religion — khadi was worn on campus, alcohol and non-vegetarian food remained absent, and the Friday all-religion prayer was attended without fail. He sat cross-legged on the floor and listened as Guru Nanak's verses were recited. A request from Dr. Sushila Nayar, in his words, was never a request. It was an order.
It was Sachdeva who made me a Reader in 1986. He signed the papers without ceremony. That was his way.
***
After a brief and troubled tenure by Dr. Prabhakar — marked by favouritism and a mark-sheet scandal that shook institutional confidence — stability returned in 1991 with Dr. J.S. Mathur, a gentle soul from Meerut.
Mathur's most significant administrative contribution was deceptively simple: he introduced double-blind coding to the Pre-Medical Test, removing the scope for manipulation that had existed in the examination system. It sounds technical. In practice, it was a declaration that the institution would be honest about how it selected its students.
He was also, quietly, a leveller. Where previous Deans had taken senior professors to supervise examinations in Nagpur and Delhi — a privilege of rank — Mathur took the juniors. Reddy, Ramji Singh, Deepak Kumar, Tyagi, Mehendale, and me. He treated us with the same courtesy he showed his peers. For those of us accustomed to being managed rather than consulted, it was a small revolution.
It was Mathur who appointed me Incharge of Medical Education at MGIMS in 1992 — a decision that not everyone welcomed. Within a month of my appointment, a senior colleague rose in a faculty meeting and objected sharply, arguing that seniors were being bypassed. I rose in response, gave him what I believed was a fitting reply, and then — in what I can only describe as a moment of dramatic foolishness — resigned the post on the spot. The room fell silent. I stuck to my resignation. I did not take the post back.
Mathur, to his credit, said nothing publicly. He understood, I think, that some battles have to be fought and lost before they can be won differently.
He was my neighbour as well, and taught my children to fold their hands in Namaste when greeting elders. A diabetic who injected insulin three times daily, he had a helpless love of sweets that he never quite conquered — he simply dialled up his insulin before a good dinner and considered the matter settled.
***
Dr. Bhaskar Chenappa Harinath was our first non-medical Dean — a PhD biochemist from a village near Tirupati who had built, over three decades, one of the finest research departments in rural medical education in India. He joined MGIMS in 1970 and spent the next forty years guiding nineteen students through their PhDs, with a focus on filariasis and tuberculosis diagnostics that earned international recognition.
He had spent time at Cincinnati and Philadelphia, and was not reluctant to mention this. "When I was in Cincinnati…" or "As I told John Morris in Philadelphia…" were phrases that punctuated his conversation with a regularity that his colleagues found, depending on their patience, either charming or wearing. He built his department with Telugu-speaking faculty recruited from Sri Venkateswara University, and the cultural distance between his laboratory world and the Punjabi-speaking senior faculty was never entirely bridged. He was, in the end, more comfortable with a research paper than a committee meeting — which is not the worst thing to say of a man in academic medicine.
***
Dr. O.P. Gupta came from Jhansi in 1971, rose through the Department of Medicine, served as Medical Superintendent, and eventually Dean. We worked alongside each other for years without a single disagreement — a record I cannot claim with anyone else in this list.
He was soft-spoken and concise. He never projected authority; he simply exercised it, quietly and without theatre. His most lasting reform was replacing long essay examinations in the Pre-Medical Test with Multiple Choice Questions — a change that introduced objectivity into a system that had previously left too much room for the examiner's preferences. He was not a man who spoke of his contributions. He simply made them and moved on.
His self-effacing quality was genuine, not performed. In an institution full of people carefully managing their reputations, Gupta was the rare administrator who seemed genuinely indifferent to his own. I respected him more than I told him.
***
Dr. P. Narang — who would later write me the letter appointing me Medical Superintendent — was a Microbiology professor of considerable polish and poise. Her father had taught in Dehradun; she had been educated at the Doon School, whose alumni included politicians, industrialists, and senior bureaucrats. Her English was impeccable. Her confidence, even when it did not quite show on her face, was never in doubt.
She had navigated her own early career as a young woman with children in an institution that did not always make that easy. She remembered it. As Dean, she took a quiet but firm position: that a young woman with small children should not be judged by her publication count in her first years of appointment. Let her settle. Let her find her footing. The papers will come. It was not policy. It was decency — and in an institution accustomed to measuring everything, it was not nothing.
She was not a risk-taker administratively, and she knew it. She worked within tradition, avoided radical departures, and maintained a warmth with students and faculty that made her genuinely beloved. In a list of leaders who were often distant or difficult, she was accessible. That is not a small thing in an institution as complex as ours.
***
Dr. K.R. Patond and I go back further than his deanship. At GMC Nagpur, he was an intern in Medicine while I was a resident — a year my junior, learning the ward as I was leaving it. We enjoyed a good relationship then, and that ease survived his elevation.
He was quiet, introverted, and spoke almost exclusively in Marathi — not out of regional pride but out of a conviction that doctors working in rural Maharashtra must communicate in the language of their patients. The result was that faculty from Punjab, Bengal, and Tamil Nadu learned, gradually and sometimes reluctantly, to conduct their conversations with him in Marathi. He was also famously unable to maintain eye contact in conversation — a shyness so pronounced it became, among those who knew him, a kind of affectionate legend.
He had come from a small farming village near Akola, the son of a father who had studied only to the fourth standard. The distance between that village and the Dean's office at MGIMS is not measured in kilometres.
It was a MUHS regulation — that one person could not hold two administrative posts simultaneously — that eventually moved the deanship from Patond to me. He chose his surgical department over the superintendency. The superintendency, as I have described elsewhere in this memoir, landed on my table.
***
The last Dean I worked under was the first I had taught. Nitin Gangane was my student before he was my colleague, and my colleague for many years before he was my Dean. He was born at Kasturba Hospital in 1961 — in the very institution he would one day lead — delivered by a woman who later became Secretary of the Kasturba Health Society. Even his birth, it seems, was plotted by Sevagram.
His father was a freedom fighter from the Hyderabad Liberation Movement who had abandoned his education at sixteen to go underground, eventually settling in Sevagram as a follower of Vinoba Bhave and Baba Amte. The son inherited the stubbornness.
On June 26, 1976 — the first anniversary of the Emergency — a seventeen-year-old Nitin attended a resistance meeting in Wardha. The police raided it. He was arrested and sent to a remand home under the Juvenile Act, where he remained until October 1977, completing his eleventh and twelfth standards while in detention, attending college during the day and returning each night. The Emergency was lifted in March 1977. Nitin stayed in the remand home for six months after it ended, because the wheels of the Juvenile Act grind independently of political events.
That experience produced a man who was constitutionally incapable of accepting authority he considered illegitimate. He was a leftist, an anti-establishment activist, and — on the occasions we disagreed, which were not infrequent — a formidable opponent. During the worst months of Covid-19, our arguments were sharp and sometimes public. But he gave me a free hand to run the hospital, and I gave him the benefit of the doubt when I could.
He became Dean in 2018 after pursuing the position with the same tenacious legal persistence he had applied to everything since the remand home. He was the first MGIMS alumnus to hold the post — leading the institution where his life had literally begun.
We both resigned our administrative posts within a fortnight of each other in January 2022. Neither of us, I think, was entirely sorry.
***
Looking back across four decades, what strikes me is less the variety of administrative styles than the consistency of the underlying challenge: running a complex institution in a resource-scarce setting, keeping it honest, and maintaining its connection to the patients it was built to serve. Some of my Deans did this with warmth, some with discipline, some with quiet stubbornness, and at least one with a combativeness that never entirely left him.
They were my neighbours, my mentors, my occasional adversaries, and — in ways none of us planned — the people who made me whoever it is I became at MGIMS.
The names on the Dean's door change. The spirit of Sevagram, built from rural service and academic rigour and the particular idiosyncrasies of the people drawn to this place, does not.
Playing the MS Innings
As I begin this part of my memoirs—as Medical Superintendent of a busy teaching hospital in central India—I often find myself thinking of the eight superintendents who preceded me. Each brought a distinct temperament to the role. Much like cricketers, no two played the same game.
One was a classic Test player—precise, orthodox, defending his wicket with a straight bat and never taking unnecessary risks. Another was a graceful stroke-maker, soft-spoken, guiding the ball through the covers with effortless timing. One superintendent resembled a patient opener, building an innings the way he built his desk: file by file, ball by ball. Another showed early promise that illness cruelly curtailed, like a career ended too soon by injury. One chose to preserve the status quo, content to block and defend. Another led like a T20 batter, attacking every delivery with speed and force. And one, sadly, spent his days exchanging letters with recalcitrant staff, leaving little behind beyond paperwork—dot balls without momentum.
***
During my residency at Government Medical College, Nagpur, the Medical Superintendent was a distant figure—someone you heard about more than you saw. At MGIMS, however, the MS was a formidable presence, close enough to touch the daily life of the hospital, and powerful enough to change its direction. When I took charge, I knew I would be judged not only by what I did, but by how I did it.
I did not step into the role under intense scrutiny or tight security. Still, I understood how quickly reputations form—and how stubbornly they resist revision. After twenty-seven years at MGIMS, rising from senior resident to professor, I knew my strengths and limitations well. I had to learn fast, decide wisely, and resist the temptation to imitate those who had come before me. I needed to find my own way.
***
Shakespeare wrote in As You Like It that “all the world’s a stage.” Leadership often feels like that. You speak, you sign, you decide—and you are watched. Yet within two months of assuming office, I found myself drawn to something decidedly unglamorous: processes. I convened a meeting of the nursing leadership and proposed mapping our existing workflows and redesigning them systematically. It was not dramatic work. It was necessary work—the kind that prevents small irritations from turning into daily disasters.
One of the most delicate challenges was leading colleagues who had once been peers. Roles had changed, but relationships had not. Some resisted quietly; others watched for signs of favouritism. Surgeons, in particular, are keen observers of hierarchy and fairness. I learned early that firmness did not require severity, and fairness did not demand distance. The feared undermining never came—perhaps because I did not try to rule, but tried to run the hospital.
Administration, however, exacts a price. To do the job honestly, I had to step back from what I loved most—teaching and research. I delivered fewer lectures, conducted fewer bedside clinics, and wrote less than I wished. The trade-off was unavoidable, and I felt it sharply. The ward had been my natural habitat. The MS office was a different ecosystem altogether.
As my administrative responsibilities deepened, problems began to reveal themselves everywhere. I became, almost inadvertently, a detective—restless until each loose end was examined. I started taking long, solitary rounds through the hospital: registration OPD, clinics, laboratories, imaging suites, CSSD, medical stores, blood bank, wards, operating theatres, medical records, kitchens, laundries, oxygen plants, palliative care units, mother-and-child buildings, emergency departments, toilets, gardens, parking areas. Nothing felt too small to inspect, because nothing small stays small for long in a hospital.
I could have delegated much of this. I chose not to. I wanted to understand the hospital not through reports, but through observation. Often, I was accompanied by the office superintendent, matrons, assistant matrons, and biomedical engineers—a moving team, each with a different lens, each noticing what the other missed. What emerged was a long list of ordinary but essential tasks: peeling paint, leaking taps, overgrown weeds, lights burning in empty rooms, wards crowded with visitors, corridors that looked tired, toilets that looked abandoned. Each problem seemed trivial in isolation, yet together they shaped the patient’s experience more powerfully than any policy circular.
***
Patient satisfaction proved elusive. To listen better, I began scheduling regular meetings with nursing supervisors and administrators. Later, we appointed a Public Relations Officer, Shaily, who introduced a new system: feedback collected digitally on iPads by social workers, then analysed every month to identify patterns. The results were sobering.
Patients complained of long waiting times, especially for specialist consultations, and of weeks-long delays for ultrasound—most painfully among pregnant women. Medicines were often unavailable or expensive. Parking charges felt arbitrary. More troubling were concerns about care itself: irregular ward rounds, poor communication, wound infections overlooked, and, in one instance, a dialysis technician chewing tobacco while on duty. None of this was unique to our hospital. But as a large public teaching institution, we carried a special responsibility. These reports forced us to confront uncomfortable truths about culture, accountability, and training. We needed to listen better, respond faster, and act decisively.
Improvement, I learned, is rarely spectacular. It is incremental, repetitive, and often thankless. It happens in small corrections—in showing up, paying attention, and refusing to look away. Walking the tightrope between administration, teaching, and research was never easy. I stumbled more than once. Yet I remained convinced that a hospital does not run on policies alone. It runs on habits, humility, and the willingness to see what others overlook.
That, perhaps, was my way of playing the game.
The Numbers Game
Negotiation is a skill they neglect to teach in medical school. You are trained to read the jagged peaks of an ECG, to decipher the complex chemistry of an ABG, and to break the heaviest of news with a steady voice. No one prepares you to sit across a polished mahogany table and haggle over the price of a high-end ventilator as if you were arguing over a sack of onions in a village mandi.
Yet, as Medical Superintendent, I found myself negotiating almost every week—sometimes every day. In the beginning, I was far too polite. I listened to vendors with a physician’s bedside manner, accepting their technical justifications too easily, only to walk away with the sinking feeling that I had paid a premium the hospital could ill afford. In Sevagram, a hospital’s purse is not just a ledger; it is a life-support system. If you fail to bargain, you don't merely lose money—you lose beds, drugs, oxygen, and the precious time of the poor. Over the years, I learned to be hard-nosed, not because I enjoyed the contest, but because every rupee saved on a machine was a rupee that could be diverted to a patient who arrived with nothing but hope.
***
The scene in the committee room was a study in contrasts. We would sit there in our simple khadi—sometimes slightly crumpled, often un-ironed, always honest. Across from us sat the representatives of multinational conglomerates, immaculate in tailored suits and silk ties, armed with glossy brochures and a confidence buffed to a high shine in corporate boardrooms.
The gulf between us wasn't just in our clothes; it was in our vocabulary and our assumptions. They came from a world where "margins" were the primary metric of success. We came from a world where a family might sell their only goat to afford a week’s worth of medicine. Yet, when the meeting began, the table had a way of leveling itself. A hospital can be underfunded, but it must never be weak.
***
I remember one specific negotiation that captures the "Sevagram style"—a dance of small concessions and moral gravity. The vendor had quoted ₹13 lakhs for a ventilator.
"The price is high," I began. "Why ₹13 lakhs?"
The agency representative smiled—a practiced, sympathetic expression. "Sir, this is high-end. Advanced modes, multiple alarms, designed for the critically ill. It is the Mercedes of ventilators."
Mr. Tapdiya didn't look at the brochure. He looked at the representative. "Break down the cost. Which specific features are driving this? We don't pay for bells and whistles we don't need."
Dhirubhai then delivered the first blow. "We understand quality, but we have a budget. Can you bring it down to eight?"
The representative’s smile wavered. It was the look of a man asked to sell that Mercedes for the price of a Maruti. "That’s a 40% reduction, Sir! If you order twenty units, perhaps we can talk 5%..."
"We cannot buy twenty," Dhirubhai leaned forward, his tone shifting from administrator to patriarch. "This hospital is not like the ones you visit in Nagpur or Mumbai. We follow a Gandhian philosophy. We subsidize everything. Our patients cannot afford private ICU rates. We need this equipment, but we cannot betray our mission to get it."
Then I would play the long game—the one vendors understood even better than morality. "Our ICU is a training ground," I added. "The residents who learn on your machines today will be the intensivists of tomorrow. They will buy the brands they trust. You aren't just selling a machine; you are buying a decade of brand loyalty. But our ceiling is ₹8 lakhs. Not a rupee more."
***
The dance would continue for an hour. They would offer "upfront payment discounts" or "extended service terms." We would counter with our greatest strength: transparency. "We pay within a week of installation," Dhirubhai would say. "No bribes, no commissions, no hidden 'extra charges.' Clean and transparent. But the price must move."
Finally, Mr. Tapdiya would deliver the closer. "We are also looking at monitors and infusion pumps. If you match our price now, we build a relationship. If not, we explore alternatives."
A few days later, the "impossible" would happen. The final offer would arrive: ₹8 lakhs. The Mercedes was suddenly available at our price.
***
What the Superintendent’s chair taught me was that the best negotiation begins long before you enter the room. It begins with "homework"—talking to alumni, comparing prices across states, and understanding the difference between what a brochure claims you must have and what your patients actually need. I learned never to be seduced by a vendor's flattery; a salesman’s compliments are often the most expensive item on the invoice.
One alumnus, Dr. Skand Trivedi, a cardiologist from Bhopal, shaped my approach more than most. He taught me to be almost unsentimental during these sessions. "You are not bargaining for yourself," he would remind me. "You are bargaining for patients you will never meet."
In the end, the numbers were never just digits on a spreadsheet. They were oxygen cylinders, vials of antibiotics, and extra days on a ventilator for a farmer’s son. In Sevagram, negotiation was never a corporate sport. It was a quiet, stubborn form of care.
The Hundred Square Foot Office
The physical spaces we inhabit shape the way we work. In Sevagram, I learned the reverse can also be true: the work shapes the space. Over twelve years as Medical Superintendent, I functioned out of three offices. Each location marked a distinct phase of my administrative life—its tempo, its pressures, and its small lessons in humility.
My first office lay in the old hospital building, close to the Hospital Information System (HIS) department where Bhavana worked. Many mornings began with a familiar rhythm. We would leave home together and walk to the hospital—husband and wife stepping into the day in tandem, the same dusty road, the same campus trees, the same rush of OPD crowds gathering at the gates.
But the moment we crossed into the hospital premises, an invisible line appeared between us.
Bhavana almost never entered the MS Office. Not because she was unwelcome—far from it—but because she chose to keep a deliberate distance. She knew how quickly institutions gossip, and how easily people confuse proximity with privilege. In a system where hierarchy is watched closely, her restraint was her quiet strength. She ran the digital backbone of the hospital next door; I ran the administrative nerve centre here. We worked within earshot, yet we guarded our boundaries with care.
It was her way of saying: let the work speak, not the relationship.
In those early years, I came to respect that discipline. It protected her reputation, it protected mine, and it protected the integrity of the office. In Sevagram, such invisible protocols matter as much as written rules.
***
In the summer of 2015, the geography of my work changed abruptly. The Central Sterile Services Department (CSSD) needed urgent renovation and expansion. New autoclaves had to be installed, sterilisation protocols upgraded, workflows redesigned. For that to happen, we had to give up a chunk of the MS Office complex—specifically the area where our clerks sat and where files moved like blood through a busy artery.
There was no choice. The hospital’s needs are rarely polite. They arrive as emergencies.
So we shifted.
I moved to the Medicine Department building, where I would remain until 2020. My new “chamber” was a lesson in enforced simplicity—barely a hundred square feet. It held a small desk, a computer, a printer, two visitor chairs, and a cupboard for a few essential books. That was all. No plush furniture. No long conference table. No illusion of grandeur.
It was not the kind of room that fits the image of a hospital head. It was, however, enough to work.
One day, during a Medical Council of India inspection, the austerity of that space became an issue. The inspector walked in, glanced around, and frowned. He seemed to be searching for something—perhaps a larger table, perhaps a larger man.
He said, almost accusingly, that the Medical Superintendent’s office did not meet the “standard” dimensions expected for the post.
I looked at him, looked at the room, and then smiled.
“Sir,” I said, “do you measure the efficiency of the Medical Superintendent by the length and breadth of his office, or by the work that comes out of it?”
He paused. His eyes moved from the cramped walls to the busy desk, to the files being signed, to the staff waiting outside. Then he chuckled, made a note that said nothing, and walked away.
That small room taught me something I should have known earlier: authority does not require square footage. It requires presence.
Three Rooms Where I Changed
Some education happens in lecture halls, under fluorescent lights, in front of PowerPoint slides. Some happens in rooms where the chairs are arranged in a circle and nobody is quite sure, when the day begins, where the conversation will go. The three workshops I write about here belong to the second kind. They did not give me a certificate. They gave me something harder to name — a way of seeing what was already in front of me, but which I had not, until then, truly looked at.
***
The Academy of Medical Sciences in Nagpur had organised a workshop on medical ethics. When it was first announced, the response was indifferent, sometimes openly hostile. Why would a doctor leave his practice on a weekend for a subject with no CPD credits, no drug company dinner, no excursion? One colleague said plainly that ethicists were armchair critics — too removed from the real world to understand why kickbacks existed. Another wondered if the Academy had made a mistake.
The organisers were not sure themselves. They had promised simple vegetarian food, no alcohol, a pen and a writing pad. Delegates would pay their own fees; no sponsor would enter the room. On the eve of the workshop, some thought of planting questions in the audience to prevent an embarrassing silence.
They need not have worried.
Seventy-four doctors enrolled. Fifty-eight came. A drug company had organised an excursion for doctors and their families on the same day; forty-four doctors still chose to stay until the end. When a speaker finished talking, hands went up before he had sat down. Arguments broke out — heated, genuine arguments — about whether patients tested for HIV should be informed, whether their spouses had the right to know, whether bad news belonged to the patient alone or to the family who would carry it. These were not abstract questions. Every man and woman in the room had faced them in their own consulting rooms and carried them home at night.
I watched doctors who had never spoken on such matters in a professional setting find that they had opinions — strong ones. I watched a psychiatrist and a surgeon discover, with some surprise, that they disagreed entirely on informed consent and agreed entirely on the ethics of dying. Something was happening in that room that scientific conferences in Nagpur had rarely witnessed: people were being honest.
One delegate said at the end, almost to himself, that he had understood for the first time what Mother Teresa had meant when she said that medicine is a vocation. Not a profession, not a business. A vocation.
I have not forgotten that sentence. It arrived quietly and stayed.
***
Sixteen years later, the Academy returned to ethics — this time in a residential setting, two days at the Surhabardi estate outside Nagpur, forty doctors, and a faculty that included some of the most serious thinkers in Indian medical ethics: Amar Jesani, Sanjay Nagral, Arun Gadre, Sunita Bandewar, Veena Johari, Arun Mitra.
What struck me, sitting in that room in December, was not the novelty of the questions but the rigour brought to questions I had always assumed I understood. Conflict of interest, for instance — a phrase I had heard many times — was not simply about taking gifts from pharmaceutical companies. It was a structural condition, embedded in the way medicine is organised and paid for, the way hospitals are run, the way private practice creates incentives that pull silently against the patient's interest. Gadre and Nagral did not sermonise. They told stories, some of them uncomfortable, drawn from their own practice. They showed, without saying it directly, that even good doctors operate inside systems that make ethics difficult, and that acknowledging this is not a confession of weakness but the beginning of clear thinking.
Jesani opened the workshop with a question that has not left me: what does it mean to be good, and is being good the same as doing good? A doctor can perform every correct procedure and remain indifferent to the person on the table. A doctor can feel great compassion and fail the patient entirely. Ethics is not located in feeling or in procedure alone. It lives in the space between them, in the quality of attention one brings to each encounter.
The session on end-of-life care, which I shared with Sunita Bandewar, made plain something I had long sensed but not articulated: that dying patients are not failed patients. That the refusal to acknowledge dying — the pivot to one more scan, one more line of treatment — is sometimes not hope but its absence, dressed in the language of medicine. To sit with a patient who is dying and tell the truth without abandoning them is, in its own way, the hardest thing a doctor does.
Sanjay Nagral had a flight to catch. I dropped him at the Nagpur airport and turned the car towards Sevagram. The 75 kilometres home felt longer than they were.
***
The training programme in palliative care that the Department of Medicine at MGIMS hosted in March 2019 was different again. Dr MR Rajagopal came from Trivandrum. Gilly Burn, who has spent a lifetime working in palliative care, came from the United Kingdom. Abhijit Dam came from a hospice in rural Jharkhand. Jimmy Rana, who had built the first palliative care centre in Nagpur from his own resources, came to speak not as a clinician but as a man who had simply seen suffering and decided he could not look away.
The ten days began with a film about Rajagopal's own life — his decades of work to make morphine available to dying patients in India, his encounters with bureaucracy, indifference, and occasional hostility from within the medical establishment. The film was not comfortable viewing. It was a record of how thoroughly the system can fail a patient in pain, and of what one person, over a lifetime, can change.

Lessons in compassion: Learning community palliative care with Dr. M.R. Rajagopal, Thiruvananthapuram, 2018.
What the workshop did, more than any lecture could, was put us in the homes of patients. Social workers had identified people living with cancer in the villages around Sevagram, and participants — nurses, physicians, a gynaecologist, an anaesthesiologist, a dental surgeon — visited them under faculty supervision. These were not ward rounds. There were no files, no monitors, no trolleys. There were families managing on small incomes, caring for someone who could not be cured, trying to understand why they still had pain when they had been given medicines for it. There were children who had not been told the truth about their parent's illness because the family had decided, unanimously, that the truth was too dangerous.
In those homes, the gap between what medicine offers and what patients need became very clear. It was not a gap that technology could close.
Gilly Burn spent a morning on communication — not the communication of information, which doctors are trained in, but the communication of presence, which most of us are not. She spoke slowly, and chose her words carefully, and the room was quiet in a way it had not been during any other session. What she described was not a skill so much as a discipline: the discipline of staying in the room with someone who is frightened, of not reaching for reassurance when what the patient needs is simply to be heard.
I have tried to practise this since. I do not always manage it. But I know now when I am failing, which is more than I knew before.
***
Three workshops. Twenty years. The questions they raised — about honesty, about power, about what we owe the people who come to us in pain — do not have final answers. They have only the practice of returning to them, in each new room, with each new patient, and trying to do a little better than the last time.
That, I think, is what they were really teaching.
Science Without Sponsors
When Dr. Sushila Nayar passed away, she left behind a vacuum that no one could fill simply by occupying her chair. It was a void that was simultaneously moral, administrative, and emotional. The Kasturba Health Society needed a guardian who could protect the Gandhian spine of the institute while ensuring the books balanced at the end of the month. Idealism without arithmetic rarely survives the winter, but arithmetic without ideals is a far more dangerous pathology.
The choice fell on Shri Dhirubhai Mehta. He was not a physician; he came from a different tribe altogether—a Chartered Accountant from the Bajaj stable, trained to read balance sheets with the same clinical scrutiny we applied to ECGs. Beneath the crisp khadi shirt was an unexpectedly stubborn social conscience. He had watched Behenji’s frugality for decades, learning that money in a charitable institution must travel in a straight line and leave no perfume behind.
***
In September 2002, I received a phone call that altered the DNA of MGIMS. Dhirubhai was at the Nagpur airport, waiting for a flight. The line crackled with terminal static, but his tone was steady.
"SP," he said, skipping the preamble, "I want to stop all funding from the drug and device industry for our conferences. Make me a plan."
That was his signature: no committees, no ceremonial position papers, just a decision followed by the work. He had little patience for data meant to cloud the obvious. "Don’t try to confuse me with statistics," he would often say dryly. "I’ve already made up my mind."
The context of that call was a dinner we had shared the previous evening at his modest, whitewashed house. We both ate like cautious diabetics: two rotis, a sabzi, dal, and curd. The food disappeared in ten minutes; the conversation lasted two hours.
***
That night, we spoke of the "circus" that medical conferences had become. We discussed banquet menus debated with more passion than research papers, and cocktail evenings that grew louder as the slides grew fewer. We spoke of delegate bags fat with corporate gifts and "travel grants" that looked suspiciously like family holidays. The companies paid the bills, we signed the receipts, and we called it education.
I had handed him a copy of the British Medical Journal featuring an article on the consequences of pharmaceutical funding. "Look at what American universities are doing," I told him. "They are beginning to refuse even free lunches. Why can’t we lead instead of follow?" He slipped the journal into his bag. The airport call told me he had not only read it; he had digested it.
***
After the call, I dissected the accounts of a recent CME that had cost ₹3.3 lakh. The industry had paid nearly two-thirds. At first glance, we appeared dependent. But the truth was revealing: the money hadn't funded science; it had funded comfort. It had gone toward elaborate meals and the "theatre" of hospitality.
The arithmetic was liberating. If we stripped the meeting to its essentials—simple food, no gifts, no frills—we could run it at a fraction of the cost. We didn't need their money; we had simply grown accustomed to the luxury of it. Habit, not necessity, was our real dependency.
***
On October 21, 2002, Dhirubhai convened the department heads in the Dean’s office. He spoke plainly: "There is nothing called a free lunch. If we accept their money, we accept their influence. We stop today."
The sentence landed with the weight of a gavel. This wasn't just a policy change; it was a mutiny against the prevailing medical culture of India. No other medical college in the country had dared to suggest that the pharmaceutical industry—the silent paymaster of academic medicine—be shown the door.
The room erupted. Colleagues worried about falling registrations and the lack of "proper" catering. Dr. Ulhas Jajoo cut through the noise: "Are we organizing conferences for food, or for thought?" Dhirubhai listened, then decided. From that day on, no drug company would fund an academic program in Sevagram. No stalls, no banners, no polite disguises.
***
Policies are easy to draft; the test lies in the first "un-sponsored" lunch. Soon after, two departments organized state-level conferences under the new rules. The food was simple and vegetarian. There were no cocktails, no glossy bags, and no branded paraphernalia. To everyone’s surprise, the halls were full. Doctors came for the science, not the gift hampers.
This move sparked a ripple across the country. We were called "radicals" and "idealists," but we had proved a point: academic dignity does not require a sponsor. We were the first in India to prove that a medical college could thrive on its own terms.
***
More than two decades have passed. Across India, medical conferences have grown into corporate launches. Banquets now resemble weddings. Sevagram remains an outlier. We continue to host meetings where the only thing on offer is the science. There are no brand ambassadors hovering near the tea counter. It is quieter, cleaner, and far more dignified. We may not offer five-star hospitality, but we offer independence. In medicine, as in life, that is the only luxury worth having.
The Price of a Prescription
In January 2011, The Lancet published a statistic that should have made every policymaker in Delhi lose sleep: healthcare costs push 39 million Indians into poverty every year. In a country where insurance coverage is a thin gauze and government spending remains modest, out-of-pocket expenditure accounts for nearly four-fifths of total health spending.
The biggest culprit is not the surgeon’s fee, the ICU monitor, or the hospital bed. It is the medicine.
In rural India, nearly three-quarters of healthcare spending vanishes into the pharmacy. I did not need a journal to validate that number; I saw it unfold daily in Sevagram—quietly and repeatedly, like a slow leak that eventually empties a household. A daily-wage laborer would arrive breathless after a heart attack, or a farmer would be carried in after a snakebite. We would stabilize them and save them, but then, at the end of the encounter, we would hand them a prescription.

That piece of paper, so light in the doctor’s hand, was unbearably heavy in the patient’s life. To honor it, a man would sell his wife’s jewelry, mortgage his small plot of land, or borrow from a moneylender at interest rates that only desperation could justify. Healthcare had become the leading cause of rural debt, second only to the dowry. I realized then that we couldn’t just treat the disease; we had to treat the bill.
The biggest culprit is not the surgeon’s fee, the ICU monitor, or the hospital bed. It is the medicine.
***
The more I watched these families struggle, the more I asked: why are medicines so expensive? When I looked closely, the market appeared as a theatre of contradictions. The same molecule—atorvastatin, for instance—was sold by one company at ₹0.80 per tablet and by another at ₹8.00. This ten-fold difference was not a matter of science or quality; it was a matter of perception.
Market leaders charged a premium because they spent crores convincing doctors that their brand was "superior." They created a monopoly not of molecules, but of minds. Then came the supply chain—the agents, stockists, and wholesalers—each adding a margin until the final markup reached 1000% or more. We could not fix the national market, but we could fix the market within our own walls.
***
We formed a Drug and Therapeutics Committee (DTC)—not as a bureaucratic formality, but as a scalpel to cut away waste. Our goal was to bypass the inflated marketplace and build a direct pipeline from the manufacturer to the patient’s palm.
The first discipline was learning to say "no." Instead of stocking every brand promoted by a medical representative, we created a list of essential medicines guided by WHO principles. We limited ourselves to two trusted brands per drug. Then came the negotiation. We invited tenders only from manufacturers with impeccable GMP compliance—Cipla, Ranbaxy, Dr. Reddy’s. Our pitch was blunt: "We buy directly. No middlemen. No marketing costs. Give us your factory price."
***
When we stripped away the marketing and the margins, the prices didn't just drop—they collapsed. The scale of the change made even our own pharmacists stare twice at the printouts.
The Economics of Survival
The difference between the market price and our procurement cost was not just a number; it was the difference between a family mortgaging their future or returning home with their dignity intact.
| Medicine | Market MRP | Sevagram | Reduction |
|---|---|---|---|
| Pralidoxime Pesticide Antidote |
₹155 | ₹44 | 71.6% |
| Anti-snake Venom Life-saving Biological |
₹450 | ₹240 | 46.6% |
| Piperacillin–tazobactam Critical ICU Antibiotic |
₹1,650 | ₹465 | 71.8% |
These numbers changed more than just expenditure; they changed behavior. Families no longer abandoned treatment halfway through the course. Doctors no longer hesitated to prescribe what was clinically necessary out of fear for the patient's wallet. We capped our own margin at 20%—just enough to cover electricity and salaries—and published a monthly Drug Bulletin by email to keep the system transparent and honest.
***
In October 2010, we introduced the "Pink Slip" initiative for minor ailments. We identified 25 common medicines—painkillers, antacids, cough syrups—and pre-packed them. If a doctor prescribed up to three of these for three days, the patient paid a flat charge of ₹5.
For the cost of a cup of tea, a laborer could walk away with a course of treatment and the dignity of not having to borrow money for paracetamol. It was a small scheme, but it carried a big idea: equity must be designed, not merely wished for.
***
The true impact showed itself in the quiet of the ICU. A year earlier, treating severe sepsis was a financial catastrophe; a ten-day course of antibiotics could cost ₹30,000. Families would sit by the bedside counting breaths and the dwindling notes in their wallets, eventually asking, with shame, if we could stop treatment because the money had run out.
After our initiative, that same course cost ₹9,000. The difference between those two numbers is not arithmetic; it is survival. A breast cancer patient who once paid ₹10,000 for chemotherapy now paid ₹3,700. Sevagram taught me that "high cost" is often an artificial construct of a greedy market. If we can push prices down without compromising quality, economics becomes a tool for compassion. That, to me, is public health in its most practical, unvarnished form.
In January 2011, The Lancet published a statistic that should have made every policymaker in Delhi lose sleep: healthcare costs push 39 million Indians into poverty every year. In a country where insurance coverage is a thin gauze and government spending remains modest, out-of-pocket expenditure accounts for nearly four-fifths of total health spending.
The biggest culprit is not the surgeon’s fee, the ICU monitor, or the hospital bed. It is the medicine.
In rural India, nearly three-quarters of healthcare spending vanishes into the pharmacy. I did not need a journal to validate that number; I saw it unfold daily in Sevagram—quietly and repeatedly, like a slow leak that eventually empties a household. A daily-wage laborer would arrive breathless after a heart attack, or a farmer would be carried in after a snakebite. We would stabilize them and save them, but then, at the end of the encounter, we would hand them a prescription.
That piece of paper, so light in the doctor’s hand, was unbearably heavy in the patient’s life. To honor it, a man would sell his wife’s jewelry, mortgage his small plot of land, or borrow from a moneylender at interest rates that only desperation could justify. Healthcare had become the leading cause of rural debt, second only to the dowry. I realized then that we couldn’t just treat the disease; we had to treat the bill.
Clearing the Corridors
By 2009, I was the Medical Superintendent of Kasturba Hospital. We had already built a firewall against the pharmaceutical industry in our classrooms. Conferences in Sevagram no longer ran on drug-company money, and our academic meetings had become quieter, leaner, and cleaner.
But the hospital corridors were a different battlefield.
Every morning, as the Outpatient Department opened its doors and the first patients began to queue up, a second stream walked in—confident, brisk, and unmistakably out of place. Young men and women in crisp shirts and ties, hair neatly combed, shoes polished, carrying leather bags that looked heavier than a medical textbook.
Medical Representatives.
Their job was to sell, and they were very good at it. They hovered outside consulting rooms like seasoned hawks. They caught interns between wards and staircases. They slid into cabins in the tiny gaps between patients, timing their pitch with the precision of a commuter train. They carried pens, calendars, paperweights, prescription pads, pen drives, even reflex hammers—small gifts, harmless in appearance, and therefore dangerous.
The influence was not harmless. It rarely announces itself. It enters quietly and stays.
***
The first warning came from an unexpected place: our pharmacists.
They began to notice a pattern in prescriptions that did not fit the clinical picture. Bright, well-meaning residents were writing for expensive tonics, unnecessary multivitamins, and “me-too” brands that offered little advantage beyond glossy packaging. A patient with diabetes would walk out with a prescription for a high-end branded statin costing ten rupees a tablet when an equivalent generic sat on the shelf for one rupee.
Why this ten-fold leap?
Often, the answer was simple: an MR had been in the room.
The pharmaceutical industry understands psychology better than most doctors understand pharmacology. They know that a gift, however small, creates a subconscious debt. When a doctor accepts a pen, it is not a bribe. It is a hook. The doctor feels no shame, because the item is trivial, but the mind registers the exchange all the same: someone has done something for me.
And once you feel obliged to listen, you become vulnerable to persuasion.
There is enough evidence to show that doctors who interact with drug companies are more likely to prescribe expensive, non-rational medicines. Most of this is not corruption in the cinematic sense. It is seduction—slow, polished, professional, and almost invisible.
That was when I realised I could not simply instruct my doctors to “be ethical.” Ethics is not a slogan you paste on a wall. It is a discipline you must protect—especially when young doctors are tired, overworked, and still learning the difference between science and marketing.
If temptation sits outside every consulting room, eventually someone will open the door.
***
So I issued an order that was bound to be unpopular.
Medical Representatives were no longer allowed inside the OPD and wards during hospital hours. No more cabin visits. No more detailing. No more hovering in corridors. No more gifts.
The reaction was immediate and noisy. Some colleagues were irritated. A few were genuinely anxious.
“How will we stay updated?” they asked. “MRs tell us about new drugs, dosages, side effects. They give samples for poor patients.”
I had heard these arguments for years. They sounded reasonable until you examined them closely.
“You are doctors,” I told them. “If you want to learn about a drug, read a textbook. Search the internet. Read a journal. Don’t let a salesman teach you pharmacology.”
And the “free samples”? That story, too, had a sentimental glow. But the truth was harsher. Samples rarely reached the poorest patients in a systematic way. They helped a few, randomly. They often stayed with staff or travelled to favoured patients. They created dependence, not access.
A hospital that truly cares for the poor must build a system of affordability—not rely on scattered charity from a company whose profits depend on expensive prescriptions.
***
Within days, the Medical Representatives’ association demanded a meeting.
About fifty of them marched into my office. They filled the room, shoulder to shoulder, anger and anxiety mixing in their faces. They were not villains. They were young people trying to make a living in a system that rewarded aggressive selling. Some looked barely older than our interns.
Their leader spoke first. His voice trembled, partly with outrage, partly with fear.
“Sir, up to half of our business comes from your hospital. If you ban us, we will lose our jobs. How will we feed our families?”
It was the classic livelihood argument—emotionally powerful and not entirely dishonest.
I felt a pang of sympathy. I knew what unemployment looks like in small towns. I knew how quickly a household collapses when a salary stops.
But I also knew what a ₹1,500 prescription does to a family that earns ₹250 a day.
So I told them, as gently as I could, what I believed was the truth.
“I am not against you,” I said. “I am fighting the grip your industry has on my doctors. The way your companies make medicines seem better than they actually are makes doctors prescribe unnecessary drugs. That makes healthcare expensive.”
Then I added the sentence that made the room go quiet.
“Your presence here is a tax on my patients.”
They listened, stiffly. Some looked away. A few stared at the floor. They had come expecting an argument about rules and permissions. They were not prepared to be told that their work, however innocent they felt it to be, was helping push poor patients into debt.
They left unhappy. But the ban stayed.
***
Removing the MRs from the corridors was only half the job. The harder task was changing the prescribing culture they had helped build.
We needed to de-program our doctors—not by moral lectures, but by teaching them a new habit of thinking. We called it reverse marketing.
Marketing usually trains you to choose the most expensive item, the one with the best packaging, the most persuasive story. Reverse marketing taught our residents to do the opposite: choose the least expensive effective option.
We put up simple charts in clinics and wards. They compared brands, not by colour or company, but by molecule and cost.
One brand: ₹100
Another brand: ₹80
Our generic: ₹15
The point was not to shame anyone. It was to make the invisible visible. Once doctors saw the numbers in black and white, many felt embarrassed. Some felt angry—at the industry, and at themselves. Most, to their credit, changed.
We trained them to look at the molecule, not the shine. We taught them that a “good doctor” is not the one who can recite brand names like a jingle, but the one who understands the cost–benefit ratio of every prescription.
***
Years later, in 2022, a biography of Dilip Shanghvi—Sun Pharma’s founder—was published: The Reluctant Billionaire. It read like a manual of how the industry works. How companies indulge doctors, inflate their self-esteem, cater to their unspoken desires, and shape habits without appearing to do so.
I remember thinking, with a mix of amusement and sadness: if our residents had read that book in 2009, they would have understood that they were not “partners” in healthcare.
They were targets in a sales strategy.
***
It has been many years since we cleared the corridors. Today, the OPD in Sevagram feels quieter. The swarm of ties and leather bags is gone. Doctors sit in their cabins without being interrupted by a sales pitch delivered between two patients. When they write a prescription, they are not thinking of a pleasant young man outside the door or a pen on their desk.
They are thinking of the patient.
But the larger truth remains uncomfortable. MGIMS is an outlier. In thousands of hospitals across India, the siege continues. The invisible hand still guides the doctor’s pen—softly, politely, and relentlessly.
And every time it does, a poor family somewhere pays for it.
The Graveyard of Paper
A medical case record is not merely a stack of paper. It is a biography of suffering and survival.
At its best, a case file carries a story that begins with fear and ends—if we are fortunate—with relief. It should tell us why the patient came, what we saw, what we suspected, what we missed, and what we finally understood. It should record not only the diagnosis, but also the thinking behind it: the false trails, the turning points, the quiet triumphs, and the occasional regrets. A good record is a witness to the struggle between life and death.
In Sevagram, however, our case papers had stopped being witnesses. They had become props.
***
For weeks after I took charge, I found myself staring at piles of case papers heaped in precarious stacks across the wards—paper towers leaning like tired men at the end of a long day. They were everywhere: on trolleys, on tables, on window ledges, inside cupboards that would not close properly. The sight was not merely untidy. It was a silent monument to our administrative failure.
Curiosity made me do what most administrators do not: I began to read them.
What I found was disheartening. Many papers were blank, not even decorated with the doctor’s trademark illegible scribble. Others contained histories so brief and cryptic that I almost envied the clinician who could apparently diagnose complex human misery in three sentences.
The most tragicomic part was the “vital signs” chart. If those sheets were to be believed, the patients in our wards were blessed with a miraculous physiological stability. Day after day, pulse, respiratory rate, and blood pressure appeared as near-identical numbers—so neat, so uniform, so unchanging that they defied the chaos of biology.
The cover page might scream a terrifying diagnosis—Septic Shock, Perforation Peritonitis, Acute Abdomen—but the inner pages offered no narrative to support it. If these records were true, patients arrived with burst intestines, had them stitched by ghosts, and went home alive—not because of their doctors, but despite them.
I knew what the truth was, of course. Our clinicians were working hard. The wards were busy. Emergencies did not pause for paperwork. Yet the gap between what was done and what was written had grown so wide that the file had become a work of fiction.
And fiction, however tidy, is useless in medicine.
***
By September, the problem had reached critical mass. We conducted a census and arrived at a number that stunned even those who were accustomed to chaos.
There were eighteen thousand incomplete case papers scattered across the hospital.
Eighteen thousand.
They were choking the Ward-in-Charge cupboards, crammed into drawers, wedged into lockers, and hidden under tables like contraband. Papers that had once been crisp and white had turned a mournful yellow. We found them in imaginative hiding spots—tucked behind water coolers, gathering dust atop refrigerators, abandoned on tabletops, flattened under mattresses in the residents’ hostel, and buried beneath unrelated files as if someone hoped they would quietly disappear.
They were not records anymore. They were orphans.
***
I decided to act.
I coaxed. I cajoled. I gave pep talks. I wrinkled my forehead in feigned anger and taxed my vocal cords in genuine frustration. I appealed to nurses, to interns, to residents, to anyone who might listen. My mandate was simple and absolute:
Finish the job. Send every file back to the Medical Records Department.
The response was compliance, but it was born of compulsion, not conviction. I knew nobody liked this work. And in my heart, I sympathised with them.
There is a special kind of drudgery in retrospective documentation. Writing notes in real time is hard enough. Writing them months later is like trying to reconstruct a monsoon from the dryness of a cracked riverbed.
“What do we write, sir?” the interns asked, eyes pleading. “How do we fill case records for babies who were delivered, cried, and left with their mothers months ago—when we were still studying Pathology?”
The surgery residents were equally pragmatic. “How do we compile injury reports for trauma patients we never saw, managed by seniors who have already graduated?”
Honestly, I had no good answer.
I stood there enforcing a rule that I knew could produce only one outcome: fiction. I was asking young doctors to fill sheets with reconstructed histories, invented physical signs, and neat narratives that had never existed. Even as I insisted on completeness, I kept wondering if these notes were worth the price of the paper they were written on.
Yet, I also knew the alternative was worse. An incomplete file is not merely inconvenient—it is dangerous. It is a medicolegal liability. It is a teaching failure. It is a betrayal of the patient’s story.
So I pushed.
***
Over four grueling weeks, the purge was completed. Those eighteen thousand case papers travelled their final kilometre—from the chaos of wards to the silence of the MRD.
But even there, what awaited them?
The technicians in the MRD would do what they had always done. They would sort the files by number, bundle them, label them, and shove them onto cold steel racks. A handful might be resurrected—pulled out for a court case, or retrieved by a postgraduate student planning a thesis based on “chart review,” a research method I had begun to view with increasing skepticism given the quality of the data.
The rest were destined to die an unsung death.
After five years of gathering dust, they would be shredded and recycled, their “stories” never read, their data never analysed. The hospital would move on, and the patients who had once filled those beds would vanish into anonymity, leaving behind only paper that no longer meant anything.
That was when the thought became unavoidable: we were not managing records.
We were managing a graveyard.
If Sevagram was to truly modernise, we did not need better penmanship or stricter scolding. We needed a revolution. We needed to stop writing fiction on paper and start capturing truth in bytes.
And so the decision was made.
The MRD would go digital.
A CT in a Village
On October 16, 2010, a small wave of excitement swept through our rural teaching hospital in Sevagram. We were preparing to install a new Computed Tomography (CT) scanner—sleek, expensive, and unmistakably modern. The old machine had served us faithfully for almost a decade, but it was now living on borrowed time. The administration, convinced that good radiology was no longer a luxury but a necessity, approved an investment of nearly ₹1.5 crore for a replacement.
Our radiology consultants and residents were euphoric. They had every reason to be.
A CT scanner can change the way a hospital thinks. It can show you a bleed inside the skull when the patient is still talking. It can pick up a small stroke before the limb has fully weakened. It can reveal a hidden abscess, a cancer, a pulmonary embolus, a ruptured appendix—things that would once have remained guesses until the body declared itself too loudly to ignore. In a place like Sevagram, where patients often arrive late and sick, such clarity can feel like a gift.
And yet, while the machine was being wheeled in, calibrated, and admired, I found myself striking a slightly discordant note. I should have been celebrating, but I was uneasy.
Not because I disliked technology. I had spent years trying to drag our hospital into the digital age. But I had also learned that every new machine arrives with two shadows: the cost it demands and the habits it changes. A CT scanner does not merely add capability. It subtly rearranges the culture of clinical decision-making.
The seduction of technology is that it looks clean and certain. The image feels like truth. Patients believe that a “state-of-the-art” scan is a magic lamp: rub it once, and the body’s secrets will appear. We cannot blame them. A CT image looks too precise to doubt.
The problem is us. We rarely take the time to explain what the scan can—and cannot—do. We do not warn them about what it might discover accidentally. We rarely talk about radiation. And we almost never admit that sometimes, the best test is no test at all.
As the new machine hummed to life, I saw three dangers we were failing to discuss.
***
My first fear was not about the scanner itself, but about what it would replace.
A CT scanner can become a shortcut for thinking. It can tempt us to skip the slow work of listening, examining, and reasoning. When that happens, the stethoscope does not disappear from our necks—but it quietly stops guiding our minds.
Headache is a perfect example. In primary care, most headaches are tension headaches or migraines. They require a careful history, a patient ear, and a sensible neurological examination—not a scan. Yet, the waiting halls of CT centres are crowded with anxious people who have had a headache for three days and have already convinced themselves they have a tumour.
Evidence has been telling us this for years. In patients with severe headaches but a normal neurological examination, serious brain pathology is rare. Still, in many hospitals, the scan is ordered not because the clinician is convinced, but because the clinician is uncertain—and uncertainty feels unbearable in a world that worships images.
The same logic applies to minor head injuries. A study in the BMJ and many later decision rules have shown that only a small fraction of patients with minor head injury need neurosurgical intervention. Most can be safely managed with observation and clinical judgment. Yet, modern hospitals behave as if every bump on the head deserves a scan.
Protocols are useful, but I began to notice something unsettling: in some settings, protocols were replacing physicians. The scan had become a reflex. The request form was filled faster than the history.
Perhaps the most troubling misuse is in back pain. Patients with aching necks and stiff backs are routinely fed into the donut of the CT machine. But research has shown a strange truth: if you scan the lumbar spines of healthy people with no back pain, a significant proportion will show “disc bulges,” “herniations,” and “degenerative changes.”
The scan finds abnormalities in the way a gossiping neighbour finds scandal—everywhere, in everyone.
Once such an image appears, the temptation to “fix” it becomes strong. Orthopaedic surgeons and neurosurgeons are not villains; they are human beings trained to correct visible problems. But when you operate on a picture rather than a person, you risk doing violence to the very spine you hoped to heal. I remember reading an article in the New England Journal of Medicine that described this bluntly: operating on scans can become an assault on the lumbar spine.
In other words, the CT scan can sometimes turn a healthy back into a lifelong patient.
***
The second danger is quieter, but more insidious.
High-resolution imaging discovers things we were never looking for—findings that are technically “abnormal,” but clinically meaningless. Medicine has invented a name for them: incidentalomas.
A healed infarct in an elderly person’s brain. A tiny benign adrenal nodule. Mild degenerative changes in the spine. A cyst in the kidney. A small scar in the lung. The patient feels fine, but the scan produces a new diagnosis—and with it, new fear.
These findings rarely require treatment. But they almost always require explanation, follow-up, repeat imaging, referrals, and a chain of events that can turn a simple complaint into a long pilgrimage through clinics.
Jerome Groopman, in How Doctors Think, quotes Dr. Terry Light on this dilemma:
“The hateful part of MRIs—I mean they can be a wonderful technology—but they find abnormalities in everybody. More often than not, I am stuck trying to figure out whether the MRI abnormality is responsible for the pain. That is the really hard part.”
That line stayed with me because it captured the daily misery of modern medicine: we are not only diagnosing disease; we are managing anxiety created by information.
The incidentaloma is not just a radiological finding. It is a psychological event.
***
The third danger is the one we speak about least, perhaps because it is uncomfortable and inconvenient.
A CT scan is not a photograph. It is radiation.
Rebecca Smith-Bindman, writing in the New England Journal of Medicine, questioned the safety of our growing obsession with imaging. She pointed out that patients receive 100 to 500 times more radiation from a CT scan than from a conventional chest X-ray.
The numbers are sobering, but what is worse is how rarely they are communicated.
A patient with a benign headache or a minor backache—exactly the sort of person who crowds imaging centres—is almost never told that the scan itself carries risk. The industry does not highlight it. The referring doctor does not emphasize it. The patient assumes that “a test cannot harm me.”
But it can.
I often wondered what would happen if CT centres were forced to display a prominent sign at the reception desk:
“Warning: Of every 100 people examined by this scanner, two might eventually develop cancer caused by this machine.”
Would people still line up so easily? Or would they pause, ask questions, and demand that their doctor justify the test?
Perhaps that pause would be good for all of us.
***
And then there is the elephant in the room—money.
A decent CT scanner costs around ₹1.5 crore to buy, and a large sum every year to maintain. A radiologist friend once did the arithmetic for me. If a centre charges ₹2,000 per scan, it needs to scan ten heads, chests, or abdomens every single day for five years just to recover the cost of the machine.
In a clean, honest practice, those numbers are not easy to achieve.
And when numbers become targets, commerce begins to influence science. New “indications” for scanning appear. Newspaper stories get planted. Continuing medical education lectures sponsored by equipment manufacturers quietly glorify early detection. Referring doctors are offered incentives. Patients are frightened into believing that the scan is the only proof of seriousness.
“Half the patients who receive CT scans in my clinic do not need this test,” my friend confessed to me once. “But I do not refuse. I have to keep the referring doctors and the patients happy.”
He did not say it with pride. He said it with resignation.
Even in teaching hospitals like Sevagram, where evidence should rule, we are not immune to such pressures. Managers, often obsessed with balance sheets, measure the worth of a radiology department not by the number of unnecessary tests avoided, but by the volume of scans performed. The more, the better.
When commerce shapes clinical decisions, the art of medicine dies quietly—without a funeral, without a mourner.
***
So, on the day our new CT scanner arrived, my hope was modest.
I hoped we would use it wisely. I hoped we would inject a little science into our ordering habits. I hoped we would return to the bedside—to the history and the physical examination—before scribbling a request form in haste.
Most of all, I hoped we would learn to explain to our patients something that modern medicine rarely says aloud:
Sometimes, the best test is no test.
It is an image-shattering task for health professionals—to shatter the illusion that the image is everything. But if we cannot do it, we will slowly become technicians of technology rather than physicians of people.
And that would be a price far higher than ₹1.5 crore.
The Architecture of the Heart
In 2014, we set out to build a ten-bed Intensive Coronary Care Unit (ICCU) on the first floor of our medicine complex in Sevagram. Most hospital wings are born of dry government grants or institutional budgets, but this one had a soul before the first bag of cement was ever opened.
The funds came from an octogenarian couple in Mumbai. They were quiet, dignified people who had endured a heartbreak that still haunts the collective memory of India: they lost their daughter and son-in-law in the 26/11 terrorist attacks. In the long, hollow years that followed, they chose to transform their private grief into a public gift. They wanted to plant a seed of life where there had been only destruction.
They had only one condition, which they shared with a humility that moved us all: they wished to remain anonymous. No marble plaques, no grand inaugurations, no names etched in brass to catch the morning sun. They just wanted the quiet, steady knowledge that their personal loss was being channeled into the survival of a farmer from a nearby village or a teacher from Wardha. We honored that wish. We used their gift to build the unit and install our first Cath Lab, creating a legacy defined not by a name on a wall, but by the rhythmic "beep" of a recovering heart.
***
Designing an ICU is a delicate exercise in empathy. It is a tightrope walk between clinical efficiency—the cold, hard requirements of medicine—and human warmth. If you lean too far toward the clinical, the space becomes a terrifying laboratory. If you lean too far toward the aesthetic, you risk the safety of a crashing patient.
To bridge this gap, I worked closely with Dr. Vinay Kothari. Vinay was a rare breed: a Mumbai-based physician who had traded his stethoscope for a drafting board to become an architect. It was a partnership made in heaven. Having worn the white coat, Vinay knew the frantic, sweaty pulse of a cardiac emergency. He knew that in a crisis, a door that opens the wrong way or a light switch that is out of reach can be the difference between life and death. Having held a compass, he knew how to translate those split-second medical needs into physical space.
Together, we sat for hours with local craftsmen, sketching ideas on the backs of envelopes and blueprints. We weren't just building a medical facility; we were trying to build a sanctuary. We wanted a place where the air felt lighter, even when the news was heavy.
***
We picked the location of the unit with the obsession of a general planning a defense. We chose a spot on the first floor that shared a common wall with our existing 26-bed Medical ICU. This wasn't just about saving money on walls; it was about "staff fluidity." In a crisis, a nurse from the main ICU could be at a bedside in the ICCU in seconds.
We positioned the entrance right next to wide corridors and ramps. In the world of cardiology, we talk about the "Golden Hour"—that window of time where intervention can stop a heart attack in its tracks. When a patient is rushed in, gray-faced and clutching their chest, every second lost in a slow elevator or a narrow, crowded hallway is a bit of heart muscle lost forever. We designed the path to be frictionless. We wanted the patient to glide from the ambulance to the ICCU bed without a single unnecessary bump or turn. Every meter of flooring was measured against the ticking of a clock.
***
When you walk into a hospital, the floor usually tells you the truth about the institution. We chose a cream-colored vinyl flooring, but the choice was far more than cosmetic. It was seamless and non-slip, but most importantly, we used a "coved" design. This means the flooring doesn't stop at the baseboard; it curves up the wall slightly to meet it. It’s a small, expensive detail, but it means there are no sharp 90-degree corners where dust, grime, and bacteria can hide.
The floor was tough enough to handle the relentless abuse of heavy trolleys and oxygen cylinders, yet it was acoustically absorbent. In an ICU, noise is a form of trauma. The constant "tak-tak" of hard heels on stone can keep a stressed patient from the very sleep they need to heal. This vinyl muffled the world, bringing a much-needed hush to the corridor.
The walls followed a similar logic of beauty-meets-utility. We painted the top half a warm cream and covered the bottom half in a rich, deep blue vinyl. It looked elegant, almost like a corporate office, but the blue vinyl was actually armor. It protected the walls from the constant, unavoidable bumps of stretchers and medicine carts.
We also made a radical decision about lighting. We got rid of the harsh, buzzing fluorescent tube lights that make everyone look like a ghost. Instead, we installed soft, recessed fixtures that added a touch of elegance. More importantly, they helped maintain the "circadian rhythms" of our patients. In an ICU, where there are no windows or clocks, it is easy to lose your sense of time. By dimming the lights in a natural cycle, we helped their bodies remember the difference between noon and midnight.
***
In most traditional ICUs, a patient’s head is surrounded by a scary, chaotic tangle of wires, tubes, and humming boxes. It looks like a telephone exchange from the 1970s. For a patient already terrified of dying, this visual clutter is an added layer of anxiety.
To fix this, we installed "pendants"—sleek, vertical columns hanging from the ceiling. These columns housed the oxygen, suction, and compressed air ports, along with dedicated spaces for infusion pumps and monitors. By moving all the hardware to these suspended columns, we cleared the floor entirely. This gave our nurses and doctors 360-degree access to the patient’s head and torso without anyone tripping over a cable or knocking over a stand during a resuscitation.
Privacy, often the first casualty in a busy hospital, was non-negotiable for us. We used heavy blue curtains with a white mesh strip at the top. The mesh was a practical touch; it allowed the air-conditioning and light to circulate even when the curtains were drawn, so the patient never felt stifled.
And then, there was the chair. Beside every single bed, we placed a comfortable, blue cushioned chair. In the West, an ICU is often a solitary place. In India, a patient never suffers alone; the family suffers with them. A wife wants to hold her husband's hand; a son wants to watch his father's breathing. That chair was our way of acknowledging that the person sitting by the bed was just as much a part of the healing process as the doctor. It was our way of saying, "We see your pain, and you are welcome here."
***
The heart of the unit was the central nursing station. We designed it to be open—no glass partitions, no "us versus them" barriers. It was positioned so that a nurse sitting at the desk had an unrestricted view of all ten beds at a single glance. If a patient so much as shifted uncomfortably, the nurse knew.
This station was the "nerve center" where residents, nurses, and consultants converged. We installed a large computer panel that pulled real-time data from our Hospital Information System. It was the digital brain of the unit, but we made sure the physical layout was just as smart.
We became obsessed with the "logic of storage." In an emergency, a nurse should never have to go on a scavenger hunt for a syringe. We organized everything into four distinct layers. Level one was the bedside—for the patient’s immediate needs. Level two was the nursing station for high-frequency items like gloves and alcohol swabs. Level three was the nursing store for specialized equipment like ventilator circuits, and level four was the remote central store for bulk supplies. This hierarchy ensured that life-saving tools were always within an arm's reach.
***
Finally, we turned our attention to the world outside the glass doors. Waiting for news from an ICU is a special kind of agony. It is a time defined by uncertainty, fear, and powerlessness. In many public hospitals in India, you see the heartbreaking sight of relatives squatting on the cold floor of a corridor, exhausted and ignored, waiting for a doctor to pass by.
We refused to let that happen in Sevagram. We created an ample, open waiting area just outside the unit and furnished it with twenty-five comfortable, cushioned chairs. We wanted the families to wait in dignity. We even chose the signage with care, using the clear, minimalist Helvetica font so that even in a state of high stress, a person could easily find their way. The doors and frames were finished with a rich wooden texture and dark brown accents, lending a sophisticated, hotel-like feel to the entrance.
Our goal was simple but ambitious: we wanted to build a machine for saving lives, but we wanted to dress it in the colors of humanity. We wanted a place where the technology was state-of-the-art, but the feeling was one of profound care. When we finally opened the doors in 2014, I stood in the center of that quiet, blue-and-cream sanctuary and felt that we had succeeded. We hadn't just built a ward; we had built a promise to our patients that even in their darkest hour, they would be treated with beauty and respect.
The Miracle in the Village
History often moves in parallel lines that seem destined never to meet. In 1977, two distinct events were shaping the future of cardiology, thousands of miles apart.
In Sevagram, Dr. Khatri, a renowned cardiologist from PGI Chandigarh, was visiting our institute. His bedside clinics were the stuff of legend. He didn't just teach us medicine; he taught us the "subtle art"—how to press a stethoscope to a chest and hear the whispered secrets of a gallop or the low hum of a failing valve. He was a master of the physical exam, a man who believed that the diagnosis lived in the patient’s story, not in the hum of a machine.
That very same year, in a sterile lab in Zurich, Switzerland, a German-born physician named Andreas Gruentzig was performing a miracle. He successfully inflated a tiny, primitive balloon inside a patient’s coronary artery, crushing the plaque and restoring the flow of life. With that single, bold act, he birthed the field of coronary angioplasty. He changed the way the world looked at heart disease forever.
It took thirty-eight years for those parallel lines to finally converge in our small village. But on February 27, 2015, the spirit of Dr. Khatri’s bedside wisdom and Gruentzig’s technical brilliance finally met in a quiet corner of central India.
***
The patient chosen for this historic first procedure was Simran (name changed), a fifty-year-old woman who had become a regular face in our wards. Simran was the human face of a shifting landscape we had long feared. While we were once a nation of infectious diseases, we were now seeing a surge in "lifestyle" ailments even in the rural heartland.
Simran was a bundle of nerves and a cocktail of pills. She was on medications for glucose, cholesterol, and blood pressure, along with nitrates to open her vessels and antithrombotics to thin her blood. Yet, her biology was outrunning our pharmacology. Her world was shrinking. She could hardly walk a city block without the crushing weight of angina forcing her to stop. She would arrive at the top of a flight of stairs huffing, puffing, and clutching her chest, her eyes wide with the fear of a heart that was slowly starving.
Dr. Udit Narang, her physician, sat her down for a heart-to-heart. He explained that the "plumbing" was simply too blocked for pills to fix. He told her that a tiny wire and a balloon could give her her life back.
Simran was terrified. The thought of a metal wire snaking toward her heart was enough to make her pulse race. But this is where the "Sevagram Advantage" came into play. Dr. Udit hadn't just studied her charts; he had treated her for years. He knew her fears, her family, and the quiet anxieties that kept her up at night. He didn't just prescribe a procedure; he offered his presence. Trust was the most important pre-medication she received. With a trembling hand, she finally gave her nod.
***
Dr. Ram Ghodeswar, our cardiologist, took the lead. I watched his hands—steady, deliberate, and calm. On the high-definition digital monitors, the procedure looked less like surgery and more like a delicate dance. He navigated the catheter to the blockage, and we held our breath as the balloon inflated, pushing the plaque back to reclaim the space for the blood to flow. Then came the stent—a tiny, gleaming metal scaffold to hold the artery open for good.
Suddenly, we saw it. It was a moment of pure physiological magic. On the monitor, the contrast dye, which had previously ebbed and trickled past the blockage like a dying stream, suddenly gushed. The blood rushed through, feeding the starved heart muscle with the oxygen it had been craving for years. It was as if a dam had burst, and life was flowing back into the parched land.
***
Even before we wheeled her back to her room, Simran looked like a different woman. The gray pallor was gone, replaced by a sense of serenity.
“I never thought it would be so quick, or so painless,” she told me later, a smile finally reaching her eyes. “I am so glad I did this here, in Sevagram. Not for a moment did I feel afraid once I entered that room.”
I asked her why. In a world of high-tech medicine and masked strangers, what made the difference?
“Because I could see the eyes I knew behind the masks,” she said simply. “I knew everyone—the doctors, the nurses, even the boy who wheels the stretcher. They all greeted me by name. That was the reason my heart was never in my mouth. My people were with me.”
***
As we cleaned up the lab, Dr. Benhur Premendran, our anesthesiologist and a proud MGIMS alumnus, turned to me. He was visibly moved.
“This is a milestone for us,” he said quietly. “Every year, hundreds of thousands of people get angioplasties in big cities and private hospitals. But the fact that we are doing this here, for the poor and the middle class, fills me with pride.”
He touched on the point that mattered most to us: the cost. In the gleaming, for-profit hospitals of the metros, a procedure like this can drain a family’s life savings. At MGIMS, we were doing it for almost a third of the price.
On that day, we proved that high-tech medicine and low-cost compassion are not mutually exclusive. We had brought Gruentzig’s Swiss invention to Gandhi’s village, and in doing so, we had kept Dr. Khatri’s legacy of bedside care alive. We hadn't just fixed a heart; we had fixed a future.
The Summit of the Mountain
The evolution of a medical department is a lot like climbing a mountain. First, you establish the base camp—that’s the day-to-day medical management, the foundation of everything we do. Then, you scale the lower peaks, bringing in intensive care units and non-invasive diagnostics. Finally, you attempt the technical ascent: the Cath Lab and angioplasty.
But there is always one peak that looms over the rest, defining the horizon of a cardiac center. That summit is Open Heart Surgery.
For decades, if a patient in Wardha needed a valve replaced or a bypass, we had to send them away. We referred them to Nagpur or Mumbai, but those referrals often felt like sentences of exile. For a rural family, a trip to a big city hospital is a logistical nightmare and a financial death trap. We wanted to change that. We wanted to prove that the highest level of surgical care didn't have to be a privilege of the urban rich. On September 4, 2018, we finally planted our flag on that summit.
***
The man who helped us cross this frontier was Govind (name changed), a forty-eight-year-old farmer from Sindi. Govind was a man of the soil, his hands calloused by years of labor. But lately, his body had begun to betray him. Simple tasks—walking to his fields or lifting a sack of grain—had become impossible.
When he arrived at Sevagram, he was a shadow of the man he used to be. He was gasping for air just from the walk to the clinic. At night, he couldn't lie flat; he felt as though he were drowning in his own skin, forced to sleep propped up against a pile of pillows. His legs were heavy and swollen, a sure sign that his heart was losing its battle to pump.
For a farmer, losing the ability to tend your land isn't just a health crisis; it’s an identity crisis. He sat in my office, his chest heaving, his eyes filled with the quiet, desperate anxiety of a man who feels his life force slipping away.
***
We admitted him immediately. The echocardiogram revealed a mechanical disaster. Govind’s heart was fighting a losing war on two fronts.
First, his mitral valve—the gateway that allows blood to move through the heart—had calcified. Instead of opening wide like a swinging door, it had turned to stone, narrowing into a tiny, rigid slit. In medical school, we call this a "fish-mouth" appearance. Second, his aortic valve was "incompetent," meaning it leaked badly, allowing blood to rush backward with every beat. His heart was essentially running in place, working twice as hard to accomplish half as much.
He needed a double valve replacement. He needed someone to open his chest, stop his heart, cut out the diseased tissue, and sew in new life.
***
This was a high-stakes debut for us. Our surgeon was Dr. Pankaj Pohekar, a young, dynamic doctor who had recently joined our team. This would be his first major "pump" case at MGIMS.
In rural India, the concept of "Open Heart Surgery" is inherently terrifying. The idea that we would stop a man's heart to fix it sounds counter-intuitive to everything a farmer knows about life. Pankaj and his team spent hours by Govind’s bedside. They didn't just talk about physiology; they talked about his farm. Once Govind understood that this procedure was the only way he would ever walk his fields again, his fear turned into a quiet, stubborn resolve.
On the morning of September 4, the operation theater was a symphony of controlled tension. To do this, we had to use the Heart-Lung Machine. It is one of the true marvels of modern medicine—a whirring collection of pumps and tubes that takes over the job of breathing and circulating blood, allowing the surgeon to operate on a heart that is still and bloodless.
Dr. Pohekar worked with superb poise. When he finally opened the heart, he called me over. "Look at this," he said. The mitral valve was exactly as we feared—a rigid, calcified slit that barely permitted a turbulent, struggling flow of blood. With steady hands, he excised the ruined valves and sutured in two metallic replacements. They were beautiful in their precision—tiny mechanical leaflets designed to click open and shut with the rhythm of life for decades to come.
***
Then came the moment that never fails to move me: the restart.
As the clamps were removed and the warm blood flowed back into the heart, we waited. The heart, now equipped with its new hardware, took over the rhythm. The monitors began to beep—a steady, strong, insistent signal. Govind was back.
Dr. Pohekar took off his bloodstained gloves and allowed himself a small, tired smile. "It’s gratifying," he whispered. "To replace those choked valves is to give a man a new lease on life. He’s going to walk long distances again."
***
Outside in the corridor, the atmosphere was thick. Govind’s son had been pacing the length of the hallway for hours. When we told him the surgery was a success, the fear in his eyes dissolved into tears.
“We had almost given up,” he confessed. “We knew he was terrified, even if he didn't say it. This has opened a new door for him.”
But there was a second reason for the family's relief, one that sits at the very core of our mission at Sevagram. Cardiac surgery is notoriously expensive. In a corporate hospital, a double valve replacement can bankrupt a farming family for three generations. It usually means selling the land, the very thing the surgery is meant to save.
However, because Govind was enrolled in the Mahatma Jyotiba Phule Jan Arogya Yojana—a state insurance scheme—and because of our commitment to keeping costs low, the entire procedure was free for him.
He walked out of our hospital a few weeks later with a new heart and, crucially, zero debt. We hadn't just fixed a valve that day; we had fixed a system. We proved that the summit of medical science could be reached even from a village in Wardha.
Success in a hospital is a fragile thing. When Govind walked home with his new heart, we felt invincible. We had scaled the peak. But the problem with summits is that the air is thin, and the footing is treacherous. As an administrator, you learn that for every triumph that makes the newspapers, there is a potential tragedy lurking in the smallest oversight. I thought we had mastered the mountain. I was wrong. Nature has a way of humbling the confident, and for me, that humility came in the form of a young mother and a battered blue file.
The Shadow on the Summit
It was a typical Thursday in my OPD. The waiting hall was a sea of people—farmers from the cotton belt, mothers with infants, the old and the infirm—all waiting for a slice of our time. In a teaching hospital, the OPD is our most vital classroom. I was mid-sentence, explaining the nuances of unexplained fevers to my residents, when she walked in.
She was twenty-four, a mother of two, with eyes that held a strange mix of vibrancy and terror. "I have a hole in my heart," she said. "Can you fix it, sir?"
She handed me a battered file, its edges warped by the monsoon rains. Inside was the paper trail of a desperate search for health: smudged ink on handwritten discharge summaries, a damp echo report, and a creased chest X-ray. Her husband stood beside her, his hand on her shoulder, his eyes searching mine for a miracle.
I examined her. Her pulse was steady, her lungs were clear, and she appeared remarkably well. But when I placed my stethoscope to her chest, her heart revealed its secret—a soft, telltale murmur and the widely split second heart sound that spoke of an Atrial Septal Defect (ASD). She had sailed through two pregnancies without knowing her heart was under strain. Now, they wanted to fix it once and for all.
***
In the hierarchy of cardiac interventions, an ASD closure is often seen as "bread and butter" surgery. Our surgeon at the time—a kind, confident man—assured the family. "It’s a simple hole," he said. "The surgery is straightforward. She’ll be home by the weekend."
That reassurance filled the room like a warm light. On the day of the surgery, we felt no foreboding. The heart-lung bypass machine took over her circulation, the surgeon opened the heart, and he sutured the coin-sized hole with precision. "I'll be done in three hours," he had told me.
Three hours passed. Then four. Then five.
The air in the hospital corridors began to feel heavy. When the surgeon finally emerged, he looked like a ghost. His voice was a ragged whisper. "I’m so sorry," he said. "The oxygenator—the machine that keeps the blood flowing—ran low. The perfusionist missed the level. Air got into her arteries. It went to her brain."
He stopped, struggling for breath. "Her heart is beating, but her brain is gone."
***
The room fell into a horrific silence. A young mother, who had walked in on her own two feet, was now "brain dead" because of a mechanical oversight—a human error that should never have happened. Her husband collapsed; the nurses wept. I stood frozen.
As the Medical Superintendent, this was my failure. I had built the theater, I had recruited the team, and I had green-lit the program. But in that moment, I realized I had built a house of cards. We had the technology, but we lacked the deep, ingrained culture of "fail-safe" checks that cardiac surgery demands.
We waived the charges. We arranged the transport. We did all the hollow things administrators do when they are trying to compensate for a catastrophe. She passed away the next day. Her husband, in a display of grace I didn't deserve, blamed destiny rather than our hands. But I knew better.
***
For weeks, I was a statue. I did not cry. I replayed the error in my mind—the drop in the blood level, the bubble of air traveling to the cerebral cortex—over and over. Then, one evening, weeks later, while sitting with my wife and my elder sister, the dam finally burst. I cried with a violence that stunned them.
"Those little girls," I sobbed. "They’ll never know their mother because of us."
That tragedy changed me, and it changed the hospital. As an administrator, I realized we were not yet ready for the relentless precision of open-heart surgery. I lacked the courage to continue. The weight of that young mother's death sat on my chest like lead.
Instead of pushing forward, I hit the brakes. I let the cardiac surgery program at Sevagram go dormant. I chose the safety of the "non-invasive" over the risk of the "cutting edge." It was a decision born of caution, but also of a deep, personal trauma.
I retired as the Medical Superintendent with that summit left unscaled. It took another year after my retirement for the hospital to find its footing and restart the program. Even then, it began in fits and starts, haunted by the memory of what had gone wrong.
In medicine, we often talk about our successes—the rankings, the awards, the "miracles." but the stories that truly define us are the ones that end in silence. I am a seventy-year-old physician now, and I have saved many lives, but the face of that twenty-four-year-old mother is the one I see when I close my eyes. We reached for the summit, but we forgot that at those heights, even a single bubble of air can be a landslide.
For a long time after that young mother’s death, I was haunted by the finality of our failure. In an ICU, when technology fails, it fails loudly and catastrophically. It leaves you feeling that medicine is nothing more than a high-stakes gamble with machines. But as the months passed and I prepared for my final year as Medical Superintendent, I realized that our obsession with "fixing" the heart had blinded us to the soul of the person carrying it.
I had hit the brakes on cardiac surgery because I feared another sudden, violent death. But in doing so, I began to look more closely at the quiet, slow deaths happening every day in our wards—the cancer patients, the elderly, the forgotten. I realized that if we couldn't always guarantee a miracle on the operating table, we could at least guarantee dignity in the hospital bed. We needed to learn that a doctor's duty doesn't end when the "cure" becomes impossible; in fact, that is often where the most important part of our work begins.
The Origami of the Heart
Nature is a master architect, but even the finest blueprints can have a flaw. Sometimes, the complex origami of the human heart folds incorrectly.
The statistics are sobering: one in every two hundred mothers will deliver a baby with congenital heart disease. For these families, the primal joy of birth is instantly eclipsed by a long, dark shadow. Some of these defects—holes in the chambers, stenosed valves, or abnormal connections between the great arteries—are serious enough to turn a newborn blue. For decades, the only answer was the scalpel. The prospect of open-heart surgery on a baby weighing only a few kilograms is enough to make any parent’s blood run cold.
But medical science has a way of evolving toward kindness. Today, we have a piece of good news that feels like a miracle: many of these defects can be repaired without ever opening the chest.
***
To perform this kind of magic in a village like Sevagram, you need three things: a well-equipped Cath Lab, a support team with nerves of steel, and a truly skilled operator. We found our operator in Dr. Abhay Bhoyar.
Abhay is a pediatric interventional cardiologist who brought back to India the wisdom he had painstakingly acquired during his training in the United Kingdom. Last month, our Cath Lab was abuzz with a new kind of energy as we asked him to take charge of these fragile lives.
Over a two-month period, a dozen babies arrived, their little hearts struggling to keep pace with the world. Under Abhay’s hands, it was a symphony of precision. We watched as he closed Ventricular Septal Defects (VSD) and Atrial Septal Defects (ASD)—the "holes in the heart." We saw him balloon open tightened valves and repair narrow aortas. The babies would arrive, have their defects fixed via a tiny puncture in the leg, spend a day or two in the ICU, and go home. Their chests were no longer heaving with the effort of breathing; they were rising and falling with unbridled joy.
***
The medicine was advanced, but the demographics remained the same. None of these babies belonged to parents who could afford a private corporate hospital. Most came from the poorest corners of our district.
These parents would arrive at MGIMS with a fragile hope and eyes filled with tears. When they left, the tears were still there—but they had changed. They were now tears of relief, the kind that come when the crushing weight of potential debt and the fear of a child's death are suddenly lifted. In Sevagram, we don't just measure outcomes in heart rates; we measure them in the quiet return of a father's dignity and a mother's peace.
***
One story, in particular, captures the essence of why we do this. Last week, a four-month-old baby girl was brought to us. Her life was already a tragedy of abandonment before it became a medical crisis. Soon after her birth, her father—a man lost to alcohol—had deserted the family, leaving the mother and the grandfather to fend for themselves.
To make matters worse, the baby was diagnosed with a Patent Ductus Arteriosus (PDA)—a persistent opening between the two major blood vessels of the heart. The mother and grandfather began a desperate pilgrimage. They took the breathless child to village clinics, district hospitals, and finally a for-profit center. Everywhere, the verdict was the same: "She needs urgent surgery, and it will be expensive."
They had no money. They had only despair. As serendipity would have it, the grandfather chanced upon Dr. Bhoyar. Abhay looked at the baby, looked at the weeping grandfather, and said simply, “Admit her.”
***
The procedure itself was a reminder of how thin the line is between life and death. In the middle of the Cath Lab, the baby’s fragile heart gave way. She suffered a cardiac arrest. The room froze. It is a moment every physician dreads—the silence of a monitor that should be beeping.
But the team didn't give up. They resuscitated her, stabilized her, and with hands that did not shake, Abhay proceeded to place the device that would plug the hole. She survived. After two days in the Pediatric ICU, the change was startling. The baby who had arrived blue and gasping for air went home a healthy, vibrant pink.
In a world that can be so harsh to the poor, some stories do have a fairy-tale ending. Sometimes, the origami just needs a gentle, expert hand to fold it back into place.
The Lifeline in the Machine
October 2007 marked the beginning of a quiet revolution at MGIMS. It wasn’t a grand, ribbon-cutting affair with flashbulbs and speeches. Instead, it was the soft, rhythmic whirring of two brand-new hemodialysis machines tucked away in a corner of our hospital.
Back then, the unit felt like a lonely outpost. We had those two machines and a single, dedicated technician named Amit. In those early days, the silence was almost unsettling; we performed maybe one dialysis a week, sometimes only one a fortnight. There were moments when I wondered if we had overreached.
But in healthcare, supply has a way of creating its own demand. As word filtered through the villages that patients no longer had to endure the long, expensive journey to Nagpur just to clean their blood, the trickle turned into a stream. By 2011, those two machines weren't just humming—they were exhausted, performing thirty-five procedures a month.
***
Early in my tenure as Medical Superintendent, I realized a fundamental truth: a million-rupee machine is nothing more than a sophisticated paperweight without the right hands to run it. Instead of trying to lure expensive consultants from the city who might not stay, we decided to grow our own expertise.
In 2012, we chose Nandini, one of our most capable nurses, and sent her for intensive training. She returned six months later with something far more valuable than a certificate; she brought back an intuitive understanding of fluid dynamics and a deep empathy for the renal patient.
That investment in human capital was the spark. Over the next decade, the surge was staggering. We went from 324 procedures in 2009 to nearly 7,000 in 2022. Today, our fleet has grown to fifteen machines, treating 600 patients every month. These aren't just statistics on a spreadsheet; they are lives tethered to our wards by a few meters of plastic tubing.
***
However, as a physician, I find it hard to romanticize dialysis. While it is a triumph of engineering, the life it offers is grueling.
Dialysis is a demanding master. It requires a patient to surrender their life to the hospital two or three times a week, every single week, without fail. It is a routine that devours time, energy, and spirit. I watch our patients arrive—physically spent and emotionally drained. The process, while life-saving, often leaves them feeling "washed out," as if the machine has taken something intangible along with the toxins.
For a rural family, it is also a financial catastrophe. Even when the procedure itself is free, the "hidden" costs are predatory. There is the bus fare to Sevagram, the loss of a day’s wages for the patient, and the loss of another day’s wages for the family member who must accompany them. It is a slow bleed of resources that can hollow out a household.
***
Operating a high-volume unit in a rural setting brings unique clinical hurdles, the most stubborn being "vascular access." To run dialysis effectively, we need a fistula—a surgical bridge between an artery and a vein.
Creating and maintaining these in a village setting is immensely difficult. We face a high failure rate and, more significantly, we operate in what I call the "Nephrology Gap." We don't have a full-time nephrologist on site. The unit is kept afloat by the heroic efforts of our nurses and technicians, overseen by our medical consultants. We manage the uremia, we fix the imbalances, but we are acutely aware that we are offering a bridge, not a final destination.
***
The ultimate tragedy is that dialysis should be a waiting room, not a permanent residence. The gold standard for these patients is a kidney transplant. Yet, in all these years, not one of our dialysis patients has moved on to a transplant.
This reflects a grim national shadow. In India, nearly 90% of renal patients die because they cannot afford long-term care, and 60% stop dialysis midway simply because the money runs out. Private hospitals charge rates that can push a middle-class family into poverty within months.
***
This is where Sevagram stands as a sanctuary. We have spent years weaving a safety net out of philanthropy and policy. We’ve been fortunate to have donors like the ICICI Foundation, who stepped in to fund new machines when our old ones were flagging.
But the real game-changer has been the Mahatma Jyotiba Phule Jan Arogya Yojana (MJPJAY). Today, roughly 95% of our dialysis patients are covered by this government scheme. It isn't perfect—the paperwork can be dense and the coverage has its limits—but it is quite literally the difference between a life lived and a life lost. It ensures that a farmer in Wardha doesn't have to sell his ancestral land just to keep his blood clean.
We have come a long way since those two lonely machines in 2007. We are keeping hundreds of people alive, but the dream remains unfinished. I look forward to the day we move beyond just maintenance—the day we can offer a definitive cure. Until then, we keep the machines humming, and we keep the faith.
The Shield of the Poor
For decades, the highest wall between a poor patient and a life-saving treatment wasn’t a lack of medical science; it was simple, cruel arithmetic. In rural India, a catastrophic illness has traditionally been a one-way ticket to poverty. I have spent a lifetime watching families sell their ancestral land, pawn their last bit of jewelry, or sign their lives away to moneylenders at usurious rates just to keep a loved one’s heart beating.
In 2012, the landscape finally shifted. The Government of Maharashtra launched a state-funded health insurance scheme—initially called the Rajiv Gandhi Jeevandayee Arogya Yojana and later renamed the Mahatma Jyotiba Phule Jan Arogya Yojana (MJPJAY). The premise was revolutionary: the state would provide financial protection to families below the poverty line for nearly a thousand different illnesses, with a cap of ₹1.5 lakhs per family each year.
When our hospital registered for the scheme in 2014, I saw it as more than just a new administrative category. To me, it was a moral tool. But as any administrator knows, a grand vision is only as good as the pipes through which it flows.
***
Implementing MJPJAY required a massive operational overhaul. We realized early on that if we left the paperwork to our already overworked residents, the system would buckle under the weight of its own bureaucracy. We needed a captain for this ship.
In 2017, we recruited Dr. Ashish Deshpande to oversee our MJPJAY cell. His mandate was clear: no eligible patient should ever be turned away because of a clerical error. We turned our social workers and data entry operators into guides. They became the bridge for uneducated villagers, helping them navigate the labyrinth of ration cards and income certificates. We wanted to ensure that the "entitlement" promised by the state actually reached the person in the stretcher.
***
The scheme became the fuel for our modernization, and nowhere was this more evident than in our Cath Lab. Suddenly, we were in a position to offer high-end angiography and angioplasty to the poorest farmers in Wardha.
Before the scheme, these procedures were a distant dream for most of our patients. Now, with a yellow ration card in hand, a farmer could walk in, receive a life-saving stent, and walk out without ever opening his wallet. This created a virtuous cycle. The patients received world-class care, the hospital received steady reimbursements, and we were able to reinvest those funds into even better equipment. It was a rare moment where the interests of the institution and the interests of the poor were perfectly aligned.
***
However, medicine is rarely as tidy as a balance sheet. We frequently encountered "overflow" cases—patients in the ICU with multi-organ failure or complex surgeries where the bill climbed well past the government’s ₹1.5 lakh cap.
In a corporate hospital, the administration would simply ask the family to pay the difference. At Sevagram, we took a different stand. We established a policy that I am still proud of today: the cap limits the reimbursement, not the care.
If a patient’s bill hit ₹2 lakhs, the hospital absorbed the extra ₹50,000. We never held a patient hostage for money. This decision cost us millions in the short term, but it earned us a currency that is far harder to come by: credibility. We became known as the sanctuary that wouldn't let a budget get in the way of a life.
***
There is, of course, a subtle danger in any insurance-driven system: the temptation to over-treat. When the government is picking up the tab, the natural barrier to ordering an extra test or a surgery disappears.
I was acutely aware of this "moral hazard." I instructed our cardiologists and surgeons strictly: perform a procedure only when the science demands it, not when the scheme allows it. We never set financial targets for our doctors. There were no "incentives" for doing more knee replacements or more angioplasties.
Yet, I must be honest—no system is entirely immune to human nature. In a teaching hospital, residents are eager to learn; they want to cut, stitch, and fix. There is always a risk that a surgeon might lower the threshold for operating on a backache or a knee because the funding is there and the "case" is interesting. We fought this constantly, trying to instill the discipline that just because a surgery is free doesn't mean it is necessary.
***
When I look back at the numbers from our Hospital Information System, the scale of the change is staggering. Between 2014 and 2022, our patient enrollment under the scheme grew by 250%. Our annual reimbursement grew from ₹23.9 crores to over ₹71 crores.
But these aren't just dry financial metrics. They represent thousands of families who kept their land, their dignity, and their loved ones. We built a shield for the poor, and in doing so, we didn't just stabilize our finances—we strengthened the very soul of Sevagram.
The Art of the Scrub
In the world of Indian healthcare, there is a certain hierarchy that everyone silently accepts. On one side, you have the "Institutes of National Importance"—the gleaming, well-funded giants like AIIMS New Delhi or PGIMER Chandigarh. On the other side, you have the rural teaching hospitals, often struggling against the tide of dust, crowds, and limited resources.
On 20 April 2018, that line blurred.
Dr. B. S. Garg and I found ourselves in a grand hall in New Delhi, standing before the Union Health Minister to receive the Kayakalp Award. The Government of India had launched this initiative to complement the Swachh Bharat Mission, creating a rigorous national competition for cleanliness, hygiene, and infection control.
When the final rankings were announced for institutes of national importance, the list read: AIIMS New Delhi, PGIMER Chandigarh, JIPMER Puducherry—and then, MGIMS Sevagram. We were ranked fourth in the country. For our 984-bed facility, tucked away in a village in central India, to stand shoulder-to-shoulder with the titans of Indian medicine was a moment of profound, quiet pride.
***
This recognition didn't fall from the sky. It was the result of a conscious, almost obsessive, focus on what I call "the invisible discipline."
In a large hospital, cleanliness is often treated as a cosmetic exercise—something you do hurriedly when you hear an inspector’s car pulling into the driveway. We wanted to change that culture. We implemented the Mera Aspataal (My Hospital) initiative, which allowed us to systematically collect feedback from the people who matter most: the patients.
We realized that for a patient, a clean toilet or a dust-free locker isn't just a comfort; it is a sign of respect. It tells them that even if they are poor, they deserve a dignified space to heal.
***
I often spoke to our nurses, supervisors, and sweepers about what Kayakalp really meant. I tried to move away from the jargon of "biomedical waste management" and speak about the daily rhythm of the ward.
I’d ask them to imagine a hospital where the day doesn't begin with a medicine round, but with a battle against the small things. It starts with the quiet removal of a cobweb in a high corner. it continues with the clearing of waste and the scrubbing of a stretcher. It involves decluttering a cupboard that hasn't been opened in years and discarding old, yellowed files that no longer serve a purpose.
We focused on the details that often go unnoticed until they fail: the availability of safe drinking water, the meticulous sorting of biomedical waste into color-coded bins, and the constant, rhythmic washing of hands. We treated the corridors, the kitchens, and the labor rooms with the same reverence as the operating theaters. In Sevagram, cleanliness stopped being a "task" and became a commitment.
***
During the assessment, the Ministry of Health looked at six specific parameters: hospital upkeep, sanitation, waste management, infection control, hygiene promotion, and overall cleanliness.
While these sound like administrative headings, they are actually the pillars of patient safety. Proper infection control means a mother doesn't leave the hospital with a fever she didn't have when she arrived. Good waste management means a needle-stick injury doesn't change a young sweeper's life forever. By aligning ourselves with these national benchmarks, we weren't just chasing an award; we were building a safer sanctuary for the 2,500 people who walk through our gates every day.
***
Perhaps the most gratifying part of the journey was the feedback we received through the Mera Aspataal portal. Patients were rating us in real-time. To see a farmer from a nearby village give us a high score for cleanliness was more rewarding than any certificate.
Competing with twenty-one massive, city-based institutions was a David-and-Goliath story. Those hospitals have thousands of staff members and budgets that dwarf ours. Yet, Sevagram rose to the occasion because our staff didn't see themselves as just "cleaners." They saw themselves as the first line of defense against disease.
For all of us, the Kayakalp award was an affirmation. It proved that discipline is not a matter of geography or budget. It is a matter of will. It showed that even in a village, you can create a world-class environment if you are willing to pick up a broom with as much heart as you pick up a stethoscope.
Chasing the Score in Seven Minutes
History is often told in decades, but sometimes the essence of an entire institution must be distilled into minutes. On 27 February 2018 — a Sunday, the kind of bright Vidarbha morning that makes you believe anything is possible — Mr. M. Venkaiah Naidu, the Vice-President of India, arrived in Sevagram to inaugurate our new operating theatre complex.
The ink was still wet on our Kayakalp citation. Four days earlier, Dr. B.S. Garg and I had stood in a grand hall in New Delhi and received an award that ranked MGIMS fourth in the country for cleanliness — behind only AIIMS Delhi, PGIMER Chandigarh, and JIPMER Puducherry. The corridors of Sevagram still carried that quiet pride. And now the Vice-President himself had come.
My task was straightforward, or so I had believed: stand before him, narrate the saga of MGIMS, and tell the story of a fifty-year journey that began with Gandhi's blessing and a handful of idealistic doctors in 1969. I had spent three evenings preparing. Thirty slides. Twenty minutes. A five-decade tapestry of service, carefully arranged.
I arrived at the venue early, ran through my opening lines in my head, and waited.
***
When Mr. Naidu walked in, the room rearranged itself around him. He was a compact, purposeful man, and he moved the way senior politicians do — as if time itself owed him a debt and was perpetually failing to repay it. He settled into his chair, looked around the room with the quick assessment of a man who has seen a thousand such occasions, and then fixed his gaze on me.
I stepped toward the podium.
He raised a hand.
"Move fast," he said. His voice was not unkind, but it left no room for negotiation. "Don't waste time. I already know the background of your institute."

27 February 2018 — seven minutes to present fifty years of MGIMS. Mr. Venkaiah Naidu is in the front row, teal jacket. The projector is running. The clock is ticking.
He glanced at his watch. Then back at me.
The room went very quiet. Somewhere behind me, I heard someone shift in a chair.
Forty years ago — as a young resident, as a nervous faculty member presenting at a departmental meeting — that look would have undone me entirely. My mouth would have gone dry, my carefully rehearsed sentences would have dissolved, and I would have stood there with thirty slides and nothing to say. But at sixty-two, something had changed. I had stood at enough bedsides, delivered enough difficult news, and navigated enough impossible administrative situations to know that panic is simply adrenaline without a plan.
I took a breath. I made a quick mental calculation.
Twenty minutes compressed into seven. Thirty slides. That is roughly one slide every fourteen seconds.
I had prepared for a leisurely fifty-over cricket match. The Vice-President had just invoked the Duckworth-Lewis method. There was nothing to do but bat.
***
I clicked to the first slide and began.
I did not linger. I did not explain. I let the images carry the weight of words I did not have time to speak. The dusty rural clinics of the 1970s, when MGIMS was still finding its feet. The first ICCU, assembled with limited money and unlimited determination. The faces of farmers who had walked into Kasturba Hospital barely alive and walked out with new hearts. The Kayakalp plaque, fourth in India. Each image held a story that would have taken ten minutes to tell properly. I gave each one fifteen seconds and trusted that a picture, as someone once observed, is worth the words you do not say.
The room was attentive. I could feel it — that particular quality of silence that means people are listening rather than merely waiting for you to finish.
Mr. Naidu leaned forward slightly on slide eleven. I noted it without breaking stride.
On slide nineteen — the one showing our dialysis unit, 600 patients a month, most of them covered by government insurance — I saw him nod. Once. Slowly.
I clicked through the final slide and looked at my wristwatch.
Seven minutes flat.
I stepped back from the podium. The room exhaled.
"Good," said Mr. Naidu. Just the one word. But in the economy of a Vice-President's vocabulary, it carried the weight of a paragraph.
***
What followed was undignified and entirely necessary.
Mr. Naidu was immediately surrounded by his security detail and whisked toward the new operating theatre complex for the formal inauguration. Protocol required that I be at the plaque before him — to receive him, to stand beside him, to speak if asked.
The problem was that between me and the plaque stood a hundred metres of corridor, a procession of television cameras, a cluster of journalists walking backwards while pointing lenses at the Vice-President, and a small battalion of local politicians who had been waiting since morning for their moment in frame and were not inclined to move for anyone.
I did not walk. I moved — sideways, forward, occasionally diagonal — through gaps that appeared and closed in the same second. I excused myself past a camera tripod. I squeezed between two MLAs who were deep in conversation and appeared not to notice me at all. At one point I found myself briefly trapped behind a television correspondent who was delivering a piece to camera with the solemnity of a man reporting from a war zone.
I arrived at the plaque, straightened my jacket, and caught my breath in the three seconds before Mr. Naidu turned the corner.
He arrived. He looked at the plaque. He looked at me — with, I thought, a slight flicker of surprise that I had beaten him there.
He picked up the ceremonial cloth and paused.
"Tell me," he said, turning to me with the directness of a man who has no patience for prepared answers, "do you have faculty living on campus? Or do you bring them in from Nagpur every morning?"
"Every faculty member lives here, sir," I said. "In the village. Among the people they serve. Some have been here for thirty years."
He considered this. "And medicines? Are you prescribing generics?"
"Every day, sir. We fight that battle every single day."
He nodded. He unveiled the plaque. He said a few words — measured, genuine, the kind of acknowledgment that a large institution might receive with fanfare but that felt, in Sevagram's quiet courtyard, like something more personal.
And then he was gone, moving briskly toward the auditorium where he would confer the International Gandhi Award for Leprosy on two doctor-researchers who had spent their careers doing exactly what MGIMS had always tried to do: taking medicine to the people who needed it most.
***
I stood in the courtyard for a moment after the convoy moved on. The cameras had followed the Vice-President. The politicians had followed the cameras. The courtyard was suddenly, briefly, empty.
It had been, I reflected, an unusual morning. I had been rebuked before I began, had compressed fifty years into seven minutes, had run through a gauntlet of television crews, and had answered two questions at a plaque while still catching my breath.
Later that evening, Ulhas Jajoo — who had missed the morning's drama entirely — called from his home.
"How did it go?" he asked.
"He gave me seven minutes," I said.
There was a pause on the line. I could almost hear him calculating.
"Seven minutes? For fifty years?"
"Seven minutes. Exactly."
A longer pause. Then, in the tone he reserves for situations that are simultaneously absurd and entirely typical of Sevagram: "And did you finish?"
"Slide thirty. Seven minutes flat."
He laughed — the deep, unhurried laugh of a man who has known you long enough to find your predicaments genuinely funny. "Of course you did," he said. "Of course you did."
***
I had started the morning fearing I would have to run a gauntlet. What I discovered instead, on a sunny Sunday in Sevagram, was something more useful: that at sixty-two, I still had a good run left in me.
The Art of the Gentle Goodbye
In 2017, an oncologist named Dr. Sankha Mitra visited Sevagram and spoke a sentence that cut through our institutional pride like a scalpel. "In India," he said, "the poor die in agony and neglect; the middle-class die in agony and ignorance; and the rich die in agony on a ventilator. No one gets a dignified, pain-free death."
It was a sobering realization. We had spent years injecting high-end technology into our wards—Cath Labs, dialysis units, and ventilators—yet we were neglecting the most basic human need: the right to a peaceful end. In a country that is ranked among the worst places in the world to die, less than one percent of those in need have access to palliative care. We had become experts at prolonging life, but we were still novices at managing the pain of the evening of one's life.
***
To address this "Nephrology of the Soul," we invited Dr. M.R. Rajagopal, the chairperson of Pallium India, to Sevagram in March 2019. Known as the father of palliative care in India, he and his team spent ten days teaching our doctors and nurses that medicine is about more than just a cure.

They didn't teach us about new machines. Instead, they taught us how to talk. We learned the delicate art of breaking bad news—how to sit in the silence of a patient's grief without rushing to fill it with medical jargon. We learned the proper use of morphine to melt away the physical agony of cancer, and we learned that compassionate care extends far beyond the hospital bed.
Dr. Rajagopal took us out of the sterile corridors and into the homes of our patients. There, among the cramped rooms and the socio-economic struggles of rural life, we saw that a disease doesn't just belong to a patient; it belongs to the entire family.
***
"Medical students must know how to ease the dis-eased," Dr. Rajagopal told us, his voice carrying the weight of three decades of experience. He spoke of the "total suffering" that families face—the poor who are sent home because "nothing more can be done," the middle class who bankrupt themselves for futile treatments, and the rich who are imprisoned in the cold, mechanical embrace of an ICU.
He challenged our young students: "When we deny access to pain relief and make people endure severe suffering, we are essentially inflicting cruel, inhuman punishment on our patients."
I watched as the message hit home. During one session, a medical student stood up, tears welling in her eyes. "This must stop," she said quietly. "We should blend cure with comfort. We must ensure we offer care that enables a person to live well, and when the time comes, to die with as much dignity as possible."
***
For a generation of doctors enamored with the power of science and the dazzle of technology, this was a vital lesson. We realized that as we reached for the "summits" of cardiac surgery and advanced interventions, we had to be equally committed to the "valley" of the end-of-life journey.
Technology is the muscle of medical science, but kindness is its heartbeat. As I sat in the auditorium, watching our students listen to Dr. Rajagopal, I felt a sense of relief. We were finally learning that being a good doctor isn't just about knowing when to start a ventilator; it's about knowing how to hold a hand when the machines are finally turned off.
The Sanctuary of Twilight

As a physician, my entire life had been dedicated to the fight. We are trained to view death as the enemy, a failure of our science, a battle lost. But my years as Medical Superintendent taught me a harder truth: there is a profound difference between extending a life and merely prolonging a death.
By 2018, I had just finished the monumental task of building our new library. I was looking forward to a period of administrative calm—a chance to breathe. But destiny, in the form of the institute’s management, had other plans. I was asked to construct a dedicated Palliative Care Centre.
I hesitated. My career was built on the pillars of Internal Medicine—curing the curable. Palliative care, the art of comforting those we cannot save, was a landscape of shadows I had not yet navigated. But as I walked the wards and saw patients with end-stage cancer tethered to machines, their eyes a well of pain and abandonment, my hesitation vanished. This wasn’t just a construction project; it was a moral imperative.
***
A dream of this magnitude requires more than just empathy; it requires capital. We found our "Architect of Compassion" in Mr. Ramu S. Deora, who stepped forward to donate approximately ₹5 crore in memory of his father, Mr. Sitaram Deora.
The catalyst was our trustee, Ms. Sarla Parekh. A force of nature with an abiding love for Sevagram, she had already funded our Medicine Department building. Her credibility was the bridge that brought Mr. Deora to our cause. With the funding secured, I dove into the blueprints. We collaborated with Mr. Ramteke, our architect, but as often happens in Sevagram, we eventually placed our trust in our own in-house engineering team. Mr. Harshal Deoda, with whom I enjoyed a long assocaiton in several buildings, and our contractor, Mr. K.P. Bardhiya, to turn drawings into reality.
***
We broke ground in June 2019. For months, the rhythmic grinding of mixers was the heartbeat of the campus. Then, in March 2020, the world stopped. The COVID-19 pandemic swept across India, bringing a suffocating silence. The skeleton of our building stood naked against the summer sky, a stark reminder of the uncertainty gripping us all.
When we finally resumed work in May 2020 under strict protocols, my perspective had shifted. The isolation of the lockdown made me acutely aware of the loneliness of the sick. I began to worry: would patients feel exiled in this new building, so far from the main hospital bustle?
That anxiety birthed a new idea. I decided to expand. We added a second floor for the Radiation Oncology department. By housing both specialties under one roof, we created a seamless ecosystem for cancer care. I also insisted on six private rooms. In a Gandhian institution, we prioritize the poor, but I knew that dignity often requires privacy, and providing options for every financial stratum was essential to our ethos.
***
I was adamant about one thing: this building must not smell or feel like a hospital. We chose a "Rose Gold" color scheme for the interiors. It wasn't just an aesthetic choice; rose gold radiates a warmth that softens the clinical coldness of medical equipment. We coordinated the walls, the curtains, and even the foldable couches for caregivers to match this palette.
To anchor the spirit of the center, we commissioned a mural for the wall behind the registration desk. It is simple but moving: a young doctor’s hand gently holding an old, withered hand. It is a promise of presence.
Outside, a miracle was taking place. I enlisted Mr. Harshal Deora, a brilliant engineer from our team, to transform the surrounding debris-strewn land. Harshal and our gardener sculpted a "step garden" filled with Tacoma, Oleander, and Bougainvillea.
In a stroke of typical Sevagram frugality, the gardener repurposed old, discarded surgical ceramic washbasins as planters. He filled these medical relics with vibrant orange and yellow flowers. Now, patients aren't greeted by concrete, but by the soothing whisper of Frangipani and Royal Palms.
***
The journey was not without its thorns. We locked horns with town planners over fire exits, eventually designing a specialized emergency staircase to transport bedridden patients safely. There was also a delicate negotiation with Mr. Deora. In his enthusiasm, he wanted his name on all four sides of the building. I had to gently explain that such an ostentatious display clashed with the simplicity of Sevagram. We compromised, placing the name prominently only on the front facade.
However, the hardest battle was with my own fraternity. Doctors are trained to fight until the last heartbeat; to many, palliative care felt like an admission of defeat. I spent hours pleading with faculty members to move terminal patients out of the noisy, terrifying ICU and into the peace of the new center. To make it more welcoming, we piped in soft music and created a meditation room for families struggling with grief.
***
On December 21, 2020, the doors finally opened. To ensure the legacy of this work, I asked my residents, Navaneeth and Fannie, to focus their MD theses on the problems of palliative caregivers. Under the mentorship of Dr. Preetam Salunkhe, they learned that medicine is as much about listening as it is about prescribing.
On that inauguration day, I sent an email to the entire faculty. I wanted them to understand that we weren't just opening a ward; we were opening a sanctuary.
From: Dr. SP Kalantri
Date: December 21, 2020
Subject: Inauguration of the Palliative Care Center and Radiation Oncology Department
Dear all,
I am pleased to announce that the construction and equipping of the Palliative Care Center and Radiation Oncology department on our campus have been completed. The building is situated 100 metres ahead of the Maternal and Child Health building and provides a picturesque view of the current Corona block.
It is a two-story building, with the ground floor comprising a registration counter, a 30-bed palliative care ward (including a few private rooms), and a small café for patient relatives to enjoy their home-cooked meals. The first floor features two palliative care OPDs, four radiation oncology OPDs, a registration and billing counter, as well as rooms for social workers and counsellors. Additionally, there is a 30-bed radiation therapy ward on this floor. The building is solar-driven and has a small garden, which provides a serene environment for both patients and caregivers.
The aim of this initiative is to provide dignified care to individuals struggling with chronic incurable diseases, and to show them that they can spend the later stages of their lives with minimal pain, misery, and agony. We hope to demystify death and ensure that caregivers and patients alike accept death as a natural part of life, and do not die alone in ICUs, surrounded by machines and strangers with tubes in all body orifices. Our goal is to promote emotional, psychological, and spiritual well-being in patients, and help them realize that they are not abandoned by their doctors, but are actively being helped.
It is undeniable that almost all cancer patients require palliative care, and it is important to introduce the palliative care team right from the beginning of the diagnosis, rather than at the end, so that they can work seamlessly with specialists to provide comprehensive care to patients. In addition, individuals with chronic incurable neurological problems, chronic heart failure, chronic liver disease, COPD, and chronic kidney disease also require palliative care. Patients struggling with cancer-related pain also benefit from palliation.
Operational Plan:
Dr. Preetam Salunkhe, assistant professor of medicine, will be the primary physician in charge of the centre. She will hold OPDs three times a week—on Monday, Wednesday, and Friday—and will also oversee all palliative care patients. She will work closely with the radiation oncology department to bring palliative care to their patients.
All departments are requested to admit or transfer patients who require palliative care exclusively. These patients will continue to stay in their units and will be rounded on a daily basis by their parent department and the palliative care centre. We encourage departments to collaborate and break down narrow silos to provide a more humane and comfortable care for patients. We will be happy to support the primary departments in this task.
We seek support from the departments of medicine, radiotherapy, surgery, ENT, ophthalmology, orthopaedics, neurosurgery, paediatrics, psychiatry, radiology, and obstetrics and gynaecology for this initiative. Without your active participation, MGIMS will not be able to run this centre.
If you have any questions, please do not hesitate to contact us. We will be happy to address your concerns.
Best regards,
SP
The Library on the Hillock
Whenever someone now praises the MGIMS library and calls it state-of-the-art, I nod politely. But in my mind I am standing beside the old Biochemistry laboratory, looking at a grey steel almirah that held thirty-five books and nothing else. Two wooden chairs. A fan that groaned more than it cooled. A slightly damp wall behind.
That cupboard was the library I first came to know. Perhaps it is because of that modest beginning that I have never been able to think of libraries as grand institutions. To me they have always felt like homes that slowly grow outward, room by room, as affection accumulates.
***
In 1969, when the college itself was young and uncertain, that single almirah was guarded with surprising seriousness by Mr NG Reddy, our first librarian, who catalogued each book as though it were precious. Deorao Taksande helped him quietly. Bhupendra Nath Das typed labels. A Nepali attendant dusted the shelves each morning.
None of them spoke about vision or facilities. They simply showed up and kept the place ready.
The library expanded almost by stealth — first upstairs, then to the hillock near Radiology — and by the time I arrived as a young man it had already become the intellectual centre of the campus. What I remember most from those years is not the size of the collection but the people who ran it. Taksande, Kusum Raole, Vijay Vairagade, Vaishali Ugale, and the attendants — Keshav Nidhekar, Mahajan, Keshav Chate, Sujata Sonar, Nanda Gosavi, Sarla Wankhede — knew every book by instinct. Mention a reference in passing and they would retrieve it before you had finished your sentence. Many had not studied beyond school, yet they possessed a librarian's memory that no software could rival.
The library functioned not because of systems but because of care.
***
When I joined MGIMS in 1982, the library quietly adopted me.
Between ward rounds and lectures, when the noise of the hospital grew too loud or a case troubled me, I would drift there without thinking. The moment I entered, the air felt different — cooler, slower, less demanding. I would pull out the BMJ or the New England Journal of Medicine and read with no plan at all. Sometimes an hour would pass before I realised I had missed lunch.
Over the years that reading room witnessed much of my intellectual growth. I prepared lectures there, marked papers there, wrote research proposals there, and occasionally sat doing nothing at all, simply enjoying the silence. The staff grew used to me. If I was not in the ward or at home, they assumed I would be at my usual desk.
I still think of two interns — Gopal Taori and Mufaddal Munim — who studied from morning till closing time, eating their tiffin at the table and leaving only when the lights were switched off. Today one works in Australia and the other in the UK. Whenever they visit, they talk not of degrees or designations but of that hall.
A library shapes people quietly. At the time I never imagined that one day I would be asked to rebuild it.
***
The turning point came not through any formal meeting but through a family conversation.
Shailaja Asawe used to visit Wardha to see her aunt, Suman Tai Bang, the Gandhian activist. She had an affectionate memory of being among the first to see Bhavana when she was born, and over the years she had become part of our extended circle — the kind of person who arrives at your home and immediately feels like she never left.
After her father, Shri Ramnarayan Manudhane, passed away, she and her siblings — Dr Nilima Raghavan, a Stanford paediatrician, and Avinash, a finance professional in New York — established the RG Manudhane Foundation for Excellence. During one of her visits I mentioned, almost in passing, that our library had outgrown itself and no longer met Medical Council requirements. I said it apologetically, the way one mentions a leaking roof to a guest.
She listened. She asked a few quiet questions. Then she said, in her direct, unhurried way: Let us build a proper one.
Soon afterwards she committed ₹2.5 crores.
I remember walking back to my office that afternoon with a curious weight in my chest. Excitement, certainly. But also the particular gravity of having been trusted. A donor's faith is not money alone — it is belief. I knew that if we failed, we would not merely lose funds. We would betray a person who had chosen to believe in us.
***
Shailaja introduced me to Sheetal Gandhi, a conservation architect from Pune. I had expected someone formal, someone who would arrive with a portfolio and a fee schedule. Instead, Sheetal arrived with questions.
She walked through the old Obstetrics and Gynaecology ward — the building that was to become the library — slowly, touching walls, measuring light, standing in doorways and looking at angles. She did not speak about what she would build. She spoke about what was already there, what could be kept, what the space wanted to become.
She knelt on the floor and began sketching. Not on paper — on the floor itself, with a chalk line, showing her team where the stacks might rise and where a reading table placed beside a particular window would catch the afternoon light. I watched her and understood, for the first time, that architecture at its best is not addition. It is listening.
***
[INSERT HERE: The image of Sheetal Gandhi and her team mapping the library on the floor — once you share it, I will provide full metadata. Insert after the paragraph ending "It is listening." This is the image that shows the library being born — not from concrete and steel but from a chalk line on a floor.]
If I am honest, those three years changed my daily life more than any administrative post ever did. I had imagined my role would be limited to supervision. Instead the library began to occupy my mind from morning till night.
My days settled into a rhythm I had never planned. Ward rounds at dawn, the hospital still half-asleep, antiseptic sharp in the corridors. By mid-morning I would be at a table with architects and contractors, arguing gently about square footage and shelf depths as though these measurements mattered as much as drug doses. After lunch I would slip a tape measure into my pocket and walk across to the stripped building — walls bare, floor dusty — and stand alone in the empty rooms trying to imagine where students might prefer to sit.
The rest of the day dissolved into small negotiations. I called the mason about unfinished plaster, the electrician about loose wiring, the plumber about leaking pipes, the interior designer about delayed furniture. Each conversation ended with the same quiet reminder: the deadline was not moving even if the work was. Once a week Harshal Deora would sit across from me with a notebook while I handed him a sheet of handwritten tasks. We would lean over it like schoolboys doing homework, deciding what could wait and what could not.
By evening the campus grew quieter. Before going home I often watered the young plants around the building, watching the dust settle on the leaves and the grass darken in the fading light. Those few minutes felt oddly calming — as though I were tending not just to the plants but to the project itself. After dinner, when the house finally slept, I returned to my desk to draft letters, adjust budgets, and run the numbers again, wondering whether we were stretching too far.
I had spent decades teaching medicine. Suddenly I was learning about ventilation ducts, electrical loads, fire exits, and toilet plumbing. Some days I felt faintly ridiculous — a physician masquerading as a civil engineer. Yet the work felt strangely satisfying, as though I were repaying an old debt to the place that had shaped me.
***
When demolition began, imagination was replaced by dust.
For weeks I watched labourers dismantle the labour room, the operating theatre, the faculty chambers, the wards — brick by brick. Walls that had witnessed births and emergencies crumbled into rubble. The pathologists downstairs protested about vibrations disturbing their microscopes. Harshal became Sheetal's right hand on the ground, solving a hundred small crises every day.
I began visiting the site daily. I stood there in a helmet, shoes coated in white dust, watching the space empty out. There is something unsettling about seeing a familiar place erased — like watching an old memory fade in front of you.
Yet slowly the new form emerged. Larger windows opened the walls to light. Cables snaked across ceilings. Shelves arrived. Desks were assembled. Godrej installed mobile compactors for decades of journals. Wi-Fi appeared at every table. A digital section took shape. When the first chair was placed and I sat on it alone in that half-finished hall, I felt a surge of emotion I had not anticipated. For the first time I could see the students who were not yet there.
***
[INSERT HERE: The exterior photograph of the library building — once you share it, I will provide full metadata. Insert after the paragraph ending "I could see the students who were not yet there." The building from outside is the reveal — the reader has followed the construction from dust and chalk lines to this.]

***
Throughout this period I kept asking colleagues and alumni what they expected from the new library. Their responses formed a kind of chorus.
Smita Singh wrote about silent zones. MVR Reddy reminded us of MCI norms. Anshu described group-study cubicles from Maastricht. Subodh proposed an e-library. Aaditya Tarnekar pleaded that classic editions of Gray's Anatomy not be discarded. Residents wanted 24-hour access. Others asked for daylight, greenery, lockers, charging points, coffee machines, digital subscriptions.
Reading those messages late at night, I understood something I had not quite admitted before. The library belonged not to any one person but to generations. I felt less like a builder and more like a caretaker entrusted with a shared memory.
***
When the building was ready in 2018, I imagined the day would be one of uncomplicated joy.
Instead it became one of the more awkward days of my administrative life.
Shailaja wished that either her father's memory be honoured or that her aunt, Suman Tai Bang — who had devoted her life to Wardha's women and children and embodied the Gandhian spirit that MGIMS claimed to uphold — inaugurate the building. Both requests felt not merely reasonable but right.
Dhirubhai, as President of the institute, preferred to do the honours himself. He was not unkind — simply firm in the view that institutional protocol should prevail.
I found myself caught between two worlds: on one side the donor who had made the library possible, whom we regarded almost as family; on the other side the head of the institution to whom I reported. The conversations that followed were polite on the surface and heavy underneath. There is a particular exhaustion in being the person in the middle.
On the day the ribbon was cut and the photographs were taken, I smiled for the camera. But I carried a quiet embarrassment. The two women who had breathed life into this project — Shailaja, who had trusted us with her family's money, and Sheetal, who had given the building its soul — were absent from the celebrations.
A library should stand for gratitude and shared effort. That day, it did not. It was a small human failing, perhaps inevitable in any institution. Yet it has stayed with me.
***
In May 2023, Shailaja Asawe passed away after a long illness.
That evening I walked through the Dr APJ Abdul Kalam Library alone. The lights were on. A few students sat studying quietly, entirely unaware that the woman who had funded the room they were sitting in had died that day. I stood near the entrance for a while and watched them — heads bent, pages turning, the soft hum of ceiling fans overhead.
Her gift had outlived all the awkwardness of inaugurations and protocols. Buildings endure longer than disagreements.
***
Today, when I walk through the hall, I see students scattered across the floor, heads bent over books, screens glowing softly, conversations hushed to a murmur. The building no longer needs my supervision. It has acquired its own life.
Yet each corner carries a memory. Here we argued about shelf height. There we worried about wiring. On that staircase I once climbed twice a day checking progress.
Sometimes I settle into a chair with the latest BMJ or Lancet, intending to read. But my eyes drift — towards the staircase we widened, the windows we cut open for light, the corners where shelves now stand. I remember walking here with a tape measure. Arguing with contractors. Scribbling lists for Harshal. Facing formal protests from colleagues when the noise of demolition rattled their laboratories and patience alike.
The building returns to me not as architecture but as days and evenings, phone calls, dust, and small negotiations that seemed endless at the time.
And then the present reasserts itself. A student turns a page. A chair scrapes softly. The ceiling fans hum.
From that grey steel almirah of thirty-five books to this bright, spacious hall — the distance seems far greater than the years that separate them. All the library really has to do — what it has done since 1969 — is offer someone a chair, a book, and the unhurried time to think.
That, in the end, is enough.
The Making of a Mural

Some works of art announce themselves with a flourish. Others grow quietly, shaped by patience, skill, and a deep understanding of place. The mural that now anchors the garden between the Medicine Department and the Registration OPD at MGIMS belongs to the latter kind. It is a work that does not shout for attention; instead, it waits for the viewer to pause, much like the figures depicted in its clay-turned-stone narrative.
The project unfolded over eight months, a period when the world—and our campus—was gripped by the uncertainties of the COVID-19 pandemic. Amidst the masks and the digital distancing, two artists, Dinesh Gudadhe and Ashok Baburao Wahiwatkar, worked with a remarkable, quiet focus. They were transforming a fleeting photographic moment into a permanent anchor of dignity for our hospital grounds.
***
The idea began with a simple question: could a long, bare wall on campus be used to create something meaningful? We initially looked at a site near the Registration OPD, but it felt cramped. A mural needs space—distance for the eye to travel and room for the story to breathe. We eventually settled on the garden between the two OPDs, a place where patients and their families naturally pause, wait, and reflect.
The artists presented four designs: a deer in a forest, a bullock cart, and a pair of swans. But the fourth stood apart. It was based on a photograph taken during a community immersion program in Dhanora, a village eight kilometers from Sevagram. In that village, our medical students don’t just study textbooks; they learn medicine at the doorsteps of rural households. That photograph—quiet, unposed, and deeply human—became the soul of the work.
***
What followed was a slow, exacting labor. More than seventy bags of clay were used to shape the figures. The process was a metamorphosis: from a pencil drawing to a clay sculpture, then to plaster moulds, and finally into the reinforced panels that form the mural today. Working outdoors, the artists battled changing weather and the physical endurance required to maintain an unerring sense of proportion on such a large scale.
The mural depicts a first-year medical student seated at the threshold of a village home. Dressed in her white apron, spectacles resting lightly on her face and a backpack slung over her shoulders, she listens. She is not diagnosing or instructing; she is learning. Beside her sits an elderly woman in a green blouse, an infant resting in her lap, meeting the viewer’s eyes. Nearby, two toddlers are absorbed in their own world, while a young man with a mobile phone represents the quiet encroachment of modern life.
To one side, a boy runs joyfully after a rolling tyre, a classic image of rural childhood that makes the mural’s laughter almost audible. The backdrop—an unplastered brick wall and unfinished steps—renders the texture of rural life honestly, without the gloss of sentimentality.
***
Technically, the work was a feat of precision. Accuracy of scale required a rigorous grid system, and the colors—earthy and restrained—were layered with acrylic paints before being sealed with a protective varnish. Hitesh Chappanghare’s expertise in casting proved invaluable, ensuring that the heavy panels were mounted with the delicacy they deserved.
The mural cost approximately ₹4.5 lakh, but its value transcends the ledger. It is a visual manifesto of how medicine is taught at Sevagram: through proximity, listening, and a profound respect for lived experience. Near the mural, we placed a line from Lao Tzu, inviting reflection rather than providing a simple explanation.
In preserving this single, ordinary moment from a sunny afternoon in Dhanora, the mural achieves something rare. It holds still the ethos of MGIMS: medicine rooted in community, where curiosity precedes intervention and humility precedes action. It ensures that even as the years pass, the meaning of that "first-year encounter" endures for every student who walks these gardens.
The MS Office: Full Circle
My own workspace evolved in tandem with the hospital, a restless migration that mirrored the growth of the institution itself. I began my tenure as Medical Superintendent in 2009, tucked away in the cavernous, high-ceilinged halls of the old hospital building. Those were the days of quiet drafts and solitary work; I sat at a weathered wooden table, often typing my own notes into the late hours, the rhythmic clack of the keys echoing through the corridor.
In 2015, the tides of renovation turned toward the Central Sterile Services Department (CSSD), and I was displaced. I moved to a tiny, hundred-square-foot cubicle within the Medicine department. It was a modest space, to say the least. During an inspection, a representative from the Medical Council of India (MCI) peered into my cramped quarters and couldn't help but mock the lack of grandeur. "Do you measure efficiency by the square foot?" I asked him, a dry smile playing on my lips. He chose to stay quiet, perhaps realizing that the weight of a superintendent's work isn't determined by the radius of his swivel chair.
***
A Poetic Homecoming
The final shift occurred in December 2020, when the MS Office moved to its permanent home. There was a profound sense of irony and homecoming in the location: we took over the very space vacated by the old library. To me, it was poetic. The hallowed hall where I had spent my youth hunched over textbooks, soaking in medical wisdom as a student, was now the bridge from which I managed the complexities of the hospital.
I took a personal interest in the design of my new chamber. Along the wall, I installed a custom open bookshelf, crafted uniquely in the shape of the letters "SP"—my own initials. It served as a functional piece of art, a reminder of the personal journey I had traveled from those early library days to the superintendent’s desk.
***
The Persistence of the Letters
When the time came for me to resign in January 2022, I prepared to hand over the keys to a new era. Dr. Poonam Shivkumar and Dr. Ramesh Pandey took over the mantle as Medical Superintendents. As I was clearing my desk, I looked up at the "SP" bookshelf and realized something that made me smile.
Their initials—Shivkumar and Pandey—formed the very same letters: S and P. Though the occupant had changed and the leadership had transitioned, the wooden alphabet on the wall remained perfectly relevant. It was as if the room itself knew that while individuals move on, the essence of the office and the service it represents remains steadfast. The letters stayed, and so did the spirit of the work.
The Emergency Room Paradox
During my tenure as a hospital administrator, no department tested my patience, resolve, and sense of inadequacy more than Emergency Medicine. It felt like an uphill battle I was destined to lose. Despite repeated attempts, the problems in the emergency department remained stubbornly resistant to reform. If I were to identify one enduring regret from my years in administration, this would be it.
The most persistent challenge was the chronic shortage of trained medical officers. In practice, we ended up with three imperfect categories of doctors staffing the emergency department.
First were residents from non-clinical departments, drafted out of necessity rather than choice. Asking them to manage critically ill patients was like forcing a square peg into a round hole. They neither had the training nor the inclination. Department heads were reluctant to spare them, and when they did, we often found pathology residents manning the emergency room at night—uncomfortable, uninterested, and unequipped. Many were simply waiting out their hours.
To plug this gap, we appointed full-time medical officers on eight-hour rotas. Some, however, had spent decades working in peripheral health facilities without updating their skills. They had grown resistant to retraining and indifferent to change.
The third group comprised freshly graduated MBBS doctors. Many signed up not out of commitment to emergency care, but to earn a modest income while preparing for the NEET postgraduate examination. Their attention was divided—multiple-choice questions on their phones competed with patients gasping for breath. Turnover was rapid. Retaining them felt like trying to hold water in a sieve.
Emergency medicine demands teamwork across disciplines. Critically ill patients rarely arrive with neatly compartmentalized problems. They come with head injuries and fractured limbs, internal bleeding and hypoxia, diabetes and hypertension—all at once. What they need is coordinated care. What they often got was a game of hot potato.
Departments passed responsibility from one to another, each insisting the problem lay elsewhere. Patients languished in the emergency department for hours—sometimes days—while negotiations played out over their bodies. Despite endless meetings and personal intervention, solutions remained temporary, cosmetic at best. It felt like trying to extinguish a fire with a garden hose.
Some moments remain etched in memory.
A young man with severe head injury arrived after a motorcycle accident. His family screamed for help. The ward was understaffed, the resident nowhere in sight. I found him asleep in a call room. When woken, he confessed—without embarrassment—that he was a pathology resident and had no idea how to manage head injuries.
Another patient with multiple fractures lay in agony. Orthopaedics refused surgery until blood pressure stabilized. Medicine declined admission until fractures were addressed. Meanwhile, the patient suffered, unattended.
A man with an acute myocardial infarction received aspirin. The cardiologist was unreachable. The resident did not know what to do next. Time slipped by. The family panicked.
A gunshot victim arrived bleeding. Surgery was called. The team was “too busy.” The family grew hostile. The resident froze.
These were not isolated incidents. They reflected systemic failures—of training, coordination, and accountability.
Compounding clinical chaos was the emotional turbulence of anxious families. Emergencies arrive unannounced, often at night, bringing panic in their wake. Relatives demanded immediate answers and instant cures. Some pleaded. Others shouted. A few threatened legal action.
Their expectations were understandable. Our responses were often inadequate.
We struggled to explain uncertainty in moments that demanded certainty. Journalists called at midnight. Videos went viral. Images of crowded wards and exhausted staff circulated freely, stripped of context. I found myself firefighting—trying to limit damage, soothe families, and defend young doctors already stretched beyond their limits.
Despite empathy and repeated explanations, situations often spiralled out of control. We listened. We reassured. We followed up. But we could not always meet expectations shaped by fear, grief, and misinformation.
Looking back, the emergency department mirrored larger institutional weaknesses—broken hierarchies, siloed departments, poor communication, and acute manpower shortages. Fixing such problems requires more than intent. It demands trained professionals, shared ownership, and sustained leadership.
We did what we could. Often, it was just enough to keep the system limping along.
I consider this my greatest professional failure—not for lack of effort, but because effort alone was insufficient.
There is, however, reason for cautious optimism. New mandates from the National Medical Council now require every medical college to develop a dedicated emergency medicine department. This structural change may finally force progress.
Yet challenges remain daunting. There are only a few hundred trained emergency physicians in India and more than six hundred medical schools competing for them—alongside private hospitals with deeper pockets. We advertised three times. Not a single applicant came forward.
Emergency medicine demands sacrifice. Few are willing.
What did these years teach me? That leadership cannot compensate for systemic shortages. That medicine, especially emergency care, is unforgiving of improvisation. And that acknowledging failure is not weakness—but honesty.
I learned, painfully, that some battles cannot be won by intent alone. But they must still be fought.
The Diminishing Likeability Quotient
One evening, My daughter Amrita once looked at me with that devastatingly clinical gaze children reserve for their aging parents.
“Papa,” she said, with a bluntness that would have made the late Vinod Mehta proud, “your likeability quotient has significantly diminished during your tenure as Medical Superintendent.”
It was a classic Lucknow Boy observation—candid, stinging, and inconveniently true.
For three decades, I had lived on a steady diet of affection. In the wards of MGIMS, I was the “good doctor”: the teacher who was accessible, the physician who listened, the colleague who lingered. I moved through the hospital corridors in a warm haze of smiles and familiar nods.
The Medical Superintendent’s chair altered that landscape overnight. It is a peculiar piece of furniture—upholstered in thorns. The moment I sat in it, my role changed. I was no longer the man who said yes to a patient’s recovery; I was the one who had to say no to a colleague’s request.
In a small, close-knit ecosystem like Sevagram, a “no” is rarely received as a professional decision. It is felt as a personal withdrawal. I sensed the change quickly. Smiles tightened. Conversations shortened. Invitations thinned. I began to feel less like a colleague and more like a fixture—functional, necessary, and quietly avoided.
One relationship, in particular, taught me how swiftly roles can eclipse history. A senior colleague I had admired since my student days had once been a mentor, almost an elder brother. Our bond had been forged long before I occupied an administrative office. But once I did, expectations shifted. He saw me as an ally who would smooth paths and bend rules; I saw myself as a custodian answerable to a hospital with limited resources and many competing needs.
When I could not oblige, it was not perceived as administrative integrity. It was read as personal betrayal. We continued to speak, but the ease was gone. What replaced it was a polite distance that neither of us named.
A similar chill crept into another relationship—with a colleague who had once been my student and later my neighbour. I had recommended her for leadership with genuine hope. I imagined a department that would move beyond laboratory walls and work shoulder to shoulder with clinicians. Policies meant to be evidence-based were experienced instead as intrusion. Boundaries hardened. Conversations thinned. What remained was a silence that spoke louder than disagreement.
The sharpest lesson came from a much younger colleague, once part of my earliest teaching years. Ambition, which I respected, collided with timing. My presence in the chair became, in his eyes, an obstruction. I did not understand this at the time. What I felt instead was an inexplicable cooling—averted eyes, conversations that stopped short.
The tension finally surfaced in a meeting where voices rose and restraint failed. I left the room with a heaviness in my chest that was physical as well as emotional. Tests later showed that my heart was sound. It was my spirit that had taken the blow.
The MS chair has a curious alchemy. It turns friends into factions. You become a manager, and in doing so, you risk losing the man. You absorb the frustrations of an entire institution. If oxygen runs low, it is your fault. If tea is cold, it is your fault. If a promotion stalls, it is your fault. You spend your days firefighting, and eventually, you smell of smoke.
And then comes the after.
In Sevagram, power is always on lease. When the lease expires, the man returns. The day I stepped down, the fog lifted with almost comic speed. Old warmth resurfaced. Conversations resumed. Affection returned without explanation, as if those strained years had been nothing more than a bad monsoon.
What surprised me most was how easily relationships healed once the chair was vacated. The disputes that had once seemed immovable dissolved into insignificance. Time, it turned out, had not damaged friendships; position had.
I learned, late in life, that the real villain is often the chair, not the person occupying it. The chair distorts vision—yours and everyone else’s. It creates a temporary amnesia of the heart.
After nearly thirteen years as Medical Superintendent, I decided in the summer of 2022 to step aside. My predecessor had served for a decade; I had already exceeded that span. Longevity, I realised, is not a virtue in itself. Institutions, like people, need renewal.
The decision was neither sudden nor easy. Administration had once energised me. I enjoyed complexity—balancing departments, negotiating crises, ensuring that patient care held steady amid uncertainty. But over time, fatigue crept in. The excitement of experimentation gave way to routine. I found myself becoming cautious, even conservative. Burnout rarely announces itself; it dulls curiosity long before it drains energy.
More troubling was the quiet distance growing between me and the roles that had first drawn me to medicine: teaching and patient care. Administrative demands crowded out time with students and at the bedside. Patients began to see me less often. Some drifted away. I could not blame them. That slow erosion of connection was the clearest signal that it was time to return to my roots.
Institutional strains added weight to the decision. Leadership structures showed signs of fatigue. Decision-making slowed. Difficult conversations were postponed. Faculty concerns often went unheard. Growth pathways stalled. Over time, talented colleagues began to look elsewhere, drawn by institutions offering clearer trajectories and greater autonomy.
The numbers reflected both effort and limitation. Admissions rose modestly over a decade; outpatient visits grew more steadily. The hospital was not failing—but it was no longer stretching itself. Institutions rarely collapse overnight. They stagnate quietly, one deferred decision at a time.
By then, it was evident to me that younger leadership was needed—people with energy, imagination, and the freedom to question settled assumptions. My staying on would not resolve deeper structural issues. It might even delay their resolution. Stepping down felt less like an exit and more like an act of stewardship.
Around that time, I encountered a line by Morgan Housel that found its way into my resignation letter:
“Those we admire most… knew when it was time to quit, time to pass the baton, time to disappear, in a way that preserved—even enhanced—their reputation.”
Leaving was painful. But staying would have been harder.
Today, as I walk the campus, the likeability quotient has returned to its natural state. We are back to being what we were meant to be—friends, healers, fellow travellers in the dusty lanes of Sevagram. The friction was the cost of the office. The relationships were the profit of a lifetime.d have been harder—to justify, to sustain, and to defend. Sometimes, the most responsible leadership decision is knowing when to step aside.
And so, I did.
Leaving on My Own Terms
By the summer of 2022, I had served as Medical Superintendent for nearly thirteen years. My predecessor had held the post for a decade; I had surpassed him in time, if not in patience. But calendars mattered less than the persistent heaviness in my gut. I was tired in a way that sleep did not cure.
Administration had once energised me. I enjoyed the complexity—budgets, people, crises that demanded quick judgement. Over time, that energy thinned. I found myself losing touch with the two things that had brought me to Sevagram in the first place: patients and students. To patients, I was no longer the physician they sought out; I was the official who was “never available” in the OPD.
My wife Bhavana noticed it first.
“These days our colleagues no longer smile in the hospital corridors. Many simply look away.”
She was right.
The daily friction of administration—saying no to colleagues, managing expectations, firefighting without pause—had hardened me. I could feel cynicism seeping in, quietly, like a leak in a boat that still appears seaworthy.
But it wasn’t only personal fatigue. The institution itself seemed to be drifting. Leadership structures were aging, succession planning remained vague, and decision-making slowed. Outside Sevagram, the world of medical education was moving fast. New institutions offered younger faculty clearer paths and greater autonomy. We were holding our ground—but no longer stretching ourselves.
The numbers reflected this stasis. Admissions and outpatient visits rose modestly over a decade, but not enough to suggest renewal. The hospital was not failing. It was stagnating. Institutions rarely collapse overnight; they decline one deferred decision at a time.
Around this period, I came across a line by Morgan Housel that struck with the force of a diagnosis:
“Nothing diminishes past success like overstaying your welcome.”
I recognised myself in that sentence. I had played my innings. Staying on would not solve deeper structural problems. It might even delay their resolution.
Months passed. Conversations with management were cordial but circular. I was reassured that I was “irreplaceable”—a word that often means “convenient.” My resolve hardened. This time, I would not negotiate with myself.
On 4 January 2023, I wrote formally to step down.
I did not argue my case at length. I stated simply that the cumulative weight of administration had begun to erode my peace and purpose, and that my family—wisely—insisted that health come before titles. I asked to be relieved within days, not months.
I quoted Vijay Merchant’s old advice: retire when people ask why, not when they ask why not.
Leaving was not easy. But staying would have been harder.
Stepping down felt less like retreat and more like stewardship. It allowed the institution the chance to renew itself—and allowed me to return to what had first given my professional life meaning.
The Sevagram Send-off
The end, when it finally came, was a study in contrasts.
On one side was the work family—the people in the trenches who keep a hospital breathing. The office superintendent, the matron, the biomedical engineers, and the pharmacy chief organised a modest farewell in the MS Office on 21 January. It was unpretentious, practical, and deeply felt.
I spoke in Marathi for nearly twenty minutes, trying to thank everyone for standing by me through the thickets of administration. I was determined not to become emotional. I wanted to leave with the stoic poise of a Sevagram boy. That resolve did not last long.
Colleagues spoke next, recalling midnight emergencies, long days that blurred into nights, and small victories that rarely made it into reports. Shaily presented me with a beautifully crafted frame—a collage of photographs from my years in office. I was deeply moved to learn that Manish, the office attendant, had stayed late into the night at the Wardha bus stand to help assemble it. Their thoughtfulness undid me.
I sent a final message to the faculty, using the cricket metaphor that had come to define how I understood the job.
***
As I walked out later that day, the contrast was unmistakable.
There was no formal send-off from the top management. No official acknowledgment from the institution I had served for four decades. The silence was unexpected. It hurt more than I had anticipated.
Yet, even that silence offered a final lesson. Institutions have short memories. They value the labour, but they have little time for the emotions of those who leave. Sweat is acknowledged; tears are not.
What endures are not official farewells, but relationships forged in the trenches. I left the MS Office behind, the designation surrendered without regret. I carried with me memories of ten thousand kilometres cycled, of countless patients seen, and of a hospital that was—if only slightly—better than I had found it.
The “SP” bookshelf remained.
The letters on the door changed.
And I was free.
The Phantom and the Anatomy Hall
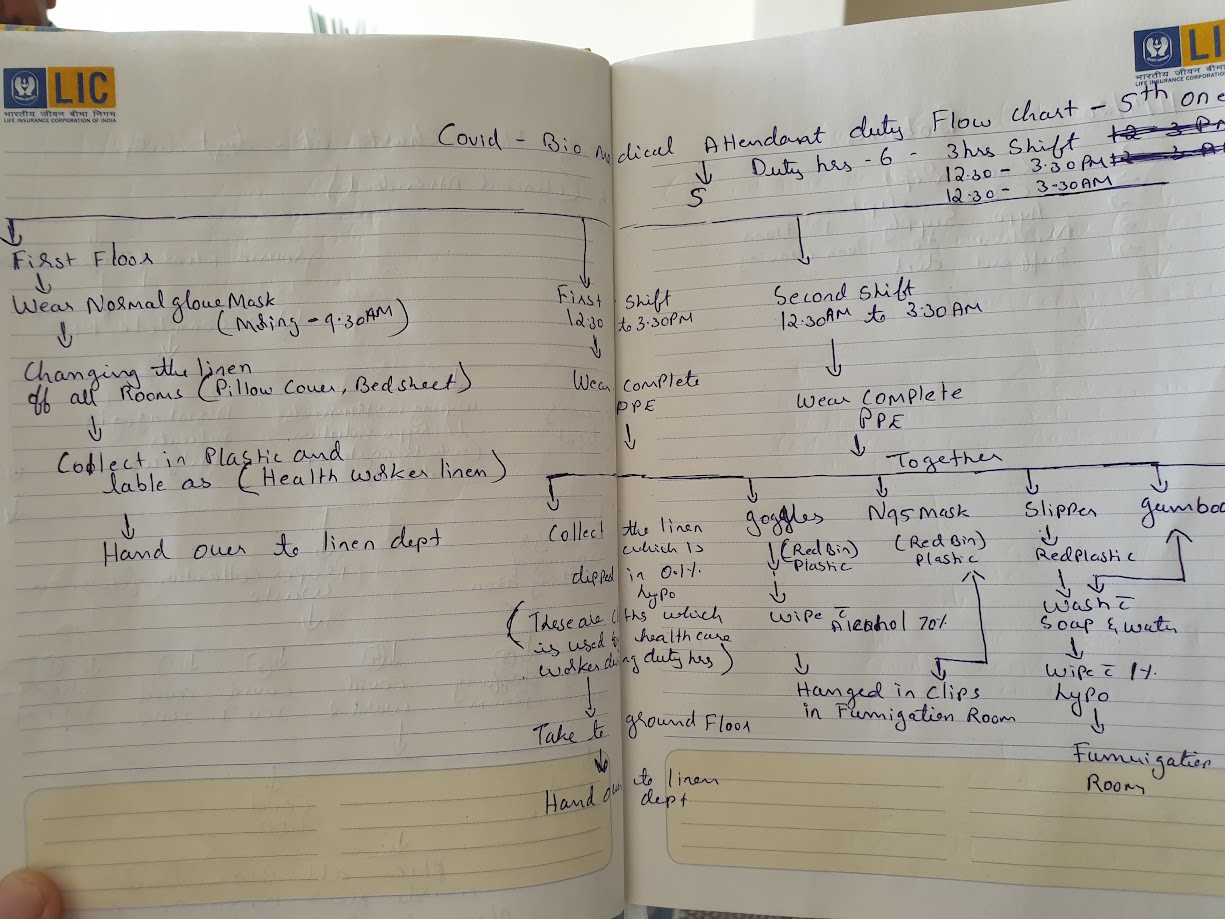
Meticulous protocols: A handwritten COVID-19 duty flow chart for hospital attendants, 2020.
In early April 2020, I stood in the central corridor of MGIMS and felt as though I were walking through a ghost town. For over a decade as Medical Superintendent, my walk through the hospital had been defined by a sensory overload: the smell of woodsmoke from the tea stalls, the cacophony of families gathered under the neem trees, and the constant, rhythmic hum of thousands of outpatients seeking healing. Now, that life had been surgically removed. The Outpatient Departments (OPDs) were eerily silent. The wards were empty. The lockdown had frozen the world outside, but for those of us inside the hospital walls, the silence was not peaceful; it was a deceptive, heavy pressure—the breath drawn before a long, sustained scream.
The Covid-19 pandemic arrived in Sevagram like a phantom. It didn't just threaten our health; it threatened our institutional identity. We are a teaching hospital rooted in the Gandhian tradition—where the "touch" of the physician and the presence of the community are the very pillars of our mission. Suddenly, that which made us human made us vulnerable. The very acts of service we had practiced for fifty years—clasping a patient’s hand, sitting close to hear a whispered symptom, performing surgeries in the middle of the night—were transformed into potential acts of biological hazard. It was a civilizational disruption that felt personal.
***
I realized that to lead through this, I needed to anchor our fear in structure. I convened an emergency meeting of all department heads in the Anatomy Lecture Hall. The choice of venue was accidental but became deeply symbolic. There we were, surrounded by the silent teachers of human structure—the skeletons and preserved specimens that represent the absolute certainty of medical science—while we tried to decipher a microscopic invader that was dismantled human certainty in real-time.
I looked at the faces of my colleagues—Subodh Gupta, Sumedh Jajoo, Dhiraj Bhandari, and the senior nursing supervisors. These were veterans who had managed chikungunya epidemic in 2007 and cholera outbreaks without flinching. Yet, in their eyes, I saw a reflection of my own uncertainty. The fear was visceral. It wasn't just the professional fear of a rising mortality rate; it was the primal fear of the unknown. Would we have enough masks? Would the ventilators hold? And the question that haunted every staff member: If I go into that ward today, am I carrying death home to my children or my elderly parents tonight?
"Our fight will be driven by science," I told the room, standing at the podium. I tried to project a voice that didn't betray the knots in my stomach. "We will not be governed by anecdotes, we will not be governed by social media rumors, and we will not be governed by fear. We will build a fortress here, but it will be a fortress of evidence."
***
Our first major step was a kind of logistical surgery. We knew the biggest danger was letting infected patients mix with the vulnerable. A standard hospital layout was a trap. So, my team proposed a tough plan: we would empty the entire old hospital building—the historic home of Surgery and Orthopedics—and turn it into a dedicated Covid Block.
It was a massive job. We had to move entire departments and relocate patients overnight. But the old building had a hidden advantage. Its layout of private rooms and separate wings was perfect for the strict routine of putting on and taking off PPE. We divided the space into a 'Red Zone' for patients and a 'Green Zone' for staff, creating a boundary that felt less like a hospital corridor and more like a front line
We also moved our screening outdoors. To keep the virus out of the building, we set up a makeshift open-air OPD in the long corridor between the Medicine department and the registration area. We realized the open air was actually our ally; natural ventilation was far safer than air conditioning, which could simply circulate the virus
***
"In those early weeks, my desk wasn't covered in files anymore. It was covered in lists of our new 'gold': N95 masks and PPE kits. I watched senior surgeons—men who had done thousands of operations—holding a simple face mask with the kind of deep respect usually saved for a delicate surgical tool.
"I recall the intense debates about using PPE wisely. Everyone—from technicians to sweepers—wanted to wear full 'astronaut' suits for every task. We had to balance their fear with the hard reality that supplies were running out everywhere. We had to teach our staff that science—not just layers of plastic—was their best protection."
***
As Medical Superintendent, I was stuck in my office, far from the bedside, yet I felt every ripple of fear from the wards. I remember the young residents and nurses preparing for their first Covid shifts. Many were barely out of their teens. I saw the red marks of tight masks on their faces, and I saw them weeping quietly in the locker rooms as they pulled on their protective gear.
The heat in Wardha in April and May is legendary—it is a dry, suffocating furnace that regularly touches 45°C. Under those non-breathable plastic PPE suits, the temperature was even higher. Dehydration was immediate; exhaustion was absolute. Yet, the physical discomfort paled in comparison to the emotional toll of what we were being forced to practice: "No-touch medicine."
For a doctor, touch is everything. But suddenly, we were forced to keep our distance. We listened to lungs through layers of plastic and spoke to gasping patients from behind glass. Later, to be honest, we stopped using our stethoscopes altogether. It felt cruel. We were caring for the most isolated people on earth, yet we were forbidden from offering the simple comfort of a hand on a shoulder. Fear was everywhere—in the canteen, in the labs, and in the silence of the ride home
And yet, I was far from the battlefield. I was sixty-four. Because of my heart condition, I was advised to stay away from the wards to save my own skin. I felt a deep, gnawing guilt. Was it right to ask young doctors to work without fear when I was safe in my office? It took time to make peace with this. Eventually, I realized my fight was not at the bedside, but at the desk—managing the chaos, enforcing science, and ensuring we used drugs rationally.
We were preparing for a war we couldn't yet see. But in the Anatomy Hall, we made a pact. We decided that while we fought the virus, we also had to fight to keep our humanity. We would adapt, we would improvise, and we would struggle—but we would never abandon the discipline of care.
The Battle for the Medical Soul
HCQ and the Mirage of Miracle Cures
While we were physically dragging beds into the old hospital building and fortifying our "Red Zones," a second, more insidious front was opening: the battle for the medical soul. In the early weeks of 2020, the vacuum of knowledge was being filled by a toxic mixture of desperation, political grandstanding, and pharmaceutical opportunism. As Medical Superintendent, I realized that my most difficult task would not be procurement of masks, but the procurement of truth.
The atmosphere in the global medical community had become feverish. Across the world, doctors were "panic-prescribing." The logic was seductive: “In desperate times, we cannot wait for trials. We must do something.” But at Sevagram, we viewed this logic as a trap. We knew that doing "something" without evidence was often more dangerous than doing nothing at all.
***
The Hydroxychloroquine Mirage
The first major contender for a "miracle cure" was Hydroxychloroquine (HCQ). It was a drug I knew well—an old, reliable workhorse for malaria and autoimmune diseases like lupus. Suddenly, it was being hailed as a magical shield against the coronavirus. The Indian Council of Medical Research (ICMR) had recommended it as a prophylactic for healthcare workers, and the President of the United States was endorsing it from the White House briefing room.
The pressure on me was immense. Staff members looked to me for the green light to start taking the pills. Families of patients begged for it. Even within our own faculty, there were voices arguing that we were being "too rigid" by waiting for data. But I sat in my office, late into the night, scouring the preliminary reports. The "evidence" was anecdotal, thin, and riddled with bias. We were witnessing the birth of a miracle through sheer repetition rather than rigorous proof.
I realized then that Sevagram had to take a stand. I reached out to my colleagues—Sahaj Rathi, Ashwini Kalantri, and Pranav Ish. We decided to voice our dissent not on social media, but in the highest court of medical opinion. We wrote a letter to The Lancet Infectious Diseases, warning that "scientific reasoning cannot be abandoned citing desperate times."
When our letter was published on April 16, 2020, we felt like a lonely outpost in a stormy sea. We argued that the blanket endorsement of HCQ was a gamble with public health. We were mocked by some as being "armchair critics" while others were "fighting on the frontlines." But for us, the frontline was the science. History, eventually, would prove us right—the drug offered no benefit and carried real risks to the heart. But in that moment, it was a battle for the very soul of how we practice medicine.
***
The War on "Irrational Cocktails"
As the first wave swelled, the list of "miracles" grew longer and more expensive. After HCQ came the tsunami of Azithromycin, Ivermectin, Zinc, Vitamin D, and eventually, Convalescent Plasma. It was as if the medical world had forgotten a century of progress and returned to the days of alchemy.
I watched with dismay as prescriptions from across the country—and even from within our district—became "cocktails." Patients were being loaded with five or six unproven drugs simultaneously. This wasn't healthcare; it was the monetization of fear. Pharmaceutical companies were prospering on the back of flawed, small-scale trials that wouldn't have passed a first-year medical student's scrutiny in normal times.
I remember a particularly heated debate regarding Favipiravir. It was marketed as a game-changer for mild cases, yet a full course cost ₹12,500—a staggering sum for the farmers and laborers who came to Sevagram. When I looked at the data, the drug shortened a fever by barely a day and had no impact on viral load or mortality. It was a classic example of a "low-value" intervention being sold as a life-saver.
***
The Poet as a Shield
In June 2020, reaching the end of my patience with traditional academic rebuttals, I turned to a different weapon: satire. I realized that when people are gripped by fear, data often bounces off them, but irony can sometimes pierce through. I wrote a poem in the voice of Favipiravir:
"My name is Favipiravir, I have made my mark In the world of Covid, I am a new patriarch... So what if you can’t locate me in Pubmed Haven’t I really painted the entire country red?"
I posted it on Twitter, which had become my digital "pulpit." The poem went viral, sparking both laughter and outrage. But underneath the rhyme was a serious administrative policy: Sevagram would stand alone. We made a collective decision that our hospital would not use these "magic bullets" unless they were part of a sanctioned, high-quality clinical trial. We refused to be part of a system that sold false hope to the poor. We stayed the course with oxygen, steroids (when appropriate), and anticoagulants—the boring, evidence-based basics that actually saved lives.
***
The Twitter Front and New Alliances
This stand for evidence-based medicine brought me into a new world of "Digital Public Health." I began connecting with a network of brilliant investigative journalists and activists—Priyanka Pulla, Rema Nagarajan, and Malini Aisola—who were digging into the regulatory failures that allowed these drugs onto the market. I found a kindred spirit in Dinesh Thakur, the whistleblower who had exposed fraud in the generic drug industry.
Together, we tried to build a dam against the flood of pseudoscience. My roles as Medical Superintendent and as an advocate for the poor were now one and the same. To protect my patients from financial ruin, I had to fight the very protocols being pushed by the state. It was an exhausting, often lonely journey, but it reinforced the core philosophy of MGIMS: we serve the patient, not the pharma company.
As the months passed, the "silent corridors" of the first wave were replaced by the "noisy war" of the second. But because we had fought the battle for the medical soul early on, we entered the next phase of the crisis with our vision clear. We knew what worked, and more importantly, we knew what didn't. We were ready for the oxygen crisis, not with magic pills, but with the discipline of truth.
The War Room
As the first wave of 2020 began to crest, my daily life as Medical Superintendent underwent a profound transformation. I was no longer just managing a hospital; I was being drafted into the strategic defense of an entire district. The "War Room" was no longer a metaphor—it was a physical reality located in the District Collector's office in Wardha.
I found myself stepping out of the familiar, sterile comfort of my wards and into the wood-paneled, high-stakes nerve center of the district administration. It was here that the abstract guidelines from New Delhi and Mumbai had to be translated into survival strategies for the people of rural Maharashtra. I had the privilege—and the immense responsibility—of working closely with two dynamic District Collectors, Mr. Vivek Bhimanwar and later Ms. Prerna Deshbhratar. These were administrators who understood that in a pandemic, a bureaucrat without a doctor is blind, and a doctor without a bureaucrat is powerless.
My role evolved rapidly from being a physician-administrator to becoming a key advisor for the district’s entire healthcare strategy. I spent more time at the Collector’s office than I could count, attending bi-weekly review meetings that often stretched into the late hours of the night. We were frequently joined via video link by the Chief Minister and senior health officials.
In these meetings, the atmosphere was a mix of exhaustion and adrenaline. We were tracking the movement of migrant workers, the availability of quarantine centers, and the terrifyingly slow arrival of testing kits. Working in tandem with the Civil Surgeons, Dr. Purushottam Madavi and Dr. Sachin Tadas, we had to build a unified front. Recognizing the need for a singular, disciplined protocol, I was appointed to chair the expert committee responsible for formulating the rules for Covid-19 diagnosis, prevention, and management for the entire Wardha district.
This committee brought together the best minds from across the region—physicians and anesthesiologists from JN Medical College and the Civil Hospital. Our task was to create a "Bible" of treatment that every clinic, private practitioner, and government facility would follow. It was a massive exercise in consensus-building during a time when everyone was panicking.
***
The toughest part of my role in the War Room was not fighting the bureaucracy; it was fighting the "tsunami of irrationality." Even as I sat in these high-level meetings, I was dismayed to witness the rapid spread of "panic prescribing" across the district. Driven by an understandable but dangerous urge to "do something," many physicians were handing out drug cocktails that had no scientific basis.
As the chair of the expert committee, I had to be the "No-Man." While other districts were scrambling to procure Favipiravir or Ivermectin, I stood firm. I stood before the Collector and the health officials and argued that we must not waste public funds on "magic bullets" that didn't work. It was a lonely position. Private hospitals were under pressure from wealthy families to provide "the latest drugs," and here I was, representing the largest hospital in the district, saying "No."
At Sevagram, we made a conscious, collective choice: our treatment protocols would be dictated by high-quality global trials (like the RECOVERY and SOLIDARITY trials), not by pharmaceutical marketing or anecdotal social media posts. We admitted nearly 5,000 Covid patients over the course of the pandemic, and we steadfastly refused to use the controversial "magic bullets" that were bankrupting families elsewhere.
***
The pressure regarding Remdesivir was perhaps the most intense administrative challenge I faced. The public viewed it as a life-saver, a "divine vial" that could snatch a patient from the jaws of death. The reality, as shown by the data, was far more modest: it didn't reduce mortality or the need for ventilators.
While the rest of the country was seeing frantic queues and black-marketing of Remdesivir, Sevagram took a contrarian stand. From March 2021, we reduced our usage of the drug by 90%. We used it only selectively for a very specific window of patients. This decision saved our patients lakhs of rupees and spared them unnecessary hepatic and cardiac toxicity.
Our approach to steroids was equally disciplined. We knew from the RECOVERY trial that steroids were a double-edged sword: they were a miracle for hypoxic patients on oxygen, but a disaster for those with normal oxygen levels. We fought a constant battle against the "steroids for everyone" approach that was rampant in the community—a practice that, as I feared, would later contribute to the horrifying outbreak of "Black Fungus."
***
My role in the district governance culminated in a very public declaration of our philosophy. In an interview with The Indian Express on June 9, 2021, I stated clearly that evidence-based healthcare was the cornerstone of Sevagram’s treatment. "We refrain from resorting to anecdotal evidence or promotional research," I told the press.
Working with the administrators of Wardha was a testament to the power of a "War Room" that actually listens to science. We proved that in the face of a terrifying new disease, the most effective weapon we had was not a new drug, but the discipline of the scientific method. We didn't just manage a crisis; we managed to keep our integrity intact while doing so.
As we moved toward the peak of the second wave, the "War Room" conversations shifted from drug protocols to something even more fundamental: the very air our patients breathed. The oxygen crisis was coming, and the governance structures we had built were about to be tested to their breaking point.
The Oxygen Crisis
On May 10, 2020, when we admitted our first COVID-19 patient to MGIMS, we were innocent. We thought the battle would be fought with PPE, N95 masks, and the strategic deployment of ventilators. We were wrong. The pandemic was not a war of complex machinery; it was a war for a single, elemental gas.
For decades, oxygen in a hospital was like water in a tap or electricity in a socket—a boring, invisible utility that simply existed. You turned a knob, and it hissed. But as the first wave swelled into the tsunami of the second, that hiss became the soundtrack of our nightmares. Oxygen stopped being a utility and became the most precious commodity on earth. It was the only drug that mattered. Without it, the sophisticated antiviral cocktails were just expensive urine, and the ventilators were nothing more than noisy bellows.
***
The nadir of this crisis—the moment that is etched into my cortex—arrived on a scorching afternoon in April 2021. The second wave was at its zenith. We had expanded to nearly 400 COVID beds, and every single one of them was occupied by a human being struggling to perform the most basic act of living.
I was in my office, buried under a mountain of mortality reports and supply chain logs, when Alpesh Raut, our biomedical engineer, walked in. In a hospital hierarchy, engineers usually wait to be summoned. Alpesh didn’t knock. The look on his face—a mixture of terror and resignation—told me the news before he opened his mouth.
"Sir," he said, his voice tight. "We have less than thirty minutes of oxygen left in the main manifold. The truck from Nagpur is stuck."
Thirty minutes. In a normal world, that is enough time to drink a cup of tea or read a newspaper editorial. In a COVID ward, it is an eternity of silence waiting to happen. If that pressure dropped, the alarms would scream in unison, and then, they would stop.
What followed was a blur of frantic, high-stakes theater. I was on the phone with the District Collector, the transport authorities, and the oxygen suppliers. My voice swung between the professional baritone of a Medical Superintendent and the high pitch of quiet desperation. We began moving jumbo cylinders across the campus like chess pieces, cannibalizing one ward to keep the ICU alive for just five more minutes.
After thirty minutes that felt like a lifetime, a truck carrying 120 cylinders rumbled through the hospital gates. It brought relief, but it was a fragile one. Those 120 cylinders would last us barely twelve hours. We were no longer planning for the future; we were living in twelve-hour increments of survival.
***
It became painfully clear that this hand-to-mouth existence—begging for trucks and praying for traffic clearance—was not a strategy. It was a gamble with human lives.
On May 21, 2021, the solution arrived not via a government circular, but through a WhatsApp message. It was from Madhukar Pai, a global health leader in Canada. He asked if I could join a digital meeting to discuss the situation in rural India.
I was exhausted. It was late, and I had spent the day fighting fires—metaphorical and literal. But the earnestness in Madhu’s message made me open my laptop. The next morning, bleary-eyed, I spoke to a group called IndiaCovidSOS and TMC Navya. I didn’t use jargon. I told them about the quiet desperation of Sevagram. I told them how my residents were running between buildings to check pressure gauges, and how we were fighting a 21st-century virus with 20th-century logistics.
The response was swift, efficient, and devoid of the red tape that usually strangles such initiatives in India. Dr. C.S. Pramesh, the Director of Tata Memorial Hospital, replied with the kind of directness that saves lives: "SP, we have a commitment for a 600 LPM oxygen generator for your hospital."
It wasn't just a promise; it was a logistical feat. This was the "invisible army" of the diaspora working in sync. FedEx and Air India operated flights bringing supplies that were then distributed to 88 locations across the country. We were one of them.
***
On July 5, 2021, the AirSep oxygen generation plant was installed at MGIMS, funded by Community Partner International.
Standing next to it, hearing the hum of its compressors, I felt a strange sense of peace. With a capacity of 600 liters per minute, it was the equivalent of receiving a hundred jumbo cylinders every day, forever. We were no longer waiting for a truck from Nagpur. We were creating our own breath from the very air of Sevagram.
We didn't stop there. The crisis had exposed the folly of relying on cylinders—those heavy, dangerous, inefficient steel torpedoes. We invested ₹28 lakhs to extend centralized copper pipelines to 150 beds across the Neuro ICU, Surgery ICU, and Emergency blocks. We repaired leaks with the obsession of a watchmaker.
The dividends were immediate. Before COVID, we consumed 90,000 cylinders a year. By fixing our infrastructure and generating our own gas, we halved our dependence on external suppliers. We became efficient not because we wanted to save money, but because we had looked into the abyss of running out.
***
Looking back, the "Oxygen Summer" taught me that resilience isn't just about courage; it's about plumbing. It taught me that while doctors treat patients, it is the engineers and the supply chain managers who save them.
The 30-minute warning from Alpesh Raut still wakes me up sometimes. But then I remember the hum of the plant behind the Medicine Department, generating life out of thin air, and I go back to sleep. The hiss is no longer a threat. It is the sound of a hospital breathing.
While we fought the logistical battle for oxygen, a different war was raging online against misinformation : The Digital Resistance.
The Architecture of Care
As the Medical Superintendent, much of my time was spent on the "macro" of the pandemic—oxygen logistics, district guidelines, and drug protocols. But the true story of Sevagram’s survival was written in the "micro" of the wards. To understand how we survived, one must look through the fogged goggles of a nurse or a junior resident.
I remember speaking at length with Dr. Jwalant Waghmare, the Head of Anatomy who stepped out of the dissection hall to become a nodal officer for nearly six months. He was our eyes and ears on the ground, identifying problems that were invisible from an administrator’s desk but catastrophic for a patient’s experience.
***
One of the earliest difficulties was unexpectedly simple: patients stayed on. Even after recovering from COVID-19 and becoming asymptomatic, many were terrified to return to villages where they might be shunned. This "bed-blocking" frustrated new admissions and exhausted a staff that was already stretched thin.
We also faced the rigidity of our own protocols. Early on, any surgical patient who tested positive—even if they were clinically stable—was transferred to the COVID ward at midnight. These transfers were chaotic and disrupted care. Dr. Waghmare and his team made a pragmatic, humane decision: we stopped the midnight transfers. We asked each surgical unit to earmark six beds in their own wards for COVID-positive patients who didn't need oxygen. This single decision reduced unnecessary movement and eased the crushing pressure on the dedicated COVID block.
Inside the wards, the atmosphere was a pressure cooker. Tensions occasionally surfaced between the nursing staff and newly inducted residents. These young doctors, often overwhelmed by the workload and the terrifying mortality rates, sometimes expressed their frustration poorly. Dr. Waghmare’s counsel to the nurses was simple but profound: "Remember, they are still learning how to function under the weight of death." That empathy defused more conflicts than any official memo ever could.
***
If the residents were the infantry, the nurses were the fortresses. I often recall my conversations with Ms. Bharti Kamble, a senior nurse who managed the COVID wards from April 2020 to August 2022. She saw the transition from a modest 10-bed unit to a massive 250-bed operation.
In those early days, Bharti and her team were the primary instructors in the "ritual of protection." They spent hours training everyone in the precise art of donning and doffing PPE—a ritual where a single slip-up could mean bringing the virus home. She spoke of the young nurses who would cry quietly while taping their gloves, gathering the courage to step into the ward.
The physical conditions were brutal. In the oppressive heat of Wardha, the non-breathable PPE was a sauna. I saw nurses collapse from dehydration and exhaustion. Their goggles would fog, their vision would blur, and their masks would slip under the weight of sweat. In that state, even simple tasks like setting up an infusion pump or finding a vein became monumental challenges.
***
Fear shaped behavior in unexpected ways. In the beginning, many were so terrified of the virus that they practiced "no-touch" medicine to an extreme. We had to rely on veterans like Benhur Premendran, our Professor of Anaesthesiology, to demonstrate that a simple gown and mask—used correctly—were enough. He had to show them it was safe to touch the patient.
Errors were inevitable in a system pushed to its limits. Many faculty members from preclinical departments, who hadn't stepped into an ICU in years, were suddenly managing ventilators and infusion pumps. I remember the story of a staff nurse’s husband who developed severe diarrhea after a resident, in a moment of sheer exhaustion, mistakenly prescribed Dulcolax instead of Paracetamol. It was a stark reminder of how thin the margin for error had become when sleep was a luxury.
***
As MS, I made protecting these frontline workers my absolute priority. We secured PPE and N95 masks when the rest of the country was running dry. We ensured that if a staff member fell ill, they had priority access to the best beds and ventilators we had. We couldn't prevent them from getting sick, but we could ensure they weren't abandoned.
Looking back, what stands out from those ward visits isn't a series of flawless medical interventions. It was the collective endurance. We learned while doing. We corrected course repeatedly. We stopped ordering repeat RT-PCRs before discharge once we realized it was unnecessary, freeing up beds faster. We eventually relaxed the rules to allow one relative to stay with a patient—realizing that the psychological comfort of a family member was as important as any drug we could prescribe.
In the end, it was not the protocols that sustained us, but the patience, the trust, and the unspoken understanding that while perfection was impossible, abandonment was not an option.
The Heavy Toll
By late April 2021, the second wave had reached a peak so relentless that death had become a constant companion in the halls of MGIMS. There is no administrative manual for losing a patient nearly every hour. In normal times, a death in the ICU is a singular tragedy that stops the clock. In the summer of 2021, the clock didn't just stop; it seemed to shatter.
I remember April 6, 2021, with a clarity that still brings a chill. Within twenty-four hours, we lost twenty-six patients. The hospital was suspended in a state of stunned motion. ICU doctors moved swiftly, filling out death certificates until their hands cramped. Nurses worked without pause, completing the overwhelming administrative formalities that follow a passing. Each death set off a frantic chain of communication: the nurse informed the supervisor; the supervisor tracked down the family; the nodal officer coordinated with the district administration for the hearse van.
In March 2020, the government had issued strict guidelines for handling bodies. It was a sterile, uncompromising process: body bags, 1% hypochlorite decontamination, and leak-proof plastic. Families were permitted to view the body from a distance, but the rites were performed by hospital attendants at the crematorium. The body was never handed over.
During that peak in 2021, the heat in Wardha touched forty-five degrees Celsius. Our hospital attendants, dressed in full, non-breathable PPE, worked for six hours at a stretch without a drop of water. They would carry as many as six bodies at a time in a single hearse van to the cremation grounds. It was a brutal, grueling service. We tried, within these impossible constraints, to ensure that every life ended with some semblance of dignity, but the sheer volume of loss pushed our systems to the breaking point.
***
In such an atmosphere of exhaustion and alarm, errors—however painful—became inevitable. On that same evening of April 6, our nodal officer received word that a patient named Gajanan (name changed) had died. Following protocol, we informed the son.
The response was immediate and furious. "I spoke to my father just a minute ago," the son shouted over the phone. "He is alive! Let me speak to him again!"
He called his father’s mobile. The phone rang. The old man answered. He was, indeed, alive.
It emerged that another patient—Ganpat—had passed away. In the cacophony of monitor alarms, muffled speech through N95 masks, and hurried handovers, a supervisor had misheard the name. By the time we realized the mistake, some relatives had already traveled five kilometers to the cremation ground, only to discover that the body awaiting rites was not their father.
Later that day, a similar mistake occurred at the cremation ground where attendants unpacked four bodies from a hearse, only to find that none matched the families waiting there. The scene was one of pure, unadulterated distress. It was a moment of deep administrative shame and human heartbreak.
***
The volume of death had overwhelmed our existing checks. Goodwill was no longer enough. That night, despite my own exhaustion, I instituted a new, rigid rule: The Rule of Dual Verification. No body would be moved from a ward unless two independent supervisors verified the patient’s identity, thumbprints, and destination. Only after this dual confirmation would the nodal officer be informed.
We apologized repeatedly to the families. It took hours of patient listening for the anger to subside. We learned a painful lesson: when compassion is stretched to its absolute limit, it must be anchored in even stricter discipline.
As the last body was taken away that night, a heavy quiet descended on Sevagram. There was no sense of "victory" in having fixed the process—only a profound sorrow and a fragile sense of order restored. We learned that even in the midst of a once-in-a-century plague, care demands meticulous attention until the very last moment. Dignity did not come easily; it had to be defended, mistake by mistake, process by process.
The Epidemic Within
Just when we thought we had finally begun to understand the rhythm of the virus, it threw a new, terrifying curveball at us. In mid-2021, as the second wave of COVID-19 was supposedly receding, the clinical picture shifted. Patients were no longer coming to us just struggling for breath; they were complaining of a dull, sinister pain behind their cheekbones and around their eyes. Some presented with blurred vision, others with black crusts forming inside their nostrils.
We realized with horror that we were witnessing the start of an epidemic within the pandemic: Mucormycosis, colloquially known as "Black Fungus."
This was not a simple infection. Caused by a group of molds called mucormycetes, it is an aggressive invader that attacks the sinuses and facial bones, often eating its way into the eye socket and toward the brain. If left untreated, it is nearly 100% fatal. If treated late, the cost is often the surgical removal of the patient's eye or jaw.
The first tremors of the "Black Fungus" epidemic didn't arrive in the form of a patient at our doorstep, but as a warning from the neighboring state of Gujarat. Priya alerted me to a disturbing spike in Mucormycosis cases there, connecting the dots that many were missing: this wasn't just a fungal infection; it was the wreckage left behind by uncontrolled diabetes and the aggressive over-use of steroids. It was a canary in the coal mine, signaling that the "panic prescribing" of the second wave was beginning to extract its delayed and terrible price.
The physiology was damningly simple, yet the implications were catastrophic. By flooding diabetic patients with high-dose steroids to treat mild Covid, doctors were essentially rolling out a red carpet for the fungus. We realized that we were facing a man-made disaster—a secondary epidemic fueled not by the virus, but by our own medical hubris. The solution, therefore, couldn't just be antifungal drugs, which were already disappearing from the shelves; it had to be aggressive prevention. We needed to stop the fire before it started.
We didn't wait for national guidelines or bureaucratic approval. Priya Smathkumar from Tata Memorial Hospital, Mumbai proposed a rapid counter-attack: we would create comprehensive patient education materials on Mucor prevention and deploy them within twenty-four hours. It was a race against ignorance. In the midst of clinical chaos, we pivoted to public health pedagogy, designing simple, vernacular guides to warn patients about blood sugar monitoring and the dangers of self-medication. It was a small, unglamorous intervention, but in a pandemic defined by helplessness, the ability to arm our patients with knowledge felt like our most potent weapon.
***
As I told journalist Maryn McKenna for Scientific American in May 2021, "The black fungus has painted the country red." But the question we had to answer as administrators and clinicians was: Why India? And why now?
We discovered that this was a man-made disaster born of a deadly collision. India was already the "Diabetes Capital of the World," and mucormycosis was a known, albeit rare, risk for those with uncontrolled blood sugar. When the pandemic hit, this vulnerability met a trigger: Steroids.
As I had feared and warned against in our "War Room" meetings, the irrational, high-dose use of steroids for mild COVID cases—often prescribed by panicked doctors in the first week of illness—had wreaked havoc. The steroids dampened the immune system and spiked blood sugar levels, creating the perfect petri dish for the fungus to thrive. We were seeing the visceral consequences of "panic prescribing." Our stand for evidence-based medicine at Sevagram had protected our own patients, but we were now the ones tasked with rescuing those who had been mistreated elsewhere.
***
Fighting this enemy was harder than fighting the virus. Unlike COVID, there was no rapid antigen test. Diagnosis required a high index of suspicion, a biopsy, and specialized CT scans—resources that rural hospitals rarely possess.
Once diagnosed, the treatment was even more difficult to secure. The only effective weapon was Liposomal Amphotericin B—a powerful, expensive, and notoriously scarce antifungal injection. As demand surged, the drug vanished from the market. It became unaffordable for the farmers and laborers of Wardha, leaving families in a state of absolute despair.
Here, the District Administration—the same team we had built trust with in the War Room—proved to be our lifeline. Recognizing the shortage, the government centralized the distribution of the drug. The district administrators came to our rescue, providing Amphotericin B injections free of charge for patients with proven mucormycosis admitted to MGIMS.
***
We established a rigorous protocol. We documented every vial, justified every dose, and kept the administration informed of every step. This was a complex, multidisciplinary war; it required our physicians, ENT surgeons, and ophthalmologists to work in a seamless loop.
Over those grueling months, we admitted and treated about fifty patients. These were heart-wrenching cases. I remember the look on the faces of people who had survived COVID, only to be told they might lose an eye to the fungus. While we could not save every eye, we saved nearly every life. Most of our patients were eventually discharged—survivors of a double siege.
Looking back, the "Black Fungus" chapter was one of the darkest periods of the pandemic. It reinforced a crucial, painful lesson that I have carried with me ever since: in medicine, the cure must never be allowed to become more dangerous than the disease.
The Anniversary Reflection
As the fires of the second wave eventually began to dim, I walked the corridors that had been so eerily silent in March 2020. I still recall the weight of that early silence, a feeling I captured in a Facebook post at the very start of the pandemic. The hospital has physically transformed since then—new oxygen plants hum with a mechanical heartbeat, and centralized pipelines snake through the walls of the medicine wards like silver veins. The "old" building stands as a battle-scarred veteran. But the most significant changes weren't made of brick and mortar; they were etched into the spirit of the institution.
I remember the first patient who arrived at our repurposed COVID block exactly 365 days prior. He was a sixty-four-year-old man from Washim, 225 kilometers away. He became, in a series of tragic "firsts," our first COVID admission, our first patient to be intubated, and our first death. Looking back from the peak of the second wave, that single death seemed like a distant, somber warning of the deluge that was to follow.
***
Over that year, we admitted more than five thousand patients. We delivered hundreds of babies to infected mothers, and we vaccinated thousands. Yet, the statistics do not capture the atmosphere of those twelve months. The nights in the ICU were never truly silent; they were filled with the relentless, aggressive noise of survival—the hiss of high-flow oxygen, the urgent beeping of monitors, and the alarms that refused to rest.
I recall the endless loop of questions that defined our conversations in the staff cafeteria and the hallways. How long will this last? When will we find a treatment that actually works? How do I hug my children when I get home without fearing I am poisoning them? As medical professionals, society looked to us as soothsayers, but the truth was that we were as uncertain as everyone else. We learned, painfully, that in a pandemic, the only thing you can be certain of is uncertainty itself.
***
Someone remarked to me that the practice of medicine in Sevagram changed more in that single year than in the previous fifty combined. We are a hospital built on the Gandhian philosophy of being "with" the patient. But the virus forced us into a "no-touch" reality. We stopped seeing faces; we saw masks and goggles. We distanced ourselves, we touched less, and we listened from afar.
Fear was the constant companion of every shift—fear in the OPDs, fear in the labs, and a heavy, silent fear carried home in the car at the end of the day. And yet, we did not stop. With fear in our hearts and hope on our lips, we kept going. I watched our ICU teams wrest lives from the tightening jaws of death, and each of those "discharged" stories brought a flicker of light to days that were otherwise heavy with loss.
***
By late January 2021, we had allowed ourselves a collective sigh of relief. The wards were emptying. The ventilators had finally stopped hissing. We believed, perhaps naively, that the monster had retreated for good. We began to talk about "normalcy" again.
But the virus was merely catching its breath. The second wave arrived with a merciless force that made the first year look like a rehearsal. We woke each day unsure if we were living through a nightmare or a waking reality. Wards overflowed. Staff fell ill just days after being vaccinated. We found ourselves sending "get well soon" messages to the very colleagues who, 48 hours earlier, had been standing beside us in the trenches.
***
As I reflected on that anniversary, I thought of Dr. Sushila Nayar, who founded this college in 1969. I wondered what she would have made of her institution during this crisis. I believe she would have been proud—not of a flawless execution, because perfection was impossible—but of the fact that we stayed.
We practiced medicine guided by science, not by the loud, irrational currents of social media. We drew extraordinary work from ordinary people—the attendants, the drivers, and the sweepers who are often invisible in times of calm but became the bedrock of our survival. This was a once-in-a-century pandemic, and it tested our resolve to its very core.
The anniversary was not a celebration; it was a testimony. We had learned that while we couldn't predict the future, we could defend the present. We stood tall when the world fell silent, and we realized that "This too shall pass"—but it would leave us forever changed.
Standing in the Storm
As the fires of the second wave eventually began to dim, I found myself walking those same corridors that had been so eerily silent in March 2020. The hospital had physically changed, but the most significant changes were not made of brick and mortar; they were etched into the spirit of the institution.
Looking back on these two harrowing years as Medical Superintendent, I am forced to ask: What did we actually learn? Beyond the flow rates of oxygen and the nuances of steroid dosing, what is the enduring legacy of Sevagram’s struggle?
For me, the defining battle was not against the virus itself, but against the "panic prescribing" that accompanied it. In the face of a terrifying, unknown pathogen, the instinct of the medical community was to "do something"—anything—even if it meant throwing the kitchen sink at the patient. At MGIMS, we made the harder choice: we chose to do only what was right.
***
The pandemic taught us that a hospital is only as strong as the trust the community places in it. During the height of the crisis, that trust was under constant siege. We lived in an era where a 30-second WhatsApp video, stripped of context, could undo months of hard work. We saw images of tired residents or crowded wards shared as "proof" of negligence, ignoring the moral burden and physical exhaustion of those in the PPE suits.
We realized that transparency was our only shield. We had to communicate relentlessly—not just with the state administration, but with the families waiting outside the gates. We had to explain why we couldn't use "miracle" drugs, why we couldn't hand over bodies, and why we were making the difficult choices we made. Trust, once shaken, is earned back slowly—one honest conversation, one consistent decision, and one patient at a time. We learned that in a climate of fear, efficiency matters, but integrity matters more.
***
Those were the days of interminable meetings. Thrice a week, either face-to-face in the Collectorate or on Zoom screens that froze at critical moments, I sat with the District Collector, the Civil Surgeon, and the political leadership of Wardha to coordinate the district’s response. These gatherings were often a strange mix of genuine administrative problem-solving and political posturing.
In one such meeting, attended by all four MLAs of the district, the Member of Parliament, and senior administrators, the tension snapped. A local MLA launched into a tirade, criticizing our nurses, residents, and attendants for "not caring properly and compassionately" for the patients. He spoke with the indignation of a man who had never worn a PPE kit in a non-AC ward.
I could not let it pass. I interrupted him, not as a subordinate, but as a shield for my staff.
"Sir," I said, my voice cutting through the hum of the air conditioner, "let me remind you of the reality. These nurses and residents work under pressure you cannot imagine. When they go home after a twelve-hour shift, they are terrified. They have old parents and young children waiting for them, and their greatest fear is not the virus itself, but that they might carry it home like a silent assassin. To question their compassion while they risk their families for your constituents is unjust."
I didn't stop there. I addressed the elephant in the room—the political pressure to prescribe unproven drugs. "Furthermore," I added, "the decision to administer medicines must remain inside the hospital. When politicians dictate that we must inject Remdesivir or infuse plasma—treatments that have no proven life-saving benefit—you are not helping; you are interfering. Medicine is not a democracy, and it is certainly not a constituency service."
I spoke for fifteen minutes. The room, usually filled with the rustle of papers and whispered aides, went silent. Everybody listened with rapt attention. When I finished, there was no rebuttal. The MLA nodded, perhaps realizing he had overstepped the boundary between governance and expertise. From that day on, the criticism stopped.
Later that evening, the District Collector called me. "Dr. Kalantri," he said, his voice relieved, "congratulations on that speech. It was bold and blunt. As an administrator, I could never have said that to an elected official, but you did. You have greatly eased the situation for all of us."
It was a small victory in a long war, but it affirmed a crucial truth: sometimes, the most compassionate thing a doctor can do is to be rude to a politician.
***
The crisis also forced us to recognize the remarkable contributions of those who are often invisible in times of calm. When we talk about "frontline heroes," we often think of the senior consultant giving an interview. But the pandemic belonged to the residents and nurses who lived inside the "Red Zones."
I remember seeing a second-year resident, Dr. Navneeth Rathod, slumped in a chair after a 36-hour shift. His face was marked with deep red grooves from the N95 mask, wounds that didn't have time to heal before the next shift began. In the sweltering heat of Wardha, inside impermeable plastic suits, our residents worked in conditions that bordered on the inhumane. They drew blood with fogged goggles; they inserted central lines while sweating profusely; they held phones to the ears of dying patients so families could say goodbye.
These young doctors absorbed the trauma of a generation. They saw more death in two months than I had seen in my first decade of practice. Yet, they showed up, shift after shift. As an administrator, my greatest lesson was that resilience doesn't come from the top down; it is carried on the shoulders of the youngest members of the team.
***
Perhaps the most somber lesson of this era was the cost of abandoning scientific temper. While other hospitals succumbed to the pressure to prescribe expensive cocktails of antivirals and antibiotics, we held the line.
We saved our patients from financial ruin and medical toxicity by saying 'No' to the noise. This decision was not without cost; we faced anger from families who demanded the 'expensive injections' they saw on TV. But we stood firm. We knew that the consequences of irrational prescribing would be far deadlier than the anger—a truth that would tragically unfold in the epidemic within .
***
As I write these final words on the pandemic years, the "War Room" has been dismantled, and the lecture halls are once again filled with the voices of students. But the silence of 2020 still echoes in my mind. We are a more sober institution now. We have seen the fragility of life and the stubborn resilience of the human spirit in equal measure.
Had Dr. Sushila Nayar been alive, I believe she would have walked these wards with a quiet nod of approval. She founded this college on the idea that healthcare is a form of social service, a Gandhian "Sadhana." In the pandemic, we were asked to prove it. We did not falter. We learned, we stumbled, we corrected course, and we kept going. In the end, it was not the protocols alone that sustained us, but an unspoken understanding that while perfection was impossible, abandonment was unthinkable.
In the end, it was not the protocols alone that sustained us, but an unspoken understanding that while perfection was impossible, abandonment was unthinkable. Sevagram stood tall when the world fell silent. And that, more than any statistic, is the story I wanted to tell.
The Studio and the Stethoscope
The pandemic was fought in two distinct arenas. The first was the sterile, terrifying silence of the ICU, where the only sound was the hiss of oxygen and the rhythmic beep of monitors. The second arena was the cacophony of the television studio and the smartphone screen. It was a world of screaming anchors, 30-second soundbites, and a "breaking news" ticker that moved faster than the virus itself.
For decades, I had been a creature of the first world—a physician-teacher content with the quiet rhythms of Sevagram. My "audience" was a batch of medical students or a terrified family in the OPD. But as the second wave crashed over India in 2021, I realized that the silence of the ward was being drowned out by the noise of the world outside. My patients were arriving not just with damaged lungs, but with damaged minds—convinced that a ₹12,000 antiviral would save them, or that a herbal coronil kit was a shield against death.
I realized then that if I wanted to save the patient in Bed 4, I had to fight the misinformation that had put him there. And so, with deep reluctance, I traded my stethoscope for a webcam and stepped into the glare of the digital public square.
***
One of my most significant interventions was with BOOM Live and the journalist Govindraj Ethiraj. The topic was ostensibly simple: "Choosing The Right Medicines." But in the context of 2021, this was a revolutionary act.
The medical establishment had become a bazaar. Doctors were prescribing "Covid Kits" that resembled grocery lists—Zinc, Vitamin C, Doxycycline, Ivermectin, Favipiravir, and steroids. It was a "poly-pharmacy" panic. On air, I had to be the killjoy. I had to look into the camera and say, "None of this works."
I remember the tension of those interviews. The pressure to offer "hope" is immense. People want to hear that there is a magic pill. When I argued for "Minimalist Medicine"—oxygen, proning, and steroids only for hypoxic patients—I was often met with incredulity. "But doctor," the subtext went, "surely we must do something?"
My argument was Orwellian in its starkness: Activity is not achievement. Prescribing a useless drug is not "doing something"; it is doing harm. It is financial toxicity. It is false hope. In my talks with Govindraj, I tried to dismantle the "more is better" fallacy. I explained that medicine is not a buffet where you pile your plate high just in case; it is a sniper's rifle. You fire only when you have a target, and you fire to kill the disease, not the patient's bank balance.
***
While the national media was obsessed with the oxygen crisis in Delhi and Mumbai, I felt a desperate need to turn the camera lens toward the village. The narrative was that rural India was "safe" due to open spaces and hardier immunity. This was a romantic lie.
In my interviews with Rema Nagarajan of The Times of India and IndiaSpend (later picked up by The Wire), I tried to puncture this myth. I spoke about the "Fear Factor" among rural doctors. I described how the government had dumped ventilators in district hospitals without training anyone to use them—like giving a Ferrari to a man who has never driven a car.
I told Rema, "A ventilator can kill you if you don't know how to use it." It was a brutal sentence, but it was necessary. The state’s response had been to throw hardware at the problem, while I was seeing software failure—a lack of trained nurses, fearful doctors, and a broken referral chain.
I also highlighted the "Digital Divide." The CoWIN app, hailed as a technological marvel, was a wall for my patients in Wardha. I described the absurdity of expecting a daily wager to log in, generate an OTP, and download a certificate. "We are vaccinating the privileged," I argued, "while the virus hunts the poor." These interviews were not just medical commentary; they were social audits of a fractured republic.
***
Perhaps the most heated battles were fought over Hydroxychloroquine. In early 2020, this old antimalarial had been elevated to the status of a divine nectar, endorsed by presidents and prime ministers.
When BOOM asked me about it, I had to walk a tightrope. The ICMR (Indian Council of Medical Research) was recommending it as a prophylaxis. To contradict the apex body is dangerous for a government-aided official. But the data was the data.
I said, "If it works in a Petri dish, that doesn't mean it works in a person." I called for a large, multi-centric randomized control trial (RCT) instead of observational guesswork. I pointed out that "safety" in the past (for malaria) did not equate to safety in a viral pandemic where the heart was already under stress.
This advocacy wasn't about being right; it was about protecting the scientific method. When I spoke to BBC World Service or VICE News, I wasn't just debating a drug; I was debating the very soul of medicine. Were we a profession of evidence, or were we a profession of anecdote?
***
The most enduring alliance I formed was with the "Resistance"—a loose coalition of journalists like Malini Aisola, Priyanka Pulla, and Dinesh Thakur. Together, we waged a war on "Financial Toxicity."
In a memorable discussion on the high cost of curing Covid, we dissected the pricing of Remdesivir and Tocilizumab. I shared stories from Sevagram—of farmers selling their wives' mangalsutras to buy a vial of Remdesivir that I knew would not save their dying father.
We coined the term "The Panic Tax." This was the extra cost paid by the poor for the ignorance of the rich. Every time a TV anchor hyped a new "miracle cure," the price of that drug spiked in the black market of Wardha. My role in these panels was to be the voice of the victim—the patient who survives the virus but dies of debt.
***
Looking back, those hours spent in front of a webcam, adjusting the lighting and checking the microphone, feel surreal. I am not a natural orator. I prefer the Socratic method of the bedside to the polemic of the panel discussion.
But I realized that in the 21st century, the "bedside" has expanded. It now includes the Twitter timeline and the YouTube comment section. If a doctor refuses to enter these spaces, they are ceding the ground to the quack and the grifter.
My media appearances were not an ego trip; they were a desperate extension of my Hippocratic oath. I realized that Silence is also a form of malpractice. When the world goes mad, the sane have an obligation to speak, even if their voice shakes.
I stepped out of the studio and back into the wards of Sevagram with a renewed respect for the power of the word. I had learned that a well-timed sentence, spoken with clarity and courage, could sometimes save more lives than a ventilator.
The Digital Resistance
A pandemic is fought in the ICU, but it is defined in the public square. As the Covid-19 crisis deepened, I realized that my duties as Medical Superintendent extended beyond the walls of Kasturba Hospital. The virus was spreading biologically, but misinformation was spreading digitally, and the latter was proving equally lethal.
I stepped into the digital arena—Twitter (now X), Facebook, and national media—not to seek fame, but to act as a counterweight to the "infodemic." This narrative explores how I used satire, collaboration, and public advocacy to defend scientific integrity when the official channels failed.
***
By mid-2020, the discourse around Covid treatments had become toxic. Pharmaceutical companies were pushing drugs like Favipiravir and Itolizumab with aggressive marketing campaigns that bypassed scientific scrutiny. The regulatory bodies seemed asleep at the wheel.
I found that citing "p-values" and "confidence intervals" did not resonate with a frightened public. So, I turned to irony. I began writing poems on Twitter, adopting the persona of the drugs themselves.
In my verse about Favipiravir, I mocked its high cost and low efficacy, highlighting how it drained the pockets of the poor while offering almost no clinical benefit.
In my poem on Hydroxychloroquine, I wrote from the drug's perspective, pleading: "Test me in a proper RCT / Before you sing my praise."
These tweets went viral. They did what a hundred academic lectures could not: they made people pause and question the narrative. I used humor to puncture the balloon of hype. It was a risky strategy for an academic, but it was necessary. I believe that when authority becomes irrational, satire becomes a duty.
***
The pandemic created unlikely comrades. I found myself part of a loose but fierce coalition of journalists, activists, and scientists who were determined to hold the system accountable.
I collaborated deeply with Dinesh S. Thakur, the public health activist. Together, we wrote a reasoned challenge to the approval of unproven antivirals in The Hindu, bridging the gap between regulatory failure and public interest.
I found a kindred spirit in Dr. C.S. Pramesh, Director of Tata Memorial Hospital. Our late-night discussions on the absurdity of testing protocols and treatment guidelines evolved into formal academic resistance. We co-authored articles in The Lancet and Nature Medicine on "Choosing Wisely," arguing that resources should be conserved for interventions that actually work.
I also worked closely with courageous journalists like Priyanka Pulla, Rema Nagarajan, Banjot Kaur, and Malini Aisola. These reporters were doing the job that medical regulators should have done—scrutinizing data and exposing conflicts of interest. By providing them with clinical context and on-the-ground reality from Sevagram, I helped ensure their stories had medical weight. We were fighting for the patient's right to truth.
***
A major theme of my public writing was the disconnect between New Delhi policy and rural reality. In my blog and articles ("Covid and Rural India", June 14, 2021), I highlighted how lockdown rules and digital vaccination portals excluded the villagers of Wardha.
I coined the term "Financial Toxicity" to describe the side effects of the pandemic response. It wasn't just the virus killing people; it was the cost of the cure. In my podcast with The Times of India and interviews with Deccan Herald, I argued that prescribing an ineffective drug like Remdesivir was not just a medical error—it was an economic crime against a family living on daily wages.
I spoke about how the obsession with RTPCR testing often delayed urgent surgeries for non-Covid patients, causing preventable deaths. I advocated for "Syndromic Management" in rural areas where testing kits were scarce—a pragmatic approach that focused on saving lives rather than filling databases.
***
A health journalist once pressed me on why I was so resistant to the "HCQ wave," given that generations of Indians remembered popping these pills for malaria. I had to dismantle the nostalgia with cold pharmacology. I explained that the "safety" of the past was an illusion; HCQ was no longer a standard malaria treatment precisely because of its toxicity profile—retinal damage, tinnitus, and the silent threat of QT prolongation in the heart. The argument that the drug worked "in vitro" (in a test tube) was a dangerous seduction; medical history is littered with molecules that killed viruses in a petri dish but failed—or harmed—the human body. To prescribe a drug with known cardiac risks to perfectly healthy staff as a prophylaxis, based on hope rather than data, was to violate the oldest commandment of our trade: Primum non nocere—First, do no harm.
The conversation inevitably turned to the ICMR, the apex body whose advisories were being treated as gospel. The journalist asked if my demand for published data was too harsh given the emergency. I countered that transparency is not a luxury for peaceful times; it is an ethical obligation in a crisis. The ICMR was issuing national directives based on observational studies they refused to make public—studies riddled with selection bias and confounding factors like geography and PPE usage. I argued that "doing something" is not a substitute for "doing science." By refusing to conduct a Randomized Controlled Trial—the only tool capable of sorting dead ends from life-saving strategies—the authorities were not reducing uncertainty; they were manufacturing it.
When confronted with defenses from colleagues at premier institutes like AIIMS, who cited small, open-label studies to justify the drug, I refused to soften my critique. They were building castles on sand—relying on trials with twenty-six participants or referencing biological theories about G6PD deficiency that didn't hold up to the 8.5% prevalence in our own population. I told the journalist that the approval of a drug for lupus does not grant it a generic passport for a pandemic. The defense of these flawed studies wasn't just bad science; it was a symptom of a medical culture that had allowed fear to override evidence. We were trying to treat a virus, but we were ending up treating our own anxiety.
***
In the midst of this conformist silence, a piercing voice emerged from Delhi—not from a radical activist, but from a Major General and orthopedician who described himself as a "medical heretic." In a scathing open letter to the Director of AIIMS, he dismantled the "halo" of the institution. He pointed out a lethal paradox: while the Director’s words were treated as Gospel, the institute's April 7th flow chart had become a bible of errors. He asked how AIIMS could greenlight Ivermectin when the WHO had explicitly flagged the lack of evidence, effectively accusing the country's highest medical body of ignoring global scientific consensus.
His critique of Remdesivir was unsparing. He correctly identified its place in the "hall of shame" of modern medicine—a drug that fueled a sordid economy of black marketing and hoarding while offering no survival benefit. But his most damning observation concerned the indiscriminate use of steroids. He lamented that "common sense is not very common," noting that the blind adherence to AIIMS guidelines had led doctors to pump viral patients full of immunosuppressants too early. He connected the dots that many refused to see: that the guidelines themselves were hastening disease progression and inviting the fungal nightmares that followed.
The letter ended not with a plea, but with a verdict on "vicarious responsibility." It captured the invisible tragedy of the pandemic: the families who pawned jewelry and sold tiny parcels of land to buy expensive, useless vials because a flow chart told them to. Reading his indictment, I felt a grim solidarity. The General had articulated the central tragedy of the second wave—that in a war-like situation, the nation needed discerning clinicians, but the system had demanded only obedient soldiers.
***
As the waves subsided, the need to document our systemic failures became urgent. Sahaj Rathi and I contributed to the book compiled by Dr. Yogesh Jain and Dr. Sarah Nabia, discussing the flaws in evidence generation. I also co-authored a book chapter on "Covid Irrational Treatments" (Brill Publishers), ensuring that this era of medical madness was recorded for future generations of students.
We critiqued the ICMR’s role, the opacity of the vaccine rollout (IndiaSpend, Aug 8, 2020), and the lack of transparency in death data (NBC News, Sep 17, 2020). We did not shy away from criticizing the "Secretive Bodies" making decisions (Appeal-Democrat, June 20, 2021).
***
Dr. Sushila Nayar founded MGIMS on Gandhian principles. During the pandemic, I interpreted "Gandhian practice" as the strict adherence to truth—Satya.
Whether it was telling the BBC that a herbal cure was fake, telling the government that their death toll was an undercount, or telling a patient's family that an expensive injection would not help, the core principle was the same.
My role as a public intellectual during Covid was an extension of my role as a teacher. I was teaching the public how to read science, how to spot a grift, and how to demand better from their healthcare system. The poems, the tweets, and the op-eds were not distractions from my job; they were the essence of it.
In the end, we learned that a pandemic is not just a biological event; it is a social and moral test. Sevagram passed that test not because we had the most ventilators, but because we had the courage to say "No" when the world was screaming "Yes." That is the legacy I leave to the archives.
The Poet as a Shield
The early months of the COVID-19 pandemic were defined by an uncritical, almost religious enthusiasm for unproven remedies. In the vacuum of certainty, desperation became a business model. Drugs with little to no evidence were promoted aggressively, embraced eagerly by a panicked public, and prescribed widely by physicians who felt they had to "do something." As Medical Superintendent, I watched this erosion of scientific temper with a mixture of alarm and exhaustion.
One of the most glaring examples was Favipiravir. It quickly displaced hydroxychloroquine as the new promise of hope, backed by a flawed trial involving barely 150 patients. Marketed as a "game-changer," a full course cost ₹12,500—a king's ransom for a rural family—and, at its absolute best, shortened a fever by a single day. The mismatch between the marketing promise and the clinical proof was staggering.
***
On June 21, 2020, I found myself unable to respond with yet another thread of data, p-values, and clinical references. I realized that data often bounces off the armor of fear, but satire has a way of finding the gaps. I decided that if the world was going to be irrational, I would meet it with irony. I wrote a poem in the voice of the drug itself and posted it on Twitter.
A Satirical Take on the 2020 Craze
I see a lot of activity, today on Twitter
Looks like I have sent a thousand hearts aflutter
Pharma is happy and the media has gone crazy
And so is public, for the picture is so hazy
My name is Favipiravir, I have made my mark
In the world of Covid, I am a new patriarch
Don’t jeer at me, nor try to pull me off
I am here to stay and shall have the last laugh
They tried me in just eighty patients
And most felt happy, no coughs, sighs or grunts
The trial was not a RCT, you object
But do I really need a trial? I am so perfect
So what if you can’t locate me in PubMed
Haven’t I really painted the entire country red?
You are sure to say, what a relief, phew
And to your anxiety, surely you would bid adieu
I can make your x-ray look good
And there is a fair likelihood
The chances are not remote
The virus can quickly leave your throat
So what the patients also get better if left alone
Ignore me at your peril and be ready to bemoan
To be happy, keep on swallowing me for a fortnight
And dig deep into your pockets just Rs 300, every night
The poem went viral. It captured, through irony, the absurdity of the moment—how a drug could "paint the country red" without ever having to prove its worth in a peer-reviewed journal. A few weeks earlier, I had done the same for Hydroxychloroquine, pleading with the public in verse to "test me in a proper RCT" before singing its praises.
I was not turning to poetry to escape science; I was using it to defend science. In a world filled with "noise," rhyme allowed me to pause, reflect, and question without shouting. If my poems provoked discomfort among pharmaceutical executives or "miracle-cure" advocates, then the verse had served its purpose.
***
Almost accidentally, I discovered that Twitter (now X) was a powerful instrument for public education. It offered something traditional academic platforms could not: immediacy. It allowed me to respond in real-time to the latest "miracle" drug or irrational testing protocol.
My focus remained firm. I wrote repeatedly against the indiscriminate use of Ivermectin, Azithromycin, Itolizumab, and Convalescent Plasma. I was equally disturbed by the official endorsement of unvalidated remedies, and I did not hesitate to question these policies publicly. This was not about visibility; it was about the responsibility of a Medical Superintendent to speak beyond the hospital walls.
***
This digital journey introduced me to a community of journalists, activists, and physicians who believed that even in a pandemic, reason deserved a voice. I connected with journalists like Priyanka Pulla, Rema Nagarajan, and Malini Aisola—interlocutors who became valued colleagues. I began a deep professional collaboration with Dinesh S. Thakur; together, we wrote a reasoned challenge to Favipiravir in The Hindu, using logic to bridge the gap between regulatory failure and public interest.
Twitter also opened doors to leaders like Dr. C.S. Pramesh, Director of Tata Memorial Hospital. Our conversations evolved into a close professional relationship, leading to co-authored articles in The Lancet and Nature Medicine on "Choosing Wisely" during COVID-19.
Looking back, my engagement on social media during those turbulent years was an act of duty. In a crisis, the defense of evidence is not optional. COVID humbled our certainties, but it also reminded me that sometimes, the best way to protect a patient’s life—and their pocketbook—is to dare to rhyme in the face of a miracle.
The Lessons of the Storm
As the fires of the second wave eventually began to dim, I walked the corridors that had been so eerily silent in March 2020. The hospital had physically transformed—new oxygen plants hummed with a mechanical heartbeat, and centralized pipelines snaked through the walls of the medicine wards like silver veins. The "old" building stood as a battle-scarred veteran. But the most significant changes weren't made of brick and mortar; they were etched into the spirit of the institution.
Looking back on two harrowing years as Medical Superintendent, I am forced to ask: What did we actually learn? Beyond oxygen flow rates and the nuances of steroid dosing, what is the enduring legacy of Sevagram’s struggle?
***
The pandemic taught us that a hospital is only as strong as the trust the community places in it. During the crisis, that trust was under constant siege. A 30-second WhatsApp video, stripped of context, could undo months of labor. We saw images of exhausted residents shared as "proof" of negligence, ignoring the moral burden carried beneath the PPE.
Transparency was our only shield. We had to communicate relentlessly—not just with the state, but with the families huddled outside the gates. We had to explain why "miracle" drugs were myths, why we couldn't hand over the dead, and why we made the choices we did. Trust is earned back slowly—one honest conversation and one consistent decision at a time. In a climate of fear, efficiency is a virtue, but integrity is a necessity.
***
The crisis forced us to see the invisible. When we talk about "frontline heroes," we picture the doctor with the stethoscope. But the pandemic belonged equally to the attendants who moved bodies in 45-degree heat, the drivers who navigated oxygen tankers through the silence of lockdowns, and the sweepers who scrubbed the "Red Zones" with meticulous, dangerous care.
These were ordinary people performing extraordinary work. They ensured that when the rest of the world shut down, Sevagram did not run out of fuel or courage. As an administrator, my greatest lesson was this: resilience doesn't trickle down from the top; it bubbles up from those holding the smallest, most essential tasks in their hands.
***
The most somber lesson was the cost of abandoning scientific temper. The "Black Fungus" epidemic remains a tragic monument to "panic prescribing." It was a man-made disaster proving that evidence-based medicine is not a luxury for peaceful times—it is a survival kit for a crisis.
At MGIMS, we held the line. We stayed anchored in science when the currents of misinformation were at their strongest. We saved patients from both medical toxicity and financial ruin by simply saying "No" to the noise. If our practice changed more in a year than in the previous fifty, it was because we were forced to rediscover our core: the pursuit of truth at the bedside.
The "War Room" is dismantled now. The lecture halls are once again filled with the voices of students. But the silence of 2020 still echoes. We are a more sober institution now. We have seen the fragility of life and the stubborn resilience of the spirit in equal measure.
Had Dr. Sushila Nayar been alive, I believe she would have walked these wards with a quiet nod of approval. She founded this college on the idea that healthcare is a form of social service—a Gandhian Sadhana. In the pandemic, we were asked to prove it. We did not falter. We learned, we stumbled, we corrected course, and we kept going. In the end, it was not the protocols alone that sustained us, but an unspoken understanding that while perfection was impossible, abandonment was unthinkable.
Sevagram stood tall when the world fell silent. That is the story.
The Patriarch
In the Marwari tradition, the word "Bhaiji" is more than a name; it is an anchor. It conveys a specific blend of reverence, respect, and patriarchal authority. For my father, who was born on June 19, 1916, in the tiny village of Taroda, the journey to becoming "Bhaiji" was not a path laid with silver spoons, but one carved out of the hard rock of survival. To understand the man he became, one must first look at the silence from which he emerged.

He was an orphan of the shadows. By the age of five, an infectious disease had claimed both his parents, leaving him with no photographs, no yellowed letters, and no stories passed down through generations. He grew up in abject penury, an experience that would have broken a lesser spirit, but in him, it forged a steel-trap mind and a relentless drive for self-reliance. He rarely spoke of the hardships of those early years—the winter mornings waking at 4:00 AM to bathe in a cold river or the ten-hour days tending livestock. He carried those scars silently, translating his pain into a staggering work ethic that would eventually define our family’s trajectory.
Fate often wears the mask of a stranger. For my father, that stranger was Shri Chiranjilalji Badjate, a Munim for the Bajaj Group. In 1932, Chiranjilalji spotted a sixteen-year-old boy in Taroda chasing after grazing cattle and saw something in the boy’s eyes—a spark of intelligence that didn't belong in the dust of a pasture. He brought him to Wardha to meet Jamnalalji Bajaj, the man Gandhi regarded as his fifth son.
The interview was not a test of academic merit, but of ego. Jamnalalji looked at the boy and asked: "Will you willingly clean the toilet?" My father didn't hesitate. He said yes. This was the "acid test" of the Bajaj Group—a search for a man who was a Peer, Bawarchi, Bhishti, Khar (Saint, Cook, Water-bearer, and Donkey). By saying yes to the most menial of tasks, my father opened the door to a forty-six-year career that would see him rise from a jack-of-all-trades earning eleven rupees a month to the Secretary of the Jamnalal Bajaj Seva Trust.
If my father had a superpower, it was his relationship with numbers. He possessed a staggering devotion to the "Parta"—the centuries-old traditional Marwari system of financial monitoring. To him, an account book was not just a ledger; it was a moral document. He had a photographic memory for figures and an uncanny ability to spot a manipulated number from across a room. Under the mentorship of Chiranjilalji, he learned the foundational adage of his professional life: "Whatever happens, the accounts must be in order."
I remember him in his office at Gandhi Chowk, surrounded by the heavy ledgers that were the essence of his world. He was a stickler for detail, often checking his work multiple times to ensure perfection. This wasn't mere bureaucracy; it was a form of integrity. In a world of shifting allegiances, numbers were the only things that didn't lie. He managed nearly a hundred acres of Bajaj land and oversaw the Shri Laxminarayan Devasthan Trust with the same meticulous precision he applied to our own household. He taught me that whether you are managing a charitable trust or a hospital budget, precision is a form of respect.
Despite his traditional roots, my father was a man far ahead of his time. His exposure to the Gandhian circles of Wardha and the influence of Jamnalalji and Jankidevi Bajaj turned him into a quiet revolutionary. Nowhere was this more evident than in his own marriage to my mother, Parvati, in 1940.
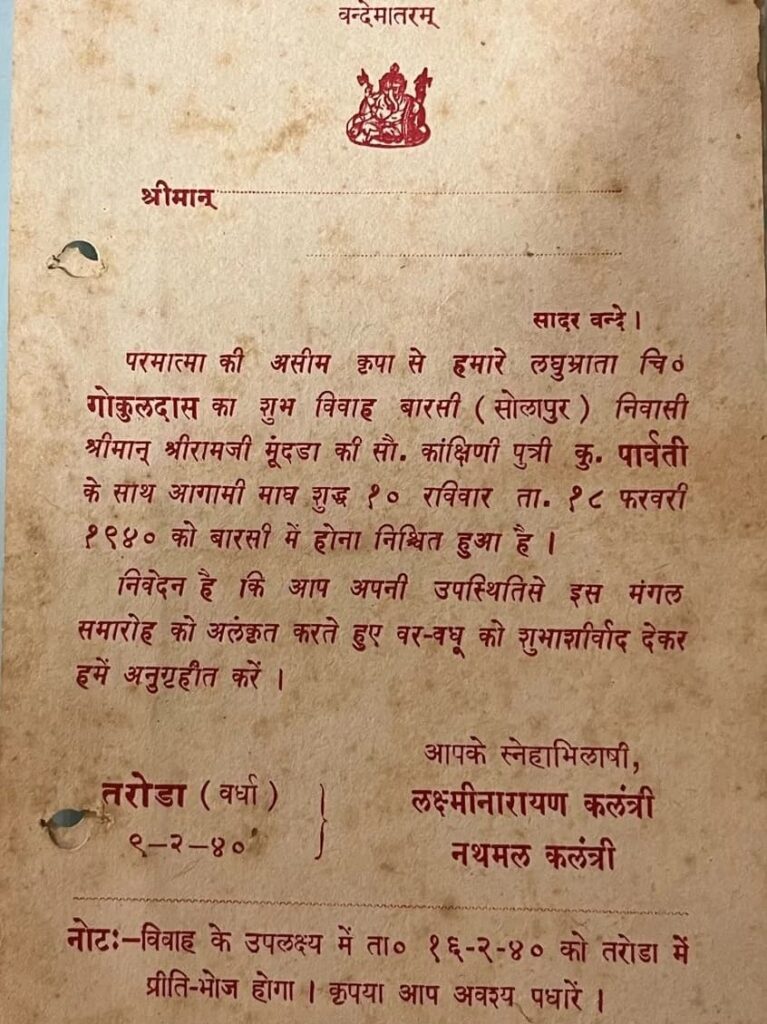
In an era where the ghoonghat (veil) was an iron rule of Marwari society, my father set a shocking condition for the wedding. "I insist that the bride does not wear a ghoonghat throughout the ceremony," he declared. To my maternal grandparents in Barshi, 500 miles away, this was unfathomable. They worried about how a girl from a traditional background would adjust to a "dark-complexioned orphan" who demanded she show her face to the world. Yet, my father prevailed. It was the first wedding in that community where the bride remained unveiled, a bold act of defiance inspired by Mahatma Gandhi’s call for women to discard the parda. He believed in the dignity of the individual over the comfort of tradition.
My father’s sense of precision extended to the very walls we lived in. In 1967, when we moved into our current residence, he didn't just buy a house; he envisioned a transformation. He sought out the renowned architect Mr. Sheodanmal to redesign our home. When the architect spent only thirty minutes inspecting the premises, my mother was disappointed, but my father knew better. He understood that a master eye doesn't need hours to see the truth.
He, along with my brother Om, dedicated themselves to the construction of "Jaishree Bhavan." My father’s eye for detail was relentless. He personally supervised the "curing" of the walls and hired a sixteen-year-old boy to lay the floor tiles with such meticulous alignment that today, five decades later, they remain as pristine as the day they were laid. He believed that if you build something, you build it to outlast you. Our home was a physical manifestation of his philosophy: solid, precise, and built on a foundation of hard work.
To present Bhaiji as a saint would be to do a disservice to the complexity of his character. He was a man of fiery temper and little patience for opposing views. He lived by a binary code: "either you are with me or against me." He was arrogant about his convictions, and his anger could be formidable. Yet, this same man was capable of extraordinary, quiet kindness.
There is the story of Mr. Tapdiyaji, a young man who was turned away from a professional office because he wasn't wearing "formal" clothes. When my father heard of this humiliation, he didn't just offer sympathy. He provided the funds for Tapdiyaji to buy a suit, lent him the family car, and personally vouched for him. That one act changed the course of Tapdiyaji’s life. For decades after, until my father’s death, Tapdiyaji would visit our home every Dussehra to touch my father’s feet. My father didn't seek gratitude; he sought to correct an injustice.
My father lived as he died—with a quiet, unsentimental fearlessness. He passed away on December 21, 1986, at the age of seventy. He didn't spend a single day in bed; he didn't endure the slow erosion of a prolonged illness. He faced death quickly, without regret, much like he faced the "acid test" of his youth.
We took his mortal remains to Haridwar, accompanied by his guide and philosopher, Radhakrishnaji Bajaj. As we immersed his ashes in the Ganges, I realized that while the man was gone, the "Bhaiji" remained. His legacy was not just the property he built or the accounts he balanced, but the resilience he instilled in us. He was a man who rose from nothing, defied the norms of his time, and taught his children that grit, integrity, and a devotion to truth—whether in numbers or in life—were the only things that truly mattered.
The Silent Weaver

If my father was the iron foundation of our family, my mother—whom we addressed as "Bai" in the Marwari tradition—was the light that filled the rooms. Born Parvati Mundra on January 5, 1925, in Barshi, she arrived in Wardha in 1940 as a fifteen-year-old bride, thrust into a world that was as unfamiliar as it was daunting. She was the first of five children, raised in a devoutly orthodox home where her father, a seller of tea and biscuits, was more focused on Ishwar Bhakti (devotion to God) than on the formal education of a daughter.
Her marriage to my father was a study in contrasts. He was nine years her senior, an orphan with no roof of his own and a stubborn, radical streak. She was a delicate girl from Western Maharashtra who had never traveled more than a few miles from her parents. Most shocking to her traditional family was my father’s ultimatum: "The bride will not wear a ghoonghat." For a girl raised in an era where the veil was a woman’s shield, this was a radical exposure. Yet, on February 18, 1940, she stepped into her new life with her face uncovered—a silent revolutionary before she even knew the meaning of the word.
The transition was brutal. The young girl who had been the apple of her father’s eye in Barshi was suddenly responsible for a household in the "Marwari Mohalla" of Wardha. Her first home was a rented space that the locals whispered was haunted by ghosts. My father, who viewed such superstitions with scientific contempt, ignored the rumors, but for Bai, the fear was real.
In those early months, she was like a "scared deer running in the forest," as she later described herself. She would cry inconsolably, begging her parents to take her back to Barshi. When her uncle came to drop her off, he had to leave stealthily while she slept, knowing she wouldn't let him go if she were awake. She woke up to a world where she had no mother-in-law to guide her, only the memory of her parents 500 miles away. Yet, it was in this "haunted" house that she found her footing. She lived there for fifteen years, and it was within those walls that five of her six children were born.
Bai belonged to an era that defined a woman by her ability to manage a home without the luxuries of electricity, gas, or running water. For years, she ran a full house with nothing but a smoke-emitting chullah (mud stove). I remember the story of my father buying her a modern gas stove in 1955, thinking it would ease her burden. Bai was so suspicious of the new technology—or perhaps so loyal to the familiar discomfort of the woodsmoke—that she made him return it. Eventually, she compromised on a "Magan Chullah," a smokeless alternative that cost ten rupees.
Watching her in the kitchen was like watching a master artisan. She had arrived in Wardha not knowing how to knead dough, but she soon surpassed her teachers. Her "jugglery" of serving steaming hot phulkas to my father, who sat cross-legged for his meals, was a sight to behold. She specialized in aloo-bhaat (potato rice) and meethe chawal (sweet rice) for guests, and for me, her kela-ka-kalvan (mashed bananas with milk and sugar) remains the taste of childhood. She didn't just cook; she nurtured. She would churn buttermilk manually—a task we children called jhagda-bilona because of the rhythmic noise—to separate the butter that would eventually become the ghee that flavored our lives.
I was the youngest of her six, born on August 15, 1957, in our second home at the Bajaj Electricals campus. My birth brought a specific joy to my parents; not only was I a boy, but I arrived at 6:27 AM on India’s tenth Independence Day. My father, always one for brevity, changed my birth name from Devendra to Shriprakash, and then quickly shortened it to "SP."
I often wonder how easily Bai, who had only a primary school education, adapted to calling her youngest son by an English abbreviation. To her, I was just SP. I remember telling her when I was five years old that my "real" parents were Lord Shiva and Parvati on Mount Kailash, and that while she shared the same name, she was just a temporary guardian. She would laugh, a light, musical sound, and continue her chores. On my birthdays, she didn't provide balloons or cakes. Instead, she would wake me early, rub my skin with haldi (turmeric) and milk, give me a new pair of locally-stitched half-pants, and offer a homemade pedha as a blessing. She never remembered her own birthday, but she celebrated ours with a quiet, fierce devotion.
Bai was a slight woman, barely four feet ten inches tall, but she had a vibrant, inquisitive mind. Despite her limited schooling, she read the Hindi newspapers from cover to cover every day. She had a deep love for Hindi cinema, a passion that often saw her sitting in the "ladies' compartment" of the local Vasant Talkies. She saw the 1975 blockbuster Sholay at least three times, and she was so enamored by the screen that she gave her granddaughters nicknames like "Padmini" and "Helen" after the famous actresses.
She had an uncanny ability to balance the old world with the new. In 1997, when she suffered her first heart attack, she was brought to the ICU at Sevagram. As a physician there, I watched her receive streptokinase, a modern clot-buster. She accepted the technology of the hospital with the same grace she used to accept a new sari from my father. She was agile and active; even in her eighties, if a guest arrived unannounced, she would disappear and re-emerge in seconds, having changed her sari and bangles to properly welcome them.
In the final years of her life, Bai’s memory began to flicker, but her spirit remained bright. She would clap and sing bhajans (hymns) whenever she heard them on the television. She had a particular fondness for the song "Sajan Re Jhoot Mat Bolo" from the movie Teesri Kasam, and she famously sang it on stage at a family wedding in 2005, much to the amazement of the younger generation.
In 2000, at the age of seventy-five, she decided to make her will. I sat with her, explaining the legal intricacies word by word. I was stunned by her clarity; she understood exactly how her assets should be equitably distributed. She wanted no loose ends, no "unbalanced accounts."
She left this world exactly as she had lived in it—with a quiet, uncomplaining grace. She passed away in the early hours of the morning, as peacefully and as quickly as my father had. She had spent over six decades as the weaver of our family's story, balancing tradition with modernity, and faith with reason. She belonged to an era of women who worked incessantly without ever asking for their contributions to be acknowledged. To her, motherhood wasn't a job; it was an evolution. She taught me that resilience doesn't have to be loud; it can be as quiet as the steam rising from a phulka or the turn of a newspaper page in the afternoon sun.
The Final Lesson
My father died on December 18, 1986. He was seventy years old. In the decades since, that date has stayed with me, not because I make a conscious effort to remember it, but because it remembers me. It is a day that sits permanently in the calendar of my soul, a marker of the moment when the "Patriarch" transitioned from a living force to a silent legacy.
That evening followed a familiar, reassuring rhythm. I was a lecturer at Sevagram Medical College then, and my life was neatly divided between the white-walled intensity of the hospital and the grounding presence of home. My commute was a ritual of its own: I would ride back on my Bajaj scooter for dinner, return to Sevagram the same night for my duties, and come home again the next day for lunch. It was a life moved by regularity, measured in the eight-kilometer stretches of road between Wardha and the college.
***
When I reached home around seven that evening, the air was cool with the onset of winter, but the atmosphere inside was heavy. I sensed at once that something was amiss. My father was uneasy, slightly breathless, and uncharacteristically restless. He said little, which was his habit, but his silence felt different—it was the silence of a man preoccupied with an internal struggle he couldn't quite name.
He went to the toilet—a ritual he had performed unfailingly before dinner for nearly sixty years—and when he returned, he was drenched in sweat. In the medical world, we are taught to look for "red flags," and seeing a man drenched in sweat in the middle of a cold December unsettled me deeply. As I watched him, his breathing became labored. Against my will, my mind began to flip through the pages of his medical history: his first heart attack in 1977, when I was a fourth-year student in Nagpur; his second, four years later. He had diabetes and hypertension—the classic markers of a heart under siege.
The clinical signs aligned with a cruel, undeniable clarity. His failing heart was no longer pumping effectively; fluid was beginning to collect in his lungs. The "Physician Son" in me took over. I told him we had to go to the hospital immediately.
***
Even the short walk to the car was an ordeal for him. Every movement required an effort that left him gasping for air. Dr. B. C. Chandak, our neighbor and a practicing physician, offered to drive us to Sevagram Hospital. My brother sat in the front seat, gripped by the urgency of the moment. I sat in the back, holding my father close, trying to be the anchor for a man who had always been mine.
Four kilometers into that eight-kilometer journey—exactly halfway between the life he had built and the hospital I served—he became suddenly, profoundly still.
I felt for his pulse. There was none. I placed my ear against his chest, hoping—against all medical knowledge, against all reason—to hear something, a flutter, a click, anything. But his chest no longer rose. The silence in the back of that car was absolute. My father had died in my lap. Nothing in my medical training, no textbook on cardiology or emergency medicine, prepares you for that instant when a body you know intimately becomes irrevocably unfamiliar. The finality was swift, a quiet exit on a dark road.
***
We reached the Medicine ICU within minutes, but the "minutes" no longer mattered. Dr. Ulhas Jajoo, a dear colleague who knew my father and me well, was there with the residents. The machinery of modern medicine hummed into life—an ECG was taken, drugs were administered, and resuscitation began. I stood there, watching the flat line on the monitor, a stark contrast to the vibrant, disciplined life my father had led.
After a few minutes, I looked at Ulhas. I saw the futility in his eyes, and he saw the realization in mine. "Stop," I told him. He understood, he agreed, and the room went silent.
We returned home to tell my mother. Her grief was raw and uncontained, a primal response to the sudden severing of a forty-six-year companionship. Though she lived with the daily knowledge of his heart disease, she had never imagined this abrupt ending. That night, as the family gathered around her, sitting in a silence that felt heavier than words, we shared the first few hours of a world without Bhaiji.
***
The funeral was held the next day at four in the afternoon. By then, the house was filled with the people who formed my father’s world—relatives like Asha, Pushpa, and Ashok Bajaj, alongside a vast crowd from Wardha. My father had always lived by reason rather than ritual. He encouraged us to question every custom and to discard anything that felt hollow or performed. In keeping with his spirit, we kept the farewell simple.
There were no shaved heads. There was no reading of the Garud Puran. There was no display of staged grief—only a quiet, profound dignity. As the funeral pyre was lit and his body returned to ash, I felt the unmistakable sense that an era had quietly closed. The man who had refused to let his bride wear a veil was now departing a world he had tried to make more rational.
A few days later, Radhakrishnaji Bajaj, my father’s mentor, traveled with us on the Dakshin Express to Haridwar. His presence was steady and consoling as we made the journey to the Ganges. We performed the immersion ourselves—no priests, no chanted mantras, no bustling crowds. Just the quiet, endless flow of the water carrying away what remained of a life lived with extraordinary discipline.
***
Looking back now, I realize my father died exactly as he would have wished. He was a man who prized independence above all else, and he was spared the one thing he would have found unbearable: the loss of his autonomy. He was never confined to a bed. He did not suffer prolonged, agonizing pain. There were no tubes, no monitors, and no helpless waiting in the shadows of a chronic illness.
As fearless in death as he was in life, he slipped away quickly, without drama and without indignity. At the time, as a young lecturer, I did not have the words for it. I had not yet learned to speak of "dying with dignity." Today, as a senior physician, I speak of it often to my patients and their families. I prepare them, gently, for the possibility of a peaceful end, away from the invasive machinery of the ICU.
Graceful Exit
December 2005 brought a sharp, biting winter chill to Sevagram. I had been back from Berkeley for seven months, slowly recalibrating my life to the rhythm of the hospital and the college. Life felt full and predictable—the wards were busy, the students were eager, and my memories of California were transitioning into evening anecdotes. But on December 5, the familiar cadence of my day was shattered by a phone call from Jaishree Bhavan. It was Kanta Bhabhi. Her voice, usually steady, was tight with an unmistakable worry. "Bai is struggling to breathe," she said.
Without a second thought, I grabbed my keys and jumped into my Maruti 800. The drive from Sevagram to Wardha is barely eight kilometers, a road I had traveled thousands of times, but that day, it felt like an endless stretch of gray tarmac. When I arrived, the vibrant matriarch of our world looked smaller, frailer than I had ever seen her. She was weak, her eyes searching the room for an anchor, unable to articulate the distress within her. When she vomited twice in front of me, the son in me felt a surge of panic, while the doctor in me recognized the signs of a system beginning its final shutdown. "We need to go to the hospital," I said firmly.
***
We admitted her to the Old Medicine ICU at Sevagram. My colleagues and mentors, Dr. O.P. Gupta and Dr. Ulhas Jajoo, attended to her immediately. The ICU is a place of high-stakes intervention; it is a landscape of beeping monitors, sterile smells, and harsh, unflinching lights. It is a place designed to fight death, often with a violence that leaves little room for the soul.
As the ECG machine hummed, spitting out a strip that told the story of a tired heart—old infarcts and a dangerously slow rate—we started the standard protocols. We administered fluids and medication, hoping for stabilization. But as the hours ticked by, a different realization settled over me. Looking at Bai, lying vulnerable amidst the tangled wires and plastic tubes, I knew this was not the environment she deserved for her final act. Modern medicine often forgets that "doing everything" can sometimes be a form of cruelty. At 9:00 PM, I made a decision that went against the grain of my training but aligned perfectly with my instincts as her son. "Let's take her home," I said.
***
My home was a ground-floor flat in Vivekanand Colony, just a two-minute drive from the hospital gates. It was quiet, familiar, and filled with the energy of the family she loved. We brought her there, away from the alarms and the antiseptic. She refused dinner—her body instinctively knowing it no longer required nourishment—and drifted into a heavy sleep.
The night was a vast, heavy silence. Kanta Bhabhi and I sat vigil by her side, watching the rise and fall of her chest. There is a specific kind of intimacy in these final hours; it is a space where the noise of the world falls away, leaving only the breath of a parent and the quiet presence of those they raised. At 4:00 AM, the rhythm of the room changed. Bai woke up. She looked sick, but there was a startling clarity in her distress. Kanta Bhabhi, with the intuition born of years of caregiving, sensed that the moment had arrived. She leaned close and whispered, "Recite a Bhajan, Bai."
***
Bai, summoning a final, extraordinary strength, moved her lips. "Sitaram... Sitaram..." It was the chant that had been her steady companion through decades of widowhood, struggle, and survival. We gently lifted her off the bed. I sat on the floor and took her into my lap, cradling her head just as she had held me countless times when I was a child.
In those final moments, there was no panic. There was no frantic rush back to the ICU, no intubation, no ribs breaking under chest compressions. There was only the warmth of a son’s embrace and the soft sound of a name she had loved. She took a breath. Then another. And then, a profound, holy silence. On December 6, 2005, in the quiet pre-dawn hours, Bai passed away in my arms. It was a "good death" in every sense—she left the world as quickly and as peacefully as my father had, but with the added grace of being held by her own.
***
The news of her passing traveled with the speed of grief. Badibai was in Indore, and as soon as the word reached her, Aalok began the long drive to ensure she reached Wardha by early afternoon. Jiji rushed from Nagpur. By 1:00 PM, the house was filled with the people Bai had nurtured, fed, and guided. We performed her final rites at 4:00 PM that same day. As we returned her to the elements under the pale winter sun, I felt a strange mixture of sorrow and relief. We had protected her dignity until the very last second.
***
Bai was a woman of her time, yet she constantly transcended it. She belonged to a generation of women who worked tirelessly for their families, often invisible in their labor, never seeking the spotlight. She was the bridge between our humble, cramped beginnings in Wardha and our later successes in the academic halls of Sevagram. But she was never a one-dimensional saint. She was complex, spirited, and fiercely real.
I remember her in all her shades: her sharp sarcasm, her occasional arrogance, her deep bouts of depression after my father’s death, and her jubilant joy in her later years. She was a woman who could watch Sholay three times and still find something new to love about it. In the early years of her widowhood, she endured financial stress and emotional pain that would have broken a lesser person. She raised us with a protective instinct that was almost primal. As we grew and succeeded, she softened, finding a sense of fulfillment in our achievements that replaced the anxieties of her youth.
***
The Phantom Presence
Holding her in those final moments, I realized a fundamental truth: while the physical umbilical cord is cut at birth, the emotional connection is only truly severed at death. And even then, it leaves a phantom sensation—a lingering presence that occupies the empty rooms of Jaishree Bhavan.
I still hear her quiet advice in the back of my mind when I face a difficult decision at the hospital. I still hear the echo of her "Sitaram" in the silence of the early morning. Bai taught me that medicine is not just about the length of a life, but about the quality of the ending. She showed me that a "good death" is the final gift a son can give a mother. She lived with grace, she labored with love, and she left with dignity. The circle of her life was complete, leaving behind a family that now walks the paths she helped pave with her quiet, relentless resilience.
The Custodian of Stories
I call her Badibai—the elder mother. Ever since I was born in August 1957, she treated me with such abundant love that she richly deserves this name. Fifteen years my senior, Asha became more than a sister; she became a second mother, a protector, the bridge between the Wardha of our childhood and the larger world beyond.
When I was born, Badibai was already fifteen, navigating the transition from girlhood to young womanhood. She had moved to Kesrimal Kanya Shala, a Marathi medium school, because Bhaiji refused to send his daughter to a co-educational institution. She wore a sari to school from the fifth standard onwards—twelve years old and already wrapped in yards of fabric that restricted her movements.
Her birth itself had been an ordeal. Born on February 26, 1942, in Barsi at our nani's home, as was the custom, Bai endured a protracted, agonizing labor before Asha arrived. Six months later, the Quit India movement would shake the very foundations of British rule, launched from Wardha where we would all eventually gather our lives. Perhaps there was something in that timing—a child born in pain, emerging into a world on the cusp of freedom, her own freedoms curtailed by the very traditions that shaped our family.
She was good at arithmetic, scoring perfect marks in tenth standard, but algebra remained a mystery that cost her a passing grade in the board exam. Bhaiji insisted she study Sanskrit, Music, and Mathematics—three subjects that held no appeal. She never had the chance to study further, to build a career, to prove herself. Yet I never heard her complain. Instead, she derived genuine happiness from watching her children and grandchildren achieve what she could not.
***
By 1959, Bhaiji was determined to marry her off quickly. Badibai grew weary of families arriving to inspect her like merchandise. When the Singhis from Indore finally came for a formal girl-seeing ceremony, my exhausted sister made a decision that defined her character forever. Asked about her education, she looked them straight in the eye: "Matric fail."
In a world built on pretense, her honesty was revolutionary. The Indore party was touched. They appreciated her refusal to let lies distort reality.
The wedding on Vasant Panchmi, February 1, 1960, became the talk of Wardha for years. Bhaiji had issued strict instructions about the number of guests, and when fewer than fifty baraatis arrived, he kept his word magnificently. They stayed at Bajaj Wadi—where Nehru, Patel, and Bose had once lived. Eleven teachers from Mahila Ashram school served three sumptuous meals. No band, no baja—only a shehnai. Tukdoji Maharaj sang a bhajan. The wedding cost Bhaiji thirteen thousand rupees—equivalent to over a lakh today.
I was barely three years old, but the stories of that wedding became family lore, told and retold until they acquired the quality of myth.
***
At eighteen, barely out of her teens, Badibai moved to Bhopal in 1961 and lived in the vast Tapdiya house. From four in the morning until eleven at night, she cooked and cleaned for twenty-odd people, a perpetually tired young woman who never complained, never even hinted to our parents the burden she carried.
Jijaji earned three hundred fifty rupees a month. Badibai supplemented their income with stitching work. Once, traveling on the GT Express without a proper ticket, she was asked to disembark at Itarsi. A compassionate TT helped her board an unreserved third-class coach. She never told Bhaiji about the humiliation.
Her mother-in-law was strict, but Badibai found unexpected allies in her jethani—the bond between them became inexpressible. When she ran out of decent saris, her jethani arranged for a shop's back door to open after hours so they could shop in secret. Balkishanji Singhi would buy saris for her. Another jethani sensed her struggle with Bhopal's biting cold and arranged for buckets of boiling water to arrive every morning, traveling five furlongs just to ease her discomfort.
These small kindnesses sustained her through those difficult years.
***
Between 1962 and 1971, four children arrived—Archana, Anand, Aalok, and Amit. Each birth brought its challenges. When Anand was eighteen months old and contracted an illness, Bai agreed to keep him in Wardha for the next eighteen months. For him, his nani became everything. When Aalok turned fourteen, he was adopted by Jijaji's elder brother—a family tradition spanning four generations. Badibai wasn't even consulted. Tormented by the thought of her son going away, she refused to eat for a week.
Jijaji was determined to give his children the best education Bhopal offered, even if it meant stretching beyond his means. Badibai saved every penny for their schooling. "I learned English from my children," she told me. "We asked our kids to learn five new English words a day and use them in sentences." She learned stitching in Wardha and knitting in Bhopal, her resourcefulness knowing no bounds.
***
In summer 1975, everything changed. Badibai contracted a severe infection following surgery. Sepsis developed. Her weight dropped below thirty-five kilograms. Jijaji drove her to Wardha, and she was admitted to the Medical College hospital in Sevagram for twenty-six days. I was finishing my medical training then, and stayed with her in the private room. She barely ate, requiring intravenous antibiotics to survive.
During those dark days, Jijaji once thought she was dying and began reciting the Bhagavad Gita. Badibai, barely able to speak, summoned enough strength to be angry: "Stop this. I am not dying!"
She recovered slowly, surrounded by family. The hospital billed us six hundred rupees for her twenty-six-day stay. When she went back to Bhopal, she carried renewed determination to live fully, to see her children grow.
***
On December 3, 1984, the world's worst industrial disaster struck Bhopal. The Singhi family woke at 1:30 a.m. with watering eyes and coughing fits. Anand saw the sky covered in white fumes and immediately understood. He made them get into their old Premier Padmini and drove toward safety. They had no time to lock the house or release their animals.
Jijaji drove through streets filled with people running, coughing, suffocating. By morning, thousands had died. Their dog and cows were dead. The plants had turned black.
Badibai never spoke much about that night, but I could see it in her eyes whenever Bhopal was mentioned—the terror, the randomness of survival.
***
In 1988, the family moved to Shail Shikhar—a home named by Archana to symbolize Bhopal's topography of ups and downs. This became Badibai's domain, where she orchestrated marriages, welcomed grandchildren, and finally created the home she had always deserved.
Her four children married well—Archana to Suresh Mintri, Anand to Kirti Gattani, Aalok to Sumita Lahoty, Amit to Dr. Pratibha Taori. Badibai supervised these weddings with grace, never interfering, always supporting. Her name Asha is embedded in two granddaughters' names—Pratiksha and Nimisha. They confide in her as a friend.
Around 2010, she developed severe lower back pain that restricted her movements. She required a wheelchair when she came to Wardha. But her willpower helped her recover completely. Last November, I was surprised when she boarded Dakshin Express—a journey that once seemed impossible.
***
"I do not recall a single day when I fought with Pushpa," Badibai told me recently. All her life, she gave elder sister's love to Pushpa—understanding her pain, her financial problems, her emotions. When Bai willed her ten tolas of gold, Badibai passed it all to Pushpa. She had once gifted Pushpa gold earrings because she herself had a pair but Pushpa didn't.
This is who she has always been—someone who measures wealth not in what she possesses but in what she can give away.
I am amazed how Badibai has embraced technology. She's often the first to send birthday wishes on the WhatsApp group Archana created. She's aware of every family happening, every milestone.
***
Today, at eighty-four, Badibai and Jijaji live in Shail Shikhar. Their bedroom houses a refrigerator, television, and tea cooktop—a small kingdom where they live without grudge. Remarkably articulate with enviable memory, they have defied their age.
Badibai can still recall her childhood neighbors from seven decades ago. Her memory for numbers remains sharp—Archana says she can recall every rupee, every bank balance, every investment.
When the pandemic arrived in March 2020, I found myself thinking often of Badibai. She who endured so much—the curtailed education, the years of domestic servitude, the illness that nearly took her life, the gas tragedy that could have ended everything. She survived it all with grace, with quiet strength that never announces itself but simply endures.
In Sevagram's hospital corridors, when patients asked about my family, I would sometimes mention Badibai—how she raised four children despite having no formal education beyond tenth standard, how she taught herself English from her children's homework, how she turned deprivation into determination. Many mothers nodded in recognition. They understood that kind of strength.
Badibai taught me that education happens in many forms—in kitchens where you master unfamiliar cuisines, in sewing rooms where you learn forbidden skills, in asking your children to explain five new words daily. She taught me that love sometimes means accepting decisions you disagree with, staying silent about crushing workloads, and giving away gold because your sister needs it more.
When I think of resilience, I don't think of textbooks or research papers. I think of Badibai at eighteen, working from 4 a.m. to 11 p.m. I think of her at thirty-three, fighting sepsis with her weight below thirty-five kilograms. I think of her at forty-two, fleeing the gas tragedy at 1:30 a.m., not knowing if she would survive.
And I think of her now, at eighty-four, sending birthday wishes on WhatsApp, learning technology with the same determination she brought to learning English, still deriving happiness from achievements she never had the chance to pursue herself.
This is resilience. This is grace. This is Badibai—the elder mother who taught me, long before I became a doctor, what it truly means to care.
Jiji
Pushpa was born on 17 May 1946 in a modest house in Marwari Mohalla, Wardha—fifteen months before India gained its independence. She was the third of six siblings, all born within those same familiar walls. All, that is, except me.
She was eleven years older than me, and from the beginning she occupied a place in my life that no one else could fill. Our eldest sister carried the authority of a second mother. Jiji was different. She was steady, always there—both companion and guide.
She studied in Marathi-medium schools in Wardha: Sarkari Madhyamik Shala, Kesrimal Kanya Shala, and Craddock High. In Class 10, she and our brother Ashok sat in the same class. I still remember the story of their Physics exam. Jiji came out in tears, certain she had failed. Ashok was calm and confident. When the results were announced, she had passed. He had not.
She wanted to study science and become a doctor. The dream was not broken with drama—it was set aside quietly. A local professor advised my father that a medical career would delay her marriage and narrow her prospects. My father chose what seemed practical. Jiji did not argue. Science gave way to Arts, and her chance at medicine slipped away almost without a sound.
She married Shri Tarachandji Chandak in May 1965. She tried to continue her studies at Yashwant College, but a new household has its own pull. Travel, responsibility, and the daily work of setting up home took over. Soon after her final exams, and the birth of her daughter Mamta, her formal education came to a quiet end.
Her married life took her across the country—Madras, Nagpur, Kagaznagar, Baroda, Gwalior, Indore. Each move meant beginning again: new neighbourhood, new faces, new household assembled from very little. She built a home each time without complaint, making sure her children never felt the strain.
She was never someone who sat still. As a girl she had loved Kho Kho, Langdi, and relay races. That energy stayed with her. I remember once she was playing Gulli Danda with us when her father-in-law arrived without warning. Our mother, worried about appearances, called her inside. Jiji slipped out through the back door and, within minutes, was seen busy with housework, as if she had never stepped out. She had a gift for finding the balance between what she was and what was expected of her.
In Kagaznagar she was at her happiest—parties, films, clubs, friendships. Later, when Jijaji was offered a position at Shri Dinesh Mills, they moved to Baroda. I visited and spent fifteen days there, cycling around the city, watching films, making memories. We went together to Ahmedabad to buy her a mixer. She was delighted with it.
In the late eighties, when times were hard, she began selling salwar suits from her flat in Indore—travelling to Delhi and Gandhinagar to bring back material. She carried this without drama. Where her husband could act on impulse, she held things together.

During my medical years in Nagpur, her home in Shankarnagar became my refuge. I went almost every weekend. The house was always full—relatives, children, noise—but Jiji moved through it calmly, cooking, serving, making space for everyone. We played cards late into the evenings. On Monday mornings, her children would hide my cycle keys, trying to delay my leaving by a few more hours.
We wrote to each other every week. Her postcards were simple, filled with the small details of her day. Once, when I failed to reply, she wrote: I may not have wealth in my hands, but my heart is rich with love and kindness. I read that line in my hostel room and felt its full weight. I wrote back at once.
That was Jiji. She never asked for much, but she held on to her people in a way that left no room for doubt.
In late 2018, she began to experience abdominal pain, bloating, and vomiting. She felt unusually tired during her walks and could no longer sustain her hour-long yoga. When she called me, I was caught up with MD examinations in Chandigarh and could not answer immediately. That evening, I sensed the worry in her voice and told her to get an ultrasound without delay. The scan revealed ovarian cancer. Just months earlier, the ultrasound had been normal.
She had surgery in February 2019, followed by six cycles of chemotherapy—three before the operation and three after. Throughout it all, she continued doing yoga when she was able, listening to music, chatting on WhatsApp, spending time with family. By February 2022 the cancer appeared to be in remission. Then it came back.
For the next three years, chemotherapy became the rhythm of her life—a session every two weeks. When I visited her recently in Indore, she looked down at her thin, tired veins and said, quietly, that she must have had at least thirty-six sessions by now.
At first she struggled to accept that ovarian cancer almost always returns—that there is no cure, only time. She wanted to live fully and hoped for a miracle. Slowly, she came to terms with her reality. Her energy faded. Confined to her room, cut off from the social life that had sustained her, she lost her appetite, her weight, and something of her spirit.
Her final years were held together by a small, steady circle. At its centre were Aalok—her sister's son—and Archana, her daughter-in-law.
Aalok never let distance come in the way. A phone call was enough; he would arrive soon after. In hospital corridors he spoke to doctors, handled the paperwork, sat through long chemotherapy sessions, lightened the mood with small jokes. Jiji waited for his visits. Yet he would never take even a glass of water from her home.
At their second-floor flat in Kanchanhar Enclave, only three remained—Jiji, her son Manoj, and Archana. Archana managed everything without fuss: appointments, medicines, the endless trips to the pharmacy. She would sit with Jiji during meals, urging her to eat a little more; on long afternoons, she stayed by her bedside, her hand resting gently on Jiji's. It did not feel like duty. It felt like affection. Jiji often told me she was fortunate to have an angel at home.
Manoj was different. He was not someone who showed his feelings easily; the hospital, the slow drip of suffering, was more than he could bear to watch. So he held everything else. He had bought this flat and put it in her name—years before any of this—without once speaking of it. He made sure treatment never paused, that every expense was met, that nothing she needed was ever out of reach. People often misunderstand such choices: they see absence and do not see what lies behind it.

I lived those years in two roles: the younger brother she loved, and the doctor she trusted. We spoke many times each day. When the pain grew, she would call, and I would listen. She had a simple faith in me that sometimes felt heavier than any clinical responsibility.
I am a physician, not a gynaecologist. But her illness pushed me to read—to understand the chemotherapy regimens, the supportive medications that could ease her symptoms. Once, I suggested something to be taken an hour before each session. It seemed to abolish her nausea. She would tell people, with quiet satisfaction, that it had worked when other things had not.
Yet the reading brought with it a deeper unease. As I began to understand the course of the disease, it became clear that no intervention—however well meant—could change the final truth.
The hardest task was telling her so. During her visits to Sevagram, we spoke often about the end. She was clear in her own mind: she did not want a long life at any cost; she wanted a life without pain. When the time came, I had to tell her there would be no more scans, no more chemotherapy—only comfort. She accepted it without resistance. Through her, I understood what palliative care truly means, not in a hospital ward, but at home. I had to remain her brother while speaking as her doctor, and I was not always sure I managed it well.
A year before she died, I spoke to her about a living will. I told her that when she could no longer speak, this document would speak for her—no ICU, no machines, a death at home. It was not an easy conversation. But I felt it was better to be honest than to offer hope I did not have.
As the end drew near, the illness slipped out of our conversations. We talked of the past instead—of places we had lived, people we had known, small shared memories. She slept more, ate very little, grew very tired. Her walks to the neighbourhood garden became short strolls inside the house, and then she could no longer turn in bed.
Our last video call was the day before she died. She opened her eyes, recognised me, and then closed them gently.
On the morning of 22 March 2026, Aalok called. I could sense it in his voice before he spoke. She had passed away at home, just as she had wished—quietly, without struggle, without machines.
Only later did I learn how carefully she had thought about those final moments. Six years earlier, she had chosen a photograph she liked and asked her grandson Sarang to keep it safely. Six weeks before her death, she told him: this is the one. She had her instructions ready. No marigolds—she had never liked them. No white jasmine either. She wanted roses. And she did not want silence; she asked for a band to accompany her on her final journey.
Even at the end, she arranged things in her own way.
When I think of her now, I do not see the illness. I see the homes she built in city after city, the postcards she wrote every week, and the quiet way she held all of us together. All my life, I called her Jiji. That is how she stays with me.
The Operating System

We began, like many couples in 1984, with an arranged marriage. No romance preceded it, no courtship worth mentioning. Just photographs exchanged, horoscopes not matched, and a wedding date fixed. What followed was not a fairy tale but something more durable: a functional partnership that has lasted four decades.
Bhavana studied biology at Holkar College, Indore, then completed a diploma in medical laboratory technology in Mumbai. She never worked in a lab. The work bored her. While pregnant with our first child in 1986, she finished a B.Ed. degree—not because she intended to teach, but because the college was nearby and she disliked idleness.
A year later, with two small children at home, she began traveling from Sevagram to Nagpur—eighty kilometers each way—to learn computers. This was 1992. Personal computers were rare. The internet did not exist in India. Most people thought computers were large machines that occupied air-conditioned rooms in banks. Bhavana simply noticed that these machines would matter and decided she should understand them.
That decision, made without announcement or drama, shaped not only her career but the hospital's future.
***
For twenty-eight years, Bhavana worked with the Hospital Information System at Kasturba Hospital, MGIMS Sevagram. She did not hold a grand title. She was not a department head. She simply made the system work.
When the hospital decided to computerize patient records in the early 1990s, most staff resisted. Doctors preferred handwritten notes. Nurses distrusted keyboards. The administrative staff feared redundancy. Bhavana trained them anyway—one reluctant clerk at a time, one skeptical physician after another.
She troubleshot endlessly. When the server crashed at 2 a.m., she drove to the hospital. When data disappeared, she recovered it. When workflows jammed, she redesigned them. She translated medical chaos—unreadable prescriptions, misfiled records, lost lab reports—into orderly digital systems.
Her colleagues debated policy in meetings. She built solutions that actually worked. The full story appears in Chapter 6 of this memoir, but the essence is simple: while others talked about modernization, she modernized.
She retired in July 2023. By then, Kasturba Hospital's information system was among the most functional in rural India. She had created it almost single-handedly, with neither fanfare nor self-promotion.
***
In 1984, I owned a Bajaj 150 scooter, registration number MH 32-922. After marriage, Bhavana learned to ride it—unusual in Wardha, where few women rode two-wheelers. We kept that scooter for twenty years, repainting it green midway through its life.
In 1999, we bought a second-hand lemon-colored Maruti 800 (MP 09-0036) from Sendhwa, Madhya Pradesh. The car had been driven for only one year and fit our budget. None of us knew how to drive.
Bhavana, then thirty-seven, took lessons. She learned methodically, practiced daily, and within months was navigating Wardha's chaotic traffic with the calm of a taxi driver. Today she drives with near-surgical precision, though I occasionally remind her that speed limits exist.
In our MLK Colony neighborhood, there are exactly four women who drive while their husbands sit in the passenger seat: Mrs. Mehendale, Mrs. Shukla, Mrs. Vyas, and Bhavana. This fact is neither progressive nor traditional. It is simply how things are.
She now drives a Honda Jazz, which she parks with the efficiency of someone solving a geometry problem. Most evenings, she drives to Wardha, navigates the market traffic, negotiates with vegetable vendors, and returns with the week's supplies. She does this without complaint, as if ferrying groceries were an Olympic event she intends to win.
***
If I had to describe Bhavana's role at home, I would call her the operating system. The house runs because she makes it run.
Laundry appears folded. Bills are paid before reminders arrive. Repairs happen before they become crises. Visitors are fed. Groceries never quite run out. The children grew up secure without realizing how much backstage work produced that comfort.
She managed an astonishing range of tasks: washing clothes, ironing, mending socks, sewing buttons, mothproofing woolens, sweeping floors, cleaning sinks and toilets, tending the garden, shopping for vegetables and rice, cooking three meals daily, entertaining relatives, managing finances, overseeing repairs, supervising the maid and gardener, paying bills—all while attending to the children's schooling, clothing, discipline, and morale.
She did this without a washing machine for the first decade. Without a car for fifteen years. Without domestic help for long stretches when we could not afford it. She simply worked harder.
Her management of people is firm but fair. Vimal, our maid, has stayed for over thirty years. Devanand, the gardener, for twenty-five. She scolds them for lateness, interrogates unscheduled leave, and raises her voice when work is sloppy. Yet she is generous with bonuses, advances for medical bills, and small gifts during festivals.
They understand the arrangement. The tongue may be sharp, but the heart is soft—what I call the coconut temperament. Hard shell, sweet interior. That is why they stay.
***
Bhavana is a perfectionist, though she would deny it. Each morning, she selects my clothes: shirt, trousers, socks, polished shoes. She reminds me monthly to get a haircut. The bedsheets and pillowcases must be arranged in a specific order. Cushions have designated corners.
This is not obsessive-compulsive disorder. It is simply her belief that chaos can be prevented with sufficient attention. She is probably right.
She shops with the same precision. In the era of online commerce, she navigates Amazon like a procurement officer, comparing prices, checking reviews, tracking deliveries. Watching her find the best deal on bedsheets is like watching someone solve a differential equation.
She has also redesigned our home multiple times—new furniture, fresh paint, rearranged rooms. Her aesthetic is neither traditional nor modern but functional. If something does not work, she replaces it. Sentimentality does not factor into decisions about sofas.
***
Bhavana's cooking is not elaborate. She does not experiment with fusion cuisine or follow celebrity chefs. She simply makes food that tastes unmistakably like home.
Her repertoire includes vegetable curries, fragrant rice, Marwari and Gujarati dishes like puran poli, and desserts: kheer, shrikhand, gulab jamuns. Former medical residents who trained under me still remember her gulab jamuns. They were soft, sweet, and arrived on time—which, in a busy hospital household, was itself a minor miracle.
Meals in our home follow a timetable. Breakfast at 7:30 a.m., lunch at 1 p.m., dinner at 8 p.m. Deviations are rare. Guests are fed regardless of arrival time. No one leaves hungry.
This is not hospitality in the theatrical sense. It is simply her belief that feeding people properly is a basic obligation. She executes it with the efficiency of a military quartermaster.
***
Bhavana tends plants with the same systematic care she applies to everything else. She works closely with Devanand, the part-time gardener, ensuring proper pruning, watering, and feeding. Old trees are replaced with newer, more colorful varieties. Flower beds are reorganized seasonally.
The results are visible. Our garden blooms year-round, not because we live in a favorable climate but because she treats horticulture like another management problem requiring persistent attention.
She subscribes to Down to Earth, an environmental magazine, and reads extensively about climate change, deforestation, and pollution. This is not fashionable eco-consciousness. She genuinely worries about what we are leaving for our grandchildren.
***
In 2012, I underwent an angioplasty. Bhavana handled it with remarkable calm. No visible panic, no tearful bedside vigils. She simply accepted the situation and did what needed doing: coordinating with doctors, managing visitors, ensuring I followed post-operative instructions.
When her ninety-year-old father suffered a massive stroke and lay unconscious, she was the first to suggest we let him die with dignity at home. Some family members hesitated, hoping for miraculous recovery. She remained firm. "This is what he would want," she said. She was right.
Her clarity in crises is often braver than my medical training. I know the science. She knows when to stop fighting.
***
Despite my position as a professor of medicine, Bhavana has never been impressed by titles or hierarchy. She punctures inflated egos, especially mine.
She is my most ruthless editor. Whenever I write something long-winded—which is often—she says, "Keep it short, SP." I argue. She insists. I eventually cut. She is usually right.
This applies to life decisions as well. When I had spent too long as hospital administrator, she said, "Retire while you're still wanted. Don't wait to be bowled out." I resisted at first, citing unfinished projects. She repeated the advice until I listened. Again, she was right.
***
From 1994 to 2004, we had a Pomeranian named Zombie. From 2013 to 2019, we had a Labrador, also named Zombie. Bhavana treated both as if they were additional children: regular feeding schedules, grooming, vaccinations, daily exercise.
She walked them herself, rain or shine. When they fell ill, she sat up through the night. When they died, she grieved quietly and then moved on. Sentimentality ended where practicality began.
***
After our son Ashwini married Shaily, they lived with us in a joint family arrangement. Bhavana managed the household as both mother and mother-in-law, navigating the delicate balance between authority and diplomacy.
When grandchildren arrived—Diti, Nivi, and Krit—she found unexpected joy. She spent hours reading to them, playing Uno, telling stories. She instilled in them a love for learning, respect for science, and concern for the environment. Watching her shape their values was like watching her debug code: patient, systematic, effective.
During a recent visit to Chandigarh, she observed the creche at PGI where our daughter Amrita works as a radiologist. Seeing how it allowed working parents to focus on their jobs without anxiety about childcare, Bhavana decided to start a similar facility at Kasturba Hospital.
She retired in July 2023 specifically to run this creche. At sixty-one, most people slow down. Bhavana started a new career.
***
For over twenty years, Bhavana has practiced yoga for one hour every morning. Recently, she added a five-kilometer evening walk, completed in under fifty minutes. She tracks her walks on Strava with the same precision she applies to grocery lists.
She reads the Times of India daily, follows science and environmental news, and shares articles she finds important. Her recent interest is classic English films—Gladiator, The Last Samurai—though her favorite remains the Hindi film Wake Up Sid (2009), which she has watched countless times.
This disciplined routine—yoga, walking, reading, watching one film nightly—is not asceticism. It is simply her way of organizing time so nothing is wasted.
***
We have argued often. About disciplining the children. About which car to buy. About trivial irritations magnified by stress. Sometimes we stopped speaking for days. Sulking is not beneath either of us.
Bhavana's temper is quick. Mine is slower but more stubborn. The combination occasionally produces thunderstorms.
But like actual storms, these episodes pass. Reconciliation is never announced. It simply happens—through shared tasks, resumed conversations, small gestures of care. The lingering tension dissolves like the smell of rain on dry earth.
I suspect marriages survive not because two people are compatible but because they learn to compensate for each other's excesses. She trims my sentences; I supply footnotes to her conclusions. Somewhere between the two, balance emerges.
***
Looking back over forty years, I realize Bhavana is not only my wife but also my closest friend and fiercest critic. We have weathered illnesses, career pressures, the challenges of raising children, and the slow adjustments of aging.
During the COVID-19 pandemic, when the hospital felt like a war zone and I worked eighteen-hour days, she kept the household steady. She did not offer grand speeches of encouragement. She simply assumed I would do what needed to be done. That quiet faith steadied me more than any pep talk could have.
She still repeats the same instruction she has given for decades: "Finish your work and come home."
I usually listen.
The Godhuli Bela Wedding
I tied the knot with Bhavana on February 17, 1984. I was twenty-seven; she was twenty-two. It was a classic arranged marriage, orchestrated by family networks and a stroke of serendipity involving a broken-down car.
Looking back, the timing feels significant. It was just weeks before the Maruti 800 first rolled onto the streets of Gurgaon, signalling a new, faster India. But our beginning was rooted in the old ways—slow, deliberate, and guided by family.
***
Fate often disguises itself as inconvenience. In October 1983, I was travelling from Bhopal to Indore with my brother-in-law, Jijaji. Thirty-five kilometres short of our destination, near Dewas, our car sputtered and died. While waiting for a mechanic, we killed time by visiting Mr. Pralhaddas Singhi, Jijaji’s elder brother who lived nearby.
There, we ran into Mr. Suresh Laddha, a 33-year-old businessman from Balwadi who had recently moved to Indore. When he learned I was an unmarried physician from Wardha, his eyes lit up. He immediately thought of his niece, Bhavana. He rushed home to tell his sister-in-law, Mrs. Kamal Laddha, who happened to be visiting from their village.
Mrs. Laddha didn't waste a moment. She changed into an elegant sari, struggling slightly with the pleats in her haste, and rode pillion on Suresh’s scooter to meet me at the Singhi home. She was visibly relieved to hear I was a doctor from Wardha. Decades earlier, in the 1950s, she had stayed at the Mahila Ashram in Wardha with her aunt, Mrs. Suman Bang. When I mentioned I knew her cousin, Dr. Abhay Bang, and colleagues like Dr. Ulhas Jajoo, the anxiety in her eyes softened. The connection was made.
A few weeks later, the formal machinery of the Marwari arranged marriage kicked into gear. A delegation—Shri Rajmalji Laddha, Professor Yadav Zamvar from Mumbai, and Dr. Suraj Mandora—arrived in Wardha to vet the prospective groom.
***
Two weeks later, it was my parents' turn. They travelled to Jalgaon to meet Bhavana’s uncle, Sharad Manudhane, in his small two-room flat. From there, the journey to Balwadi—190 kilometres away—was an adventure in itself.
Mr. Manudhane borrowed an Ambassador car from a neighbour, and they set off through the dense forests of Shirpur and Sendhwa. A heavy rainstorm battered the roof of the car, the wipers slapping a hypnotic rhythm against the windshield as they navigated the muddy roads. But the destination was worth the trek. My parents were charmed not just by Bhavana’s poise and education, but by the warmth of the Laddha family. They returned to Wardha with a clear verdict: we would be lucky to have her.
***
In November 1983, I visited Bhavana’s modest home in Raj Mohalla, Indore, for the formal "viewing." I was accompanied by my elder brother Om and my brother-in-law.
The meeting lasted thirty minutes. It was a stiff, formal interview typical of the era. I sat across from her, introducing myself, discussing my career, and delicately enquiring about her education. She was shy but possessed a quiet grace that filled the room. We didn't go to a coffee house or a garden; we sat in her living room, acutely aware of the family members listening from behind the curtains.
I stole glances at her. She was stunning—a BSc graduate from Holkar Science College who had also studied medical laboratory technology in Mumbai. But more than her beauty or her degree, I sensed a shared temperament. I wasn't looking for a professional peer; I was looking for a partner. Driving back to Wardha, I knew I had found her.
My father finalized the date: February 17, 1984. I had six weeks to prepare.
***
It is hard to convey to a modern reader just how modest our beginnings were. In 1984, my salary as a medical college lecturer was ₹1,500 per month. Even five years later, by the time our second daughter was born, it had only risen to ₹5,900.
We owned no car, no computer, no mobile phone. A flight was a luxury we couldn't imagine; we travelled strictly by second-class train. Yet, we never felt poor. A train ticket to Mumbai cost a fraction of our salary. We found joy in library books, evening walks, and cinema halls. As my friends Dr. Ramji Singh and Naresh Kumar often remind me, we lived simply, but we lived well.
***
I threw myself into the wedding preparations, starting with the invitations. Mr. Ramesh Fattepuria pointed me to a skilled screen printer in Sitabuldi, Nagpur. The cards cost 90 paise each—a total of ₹270 for 300 cards.
Screen printing was a slow, manual art. Ink was pressed through a mesh stencil onto the paper, one card at a time. I wrote the text in Hindi, keeping it elegantly simple and adding a request that was rare for the time: "No gifts, please." I hand-wrote the addresses on all 300 envelopes myself. It was laborious, but I was proud of the result.
***
For my wedding attire, I turned to my friend Dr. VK Gupta, a man with a keen eye for fashion. Along with our friend Suhas Jajoo—a staunch Gandhian who wore only Khadi and had never tied a tie in his life—we scoured the markets of Nagpur.
We ended up at Lords Taylor, a renowned shop near Variety Square. It was an amusing trio: the groom, the fashion expert, and the Khadi-wearing Gandhian, all debating fabric swatches. Suhas, despite his simplicity, often cast the deciding vote. We were young, broke, and incredibly happy.
***
My father was a man who viewed rituals as suggestions rather than rules. When the pundits advised a midnight wedding for my sister, he ignored them and held it at 7:00 AM. For my brother’s wedding, he ignored the advice to leave early and insisted the procession leave Wardha precisely at midnight because "the train leaves at midnight, so why shouldn't we?"
He applied the same no-nonsense punctuality to my wedding. He didn't care for superstitions; he cared for schedules.
On February 16, a group of 21 Baratis—family, friends, and elders—boarded the Nagpur-Dadar Sevagram Express. We reached Bhusawal at 5:00 AM, where a fleet of six Ambassador cars, arranged by the Laddha family, waited to ferry us the final four hours to Balwadi.
***
We arrived in Balwadi at 10:00 AM and were housed at Mehboob Manzil, a spacious, newly built home owned by three local cotton merchants who had kindly opened their vacant property to us.
To keep the younger guests entertained, my brother-in-law Vivek set up a VCR and screened the classic film Madhumati. The kids were so captivated by Dilip Kumar and Vyjayanthimala that they watched the movie in fragments three times over two days.
True to my father's wishes, there was no ostentatious procession. I refused the traditional white horse and the street dancing. The wedding took place at the most auspicious hour: Godhuli Bela—the "cow dust hour," when twilight falls and cattle return home from the fields.
At 6:00 PM, under the soft glow of the setting sun, Pandit Chimanilalji Shastri conducted the ceremony. It was efficient—just 45 minutes. In the 1930s, Kaka Kalekar, the well-known Gandhian and Vice Chancellor of Gujarat Vidyapeeth, had studied ancient Hindu scriptures and designed a wedding manual that compressed the entire ceremony into forty-five minutes. My father, who worked with the Bajaj group, had witnessed such weddings and earnestly believed in these brief rituals—far better than the midnight feras that dragged on until dawn broke.
As Bhavana's father placed her hand in mine during the Kanyadaan, I saw the mix of grief and hope in his eyes. We took the seven vows (Saptapadi) around the fire, signing a divine contract not with ink, but with steps.
***
The return journey was a lesson in humility. We boarded the train from Jalgaon, where the family had booked a First Class coupé for the newlyweds. It was a luxury—privacy, padded seats, silence. But as the train pulled out, we realized that two of our elderly relatives were squeezed into the crowded second-class compartment.
The guilt was instant. At the very next station, Bhusawal, we gathered our things and swapped seats. We spent our wedding night not in the isolation of a first-class cabin, but on hard wooden berths in second class, surrounded by chattering family and shared laughter. It felt more like home than the coupé ever could.
***
We returned to my childhood home, Jaishree Bhavan. Our room was a sanctuary—airy, cool, with large windows and a bathroom that felt luxuriously modern for the time.
Bhavana slipped seamlessly into the rhythm of a joint family. A month later, my brother Ashok and his family moved in, making the house even fuller. Bhavana’s mornings began early. She prepared tea and a hearty breakfast before I left for the medical college on my Priya scooter—a daily 8-kilometre commute.
For the first few years, I lived a double life: spending my days and on-call nights in a small room at the hospital hostel (Kabir Niwas), and my off-duty hours at home with Bhavana. She didn't move to the Sevagram campus until December 1988.
***
In late February, we took our first trip together: two weeks in Udaipur and Mount Abu. We walked the banks of Lake Pichola, marvelled at the Rajput palaces, and soaked in the history of Chittorgarh. We stayed in decent three-star hotels, a splurge for us, but true to form, we took the non-AC second-class train back home.
It was a simple start. No grand gestures, no debt-fueled luxury. Just a broken car, a rainy drive, a 35-minute ceremony at twilight, and a marriage that has lasted forty years.
Her life in Sevagram unfolded differently in the years that followed Her story in Sevagram unfolded far beyond that modest wedding, and I have written about it in Part II – The Quiet Architect..
Ashwini Arrives
First Child, First Fever

The birth of a first child turns a household into a state of high alert. Every small symptom becomes a headline; every silence feels loaded with meaning. When Bhavana became pregnant with Ashwini, I lived in that peculiar mixture of excitement and nervousness that only first-time parents understand. We were happy, of course, but we were also watchful—listening to every new complaint, reading omens into every pause.
Bhavana conceived while she was preparing for her B.Ed. examinations. The due date landed inconveniently close—barely two weeks before her exams—because life rarely checks our schedules before making its plans. The first trimester passed smoothly, marked only by mild morning sickness which she handled without drama. In those days, there were no routine ultrasounds to reassure us, no colourful scans with neat measurements. We depended entirely on clinical judgement, experience, and the steady confidence of our obstetrician, Dr. Shakuntala Chhabra.
***
Dr. Shakuntala Chhabra
Dr. Chhabra was thirty-seven then, petite and youthful enough to be mistaken for a medical student until she began speaking. She spoke fast, moved briskly, and seemed powered by an internal motor that never needed rest. Her energy filled the ward. She possessed that rare gift of making patients feel that everything was under control—even when it wasn’t.
Over time, she and I had developed a warm professional rapport. She would call me for advice when medical complications appeared in her practice, and I admired the way she handled obstetrics with both confidence and care. She was serious about her work, but never solemn. She brought lightness into a space where families often carried heavy fear.
***
The Long Admission
In her second trimester, Bhavana began having episodes of preterm labour. Dr. Chhabra advised absolute bed rest. That is how Bhavana landed in Private Room No. 3 at Kasturba Hospital, where she stayed for weeks. It was a long admission, the kind that tests patience, stamina, and the ability to find meaning in small routines.
I spent most of my spare time with her. I brought meals, sat beside her bed, tried to look calm, and pretended that everything was normal. It wasn’t. But Bhavana, even then, had a steady core. She accepted the situation without melodrama. She worried, naturally, but she did not collapse.
To keep her spirits up, I turned to the only distraction I had at hand: poetry. I wrote short, rhyming, four-line verses for her every day. The Obstetrics residents began dropping in daily, not just to check the fetal heart rate, but to ask with a smile, “Today’s poem?” It became our small ritual—a private joke that turned a sterile hospital room into a place where life was quietly preparing to begin.
***
The Thirty-Six Hours
As the date approached, the fetal kicks grew less vigorous. Bhavana went "post-date"—a phrase that never brings comfort in obstetrics. She was admitted to the labour room, and Dr. Chhabra was determined—stubbornly, lovingly determined—that Bhavana would deliver vaginally.
Bhavana endured the hours with the quiet endurance she summons when she has no choice. Dr. Chhabra coaxed, encouraged, and used oxytocin, but the uterus refused to cooperate. Labour stretched on. Time began to feel heavy. After thirty-six hours of waiting, Dr. Chhabra finally recommended a caesarean section. She rushed to her quarters to freshen up, preparing for surgery.
Then came one of those moments that remind you how quickly medicine can pivot. When Dr. Chhabra returned, she reassessed Bhavana, looked at the situation afresh, and decided to make one final attempt. The nurses were instructed to prepare for a vaginal delivery. The room shifted gears instantly—quiet urgency, purposeful movements, everyone doing their part without fuss.
Bhavana pushed with everything she had left. A few intense moments later, we heard it—the first cry. A thin, fierce announcement that a new person had entered the world.
Ashwini.
Dr. Chhabra’s face broke into a broad, beaming smile. She looked triumphant, not for herself, but for Bhavana. I stood there overwhelmed—relieved, grateful, slightly stunned—watching the drama of thirty-six hours resolve into a single sound.
3:30 PM, 18 March 1986
Ashwini arrived at 3:30 in the afternoon. When I held him for the first time, I felt the kind of wonder that makes even a doctor feel unqualified. He was small, warm, perfect in the way newborns seem perfect—tiny fingers curled like question marks, toes that looked too delicate for this rough world.
Bhavana was exhausted in the most complete way possible. Yet she could not stop smiling. It was as if the pain had been erased by a single, sudden certainty: he is here. I watched her face and realised that childbirth does something extraordinary. It empties you, and then, in an instant, it fills you.
Those weeks in Private Room No. 3 changed us. They made us older overnight. And they gave us a memory that still feels bright, even after forty years.
Amrita Arrives

By late 1989, the geography of our lives shifted once again. We moved from the modest "Type 2" quarters near the school to a larger home in Vivekanand Colony. It was the kind of neighborhood that quietly shapes your social life without asking for permission. We were surrounded by Sevagram’s familiar stalwarts—Dr. Ghosh with his dogs, Dr. Ghuliani with his Scrabble board, and Dr. Naik with his Cine Club. In time, their habits became part of the colony’s soundtrack, as recognizable as the morning calls of vegetable vendors and the evening clatter of utensils.
The house felt like an upgrade in every sense—more space, more light, more air. It also felt like a small promotion in the unwritten hierarchy of campus living. Bhavana liked the order of it. I liked the convenience. Ashwini, now three-and-a-half, liked the novelty of new corners to explore. And soon, we had another reason to feel that life was moving forward.
***
Bhavana was expecting our second child. Ashwini was a busy, curious toddler who had mastered the art of asking questions at precisely the wrong time. He was thrilled at the idea of a new baby, though he hadn’t yet grasped the small detail that a baby comes with its own demands, and that parental attention is not an unlimited resource.
We were calmer this time. The first pregnancy had taught us how little control parents truly have and how much they must learn to trust the process. We knew the terrain better—both the emotional landscape and the hospital corridors.
***
On a quiet evening in October 1989, the waiting ended. Unlike Ashwini’s birth, which had felt like a long ordeal, this time there was a sense of calm readiness. The hospital was barely five minutes away from our new quarters. When labor pains began, we didn’t need a taxi or an ambulance. We simply walked.
Dr. Shakuntala Chhabra was there again. Her presence had the reassuring effect of a familiar landmark. The delivery was smooth. At 11:47 p.m., the silence of the night was broken by a new sound—the cry of a baby girl.
We named her Amrita.
Holding her, I felt something settle into place. We were now a family of four—the classic Indian ideal of Hum Do, Hamare Do. The house in Vivekanand Colony, which had felt a little large for just the three of us, suddenly felt full, as if it had been waiting for this fourth person all along.
***
While the adults were celebrating Amrita’s arrival, Ashwini provided the comic relief that later became part of hospital folklore.
During those days, the staff doted on him. He wandered around the waiting areas with the confidence of a child who knows he is welcome everywhere. One evening, Dr. Anuradha Gokarn—a lively house officer—spotted him playing and called out with mock seriousness.
“Ashwini! I heard you dressed up for the Staff Club party. What did you become?”
Ashwini puffed out his chest, pleased with the attention. “I became Lord Hanuman!”
Dr. Anuradha’s eyes twinkled. She looked him up and down and said, “Hanuman? But Hanuman has a long tail. You don’t have a tail. How did you become the Monkey God without a tail?”
Ashwini didn’t miss a beat. With the supreme confidence of a three-year-old who believes facts are negotiable, he said, “Oh, that was easy. I used Phali for the tail.”
Dr. Anuradha burst into laughter right there in the corridor. Ashwini meant phali—the long green bean that had been pinned to his costume. But to Dr. Anuradha, “Phali” meant something else entirely. It was the nickname of her fiancé and batchmate, Dr. Fali Langdana. The image of her future husband being used as a tail for a toddler’s Hanuman costume was too delicious to resist.
The story traveled through the doctors’ mess at the speed of gossip, which is faster than any ambulance. For days, it resurfaced at tea breaks and ward rounds, bringing a little laughter to the serious business of medicine.
***
With Amrita in the cradle and Ashwini supplying entertainment, the 1980s drew to a close. We were settled, we were happy, and we were blissfully unaware that the decade ahead would bring a revolution that would change how we worked, lived, and communicated. For the moment, though, our world was small and complete: a new home, a newborn daughter, a proud little boy, and the comforting feeling that life had arrived at a good place.
Akhtar’s Auto
While the hospital was modernizing, our personal lives revolved around a different kind of infrastructure: schooling. It is one thing to plan wards and workflows; it is quite another to plan a child’s education in a small town where choices appear suddenly, disappear quietly, and always come with conditions. In those years, Bhavana and I discovered that raising children is essentially a series of decisions taken with incomplete information, followed by long periods of hoping you chose wisely.
Ashwini’s early schooling was eclectic—a tour of Sevagram’s educational landscape. He began at Mahila Ashram, a Gandhian school with a Marathi-medium curriculum and a simplicity that suited the place. Then came Agragami Convent in Wardha for three years, and later, Kasturba Vidya Mandir in Sevagram for the fourth grade. Kasturba Vidya Mandir had one unbeatable advantage: it was across the road. Ashwini could roll out of bed and walk into his classroom, half-awake and still chewing his breakfast.
***
In the mid-1990s, a new institution appeared, and with it came a new kind of parental restlessness. Bharatiya Vidya Bhavan opened a campus at the Lloyd’s Steel Factory in Bhugaon. It was called Lloyd’s Vidya Niketan, and it promised what every ambitious school promises: a rigorous English-medium education, good facilities, and the reassuring glow of a famous name.
Bhavana and I were impressed by the Bhavan’s reputation, and we made a decision that felt bold at the time. We would move both Ashwini—now entering fifth grade—and Amrita to Lloyd’s. They passed the entrance test, and we paid a refundable deposit of Rs 10,000. It was refundable, yes, but it was still Rs 10,000—an amount that carried real weight in those days, even when spoken casually.
***
We had solved the admission problem only to create a logistical nightmare. Lloyd’s was in Bhugaon, fifteen kilometers from Sevagram. Unlike city schools, there was no neat yellow bus turning up at your gate. We had traded a school across the road for one that required a daily expedition.
We were not alone. Dr. Prakash Behere, a psychiatrist who had returned from the UK, was also looking for transport for his sons, Aniruddha and Shashank. Dr. B.S. Garg’s daughter, Neha, faced the same problem. So did Aditya Farsole from Wardha. We formed what can only be described as a coalition of anxious parents—polite in conversation, slightly desperate in intent. We needed a chariot for our children, and we needed it quickly.
***
The solution arrived in the form of Akhtar.
It was Mr. Farsole who found him—almost by accident—at a time when we were discovering, with mild embarrassment, how few of us actually owned a car. Akhtar was willing to do the long daily run, which in itself made him a rare man. He was tall, thin, and so soft-spoken that you sometimes had to lean in to catch his words. He drove his auto with a caution that was almost philosophical. At times, the pace was so leisurely that the children could have stepped out, walked a few paces, and climbed back in without the vehicle needing to slow down.
He tried, occasionally, to discipline his passengers, but children have their own democracy. They listened when they felt like it and ignored him when they didn’t. The auto was a tight squeeze, yet it worked. Every morning the "Lloyd’s Auto" buzzed through Sevagram and Wardha, collecting Ashwini, Amrita, Shashank, Neha, and Aditya. That three-wheeler became their moving clubhouse. For the thirty minutes it took to reach Bhugaon, they bonded over jokes, complaints, last-minute homework, and the rhythmic bumps of Wardha roads. Akhtar, in the front, drove as if he was transporting fragile glass.
***
The commute was long, but it turned out to be worth it. Under the leadership of the Principal, Mr. Dass, and his wife—who became friends and even invited us to the school—the children flourished. Lloyd’s gave them more than an English-medium education. It gave them a circle, a shared life, and the confidence that comes from belonging.
Ashwini found his tribe quickly—Shashank Behere, Aaditya Jain, Vaibhav Patni, Gayatri Saraf, Vikram Belkhode, Tahsin Taaj, Ram Agrawal, and Sudhir Rawlani. Many of them later became doctors or dental surgeons, which is what happens when bright children grow up around a medical campus and begin to think stethoscopes are part of the natural world. Amrita built her own world too, with friends like Abhilash Dass, Neha Bhomiya, and Mahodaya.
Looking back, I realize that the real education did not happen only in classrooms. It happened in that auto-rickshaw, in shared tiffins, and in the small negotiations children learn to make every day.
***
There is a pleasing circularity to life. Today my granddaughters, Diti and Nivi, go to the same school where Ashwini and Amrita studied. They travel in a school bus now—comfortably, safely, with a driver who does not whisper and a vehicle that does not invite children to get out and walk. They enjoy the same bonhomie their father and bua once did, only with better suspension.
What has changed most is not the school, but the parenting.
Modern parents attend monthly teacher-parent meetings with the seriousness of a board meeting. They sit for hours, discussing unit tests and "part-completion" scores, dissecting marks into neat categories like stock market graphs. There is a great deal of diligence in it, and also, if I may say so, a great deal of anxiety.
Bhavana and I never attended a single such meeting during the six years our children were at Lloyd’s. We never "projected" them. We didn’t negotiate grades. We were, in this one matter, blissfully relaxed—perhaps even irresponsibly so by modern standards. And yet, they never let us down. They studied, they grew up, and they found their way without us hovering over their report cards like anxious auditors.
In the end, that may be the quiet truth of parenting: you do your best, you make a few sensible decisions, you worry more than you admit, and then you step back and let the children become themselves.
Guidance Point
Destiny rarely announces itself. More often it slips in quietly, disguised as an ordinary day. For Ashwini, it arrived through a coaching class in Nagpur.
In the early 2000s, Nagpur had become the natural migration site for medical aspirants from across central India. Students travelled in with holdalls and anxious parents, rented small rooms, and disappeared into libraries and classrooms. The days were long, the food forgettable, and the conversation always circled back to ranks and cut-offs. It was hardly a romantic setting, yet this is where many modern love stories begin—between notes, mock tests, and shared worry.
In April 2004, Ashwini was preparing for the entrance examination of the Mahatma Gandhi Institute of Medical Sciences. Wardha’s easy pace no longer suited the intensity he needed, so he moved to Nagpur. Rajabhau Khapre from our Pharmacology department offered him a small room in Giripeth, a practical kindness that, unknowingly, set the stage for everything that followed.
***
At Guidance Point on West High Court Road, Ashwini joined a batch of equally tense students. Among them was Shaily Jain, an eighteen-year-old from Kunkuri, who had studied at Carmel Convent in Raigarh and had come to Nagpur with the same dream. She stayed in Bajaj Nagar and carried herself with a quiet seriousness, the kind you see in students who know that effort, not luck, will decide their future.
There was no dramatic introduction. They began the way most friendships begin—sharing notes, discussing questions after class, walking out together after long tests. Anxiety is a great equaliser; it dissolves formality. Familiarity grew almost unnoticed.
Around that time, my elder sister Pushpa lived in Giripeth, close to Ashwini’s room. Every Sunday I travelled by bus from Wardha to Nagpur to spend the day with them. Those Sundays were not leisurely visits. I carried sheaves of notes and a sense of duty, because my task was to coach Ashwini—and whoever else turned up—for the most feared component of the entrance test: Gandhian Thought.
***
In the MGIMS system, Gandhian Thought could undo a brilliant student. No matter how well you scored in Physics, Chemistry, or Biology, failing to cross the minimum marks in that paper meant the end of the dream. I had spent months condensing Gandhi’s autobiography into handwritten summaries and questions.
Our sessions became routine. A few students would sit cross-legged on the floor with notebooks open while I spoke, drawing diagrams on scrap paper and translating philosophy into plain language.
One Sunday, Ashwini arrived with Shaily.
She sat quietly at first, almost apologetic about taking up space, but her attention never wandered. When I paused to ask a question, she answered softly but precisely. She didn’t merely memorise; she seemed to think her way through the ideas. Over the weeks she kept returning, and gradually her shyness faded.
What I remember most is not any particular conversation, but the ease between the two of them. They sat side by side, sharing a book, arguing gently over answers, laughing at small mistakes. Nothing theatrical. Just the unselfconscious companionship of two young people walking the same steep road. I was teaching them Gandhi, but in those afternoons they were learning each other.
***
n April 2004, Ashwini and Shaily travelled to the Hislop College centre in West Nagpur to take the entrance examination for the Mahatma Gandhi Institute of Medical Sciences. Like hundreds of others, they walked out with admit cards folded into their pockets and a silence that comes only after long exams.
Entrance results rarely distribute joy evenly.
When the results came, the news hit us hard. Shaily’s name was missing. Ashwini had done well, but for the two staff seats he stood third—close enough to imagine success, far enough to lose it. For a day or two the house fell unusually still. We moved about normally, spoke of ordinary things, and avoided the subject because there are disappointments for which parents have no useful sentences.
So we turned, as families do, to a practical alternative. Ashwini enrolled at Fergusson College in Pune for Biotechnology. He packed methodically and tried to sound cheerful on the phone, but the detour weighed on him. For a boy who had grown up wandering hospital corridors and treating stethoscopes like toys, anything other than medicine felt temporary, as though he were waiting in the wrong queue.
***
That year I left for the United States to begin my MPH at University of California, Berkeley. I told myself it was necessary, yet a part of me wondered if I was chasing my own growth while my son struggled with his.
A few weeks later the waitlist moved, a seat opened, and Bhavana called to say simply, “He got in.” Ashwini returned to MGIMS. I thought the crisis had passed.
Then, in July 2006, an email arrived that unsettled me more than any entrance result.
But success in the exam did not bring immediate peace. While Shaily began her own journey of recalibration elsewhere, our home was facing a silent storm.
In 2006, Ashwini sent me an email that served as a clinical awakening for me as a father. It was a mirror held up to my own obsession with work, forcing me to see the "other side of the coin."
Ashwini wrote that he felt I was always busy—at the hospital, with a book, or on the laptop—and that we were living like strangers in the same house. He did not want advice or money. He wanted time. And then, plainly and without drama, he added that Shaily was the person he wanted to spend his life with.
It read less like rebellion and more like a plea. For the first time, I realised that while I had been busy being a professor, I had forgotten to be a father.
***
Shaily’s first email arrived on 16 January 2005. It opened with a careful “Dear Uncle,” the kind of address that carries both respect and distance. The note was measured and direct. She did not ask for favours; she asked for guidance—what to read, how to prepare, what options remained if one door closed.
When dentistry proved too expensive and government seats too scarce, she adjusted without complaint and joined Biotechnology Engineering in Raipur. That quiet course correction impressed me more than any entrance rank. Many students cling stubbornly to a single dream and lose heart when it slips away. Shaily simply chose the next path and kept walking.
Over the months her emails grew less formal. They began to include small details of her life—debates she had entered, articles she was reading, poems written late at night. Without noticing, we had slipped into an easy correspondence. I would reply like the teacher I have always been, marking up her drafts, fussing over margins and font sizes, pretending to discuss formatting while smuggling in affection.
***
When Shaily first met Bhavana, the formalities lasted barely five minutes. After the initial greetings, Bhavana asked her a few simple questions—about her parents, her studies, how she had managed alone in Nagpur—and then mostly listened. That is her way. She watches quietly, storing impressions, saying little. By the end of the visit she was already moving about the kitchen as though nothing unusual had happened, but I knew the evaluation was complete.
The same day she wrote to me, in her characteristically brief style: “I feel relieved. Ashu has chosen well.” In our home, that sentence carried the weight of a blessing. Once Bhavana says yes, the road ahead clears almost on its own.
In January 2010, that quiet assent took us to Kunkuri for the engagement. As we entered the venue, a large banner announced, Patni Family Welcomes You. Someone explained, with pride and a laugh, that this was their Jain sub-tradition, and we found ourselves folded into it without ceremony. What stayed with me, though, was not the banner or the rituals but the sight of a granite church rising from the red soil of the small town—solid, unexpected, and serene against the sky. I remember thinking that Shaily was much the same: steady, self-possessed, and quietly present, as though she had always belonged there and we had simply taken time to notice.
***
Years later there is a symmetry that still amuses me. The boy who once hid between the pillars of the department now teaches there. Ashwini is a Professor in the same institution where he once chased dragonflies as a child. Shaily, trained as an engineer, found her place in hospital administration, moving through wards and offices with the same steadiness she once brought to coaching classes.
They live with us in Sevagram with their daughters, Diti and Nivi. Our days overlap—home, hospital, school—all within walking distance. It is an ordinary life, and therefore a deeply satisfying one.
Looking back, nothing about their story felt dramatic at the time. It grew quietly—through shared notebooks, Sunday classes, hesitant emails, and one honest letter from a son to his distracted father. That, more than anything else, was when I understood that love does not arrive with trumpets. It enters softly and stays.
***
The Sevagram Symphony: A Monsoon Wedding
Fixing a wedding date in an Indian household rarely begins with the stars. It begins with the calendar. By the spring of 2011 ours lay open on the dining table, squares filled with pencil marks, arrows, and crossed-out plans. Shaily’s engagement at Kunkuri had been small and affectionate, but the wedding would draw far larger numbers, the sort that gather naturally around a campus family where everyone knows everyone else. Kunkuri, charming as it was, simply did not have the space.
The mind moved quickly to the next practical question. Amrita’s final MBBS examinations were due at the end of the year. Ashwini, fresh from internship, was preparing for the Australian medical entrance. If we postponed, the wedding would drift into 2012, and life would scatter us in different directions. So we chose July 9 and closed the diary before anyone could change it.
In Wardha, July is less a month than a mood. The monsoon arrives like a strict schoolmaster, uninvited but authoritative. Some days it drizzles politely; on others it floods the streets without warning. We had three months to prepare for a thousand guests and whatever sky decided to accompany them.
***
I have always had an allergy to what I call “wedding English”—that ornate language of “benign presence” and “cordial solicitations” that sounds as if borrowed from a government circular. This was not a printed card anyway, only an email to old friends, and I wanted it to sound like us: plain, slightly amused, aware of time passing faster than we liked.
One evening I sat at the dining table with my laptop open, typing and deleting, typing and deleting again, trying to find the right beginning. Finally I wrote what felt simplest and truest:
How quickly children grow up—or perhaps it is we parents who grow old faster.
The arithmetic, I realised, was unforgiving. Somewhere along the way I had crossed fifty without noticing,
and Ashwini, who had once needed pocket money for comic books, was suddenly half his mother’s age and ready to be married.
A few more lines followed.
That sounded less like an announcement and more like a conversation, so I pressed send.
When it came to drafting the wedding invitation email, I turned to my old friend Dr V. K. Gupta, the Allahabad pathologist, and we would talk over the phone, sometimes late into the night, polishing each sentence until it finally sounded like us.

***
We had built our house on Gandhi Ashram Road a year earlier, opposite the old hospital building. In front of it lay four acres of scrub and wild grass. For weeks we entertained the romantic idea of hosting the reception there. Under the dry June sun the ground looked generous and welcoming, a green spread where a thousand chairs might fit comfortably.
Then the first rains came, and the black cotton soil of Sevagram revealed its nature. The surface softened overnight. Shoes sank. A labourer took two steps and disappeared ankle-deep in mud. Walking required negotiation. We stood watching, trousers splashed, and quietly abandoned the plan.
We shifted instead to the large ground behind the Dean’s office. Ironically, we had once lived directly across from it. It was not picturesque, but it was firm. In a Sevagram monsoon, firm ground is a luxury.
***
On 8 July 2011, Shaily’s family—seventy-five strong—arrived from Kunkuri and settled into the Yatri Niwas Wardha opposite the Gandhi Ashram Wardha. Other guests occupied Arogyadham, vacant flats, and the guest house. For two days the colony lost its boundaries. Doors remained open. Someone was always brewing tea. Children ran in and out of unfamiliar houses as though they had lived there for years.
There were no event managers, no headsets, no printed schedules. Instead, there was Parmanand Tapadiya. A chartered accountant by profession, he carried himself with quiet authority and knew half the town by name. He did not assemble a team; he simply mentioned what needed to be done, and people stepped forward.
Doctors, shopkeepers, and businessmen found themselves checking bathrooms, tasting dal, arranging mattresses, and directing guests. No one spoke of “coordination.” They simply worked.
***
Ashwini once suggested that the ceremony be held inside the Ashram grounds. We had to gently refuse. The Ashram’s silence does not sit comfortably with wedding drums. We chose the Yaatri Niwas instead, a modest government guest house a kilometre away.

Radiant beginnings: Shaily on her wedding day, July 2011.
The ceremony followed the Wardha method, shaped by Vinoba Bhave and Kaka Kalelkar—simple, unhurried, and free of excess—and it concluded, almost to the minute, in thirty-five quiet minutes. We chose Godhuli Bela, that soft hour when cattle return home and the light turns dusty gold. There were no loudspeakers and no theatrics—only the low murmur of mantras and the faint smell of ghee and smoke. Watching Ashwini and Shaily sit side by side, calm and attentive, I felt the familiar parental astonishment at how quickly childhood folds into adulthood.
Ceremonial traditions: Ashwini during the wedding festivities, July 2011.
***
The reception began about an hour later. By then the clouds, which had threatened us all week, simply held back, as though granting us a brief reprieve. After weeks of watching the sky with suspicion, we stepped out onto dry ground. Guests kept arriving in a steady stream until the count crossed twelve hundred. They blessed the couple, filled their plates, returned for second helpings, and lingered long after the formalities were over, talking in small circles as dusk slowly gathered.
By the time the final guest left and the colony returned to its usual quiet, the lesson felt obvious. In a place like Sevagram you do not purchase a wedding. You grow it. The weather may misbehave, the soil may sink underfoot, and the guest list may outnumber the chairs, but when friends show up at three in the morning, rebuild a rain-soaked stage, and serve food with their own hands, everything else falls into place. The mud dries. The lights go out. What remains is the memory of having stood together in the rain.
***
Much of the wedding now blurs into a procession of folded hands and smiling faces, but four scenes remain steady in my mind, as clear as if they were lit by a brighter lamp than the rest.
The stage was the first. It became, almost by accident, the heart of the reception. Atul Patel, Amit Gandhi, Anil Kusumbia, Prem Jethwa, Raju Fattepuria, and Raju Verma refused the easy option of hiring a decorator. They wanted something that belonged to Sevagram, something that looked as though it had grown from the soil rather than arrived in a truck. For days they hammered planks, tied gunny cloth, spread plaster of Paris with their palms, and combed it into gentle curves. Gaju Rudrakar arrived with his brushes and added Warli patterns along the surface, and slowly the structure began to resemble a large village hut—simple, earthy, and unmistakably ours.

Built with love: Family friends working tirelessly on the reception stage, July 2011.
One evening a sudden downpour washed half the plaster away, reducing the hut to dripping streaks of white. No one complained. They stayed back under torchlight, sleeves rolled up, hands grey with lime and mud, repairing the damage through the night. By morning the stage stood ready again, sturdier for the setback, carrying the quiet pride of the people who had built it themselves.
Hospitality unfolded with the same quiet competence. Shrikant Gandhi and Shyam Kuldhariya moved between guest houses with lists in their pockets, checking bedsheets, buckets, and drinking water as though running a small hotel. At the Yatri Niwas Wardha, Pradeep Bajaj and Om Jogani were everywhere at once—guiding families to rooms, arranging extra mattresses, finding tea for those who had travelled all night. At three in the morning, when most of us were asleep, Ajay Rathi and Vishal Rathi stood at the Wardha railway station, waiting for late trains and greeting half-awake relatives with the reassurance of familiar faces, so that no one arrived feeling like a stranger.
Food came next, and with it the wisdom that an Indian wedding is remembered less for its speeches than for its dal. P. L. Tapadiya brought in Mr Tolaram, who understood this truth instinctively. From dawn the fires were lit and the large vessels rarely empty. Volunteers tasted, adjusted salt, and stirred again. The meals were generous and comforting—food that invited second helpings and long conversations rather than photographs. No experiments, no theatrics, just the steady pleasure of a community eating together.
Cleanliness, though less visible, held everything together. Akhilesh Sinhal and Rupesh Sinhal quietly took charge, moving about with mops, buckets, and an endless supply of water. In the middle of the monsoon, with hundreds of muddy feet crossing the grounds, they kept the place orderly and dignified. Guests rarely noticed their work, which was precisely the point.
Looking back, these tasks—building, hosting, cooking, cleaning—seem modest on paper. Yet it was these very acts, carried out without fuss by people who considered the wedding their own, that held the celebration upright.
***
The Hands That Carried the Wedding
At the centre of everything stood Shri Parmanand Tapdiya, quietly holding the threads together and making sure nothing unravelled.
At the Yaatri Niwas and the guest houses, Pradeep Bajaj, Om Jogani, Harish Kachliya, Sunil Kela, Sanjay Taori, Shrikant Gandhi, Shyam Kuldhariya, Sunil Patel, Ravindra Rathi, Vijai Kharangana Rathi, Kamal Sinhal, Bharat Somani, Gopal Taori, and Kishore Fattepuria moved from room to room, arranging beds, water, and tea, receiving each arrival as though welcoming family home.
In the kitchen, Nandkishore Bhutada, Bablu Chaube, Ashok Goyanka, Dilip Jajodia, Gopi Jajodia, Harish Mudia, and Shyamsundar “Pappu” Rathi watched over the bhojan, while Ramprasadji Gautam guarded the stores and Bharat Doshi ensured breakfast appeared on time, every time.
The stage took shape under the hands of Rajendra Fattepuria, Amitkumar Gandhi, Prem Jethwa, Anil Kusumbia, Atul Patel, Rajabhau Umate, and Raju Verma, who built it plank by plank until it felt less like a structure and more like a part of Sevagram itself.
During the reception, Sunil Chandana, Shyam Taori, Bhogibhai Gorsia, Gauri Tibdewal, Ulhas Jajoo, Suhas Jajoo, Yogendra Fattepuria, and Pappu Taori kept the flow steady, guiding guests, solving small crises, and making the evening feel effortless.
The rituals were conducted with care by Damodar Darak for the pooja, Vijay Mohta for Ganesh, and Sushil Vyas for the baraat, their voices carrying the ceremony forward without haste.
And at the margins, where the hardest work often hides, Ajay Rathi and Vishal Rathi waited at the station for late-night arrivals, Mahesh Mokalkar, Vinod Sinhal, and Asif Bhai kept the vehicles moving, while Akhilesh Sinhal and Rupesh Sinhal quietly kept the grounds clean, so the celebration could proceed with dignity.
By the time the last guest departed and the heavy Wardha silence returned to the colony, I was struck by a simple realization. A wedding in a place like Sevagram is not an event you buy; it is an event you earn.
If anyone asks me what I learnt from that monsoon wedding in 2011, I give the simplest answer: the weather is unpredictable, the soil is stubborn, and the guest list always grows beyond the capacity of the chairs. But when fifty-four friends show up in full strength—to greet guests at 3:00 AM, to rebuild a rain-washed stage, and to serve food with their own hands—everything else becomes manageable. In the end, the mud dries, the clouds part, and what remains is not the exhaustion, but the profound, shared satisfaction of a community that knows how to stand together in the rain.
.
Amrita and Sahaj: A Sevagram Story
In 2013, our daughter Amrita moved through her MBBS with the quiet focus of someone on a private mission. While others studied in bursts before exams, she kept a steady routine, rising early, reading late, and treating each posting as if it already mattered. She finished first in her first year, then again in her second, and once more in her final year, collecting gold medals so regularly that relatives stopped sounding surprised and simply nodded, as though this was expected.
At MGIMS, achievement came with an obligation. Before postgraduate training, every graduate had to serve two years at a rural health centre. Postings were allotted strictly by merit, and ranked second in her class, Amrita could have chosen something comfortable and close to home. Instead, she chose Pargaon near Kolhapur.
Pargaon was little more than a health centre, a few houses, and long stretches of road that dissolved into fields. Evenings fell early, buses were uncertain, and silence lingered. She cooked for herself, washed her own clothes, and often ate alone with a book propped against a tumbler. What sustained her was friendship. Every Friday, Girish Mote rode twenty-five kilometres to drop her at the highway so she could catch the bus to Pune for coaching classes, while Apurva Kulkarni, Anuj Birbal, and Prerna, Anuj’s fiancée cared for her in Pune with food, gossip, or simply company. Her eventual DNB in Radiology belonged as much to that small circle as to her own effort.
***
The proposal that would take her from Pargaon to Delhi began quietly one evening at our dining table. We had finished dinner and were lingering over ice cream when Shaily, my daughter-in-law, mentioned an old classmate from Raigarh. She said his name casually, almost as an afterthought: Sahaj Rathi. The conversation moved on, but the name stayed.
Sahaj had trained at the Armed Forces Medical College and later completed his MD at University College of Medical Sciences. His father was a cardiologist at Max Super Speciality Hospital Saket and his mother ran ultrasound clinics in Patparganj. Vidushi, his sister was doing Medicine at Lady Hardinge. They belonged to the polished world of Delhi medicine. We were Sevagram people, shaped by a village campus where excitement meant a good seminar or a generous monsoon, and we worried that our simplicity might appear provincial.
When we visited them in Delhi that December, we carried that nervousness with us. Dr Rajiv opened the door himself and ushered us in, and within minutes we were seated around the table with tea and snacks, talking over one another like relatives. Later, at the Hilton Garden Inn Mayur Vihar, they casually suggested hosting the wedding there. We thanked them and asked for Nagpur instead. They agreed at once, and the ease of that conversation told us everything we needed to know.
***
We fixed the date for June 20, 2014. Rani Kothi, our first venue on Wardha Road turned out to be an unfinished construction site, and two months before the wedding we began again. One evening we drove to Nagpur and walked into the Radisson Blu Hotel Nagpur with a list of requirements. Shri Parmanand Tapdiya sat across the manager with his small notebook and patiently negotiated each line, crossing out numbers until a fresh sheet appeared. The hall was booked that day. When we still fell short of rooms, my nephew Amit Singh suggested the Airport Centre Point Nagpur, which solved the problem neatly.
Those weeks meant repeated journeys on the old Wardha–Nagpur road, dusty and broken, but slowly the confusion settled into order.
***
As the wedding approached, friends arrived not as guests but as workers. Alumni returned from Delhi, Haryana, Bhopal and elsewhere, and the reception ground near GC Commerce College Wardha felt less like a venue and more like a reunion. Old ward stories resurfaced, jokes travelled from group to group, and for a few hours we were residents again.
Work happened quietly in the background. Rupesh Sinhal and Om Jogani stood at the railway station from dawn, receiving each arrival. Tarvinder Singh Oberoi placed his fleet of cars at our disposal. Ashok Goenka handed over the keys to his new car without ceremony. Ajay Rathi opened his newly built house near the hotel to our volunteers, and it became our refuge, with mattresses on the floor and tea constantly brewing. Years later, when he died of a sudden stroke in that same room, the memory returned with unexpected force; the house that once sheltered our celebration had also witnessed his final hours.
Even the banquet hall offered its own small comedy when two friends (Vinod Sinhal and Vinod Fattepuria) caught staff removing untouched plates to inflate the bill, after which several of them began sharing plates in mock protest, laughing as though they were back in hostel days.
***
On the wedding day, Amrita stood beside Sahaj, radiant and composed, and I found myself thinking of the young doctor riding pillion on a motorcycle along the Pargaon highway, clutching her bag against the wind. The journey from that lonely health centre to this bright hall seemed impossibly long and yet perfectly natural. She was leaving for the capital, but she carried Sevagram with her—its grit, its friendships, its quiet strength.

By the time the vidai came, the hall had grown still. Garlands lay wilted, chairs were stacked aside, and relatives embraced her one by one. She hugged everyone steadily and smiled, giving small practical instructions about calling when they reached home. Not a single tear fell. Bhavana stood beside her, calm as always. When the car pulled away, Amrita simply waved through the window, and that quiet steadiness, more than any display of grief, stayed with us long after the lights went out.
***
The festivities did not end with the departure of the baratis from Nagpur. The next morning, the centre of gravity shifted back to Wardha. If Nagpur had been about bookings, room lists, and the choreography of arrivals, Wardha felt like a return home. This was where the people who had watched Amrita grow up gathered to celebrate—the nurses who remembered her wandering through hospital corridors as a toddler, the professors who had guided her through exams and postings, and the neighbours who had seen her wobble past on her moped with a satchel slung over one shoulder. They came not merely as guests, but as stakeholders in her story.
Friends and relatives travelled in from every corner of the country. A large group of alumni from MGIMS—now practising in Delhi, Mumbai, Punjab, Haryana, and Bhopal—found their way back to Sevagram as though memory itself had called them home. They arrived with small bags and large memories, slipping easily into the old ease of hostel days.
I was particularly moved to see Dr Manoj Singh, my student from the 1990 batch and now an accomplished intensivist. He had flown in from Australia for no reason other than this wedding—no conference, no errand, simply affection.
***
By evening, the open ground near GC Commerce College Wardha looked less like a reception and more like a reunion. Groups formed and dissolved. Someone revived a chaotic night duty from years ago; someone else retold a hostel prank. Laughter travelled across the field, hands clapped shoulders, and for a few hours the years fell away. We were residents and students again, speaking the effortless language of a shared past.
As I watched Amrita and Sahaj on the stage, greeting each well-wisher with folded hands and patient smiles, a quiet calm settled over me. She was leaving for the capital, yes, but not empty-handed. She carried the blessings of the village that had raised her and the city that had shaped her.
An event of this scale, moving between Sevagram’s quiet lanes and Nagpur’s restless traffic, could not have run on plans alone. It rested on many steady hands and willing hearts, each doing a small task without fuss until the day unfolded as though it had arranged itself.
What follows is the circle of friends and family who quietly took charge, each doing a small part, and together making the day flow without a ripple.
The Hands That Made It Happen
At the centre: Shri Parmanand Tapdiya, who quietly held every thread together, with Ashok Goenka, ready wherever an extra pair of hands was needed.
Welcoming our guests: Rajendra Fattepuria, Bhogibhai Gorsia, Vijay Rathi, Bharat Somani, Parmanand Taori, Bharat Doshi, Suhas Jajoo, Chandu Fattepuria, and Shrikant Gandhi, who managed hotels, rooms, and late-night arrivals with unfailing patience.
Travel and transport: Om Jogani and Rupesh Sinhal at the railway station, Vinod Sinhal with the vehicles, and Sunil Patel bringing guests safely from Wardha.
Arrangements and provisions: Gopi Jajodia, Sunil Kela, Sanjay Taori, Atul Patel, Raju Verma, Ajay Rathi, and Parsan Kothari, who ensured that every ceremony had what it needed — from fruit baskets to train tiffins.
Hospitality: Bhogibhai Gorsia, Suhas Jajoo, Chandu Fattepuria, and Shrikant Gandhi, whose warm manuhar made every guest feel at home.
Amrita’s Gold
Success is usually presented as a photograph: a smile, a certificate, a stage, applause. But its real beginnings are far less glamorous. They are often found in the dark, quiet hours when the rest of the town is asleep and only the determined are awake.
***
For Amrita, those beginnings were in Wardha.
After doing well in her tenth standard, she enrolled at Jankidevi Bajaj Science College. College, however, was only the baseline. The real work happened elsewhere—at tuitions, in notebooks, and in the daily discipline of showing up even when you didn’t feel like it. I still carry a vivid image from those years: Amrita and her friend Anvi, bundled up against the winter chill, riding a moped through the pitch-black streets to reach Professor Chaudhary’s chemistry class.
The roads were deserted. Stray dogs owned the silence. Streetlights were patchy. Yet day after day, the two girls navigated those empty lanes with the single-mindedness of people who know that effort is not optional. It was not bravery in the dramatic sense. It was routine bravery—the kind that goes unnoticed because it repeats itself every morning.
***
When the time came for the Pre-Medical Test (PMT), Amrita moved to Nagpur. She stayed in a rented room at Chhatrapati Square with Anvi and Rutuja Gangane. They lived the spartan life that serious students live without making a fuss about it. They rented a cooler and a fridge for Rs 500. They ate tiffin food. They studied until their eyes blurred and their backs ached. Their world shrank to textbooks, test papers, and the constant anxiety of time running out.
When the results came, there was an irony that still makes me smile.
Amrita had mastered calligraphy—her answers looked beautiful, as if handwriting could charm examiners into generosity. She scored brilliantly in the science group. But in the Gandhian Thoughts paper—the subject that our institute takes seriously, almost as a moral signature—she barely scraped through: 26 out of 60.
She was heartbroken. I tried to console her with the standard adult line: exams are subjective, marks don’t always reflect knowledge, life is bigger than one paper. She wasn’t interested in philosophy. She was interested in fairness. Fortunately, her science scores were strong enough. She secured admission to MGIMS. The news spread fast, as good news does in Wardha. My little girl was going to be a doctor.
***
Medical school is hard. It becomes harder when your father is a professor in the same institute.
Like Ashwini before her, Amrita walked the corridors of MGIMS with an invisible backpack full of expectations. She was constantly watched. If she did well, there were whispers: "She is Dr. Kalantri’s daughter—of course she’ll do well." If she slipped, the whispers would have been worse.
So she did what sensible children of professors learn to do early: she worked harder than necessary. Throughout MBBS, she consistently ranked among the top three in her class. She didn’t argue with gossip. She answered it with marks.
***
Amrita was not only a student with good grades. In 2012, during her internship, she surprised me with a feat that felt almost unreasonable for a 23-year-old. She decided to organize Medicon 2012, a national research conference for undergraduates.
Organizing a conference in a metro city is one thing; organizing it in Sevagram is an exercise in sheer willpower. But Amrita didn't just want to host an event; she wanted to make a statement. The theme she chose was “Return to Your Roots,” a challenge to young doctors to look beyond textbooks and understand the ground realities of Indian healthcare.
For months, our lives revolved around the Hospital Information System room near the Obstetrics gate, which had been converted into her "War Room." She led the MGIMS team as the Organizing Secretary, but in practice, she was the CEO, the diplomat, and the crisis manager all rolled into one.
She rallied her batchmates and the students from the 2010 batch, transforming a group of tired interns into a fiercely efficient workforce. The atmosphere was electric. They worked with the frantic, joyous energy of a family preparing for a wedding. They secured computers, haggled with printers, designed brochures, and turned a quiet corner of the hospital into a buzzing headquarters.
The guest list was intimidating. Amrita was coordinating with legends: Dr. Vinay Kumar (the editor of Robbins Pathology, a name every medical student reveres), Dr. Abhay Bang, Dr. Binayak Sen, and Dr. Sanjay Nagral.
I watched her interact with them—not as a fan, but as a host. She managed their schedules, their travel, and their expectations with a poise that I, even after decades of teaching, found enviable. When Dr. Vinay Kumar walked the corridors of MGIMS, it wasn't the faculty who were running the show; it was Amrita and her team.
Perhaps the moment that made me proudest happened before the conference even began. Organizing a four-day event for 400 students requires money. The easiest path is always the Pharmaceutical Industry, which is usually eager to sponsor such events in exchange for visibility.
Amrita and her team said no.
They made a deliberate, ethical choice to reject Pharma sponsorship. Instead, they raised funds through delegate fees, the Forum for Medical Students’ Research (INFORMER), and institutional support from MGIMS. They secured grants from the Lady Tata Trust and the BMJ Group. They negotiated prizes and travel grants from ICRAG (International Clinical Research and Global Health). They proved that you could run a world-class academic event without compromising your independence.
From July 11 to 14, 2012, Sevagram transformed. Over 400 students from across India descended on the campus. The air was thick with ideas—stem cell research, public health debates, Clinical Pathological Correlations (CPC), and fiery panel discussions.
I stood at the back of the auditorium, watching Amrita move through the crowd. She was everywhere—solving technical glitches, greeting delegates, ensuring the food was ready, and keeping the timeline ticking. She looked exhausted, yes, but she also looked completely in her element.
That was the moment I realized she had outgrown the label of "student." She was no longer just learning medicine; she was shaping the conversation around it. She was becoming a leader.
***
That same year, she gave me another glimpse of her temperament. She was selected for the MVPM Scholar Award—one of only five students from the community to receive it. The ceremony was in Pune.
As we settled into the AC compartment of the Nagpur–Pune Express, I began worrying like an anxious parent who cannot stop himself. Amrita hadn’t prepared a speech.
"You need to rehearse," I urged her.
She brushed it off, put on her headphones, and looked as calm as if she were going for a picnic. I spent the night tossing and turning, imagining her freezing on stage. In the morning, as we took a taxi to the auditorium, I saw her typing furiously on her iPad.
"What are you doing?" I asked. "Writing my speech," she said casually.
My heart sank. Last minute. The worst kind of planning. The kind that gives fathers hypertension.
But when she took the stage, she was effortless. She didn’t read; she conversed. "I cannot tell you what to do… because I don’t have a clue either," she told the audience. "But here I am. So I must have done something right."
She quoted Maya Angelou. She spoke of resilience. She held the room in the palm of her hand. The hall erupted in applause. I sat there with the familiar mixture of pride and embarrassment that fathers experience when their children prove them wrong. She knew exactly who she was.
***
Marriage to Sahaj took her to Delhi, but it did not soften her ambition. If anything, it sharpened it.
She entered the demanding world of DNB residency, choosing Radiology at Mata Chanan Devi Hospital. She hoped for work–life balance, but the balance came with a price. She was the only candidate. There were no peers to exchange notes with, no lively group discussions after duty hours, and teaching support was sparse.
Many people would have complained. Amrita did what she usually did: she found a way around the problem. In the evenings, she went to Ganga Ram Hospital and the Army Base Hospital to learn MRI and CT reporting. She became, in effect, a self-taught radiologist—built not by a perfect system, but by stubborn effort.
***
Then came the final test: the DNB examination. The passing rate is notoriously low, and the practical exam has a reputation for being a black box. You walk in prepared and walk out uncertain.
When the results were declared on 22 September 2018, I was stunned. Amrita hadn’t just passed. She had secured the First Rank in India. She was the Gold Medallist.
***
How does a father react when his daughter achieves something that feels almost unreal? Do you announce it loudly? Do you stay silent and savour it privately?
Bhavana and I sat in the audience at Vigyan Bhavan, flanked by Sahaj and his parents. When Amrita’s name was announced and she walked up to the stage to receive the medal from the Health Minister, time seemed to slow.
I thought of the girl riding a moped through the dark lanes of Wardha. I thought of the intern running a national conference. I thought of the young woman typing a speech in a taxi, unconcerned by my panic. I thought of her long, lonely evenings in Delhi, chasing skills because the system had not offered enough teaching.
And then she stood there, holding the gold medal.
My eyes filled. Not because it was a piece of gold, but because it carried the weight of her journey—every early morning, every small sacrifice, every quiet decision to work harder than necessary. The spotlight was brief. But the work behind it had taken years.
And that, I realized, is how success is really made.
The Canine Coup
In 1994, a dog entered our home not by accident, but by invitation. Until then, dogs belonged to other people’s houses and to the street, not to ours. This first entrant was a white Pomeranian, promptly christened Zombie—a name that made sense to no one outside the family and never needed explaining.
The idea, as with many domestic revolutions, began with Bhavana. She had always had a soft corner for animals, and when she finally voiced a desire for a pet, it found a sympathetic ear in Mr. Ashok Bang at Gopuri. We had known his family for almost four decades. A family friend who already lived with four or five animals, he treated the addition of one more dog as a minor administrative task. He went to Gadchiroli to his younger brother, Dr. Abhay Bang, returned with a two-month-old Pomeranian, and handed Zombie to us as casually as one might offer a potted plant.
***
Zombie lived with us in Vivekananda Colony from 1994 to 2004—long enough to stop being a pet and start becoming family. Ashwini was eight, Amrita five. They grew up with Zombie underfoot, over furniture, and occasionally on their nerves.
He was a classic Pomeranian: small in size, enormous in self-importance. He moved with a feathery bounce, barking at strangers with the ferocity of a wolf trapped in a cotton ball. He demanded attention, sat on laps uninvited, and ruled the house with high-pitched authority. There are photographs somewhere of the three of them together—Ashwini, Amrita, and Zombie—all looking equally convinced of their importance to the household.
Zombie died in 2004, suddenly and without warning, while I was in Berkeley. There were no signs of illness, no prolonged goodbyes—just a heart that decided it had done enough. Bhavana handled the aftermath with quiet efficiency. Bhaskar, the local electrician who helped us with most things mechanical and many things emotional, buried Zombie in the backyard. It was an unceremonious ending for a dog who had lived a thoroughly domestic life.
For the next eight years, we remained dogless. The house adjusted. Silence reclaimed certain corners.
***
In March 2012, Ashwini—then newly married—brought home a black Labrador from Nagpur. Bhavana stepped into the role of his primary caretaker, naming him, feeding him, and managing the rituals of grooming and vaccination with her usual dedication. We named him Zombie again, perhaps to honour the memory, though the personality could not have been more different.

Exploring the green: Zombie on a backyard adventure.
Where the Pomeranian was frantic, the Labrador was philosophical. He had the classic Labrador temperament: a deep chest, a perpetually wagging tail, and eyes that looked at you with soulful, unconditional love. He didn't demand attention; he leaned into it. He was a creature of comfort, happy to sleep at your feet for hours, his presence a warm, heavy anchor in a busy house. He accepted Bhavana’s devotion as his birthright, settling into our household as if he had always belonged there.
***
It was this second Zombie who gave us an episode that refuses to fade.
It happened on Diwali evening in November 2017, around five o’clock. In an hour, we were to perform the Lakshmi puja. The house was in that peculiar Diwali state: flowers being arranged, lamps being tested, people half-dressed, half-devotional. In the middle of this controlled chaos, Zombie began barking. This was alarming. He was not a barker.
The barking led us to the kitchen gallery. When we opened the door, we saw Zombie and an eight-foot cobra across the steel criss-cross fence of our neighbour, Dr. M.V.R. Reddy—almost face to face. The cobra raised its hood, aimed, and struck. Zombie swerved and escaped. Again the hood rose. Again it struck. Again Zombie turned away, missing the bite by inches.
For ten to fifteen minutes—though it felt much longer—we stood helplessly as this unlikely duel continued. By rough count, the cobra struck at least fifty times. Each time, Zombie ducked, twisted, or turned away—not aggressively, but with focused calm.
We shouted. We tried to pull Zombie away. We tried to shoo the cobra out. Nothing worked. Eventually, the cobra tired of the exercise. It lowered its hood, turned with what looked suspiciously like irritation, and slipped into the garden bushes. Zombie remained where he was, victorious without knowing it.
The sarpamitra could not be reached—it was Diwali. By the time help arrived, the cobra had vanished. Zombie survived that Diwali. The puja happened, slightly delayed and noticeably subdued. The lamps were lit with gratitude rather than enthusiasm.
He was a kind, wonderful, and quiet dog who lived with dignity till his last breath. He stayed with us until March 2018, when he died suddenly—once again, presumably of a heart attack. He died young. He was buried in the open space in front of our home, a quiet neighbour even in death.
***
The third arrival came not through adult deliberation but through the steady persistence of a grandchild. He arrived in 2024, bought from the same pet owner in Nagpur who gave us the second Zombie.
Hedo, a Golden Retriever, was named by Diti, who had just begun reading mythology and found the word irresistible. We resisted at first. Diti was given a lecture on shared responsibility—feeding, cleaning, walking, the endless small chores animals impose on humans. She listened patiently, agreed to everything, and wore us down.

Quiet corners and loyal friends: Diti and Hedo sharing a moment.
Hedo is different. If the Pomeranian was a watchman and the Labrador a companion, the Golden Retriever is a pure extrovert. He has a coat like spun gold and a personality to match. He loves everyone—the postman, the milkman, the neighbours, the guests. To Hedo, a stranger is just a friend he hasn't licked yet. He carries things in his mouth—socks, toys, sometimes just a leaf—as if offering gifts to the household gods.
***
Today, Hedo is two years old and no longer "the dog." He is part of the house’s fabric. We take him for his morning and evening walks, feed him, and negotiate with him. Diti plays mother to him. Nivi, the moment she returns from school, seeks him out.
A year ago, when Ashwini and Shaily took the children on a ten-day trip to the Konkan, they took Hedo along. Finding hotels with "Pets Permitted" signs proved difficult, but that inconvenience mattered more to the humans than to Hedo. He enjoyed both the road trip and the holiday. More recently, he accompanied them on a trek near Chandrapur, a two-hour drive from Sevagram, enjoying the forest trails as much as the children did.
***
Several times a day, when I am at my computer, he pads over and positions himself near the table. He then signals—politely but firmly, nudging my elbow with a wet nose—that his back requires stroking.
I oblige. He sits still, absorbs the attention, looks at me with what I choose to interpret as gratitude, and walks away, his business concluded.
It is a small, wordless transaction. But then, so are most lasting relationships.
Joyful Chaos
Diti was born on 14 March 2013, by caesarean section in our own hospital. Something shifted quietly in our lives that day. Until then, our home had the orderly rhythm of two working professionals — early mornings, hospital hours, predictable fatigue, predictable order. One baby ended all of that. The house began tolerating toys. The schedules gave way to giggles. Diti did not slip into our lives. She arrived into them — with restless, unstoppable energy, as if she had been born with a small motor running inside her that nobody had thought to ask about.
The Grandchildren

Diti, thirteen.
Barefoot on the porch steps, lost in a book. The world could wait.

Nivi, ten.
Balancing a basket on her head with complete confidence. Sevagram 2024.

Krit, five.
That grin says he has already eaten half the rotis on the plate.

Samanvi, two.
Discovering red berries on a cold morning. Everything is still new.
✦
In 2016, I discovered long-distance cycling. Diti — then three — fell in love with it the way children fall in love with new worlds: completely, without reservation, and with no interest in going back.
Her father bought her a small bicycle. She was soon weaving through the staff quarters and gardens of Sevagram, ringing her bell with the authority of someone who had always owned the campus. By seven, she had become my riding partner.
During COVID, when schools shut and the world contracted to four walls, cycling became our shared escape. We would pedal to Pavnar — a seven-kilometre stretch that offered everything a cautious adult avoids: steep underpasses, sudden cattle, stray dogs appearing from nowhere like examiners in a viva. Diti tackled all of it with a fearlessness that still amazes me. Twice she cycled twenty kilometres without stopping. On those rides she asked for stories, as if the rhythm of pedalling opened the mind to listening. I told her about my childhood in Wardha, about Gandhi, about the history of the soil we were riding through. Those wind-swept mornings — the road empty, the air clean, the world not yet awake — remain among the happiest of my life.
At ten, Diti picked up a new hobby: football — traditionally a boys' game. She never played with girls her own age, choosing instead to play with boys three years older, who, according to her, were real competition. She was always drawn to sport. By all accounts, she has had two fractures, several wounds, and infinitely scraped and bleeding knees. These were medals to her — signs of pride, not misfortune.
If Diti's legs belonged to wheels and footballs, her mind belonged to books.
She became a voracious reader with no patience for waiting. She began with The Jungle Book, moved to Enid Blyton, and by nine had worked through all seven Harry Potter books. She read at the dining table while her food went cold. She read in the car. When the house became too noisy — which, with Nivi around, was often — she discovered the one place nobody disturbs a child for long: the bathroom. Many chapters were finished there, in undisturbed peace.
I introduced her to Greek mythology, and she was immediately captivated by Odysseus. She could visualise Scylla and Charybdis with startling clarity, and she was genuinely outraged by the cruelty of Greek kings — as if she were reading the news, not a legend two thousand years old. Intrigued by Greek mythology, she moved on to Percy Jackson. Diti doesn't merely read stories. She moves into them and takes up residence.
— ✦ —
Nivi arrived on 18 November 2016, and brought with her a different kind of attention. Where Diti loves books and sport, Nivi grew her passion for flowers and fruits. She tried to emulate her sister — as all younger siblings do — by completing an eight-kilometre cycle ride through Sevagram without complaint. And there she stopped, bored. She comes home from her school bus carrying flowers, twigs, and leaves, and noise. Lots and lots of noise.
She watches trees the way other children watch cartoons. She notices a new leaf, a fallen flower, a change in bird call. Walking near home with her Dadi Bhavana, she would pause at plants and ask questions that suggested she had been thinking about them long before she asked. She went to Anand Niketan, a Marathi-medium school in Sevagram. She struggled at first, as newcomers do. Then she did what Nivi typically does: she adjusted, and mastered the language. By her second year she spoke Marathi as if she had always belonged to this soil.
A year later, she moved to Lloyd's Vidya Niketan — the school where Diti studies, and where her father Ashwini and her bua Amrita also went. The transition from Marathi to English was a torment on her tender heart, and she simply refused to go. It took tremendous patience, persistence, daily ingenuity, and the passage of time to finally help her feel at home. Now she enjoys her forty-five-minute bus rides as much as she loves her fruits and flowers.
She is also our resident food authority. A fruit vendor makes her eyes light up like a festival. She moves from strawberries to mangoes with the devotion of a connoisseur, and — true Sevagram child that she is — she loves baingan ka bharta with equal enthusiasm. No fruit is too seasonal, no vegetable too humble.
Nivi's favourite pastime is Uno — specifically, Uno with Bhavana, whom she outmanoeuvres with a sly intelligence (and no small amount of luck; Bhavana would let her cheat) that is both charming and mildly alarming. She has studied her opponent carefully. The mischievous grin when she plays a wild card tells you she has been planning it for several turns.
During the long, anxious days of the pandemic, their daily Uno sessions became a household ritual — part entertainment, part therapy, part proof that ordinary life was still possible. As the girls grew older, they began sleeping in our room. Their breathing, their clutter, their voices at odd hours — everything that might once have felt like disruption began to feel like warmth. They reminded us, in the middle of busy professional lives, that the most important titles we held were not Doctor or Professor. They were Dada and Dadi.
— ✦ —
Krit was born to Amrita in December 2020, and he arrived differently from his cousins — loudly, cheerfully, and with no interest in being overlooked.
He is rowdy, boisterous, and naughty, yet so utterly charming that you wouldn't have the heart to tell him off — the kind of child who can turn a quiet house into a festival in under five minutes, then bring the house down with his tantrums. He started crèche at one year old at PGI Chandigarh, joining thirty other children, and by the summer of 2021 had already become a character. On a flight with Amrita, he entertained the entire cabin with his antics. The other passengers were, by all accounts, delighted.
When Krit visited us in Sevagram, the house entered a state of cheerful rebellion — studies kicked aside, responsibilities forgotten. Diti — observing him with the sharpness of an elder cousin who has paid close attention — offered what may be the most accurate description of him anyone has managed: "He's funny, smart, determined, naughty, and happy. Like Nivi, he loves food. And like me, he opens any book he can find — even though he can't read yet." Three sentences. Entirely correct.
— ✦ —
The family grew again on 14 March 2024 — which is, by a beautiful coincidence, Diti's birthday. Samanvi was born in Chandigarh. In a detail that felt almost arranged, she was delivered by Dr. Riti Narang — an MGIMS alumna, a Sevagram girl, and the daughter of our own faculty colleagues. The circle, as it sometimes does, closed neatly.
Bhavana reached Chandigarh within hours of the news. The baby, however, was in no hurry to receive a name. For six months she remained nameless while Amrita searched lists, school registers, and the internet with the seriousness of someone making a permanent and irreversible decision — which, of course, she was. Finally, six months later, she became Samanvi.
A true lily. She is quiet, observant, and content. She dotes on her brother, and there could not be two siblings more different, yet so fond of each other.
In December 2024, the story took a transcontinental turn. Amrita, Krit, and Samanvi moved to Richmond, Virginia, to join Sahaj. The first year in a new country is never gentle — viral infections, unfamiliar schools, new systems, and the particular loneliness of being far from a place where a doctor is always one phone call away. Bhavana travelled to Richmond twice over the past year, helping Amrita settle in.
Watching them build a life in America, I felt something I had not quite anticipated: pride and wistfulness in equal measure. The roots that had held us in Sevagram for four decades had, quietly, grown wings. The family that began in a small quarter in Wardha was now spread across two continents — still close, still familiar, just farther away than we had ever imagined they would go.
The Three Departures
For nearly a decade, my elder brother Om lived with myasthenia gravis, an illness that did not announce itself loudly but stayed, patient and persistent, in the background of his life.
In those early years, it seemed manageable. His eyelids would droop, giving him a tired look, but tablets held the disease in check, and he carried on with his routines. He ran his shop, met people, argued about small things, and spoke as freely as he always had. If the illness was present, it remained in the margins.
That changed in 2024.
Tired of taking medicines every day, Om stopped them. What followed was not sudden, but it was relentless. His voice began to fade, first becoming slurred, then hesitant, and eventually falling silent. Swallowing grew difficult, and meals turned into careful, prolonged efforts. Even a sip of water demanded attention. Conversations, once easy and frequent, became brief and then rare. Slowly, almost without our noticing when it began, silence settled around him.
In October 2024, I took him to the Central India Institute of Medical Sciences in Nagpur, an institution founded by Dr. G. M. Taori. Dr. Neeraj Baheti confirmed what we had begun to suspect: the disease had advanced, and the antibody levels were high.
We began treatment with intravenous immunoglobulin, followed by steroids, and later rituximab. A nasogastric tube was inserted when swallowing became unsafe, and it soon became his main source of nutrition.
There were small improvements that we held on to. His eyelids lifted, and the troubling accumulation of saliva in his throat reduced. But his neck muscles remained weak, and his head would fall forward, as if even holding it upright had become too demanding.
For weeks, he travelled between Yavatmal and Sevagram, always accompanied by his wife or his son Raju. We began to live within the rhythm that serious illness imposes—a new treatment, a brief stabilization, a quiet hope, and then a gradual decline that no intervention could fully arrest.
Looking back, those weeks feel both long and brief, as if time had stretched and contracted at the same moment.
The illness did not take only his strength; it altered how he saw himself.
Om had run his shop for decades. It was not just a livelihood but a structure around which his days were organized. Over time, however, the world around him had changed. Online businesses had altered buying habits, and the small shop that had once sustained him no longer fit into that new order. He closed it.
I remember the day the shutters came down. There was no ceremony, no conversation, just a quiet acceptance. Yet something shifted in him after that.
In the months that followed, dependence replaced independence. Where he had once moved through his day with ease, he now required help for the smallest tasks. Tubes and medicines entered his daily life, and the space around him grew quieter. He never spoke of it directly, but one could sense the weight of it—the slow realization that the life he had known was slipping away.
On 26 November 2024, Om died in Sevagram Hospital.
The night before, I sat beside him. He was fully conscious and aware. At one point, he joined his palms in a gentle pranam and looked at me for a long moment. Then, with a slight movement of his hand, he pointed towards the monitors and the intravenous lines.
He did not need to say anything. I understood what he meant.
A little later, he asked for water. He drank it slowly, taking small, deliberate sips, as if aware that this simple act had acquired a finality. After that, he closed his eyes and rested.
By morning, he was gone.
We had already made the decision that there would be no ventilator, no chest compressions, and no attempts to force life back into a body that was no longer able to sustain it. It was a difficult decision, but it allowed him to leave without struggle.
In those last hours, I was not only a physician. I was his younger brother, sitting beside him, aware of what medicine could do—and what it could not.
A year later, on 24 December 2025, my elder brother Ashok died in Pune at the age of eighty-two.
Two days earlier, he had travelled there to spend some time with his younger son Sumit and his daughter Surekha. It was an ordinary decision, the kind that families make without thinking much about it.
On the morning of the 24th, he developed chest pain. His daughter-in-law, Chanchal, called me, and as she described his symptoms, the diagnosis became clear almost immediately. This was a heart attack.
I asked her to give him aspirin and another antiplatelet drug, along with a statin, and to take him at once to Dr. Kalidas Bharati’s hospital in Pimple Saudagar, which was close by. I also called Dr. Bharati myself. In such moments, familiar professional connections become deeply personal.
Ashok reached the hospital in time and received emergency treatment, including a clot-buster. For a short while, he improved, and we allowed ourselves to believe that the worst might have passed.
Within two hours, a second heart attack took him away.
We reached Pune late that night. The next day, as we performed his final rites, the speed of what had happened still felt unreal.
There was grief, but also a quiet understanding that he had not suffered for long. He had not been confined to a bed or lived through a prolonged illness. His departure was sudden, but it spared him the slow decline we had witnessed the year before.
On the morning of 22 March 2026, my sister Pushpa died at home in Indore. She was eighty.
The news came through a phone call from my nephew Aalok.
Her illness had begun in 2018, when she developed ovarian cancer. She went through what such a diagnosis demands—major surgery, cycles of chemotherapy, blood transfusions, and repeated hospital visits. I remember her first call to me when I was at PGI Chandigarh, where I had gone to examine MD students. She spoke of abdominal distension, and even before the tests were done, I felt a quiet unease. The ultrasound confirmed that the disease had spread beyond the ovaries.
All my life, I had called her Jiji.
She faced her illness with a steadiness that did not draw attention to itself. She went through each cycle of chemotherapy without complaint, accepting the discomfort as part of what had to be done. When she called me, it was often for advice, but also for conversation. Over time, I found myself balancing two roles—that of a brother and that of a physician, sometimes offering guidance, and at other times holding back, trying to prevent unnecessary interventions.
Our conversations ranged far beyond her illness. We spoke of the places she had lived—Nagpur, Sirpur-Kagaznagar, Baroda, Gwalior, Indore—and of the years that had shaped our lives. Those calls carried fragments of memory, often unplanned, but always welcome.
A year before her death, she asked me to draft her living will. She was clear in what she wanted—no ICU, no life-sustaining machines, and a wish to remain at home.
When I visited her in Indore a fortnight before she died, I was struck by how frail she had become. Yet her awareness was intact. That evening, we sat together and completed her will. Aalok was present. She signed each page carefully, and when it was done, she seemed lighter, as if something that had weighed on her for months had finally been set aside.
I spoke to Dr. Pankaj Singhai, a palliative care physician in Indore, who, along with his team, ensured that her care could continue at home.
In her final days, she gradually withdrew. She slept more, spoke less, and stopped eating. The day before she died, I saw her on a video call. She opened her eyes briefly and looked at the screen, but she did not have the strength to speak.
I ended the call and sat quietly for a long time.
In the days following her passing, a beautiful story was shared with me that perfectly captures her spirit. Six years ago, she traveled to Lotus Valley with her family. This was just a year after she had faced her grueling battle with cancer, surviving both surgery and chemotherapy. During that visit, a photograph was taken of her that she truly loved. She handed it to her grandson, Sarang, asking him to edit and preserve it for the future.
Just six weeks before she left us, she instructed her family that this was the very picture she wanted displayed when people came to the house to pay their last respects. Because she so dearly loved roses, she requested that her funeral bier be adorned with them, rather than the traditional white jasmine and lavender. She didn't want a somber farewell; she wanted a celebration, complete with a band playing music as her final journey began from our home. She had meticulously orchestrated every minute detail, ensuring her family understood her wishes for the photo, the flowers, and the music. That was my sister, my Jiji—everything in perfect order, beautifully planned exactly as she wished.
In the span of a year, I lost two brothers and a sister, each in a different way.
Om’s illness unfolded slowly, allowing us to witness both his suffering and his endurance. Ashok’s death came suddenly, leaving no time to prepare. Pushpa’s journey moved between these two—prolonged, yet marked by a quiet acceptance.
Their departures were different, but what followed was similar.
The house feels quieter now. Conversations that once seemed ordinary return in fragments. Names, places, and moments surface without warning.
When I think of them, I do not think only of their illness or their final days. I remember Om in his shop, Ashok making plans without fuss, and Jiji speaking of her life across Nagpur, Sirpur-Kagaznagar, Baroda, Gwalior, and Indore.
We were, for many years, three brothers and a sister.
That is how I choose to remember us.

Om, Rajesh, and I — October 2024. Six weeks later, he was gone.
Har ki Doon
In May 1999, Vidarbha was doing what Vidarbha does best—turning into a tandoor. We wanted an escape, and in a burst of optimism that now feels slightly reckless, we decided to do something we had never done before: a Himalayan trek.
Har ki Doon, in the Garhwal region of Uttarkashi, sounded just right—remote, green, and reassuringly far from Wardha’s hot winds. Dr Suhas Jajoo and his family joined us. Our little expedition included Bhavana (37), Ashwini (13), Amrita (10), Ashwini's cousin from Indore, Tushar (14), and me—six people, all novices, powered mainly by enthusiasm and the belief that mountains are always kinder than cities.
***
We began with a tactical error. On the way, we decided to stop in Agra so the children could see the Taj Mahal. It was a noble idea, and a foolish one.
May in Agra is not summer; it is punishment. The Taj, which poets describe as ethereal, was radiating heat like a giant marble tawa. Walking on that white floor felt like stepping onto a griddle. Even the air seemed to shimmer with irritation. To make matters worse, the water was saline and undrinkable. We were thirsty, sunburnt, and slightly dazed, and it dawned on us—slowly, like a late diagnosis—that the Taj is best admired in winter.
That evening we fled Agra and boarded a train to Delhi, desperate for cooler air and kinder temperatures.
We had booked the trek through a Pune-based agency and paid Rs 17,000 for the entire group. It was a package deal that introduced us to Mr Joshi, a gentleman from Pune. The mountains do strange things: they tire you out, make you hungry, and also make friendships stick.
That one did. Even today, Mr Joshi sends Diwali greeting cards to our children every year. It is a small gesture, but it carries the warmth of that journey.
***
From Delhi we took a bus to Dehradun, and then another to Sankri—the starting point of our foot journey. Somewhere along the way, the world began to change. The dust and noise of the plains gave way to pine forests, rushing streams, and that sharp, clean mountain air that feels like it has been filtered through prayer.
We entered the Govind National Park and suddenly everything looked like a calendar—green slopes, tall trees, the occasional glimpse of snow in the distance. Our guide pointed out flora and local details, but we were mostly focused on the basic survival skill of trekking: putting one foot in front of the other without complaining too loudly.
***
We learnt our first Himalayan rule quickly: the weather is a fickle friend.
In the day, the sun was bright and the walking warmed our blood. But the moment the sun dipped behind a peak, the temperature dropped like a curtain. Nights in the guesthouses were bitterly cold. We piled on blankets, wore extra layers, and huddled together like people who had suddenly discovered the value of body heat.
***
The trek was not easy. On the second day, we raced against menacing dark clouds to reach our campsite before the rain hit. The following day we climbed towards Osla village (2,590 metres), a hamlet surrounded by apple orchards and snow-capped peaks. The beauty was almost unfair—so perfect it felt staged. But the altitude was beginning to bite.
As we climbed higher towards Har ki Doon, I began to feel the tell-tale signs of mountain sickness: nausea and breathlessness. I had spent years diagnosing others, but the Himalayas have a way of reminding you that the body doesn’t care about your degrees.
***
To distract ourselves from fatigue and thinning air, we invented a game.
We began composing nonsense rhymes—silly, off-key, and utterly shameless. It started clumsily and then became competitive. The children—Ashwini, Amrita, and Tushar—would shout out a verse, and the adults would chorus back. Our ridiculous anthems echoed through the valley, startling birds, entertaining strangers, and keeping our spirits afloat.
It turned out laughter was the best antidote to exhaustion. It didn’t increase oxygen saturation, but it certainly improved morale.
When we finally reached the Har ki Doon valley—with its glaciers, wide meadows, and pristine stillness—the sense of achievement was overwhelming. We spent a day exploring, meeting other trekkers, and feeling very small against the vast canvas of nature. In that valley, you don’t just admire the mountains. You accept your size.
***
The return journey brought us back to reality with a jolt.
We descended to Sankri, took the bus to Delhi, and walked straight into a heatwave. The capital was boiling at 45°C. Our faces—already red from mountain sun and snow burn—were now scorched by city heat. It felt like being punished twice for the same holiday.
We also ran into an unexpected snag with accommodation. We tried to check into a Jain dharamshala, hoping for a clean, quiet place to rest. The caretakers, on realising we were not Jains, turned us away. It was a small moment, but it stung. Religious boundaries, I realised again, can sometimes trump basic hospitality.
Fortunately, life has a habit of balancing disappointments with kindness. Dr S K Ghosh and his wife—friends and colleagues—rescued us. They welcomed us into their Delhi home with open arms. Their warmth washed away the bitterness of rejection and the fatigue of travel. We arrived as exhausted travellers and were treated like family.
***
We returned to Sevagram sunburnt, peeling, and thoroughly tired—but happy. Har ki Doon remained my only foray into high-altitude trekking. Bhavana and I never went back to the mountains in that way. One trek was enough to satisfy our curiosity and test our knees.
But the bug had bitten the next generation.
Years later, Ashwini and Shaily explored Leh and Ladakh. Shaily went even further—she did the Chadar Trek, walking on the frozen Zanskar River in the dead of winter. When I read her blog describing that sheet of ice and the brutal cold, I smiled. I remembered our own clumsy rhymes, our heavy breathing, and our childlike pride at reaching Har ki Doon.
We had stopped at the meadow.
Our children went on to walk on ice.
The Accidental Pilgrimage
We grew up on the flat, sun-baked plains of Wardha. In a small town, you know your neighbours well. You know how they take their tea, what makes them laugh, the pace of their walk. So when Suhas and Shubhada Jajoo proposed a trip to the Char Dham — the four Himalayan shrines of Gangotri, Yamunotri, Kedarnath and Badrinath — in the summer of 2019, it did not feel like a religious duty. It felt like an old conversation, picked up again.
Five families signed up: Suhas and Shubhada; my wife Bhavana and I; Shrikant Gandhi and his wife Shobha; Sunil Tapdiya and his wife Sunita; and Parmanandji Tapdiya with his wife Shobha. We were old friends, and Suhas and I went back further than the rest — we had studied together at Government Medical College, Nagpur, in the 1970s. He trained in surgery, I in internal medicine. We had learned how to read the human body side by side, as young men.
There was a sixth member of our party, though he came without his family. Chandu Fattepuria had been at school with me at Cradock, long before any of us had thought about medicine. He went on to become an engineer, then left engineering altogether and settled in Indore, where he built a name for himself in the Jain community — for his grasp of Jain customs and rituals, his bhajans, and his gift for leading people. He joined us at Delhi. His wife, Usha, stayed behind; she was not keeping well.
My own journey started with a detour. I had been in Chandigarh, at the Postgraduate Institute of Medical Education and Research, examining MD Medicine candidates. Rather than fly home to Wardha and then travel north again, I arranged to meet the others at Delhi airport.
I remember standing in the terminal, scanning the crowd, until I spotted them coming out after their flight from Nagpur. There is something comforting about finding familiar faces in a busy airport. Ten of us were about to travel through the high ghats, and the original plan — one cramped twelve-seater bus — had already been dropped. Vaibhav, Tapdiyaji's son who lives in Delhi, had insisted on comfort over economy for the mountain roads. He arranged three Toyota Innovas instead.
Shobha Gandhi rode in our Innova all week — she, Shrikant, Bhavana and I made up that car. Shrikant always took the front seat. Bhavana and I had the middle, and we would offer Shobha the middle seat too, since it was roomier. She always laughed and refused, hopping into the back with the ease of a child, and stayed there the whole trip. She turned out to be the group's chatterbox, keeping us entertained with stories, jokes and anecdotes that made the long hours on the road disappear. The Tapdiya family filled the second. In the third sat Suhas, Shubhada, and Chandu Fattepuria — our old school friend from Cradock High, who had swapped an engineering degree for a life in business in Indore.
A travel agent, recommended by Dr Yogesh Saboo, a well-known surgeon from Nagpur, had arranged the logistics. Yogesh was a close friend of Suhas's. His sudden death from a heart attack, at home in May 2026, would later leave a deep ache. But in May 2019, none of us knew that. The road lay open, and we were simply old friends escaping the heat of the plains.

We left Delhi early and reached Rishikesh by two in the afternoon, ready to head north. There we hit a snag. Our drivers discovered that the Char Dham route needed a special permit, and none of the cars had one. The permit office was eighty kilometres back the way we had come. There was nothing to do but turn around. By the time we had covered the hundred and sixty kilometres, back and forth, it was dark. We had to make a two-hour detour and spend the night in a small guest house whose name I no longer remember, before finally picking up the route again the next morning. The journey had begun with a small drama of its own.
I am a doctor. My view of the world is shaped by logic, physiology, and the plain facts of the human body. I have never been a deeply religious man. My parents and sisters liked to tell the story of how, before I turned seven, I wore a dhoti and a tilak, read the Ramayana and the Mahabharata, and performed daily poojas.
Adulthood changed that. Years in the lab and on the ward reshape how you see the world. I still believe in something larger than myself, and I still bow before the divine when life asks for an anchor. But I no longer follow the daily rituals of a Hindu household. When I visit the Laxminarayan temple in Wardha, I go for peace of mind, not obligation. This yatra was not, for me, a search for merit or salvation. It was a holiday — a chance to breathe mountain air with people who knew me well.
My worries were more physical than spiritual. I suffer badly from motion sickness, and the thought of eight hours a day on narrow mountain roads filled me with quiet dread.
Then Bhavana handed me a small white pill. She had packed everything from woollen caps to what amounted to a travelling pharmacy. The pill was Cinnarizine, and it cost barely a rupee.
An hour after I took it, the world stopped spinning. As the Innova climbed higher, taking sharp bends where the road simply ended in air, my stomach stayed calm. Bhavana, too, felt none of her usual travel sickness. That one tablet, taken each day, turned what could have been misery into something close to joy. I remember looking out at the green valleys below, feeling nothing but calm, and silently thanking the chemist who had first made that molecule.
As the roads climbed, age and illness made their presence felt. At my stage of life, with my own history of heart trouble, the thin mountain air pushed hard against me. A short climb left me gasping for breath that was not there. We had no choice but to rely on local coolies and Sherpas — many of them young Nepali men who came to the shrines each season to earn a living — and their sturdy horses and donkeys.
There is something uncomfortable about being carried by another human being. I sat on the horse, felt the coolie's steady footsteps beneath me, and felt a kind of guilt settle in my chest. Here was a young man, half my age, sweat soaking his shirt, carrying my weight up a mountain for a few hundred rupees. It felt unequal — almost feudal — set against the idea of a spiritual journey. I kept my eyes down and said little, caught between medical necessity and a quiet unease.
Shrikant Gandhi, meanwhile, walked the same steep tracks with no stick and no visible strain. He was always a few steps ahead of the rest of us, breathing easily, looking as if the climb cost him nothing.
Shrikant had his own ritual. Whenever he spotted a temple by the roadside, he would ask the driver to stop, step out, and — as if he had been waiting for exactly this moment — produce a small steel thali from his bag. In it he kept everything he needed: rice, flowers, sandalwood paste, red kumkum powder, a few incense sticks, and a small diya. He would perform his pooja right there, unhurried, whatever the hour or the weather. Watching him, I felt the quiet force of real devotion.
Anyone watching him would have guessed his heart was in perfect health. Two years later, doctors found severe blockages in three of his coronary arteries and rushed him into angioplasty. His easy climb up those hills is a lesson doctors should not forget: will, adrenaline and devotion can carry a man further than his arteries would suggest. The body does not always tell the truth in advance.
Our first two stops could not have been more different. Gangotri matched every idea I had of a Himalayan shrine. Among white granite rock and the roaring, icy channels of the young Ganges, we stood at the VIP Ghat and performed the traditional rituals, our hands numb in the freezing water where King Bhagirath is said to have meditated. It felt clean, timeless, and still.
Yamunotri broke that peace. As we neared the shrine, the crowd thickened into chaos. Pilgrims bathed in the hot springs, cooked over open fires, and left rubbish behind them. The air was thick with smoke and the smell of too many people in too small a space. A hundred metres from the inner shrine, I stopped. I could not go further. I turned back, choosing to keep my own idea of the sacred rather than push through the mess in front of me.
The real heart of the trip, though, did not happen inside a temple. It happened because of a snowstorm.
Five days in, as we prepared to head for Kedarnath, a blizzard swept the mountains. Roads vanished under snowdrifts. The helicopters we had tried to book stayed grounded. We were stuck at the base camp in Sitapur, with no way forward and no way back.
We had to drop Kedarnath from the itinerary and plan a straight run to Badrinath once the weather cleared. But those two unplanned days at Sitapur turned out to be the best part of the whole trip.
Trapped together in the cold, the usual roles and worries of daily life fell away. The women gathered in the small kitchen, laughing over pots of upma and poha, cooking meals that tasted of home. We played cards, told old stories from our medical college days, and laughed the way we had not laughed in years. Even Parmanandji Tapdiya — seventy-four years old, famous back home for his strict, no-nonsense discipline — softened. The cold seemed to loosen something in him. He joined the jokes and the laughter, a side of him none of us had seen before.
Sunil and Sunita, it turned out, make this pilgrimage almost every year. The journey is tiring, but their devotion and their will carry them through. Sunita was born Maharashtrian, but her speech, her customs, the rituals she follows — all of it is Marwadi. Meet her and you would never guess she came from a Maharashtrian family and not a Marwari one. Their easy, constant conversation kept the whole group feeling like family.
Shubhada was thrilled through it all. For years she had dreamed of a holiday that combined faith and travel in equal measure, and this trip gave her both. She and Suhas are both busy doctors, and finding time for a trip like this had never been easy. But over the years they had learned the art of carving out time from a demanding practice, and they enjoyed every minute of the journey.
Those two days made up for every bumpy mile and every hour of travel fatigue. The trip taught me something simple: it is rarely the destination that matters. It is who sits beside you in the car.
When the storm passed, we reached Badrinath, set between the peaks of Nar and Narayan. The cold there cut through our woollens. Neelkanth Peak rose behind the temple, a wall of white and grey ice against the sky.
Despite the cold, the place felt clean and calm. We visited Narad Kund, watched steam rise off the hot springs at Tapt Kund, and walked to Mana village — the last Indian settlement before Tibet — where the Saraswati river roars beneath the stone slab of Bhim Pul. Standing there, looking at the mountains, I understood what pilgrims come for. Not a transaction with God, but a reminder of how small we are, and how lucky we were to be alive, well, and together.
For Bhavana, the trip was a welcome break. We had done the Har Ki Dun trek together once before, with Suhas, Shubhada, and our children — but that was long ago, in 1998. She has always loved mountains and snow. Like me, she is not a religious person, but she enjoyed every bit of it: the fun-filled days, the snow-filled nights, the roads, the mountains, everything in between.
From Badrinath, we wound down through the Panch Prayag — Vishnuprayag, Nandprayag, Karnaprayag — where rivers meet the Alaknanda in bursts of white and turquoise. We passed Rishikesh, watched the sadhus near Ram Jhula, and headed back to the heat of Delhi and, finally, home to Wardha.

On the way to the airport, we stopped at Akshardham temple for a few hours before our flight. After Yamunotri, the contrast was sharp — clean, orderly, calm. It felt like a different world from the crowds we had seen in the mountains.
Through it all, Chandu kept us laughing with his poems. He writes and sings well, in clear, simple Hindi, and I found myself impressed by his verses. Years ago, in medical college, I too used to write rhyming poems. Watching Chandu now, I felt the old habit stir again, and a few days after we returned — the memory of the Innova's motion still in my body, the mountain cold still in my mind — I sat down and wrote.
I shared the poem with our Yaatra WhatsApp group:
वो बातें, वो मौसम, नदी का किनारा
वो बर्फीली हवा
वो घाटियां, वो पर्वत का अद्भुत नजारा
वो चंचल इनोवा
वो यमुनोत्री की चढ़ाइयां, वो तंग गलियां
वो घोड़े, वो पालकियां और वो डंडियां
हमको तो राहें ही चलाती थीं, हम खुद बनाते रस्ते
फूलती सांसों के साथ, गिरते-संभलते मस्ती में चलते
वो गर्मी की सुलगती दुपहरी में बर्फीली छांव
हर पल संभालती हमारे डगमगाते पांव
जहां भी जाते, देखतीं हमारी ठिठुरती नजरें
पहाड़ों ने ओढ़ी कैसी ठंडी सफेद चादरें
वो नदी के तट पर श्रद्धा के सुमन
वो पिंडों की थाली, वो गंगाजी को समर्पण
वो कैमरे में कैद मनमोहक मुद्राएं
वो अनोखी अदाएं, पुरुषों की समझ में न आएं
सरसराती हवाओं के संग, वो गीतों का गुंजन
भक्ति से भीगता, हमारा मन; नम होते नयन
वो कचौड़ियां, वो उपमा और वो थेपले
खुलकर खाते हम, जीते हर लम्हे
उन तपती किरणों, उस सुलगती धूप से राहत
वो हेलीकॉप्टर के सपने, वो केदारनाथजी की चाहत
हम जो साथ थे, चलने लगे थे रस्ते
मंजिल से बेहतर लगने लगे थे रस्ते
रखें हम संजोकर इन स्मृतियों को, मन के नीले अम्बर में
उड़ना है हम सभी को, केदारनाथजी इस सितम्बर में
We never reached Kedarnath. But looking back from my desk in Sevagram, I think we found what we needed anyway — old friendships, tested and renewed against the Himalayan cold.
Every so often, Shubhada still reminds us that Kedarnath is due. We laugh, and go back, for a moment, to those days.
दिल ढूँढता है, फिर वही, फ़ुर्सत के रात दिन
— मिर्ज़ा ग़ालिब
Monsoon Century-and-Half
It was a mild, drizzling morning on 31 July 2016 when I decided to do something that sounded heroic at 4:30 a.m. and mildly idiotic by breakfast: cycle from Sevagram to Warora and return. One hundred and fifty kilometres. On a Sunday. For fun.
I had cycled regularly, yes, but long-distance cycling is not an extension of “regular cycling” in the way a longer lecture is an extension of a ward round. It is a different species altogether. It demands not only legs, but patience, planning, hydration, and an ability to tolerate your own thoughts for several hours without asking for mercy.
I was excited, but I was also anxious in that familiar way doctors feel before an unfamiliar procedure—confident enough to start, uncertain enough to worry. The only thing that made the idea seem less reckless was the company. Ashwini was riding with me, and so was Abhishek Raut from Community Medicine—both younger, fitter, and far more relaxed about distances that made my mind do nervous arithmetic.
We set off at 5 a.m., when Sevagram was still half-asleep and the air carried that damp, earthy smell that arrives just before sunrise in the monsoon. The road was quiet, the trees looked freshly washed, and the drizzle made the world feel gentle. For a while, I began to believe that the day had been designed for cyclists.
New Bicycle, New Confidence
A few weeks earlier, I had bought a Marin 7-gear flat-bar bike from Nagpur. It was comfortable, responsive, and—most importantly—kind to a man who had crossed sixty and was no longer interested in suffering for style. The bicycle felt like a small miracle of engineering: it didn’t demand athleticism, only sincerity.
I dressed like a man preparing for battle with his own joints. A blue bandana to stop sweat from entering my eyes, a helmet to protect the one organ I still needed daily, gloves for grip, and a kneecap for reassurance. In my mind, these accessories were not optional; they were negotiations with age.
As we rolled out, the rain stayed with us for half an hour, then stopped abruptly—as if it had merely come to check whether we were serious. The road turned into a ribbon of grey, glistening under the emerging light. It took almost an hour for the sun to appear from behind the clouds, and when it did, it didn’t arrive dramatically. It slipped in quietly, like a shy guest.
Villages, Roads, and the Slow Unfolding of Distance
Our route carried us through a chain of villages—Karanji Bhoge, Karanji Kazi, Madni, Taroda, Mandgaon, Jam, and then Warora. These names, which might mean little on a map, begin to feel personal when you pass through them on a bicycle. You notice small things: women sweeping courtyards, men cycling with sacks of vegetables, children in uniforms walking to school with water bottles swinging from their wrists.
A bicycle makes you see what a car hides. It also makes you respect what a bus driver takes for granted.
We stopped for breakfast at Hotel Ashok in Jam at 7 a.m. It was not a gourmet stop, but it was perfect. A proper breakfast in the middle of a long ride is not about taste; it is about survival. You eat with gratitude, drink with urgency, and treat the chair as if it is a luxury resort.
From Jam to Warora, we rode on the Nagpur–Hyderabad highway. The highway looked impressive and behaved like a bully. Trucks passed too close, as if they were testing our nerve. Some motorcycles came from the wrong side, with the confidence of people who believed traffic rules were for other citizens. Cows wandered into the road with philosophical calm, and stray dogs occasionally barked at us, as if offended by our unusual hobby.
The three of us rode steadily, speaking occasionally, mostly listening to the hum of tyres and the steady rhythm of breath. In the early hours, the body feels cooperative. It hasn’t yet begun to bargain.
When the Ride Stops Being Romantic
Long rides begin as poetry and end as prose. Somewhere after the halfway mark, the romance of the journey fades and the reality asserts itself. The sun grew stronger. The greenery thinned in stretches. The wind began to misbehave, coming from the side with a force that made the bicycle wobble slightly, the way a rude person nudges you in a crowded corridor.
Side winds are not dramatic. They are just annoying enough to wear you down. They demand constant correction—small adjustments of posture, grip, balance. They drain you quietly. You don’t notice the fatigue arriving, but suddenly it is sitting on your shoulders like an unwanted relative.
At times, we began to question our sanity. Why were we doing this on a Sunday? Why weren’t we reading a book at home, or sleeping, or pretending to be “resting”? The question came and went. We kept pedalling because stopping would make the question louder.
We ate the snacks we had carried—homemade food that tasted wonderful not because it was exceptional, but because we were hungry enough to respect it. Hunger improves flavour. So does effort.
The road threw its small hazards at us: broken stones, patches of gravel, sudden potholes, and the constant anxiety of being too close to fast-moving vehicles. The bicycle, meanwhile, remained loyal. It did not complain. It simply rolled forward, waiting for the rider to do his share of the work.
The Puncture That Waited for the Finish Line
By noon, we had covered half the distance and were feeling reasonably confident. That confidence, I later realised, was premature and therefore dangerous. Long-distance cycling punishes arrogance, even the quiet kind.
At some point, I began to feel a drag. It was subtle at first—the bicycle felt heavier, less willing. I told myself it was fatigue. Then the resistance grew unmistakable. My tyre had punctured, and I had not noticed it in time.
We cycled nearly ten kilometres before finding a cycle shop. By the time we stopped, we were only four kilometres from home. That was the cruelest part. The puncture had waited patiently, like a villain with timing, choosing the moment when I could already smell the finish line.
I watched the mechanic work with the calm competence of someone who had done this a thousand times. I, who could manage a medical emergency with reasonable clarity, stood there feeling helpless in front of a piece of rubber. It was humbling, and also slightly comic. The body can be trained, but the mind still expects life to be convenient.
When the tyre was fixed, we rode the last stretch to Sevagram and arrived home at 3 p.m. We had completed the 150 kilometres in a little over nine hours.
Exhaustion, Elation, and the Quiet Aftermath
We were drenched, tanned, drained, and strangely cheerful. The fatigue was real, but it carried a sweetness. We collapsed onto our beds with the satisfaction of people who had voluntarily chosen discomfort and survived it.
For Ashwini and Abhishek, it was a solid ride, perhaps even routine. For me, it felt like a private milestone. I had tested my limits, argued with my doubts, and returned home without being carried in an ambulance. That alone felt like success.
Later that evening, as the soreness settled into my thighs and my shoulders, I realised something important. The ride had not made me younger. It had simply reminded me that ageing does not mean surrender. It means learning new ways to challenge yourself without being foolish.
I went to sleep that night already thinking of the next ride. Not because I had conquered cycling, but because cycling had conquered me.
The Guangzhou Misadventure
In the winter of 2019, Bhavana and I planned a three-week visit to Amrita and Sahaj, who were both pursuing fellowships in Vancouver. Amrita was specialising in abdominal ultrasonography at Vancouver General Hospital. Sahaj was training in liver transplant. It was the sort of trip parents look forward to—time with children, a new city, and the quiet satisfaction of seeing them build lives far from home.
To get there, we took an overnight train to Delhi and then flew with China Southern Airlines. The route had a layover in Guangzhou before the final hop to Vancouver. It sounded straightforward, the kind of itinerary you book and forget.
We had a comfortable six-hour flight to Guangzhou. Dinner arrived on time. We watched a couple of movies. We tried to sleep. Somewhere in the middle of that half-sleep, I called Amrita, Sahaj, and Ashwini to tell them we had reached Guangzhou. I even added, with unnecessary confidence, that at 5:30 a.m. the sun was blazing and the city looked brightly lit.
A few hours later, we were going to understand what that “bright sunny morning at 5:30” really meant.
***
At the airport, we ate parathas we had brought from home—our small act of vegetarian self-respect in an unfamiliar country—and then caught some shut-eye. Our bags were checked in. Boarding passes were in hand. We had several hours to kill.
International airports, in theory, offer many ways to waste time: first-class lounges, designer shops, and restaurants that charge in dollars and taste in disappointment. Guangzhou airport had plenty of everything, except one thing we cared about—vegetarian food that didn’t look suspicious.
So I did what restless travellers do. I decided to explore the entire Terminal 2. Eventually we settled near Gate 142, where the seats were slightly more comfortable and the corner felt quieter. Our plan was simple: stroll to the gate two hours before boarding and behave like experienced flyers.
It was a plan built on one fragile assumption—that we knew the time.

Bhavana at Guangzhou airport — twenty-four hours, no ticket, no Mandarin, and nowhere to go. Vancouver was still a continent away.
***
Guangzhou airport, to my astonishment, had no visible clocks. I went to the enquiry counter to ask for the local time. The girl at the counter didn’t have a watch. It was such a perfect moment that I almost laughed, except the joke was on me.
The airport had free Wi-Fi, but Google was blocked. My Garmin watch, normally a reliable companion, didn’t show local time. We were stranded in the most modern of places with the most basic information missing.
So we waited—calmly, foolishly—about 400 metres away from our gate, unaware that time was quietly running away from us.
After a while, we checked our watches. It was 11 a.m. Our flight was scheduled for 1:20 p.m. Boarding would begin around 12:50. Plenty of time, we told ourselves. We walked leisurely towards Gate 150, still feeling like responsible adults.
***
Then my phone rang. It was Ashwini.
He asked where we were.
I reassured him that we were fine and ready to board. Then, almost casually, I asked if he could check the local time in Guangzhou for us, because the airport had no clocks.
There was a pause.
“It’s 1:43 p.m. in Guangzhou,” he said.
It hit me like a slap. We had missed the flight. Not by hours. By minutes. By a cat’s whisker.
As we reached the gate, the emptiness confirmed it. The display board showed our flight was “closed.” Bhavana looked at my face and read it instantly—the disbelief, the fear, the sudden shame of having done something so avoidable.
Only then did the obvious truth land: I had forgotten to factor in the time difference between Delhi and Guangzhou. The departure time on the boarding pass was local time. The sun at 5:30 a.m. had not been poetic. It had been mathematical.
***
“How could I have made such a foolish mistake?” I kept asking myself. I had prepared thoroughly before leaving India. I had checked passports, tickets, medicines, everything. And yet we had missed the flight because we didn’t know what time it was.
Mistakes happen, of course. Even experienced drivers forget to fill petrol. Even regular commuters miss trains. Even frequent flyers can miss flights.
But some mistakes are expensive.
We rushed to the transfer counter. The clerk stamped our ticket with two brutal words: “Didn’t board.” Then she directed us to the China Southern Airlines counter.
The attendant there was a young, slim Chinese woman with spectacles and good English. She listened carefully and then said, politely:
“The next flight is 24 hours away. Seats are available. The tickets will cost 1300 dollars.”
“For both of us?” I asked, still trying to be optimistic.
“No. For each.”
“Canadian dollars?” I asked, bargaining with geography.
“No. US dollars,” she said, now slightly firmer. “On-the-day tickets booked at the airport can be expensive.”
She sounded sympathetic, but sympathy doesn’t pay bills.
We did the mental arithmetic. Our error would cost us nearly two lakh rupees. And we were only at the start of the itinerary. Buying a one-way ticket could also disrupt the entire booking and risk cancellation of the return journey. We were trapped in the fine print.
***
As we stood there, we realised we had hit a wall—three walls, actually.
First, the next flight was 24 hours away.
Second, the airline required a Chinese credit card to purchase tickets. International cards were not accepted.
Third, we did not have a Chinese visa, which meant we could not simply walk out and check into a hotel in the city. We were stranded inside the airport like passengers in a polite prison.
It is difficult to remain calm in such situations. But panic is useless. It only adds noise to an already complicated problem.
***
This is where the modern family system kicked in—children, phones, emails, and mild desperation.
Sahaj was constantly on the phone with Expedia and the airline ground desk, trying to keep me calm while negotiating with two systems that both insisted the other was responsible. “A couple of hundred dollars will hurt,” he said, “but losing the whole ticket will hurt more.”
Amrita began writing emails to China Southern, stating that her parents were stranded at the airport and needed help. She called us repeatedly, soothing our frayed nerves with the calm authority that daughters develop once they begin parenting their parents.
Ashwini composed a few tweets to the ministry, doing what young people do instinctively—create public pressure with minimal words.
And I did what I could do best: plead, explain, and appeal to human kindness.
After an hour, I wrote a letter—old-fashioned, earnest—explaining who we were, where we came from, how we missed the flight, and why we could not afford new tickets. The counterwoman read it carefully and showed it to her colleague.
We waited in the empty airport, watching time move in slow motion. Nothing seemed to happen. Half an hour passed. Another. It felt endless.
***
Then Bhavana nudged me.
A China Southern Airlines employee was walking towards us with a piece of paper in her hand.
She asked for our old boarding passes. She took them politely. Then she handed us new boarding passes for the next day’s flight—without any additional charges.
“Please note the date and time,” she said, and then added, with a gentle chide, “And this time, don’t miss your flight.”
For a moment, I couldn’t speak. It felt like an angel had descended into Terminal 2, armed not with wings but with a printer.
I thanked her profusely, folded my hands, and said “Namaste.” She smiled and did Namaste back. In that brief exchange, two cultures met at the level that matters most: decency.
“What about our checked-in luggage?” I asked, now worried about the next disaster.
“It will travel with you,” the counterwoman reassured us. “You will collect it in Vancouver.”
Then she asked, thoughtfully, “Would you like me to arrange a transit visa for you?”
We declined. We preferred to stay in the waiting hall. After what had happened, we didn’t want adventure. We wanted stillness.
***
The next day, we reached the gate absurdly early—Gate 173, a good 800 metres away—determined not to repeat history. At 1:20 p.m., we finally boarded the Guangzhou–Vancouver flight, the longest we had ever taken: eleven and a half hours.
We ate the vegetarian meals—rice, vegetables, tofu, curd—and walked around the plane every two hours, mindful of the risk of clots in cramped seating. We watched movies to pass time: Life of Pi and Finding Nemo, both oddly appropriate for travellers who had recently been lost.
At 11 a.m., we landed in Vancouver. Immigration was routine. Our luggage had already arrived. And then, a few metres later, there was Amrita—waiting arms, familiar smile, the kind of welcome that makes airports feel like home.
We took a short taxi ride to their apartment at 1366 West 13th Avenue. Sahaj opened doors and elevators with digital keys—one of those modern conveniences that still feels like magic to people of my generation. From the tenth floor, the view was spectacular: mountains, sky, walking paths, manicured hedges, and maple trees in their winter beauty.
We showered, ate our first meal in Vancouver, and finally exhaled.
***
A few days later, I searched the internet for “missed flight” and discovered a little-known policy called the two-hour rule, also known as the flat-tire rule. It isn’t advertised loudly, but it exists in some airlines: if you arrive within two hours of a missed flight, staff may put you on the next available flight on standby, sometimes at no extra cost. If the last flight has already departed, you may be put on the first flight the next day.
Perhaps that rule saved us. Or perhaps it was simply the kindness of a woman at a counter who decided that two confused parents did not deserve a two-lakh-rupee punishment for a time-zone mistake.
Either way, Guangzhou taught me something I should have known long ago: travel, like life, rewards calmness. It punishes arrogance. And when things go wrong, it helps to breathe, ask for help, and trust that you will eventually reach where you are meant to be—just a day later, and a little wiser.
The Brevet That Broke My Confidence

I first came across the word brevet in November 2015. At the time, I didn’t even know how to pronounce it correctly. It sounded like something you eat in a French café and regret later, preferably with a glass of water and a long apology to your stomach.
But within a year, the word had entered our household vocabulary. Ashwini had completed 200- and 300-kilometre brevets in Nagpur and earned the title of Randonneur. That is how I learnt what a brevet truly is: a long-distance cycling event, non-competitive in spirit, but strict in discipline. You must finish within a time limit. You must stamp your brevet card at control points. You must keep going through fatigue and weather without external support. It isn’t a race, but it certainly isn’t a picnic either.
In early August 2016, Ashwini persuaded Abhishek Raut and me to attempt a 200-km brevet organised by Nagpur Randonneurs. I had done a few 50-km rides and my 150-km Sevagram–Warora loop, which had made me feel briefly invincible. A brevet, however, carried the weight of rules, timing, and the quiet fear of public failure. In a village like Sevagram, where everyone knows everyone, failure doesn’t remain private for long.
Ashwini, acting like a strict coach, told me not to hide behind age or the stent in my heart. “Believe in yourself,” he said. “Your enthusiasm will cover the rest.” I didn’t tell him that enthusiasm is not a substitute for skill, but I nodded anyway, because that is what fathers do when sons speak with the confidence of youth.
***
Because we lived in Sevagram—seventy-five kilometres from Nagpur—and the brevet started early, we booked a small hotel near the airport the night before. The housekeeper looked startled when she saw three bicycles and cycling gear in the room. It must have felt like hosting a travelling circus, minus the elephants and the dignity.
We ate, slept early, and woke at 3:10 a.m.—the kind of time at which even the alarm clock seems embarrassed to ring. We showered quickly, pulled on our jerseys and cycling shorts, ate a couple of bananas, and carried our bicycles down four floors using the staircase. That itself felt like a warm-up event, and not the kind I had planned for.
At 4:40 a.m., we mounted our bikes and cycled towards Futala Lake, the starting point. Bhavana called from her parents’ home to wish us luck. Her voice was calm and steady, as if she was sending someone to a conference. Mine was pretending to be calm, as if I was not quietly wondering what I had signed up for.
***
We reached Futala about ten minutes late. The place was buzzing with cheerful cyclists—some charismatic, some intimidatingly fit, some looking as if they had been born with gears in their legs. We filled forms, signed waivers, got our bikes checked, stamped our cards, and fixed rider numbers to our handlebars.
The route was simple: Nagpur to Jamb on NH44, a detour to Sevagram, and then back to Nagpur on the same road. Two hundred kilometres in thirteen-and-a-half hours. On paper, it sounded manageable. In the body, it sounded like an experiment.
We were flagged off at 5:15 a.m., and the early energy carried us like a wave. In the first hour, everything feels possible. The mind becomes wildly optimistic. The body behaves as if it is younger than it is, as if it has been waiting all its life for exactly this kind of trouble.
***
I found a rhythm quickly. Even my forgotten cycling shoes did not stop me—I rode the first sixty kilometres in leather shoes. Not ideal, but my legs were cooperative, and I felt absurdly pleased with myself, like a man who has solved a problem by accident and now wants credit for it.
We reached Jamb in just over three hours. We checked in, got our cards stamped, ate bananas, filled our water bottles, and sat down for a few minutes, feeling like seasoned cyclists. The next segment from Jamb to Sevagram was familiar territory. I knew that road like the creases of my palm and could predict the bumps and potholes without looking.
I expected it to be easy. It wasn’t.
***
As we turned off the highway towards Sevagram, a fierce headwind hit us. It was relentless, cruel, and demoralising. A headwind is the kind of enemy you cannot see but cannot ignore. It drains energy, slows speed, and makes you question your life choices, including the ones you made decades ago.
We crawled past villages, inching forward. My breathing grew heavier. The early endorphins faded. The legs began to complain in a language they speak fluently. Still, we reached Sevagram at 10:45 a.m.—a hundred kilometres done in under six hours. It felt like a small victory, though I didn’t realise it was also the calm before the mess.
***

The Sevagram checkpoint was barely two hundred metres from my home. Friends welcomed us with roses. Vaibhav Patni was there. Shaily and little Diti had come too, eyes bright with curiosity. Diti looked at the helmets, jerseys, and bandanas as if we were characters from a colourful cartoon who had wandered out of her storybook.
I sat on a concrete bench, ate hot khichdi, drank water like a fish, chatted happily, and felt a second wind. What I did not feel was urgency. I stayed too long—almost forty-five minutes—because it felt harmless, and because home has a way of making you forget that you are still in the middle of a task.
Experienced riders warn you: don’t waste time at control points. Sevagram is not the destination. It is a stamp and a goodbye. I learnt this too late, the way most people learn important lessons—by paying for them.
***
Barely five kilometres after leaving Sevagram, my rear tyre went flat. I had watched dozens of YouTube videos on fixing punctures. I had even tried practising at home, with disappointing results. But I had never fixed a puncture on the roadside, in the middle of a brevet, with time bleeding away.
Ashwini returned, flipped my bicycle, removed the tube, replaced it with a new one. Then we discovered the mini-pump was not working. Mihir Hardikar stopped to help, only to find that his tyre had also gone flat. Two punctures in one scene felt personal, as if the road had decided to teach us humility.
A motorcyclist offered to take me to the next village to find a repair shop. We tried one. It was closed. We went to Madni and finally found help. Half a dozen villagers gathered around my bicycle, curious and enthusiastic. They admitted they had never fixed such a tyre before, but they experimented with the seriousness of surgeons. When I offered a tip, they refused. “It is our moral duty to help a doctor,” they said.
The doctor, meanwhile, had no idea how to help himself.
***
When I returned to the puncture spot, Ashwini looked exhausted. “Let’s go,” I said. “I’m quitting,” he replied. I was stunned. I tried to persuade him, but he was firm. He knew what was in store, and he respected his limit.
So I continued alone. The loneliness of a long ride is not dramatic. It is quiet. It is you, the road, and the ticking clock. My phone battery died. I did not have a watch. The bike computer refused to show time. I calculated progress using milestones like a man doing arithmetic in an exam hall, trying to convince himself that numbers could still save him.
Rain began near Taroda. I welcomed it. It cooled my skin and distracted my mind. Locals stopped me, asked my age, asked why I was doing this, asked if there was prize money. When I said there was none, they looked at me as if I had confessed to madness. Their expressions said what my family had been saying politely for days.
***
At 145 kilometres, I met Abhishek again, struggling with knee pain. We rode together for a while, trying to pull each other forward. Then my rear tyre hissed again. That soft sibilant sound is enough to break a cyclist’s spirit.
We found a truck-tyre mechanic. He refused at first. “I don’t repair cycle tyres,” he said sternly. We pleaded. He relented grudgingly. The tyre lived again, but time had died. At 3:40 p.m., we realised we could not reach the Butibori checkpoint before the deadline. We stopped chasing it. We reached late and accepted the verdict: DNF—Did Not Finish.
It stung, but it did not crush me. I was too tired to be dramatic, and perhaps that was a blessing.
***
On the drive back, I refused to wallow. Those twelve hours had taught me something that comfort never teaches: endurance is not only physical. It is emotional. It is the ability to continue when the mind is looking for excuses and the body is offering complaints.
I remembered Stevenson’s line: “To travel hopefully is a better thing than to arrive.” It sounded less like poetry and more like a cycling manual. Back home, I showered, changed into dry clothes, told Diti a simplified version of the day, and ate dinner with the family. I had earned the meal, even with a DNF.
If It’s Not on Strava, It Didn’t Happen
After my first 200-kilometre brevet ended with a blunt “DNF”, I behaved like most people do after a public stumble. I told myself I didn’t care. I announced, with a face of forced maturity, that the experience itself was enough, and even quoted Robert Louis Stevenson to anyone who looked remotely sympathetic. The truth was simpler and less noble: I was irritated, not at the punctures or the headwind, but at myself. The brevet had exposed me. It had shown me that enthusiasm, by itself, is a charming but unreliable friend. It cheers loudly at the start and disappears the moment the tyre hisses.
So, after a few days of sulking in private, I did what I often advise my students to do after an unexpected result: I went back to the basics. I trained. I rode fifty-kilometre loops around Sevagram. I rode with Ashwini and a few medical students who were young enough to treat fatigue as a temporary inconvenience. I learnt to eat before I felt hungry and drink before I felt thirsty—an old cycling rule that sounds obvious until you forget it at the wrong time. When Nagpur Randonneurs announced an all-night 200-kilometre brevet in early September 2016, my family looked worried and I looked secretly excited. Night riding on a national highway with blinding headlights and unpredictable traffic sounded like the sort of plan that only cyclists, and slightly reckless men in their sixties, would consider reasonable. I decided I qualified.
***
The announcement was met with predictable resistance at home. Bhavana and Ashwini tried to apply brakes gently, the way you slow down a car without making the passenger jerk forward. “Why don’t you do a daytime brevet?” they suggested. “Wait for November. Make haste slowly.” They were not wrong. I wasn’t supremely confident either, and I carried my own private anxieties, which I didn’t say aloud because saying them aloud would give them weight. What if I got sleepy on the road? What if a truck brushed past me? What if I got another puncture in the dark and stood helpless, watching time leak away?
I argued like a man trying to convince himself more than anyone else. I promised I would ride cautiously. I promised I would stop if I felt unsafe. I promised I would not chase speed. In the end, they gave in—not because they were convinced, but because they could see how badly I wanted to try again. The registration was closing in a couple of hours, and I signed up quickly, before my courage could change its mind.
***
This time, I was not alone. A small Sevagram contingent joined the brevet: Dr Nikita Bhugra, a resident in Anaesthesiology, and two MGIMS students, Sumedh Manikpure and Alfred D’Souza. We had done a few practice rides together, the kind where you talk too much at the start and become silent by the last ten kilometres. On Sunday evening, we loaded our cycles into a car and drove from Sevagram to Nagpur, carrying not just bicycles but our nervousness as well.
The starting point was Zero Mile, a place that carries symbolic weight even when you are too anxious to appreciate symbolism. The volunteers were efficient and kind. They checked our bikes, handed us rider numbers, made us sign the liability waiver, and gave us brevet cards that looked deceptively innocent for something that could ruin your sleep and self-esteem in one night. At five o’clock, Aditi Hardikar flagged us off, and twenty-two cyclists rolled into the evening, each carrying a private mix of excitement and dread.
***
Barely a few hundred metres from the start, at Variety Square, we ran into heavy traffic. Vehicles were packed bumper-to-bumper at a red light, and I had to thread my bicycle through the chaos like a man trying to pass a catheter in a poorly lit ward. I am not naturally skilled at negotiating aggressive traffic. I ride with caution, which is another way of saying I ride with fear disguised as wisdom. But once we hit National Highway 6, the space opened up. The road was broad, the tarmac smooth, and the city’s noise slowly faded behind us. It was not poetic. It was practical. For cycling, practicality is a blessing.
***
About thirty minutes into the ride, I suddenly remembered something important, something modern, something ridiculous: I had forgotten to start Strava. To non-cyclists, this may sound like a minor error. To cyclists, it is an existential crisis. If the ride isn’t recorded, did it really happen? Will the world believe you? Will you believe yourself?
I stopped abruptly, pulled out my phone from the rear pocket of my jersey, opened the app with trembling fingers, and pressed “Record.” The GPS began tracking my movement, and I felt a strange relief—as if the road had finally agreed to witness my effort. We resumed the ride, and I promised myself that if I finished the brevet, I would never again begin a long ride without checking the basics: lights, bottles, bananas, and the blessed “Start” button.
***
At the 38-kilometre mark, Sumedh had a flat. We all stopped and tried to fix it, but our collective competence was still at the “watching YouTube” stage. Fortunately, a support vehicle happened to pass nearby. Wilfred accompanied Sumedh to a puncture shop, and the wheel returned to life without too much delay. The incident served as a reminder that brevets do not begin gently. They test you early, to see whether you are serious or merely enthusiastic.
We stuck to our plan—an average of 20 kilometres per hour. It was not glamorous, but it was sustainable. At the checkpoints, volunteers welcomed us with bananas, khichdi, water, and encouragement that felt strangely personal for people who had just met us. Each stamp on the brevet card felt like a small assurance that we were still in the game.
***
Five kilometres before Talegaon, we hit a long downhill stretch. The bicycle began to glide, and the wind rushed through my helmet, wiping sweat off my cheeks as if it was doing me a favour. Speed is intoxicating, especially when you have been pedalling patiently for hours. The temptation is to let go and fly, to believe for a moment that gravity is your friend and you are younger than your birth certificate claims.
We resisted. We kept control. It was one of those small adult decisions that you feel proud of later, when you are not lying in a ditch. When we reached Talegaon checkpoint, the first hundred kilometres were done. We felt elated. The body was still cooperative, the mind was still optimistic, and the grass looked very inviting.
***
There was a small garden nearby. The idea of lying down for five minutes felt irresistible. It felt harmless. It felt deserved. But I had already learnt what “harmless” means in a brevet. It means you will lose time and pay for it later. We sat briefly, stamped our cards, ate, drank, and left before comfort could turn into a trap. I knew that if I lay down, even for a few minutes, the body would start negotiating. It would say, politely at first, and then firmly, that it had done enough.
***
Soon after Talegaon, a long climb awaited us. I had studied it in advance—the length, the gradient, the likely time it would take. That knowledge helped, because climbing a hill is half legs and half psychology. I dropped gears. I stayed light on the pedals. I focused on cadence, not speed. I tried to keep my thoughts clean and simple, because when the breath becomes loud and the heart begins pounding, the mind starts bargaining like a lawyer.
Slow down, it whispers. Stop, it suggests. Walk, it offers. Who asked you to do this, it asks, as if you were an innocent man dragged into the affair.
I countered with quieter thoughts—clouds, birds, stars—anything that kept panic away. Slowly, the top arrived. Relief came not because the hill was conquered, but because doubt had been silenced. The road flattened out, and the body behaved again.
***
Alfred and Sumedh moved ahead. Nikita was a few kilometres behind. I found myself riding alone for a long stretch. It was past midnight. The highway was darker, the traffic thinner, and the world felt strangely private. I had never spent two hours on a saddle, alone, on a national highway at that hour. To my surprise, I did not feel afraid. I felt free.
There is something liberating about moving through darkness with only your headlamp, the moon, and the hum of tyres on tarmac. You stop performing for others. You stop thinking of how you look. You become only a body in motion, negotiating distance. At some point, I began talking to myself, quietly and foolishly, the way people do when they are alone and tired and slightly proud of being brave. I discovered that solitude, when chosen, can feel like a gift.
***
The third checkpoint was Kathiawad Dhaba, about sixty kilometres from Nagpur. I reached it with a sense of gratitude that felt almost devotional. I sprinkled cold water on my face, drank coffee, ate bananas, chatted briefly, and sat down longer than I should have. Thirty minutes in a brevet is a small crime, but this time I could afford it. I had time in hand, and I allowed myself the luxury of believing that I would finish. The coffee gave my mind a jolt, and the chatter with volunteers reminded me that even in a solitary sport, you are rarely entirely alone.
***
At two in the morning, with sixty kilometres to go, I rode more leisurely. The road was dim, the breeze kind, and the fatigue oddly manageable. As I neared Nagpur, the streets looked wet, suggesting recent rain. The air was cool. The city felt gentler than it does in daylight. I crossed familiar squares, turned at Variety Square, and found myself on Wardha Road. The finish was close enough to taste, and that was when I decided to stop being philosophical and start pedalling properly.
I pushed harder, not like a sprinter, but like a man who can smell the end and doesn’t want it to slip away. A few minutes later, I reached the final checkpoint near Nagpur airport. The volunteers cheered. They stamped my card. They smiled as if they had been expecting me. The title arrived quietly, without fanfare, the way real achievements often do.
I was a randonneur.
***
Later, people asked me how it felt. I could have said it felt triumphant. I could have said it felt heroic. But the truth is, it felt strangely ordinary. I was tired. I was hungry. I was sweaty. My legs were sore. Yet inside, something had shifted. I had crossed a line I had drawn for myself. I had learnt that a DNF is not a full stop. It is a comma. If you are stubborn enough, you can continue the sentence, and write the next paragraph on the road.
Crosswinds and Confidence

On 14 November 2016, I hit a double century again—200 kilometres on a bicycle in a single day. Even as I write that sentence, it sounds slightly theatrical, as if I am borrowing someone else’s life. But it happened, and I remember the day not as a grand triumph but as a long, honest negotiation between my legs and the wind.
This success mattered more than the number suggests because it came after a phase where cycling had already taught me its favourite lesson: it does not reward confidence alone. It rewards preparation, patience, and the ability to keep moving when the mind begins to invent excuses.
By then, I had tasted both sides of the sport. I had experienced the high of finishing, and I had also swallowed the bitter tablet of a DNF. The earlier failure had left a mark—not a wound, but a memory. It made me less dramatic, more alert, and slightly less eager to behave like a hero at the start of a ride.
***
The route that day took us from Nagpur towards a little beyond Pandhurna and back. The national highway was buttery smooth, the kind of surface that tempts you into optimism. It makes you think you can ride forever, and that perhaps the body has no expiry date.
But the weather had its own plans. Crosswinds arrived early, strong enough to sap energy and test the mettle of even confident riders. A crosswind is not like a headwind that blocks you openly. A crosswind is sly. It pushes you sideways, disturbs your balance, forces you to grip harder, and drains you slowly without announcing itself.
There is a particular fatigue that comes from constantly correcting your line. Your legs may still be pedalling, but your mind is doing extra work, staying alert, refusing to relax. It is like walking through a crowded OPD corridor while carrying a tray of glass bottles—your pace slows, your shoulders tighten, and you begin to feel older than you are.
Still, the road helped. The surface was kind, the gradients were manageable, and the wide highway gave us space. Experience also helped. I was no longer the wide-eyed novice who believed enthusiasm could substitute for strategy. I had learnt, through small humiliations, that long rides are won by small decisions—when to eat, when to drink, when to slow down, when to stop pretending you are fine.
***
A brevet is described as non-competitive, and that is true. Nobody hands you a medal at the end or announces your name on a loudspeaker. Yet, there is a quiet intensity in the air. The clock is always present, even when you don’t look at it. The body keeps doing calculations: how far, how fast, how long, how much left.
The difference between a brevet and a casual long ride is discipline. You can’t drift. You can’t waste time at stops. You can’t turn it into a sightseeing tour just because the sky looks pretty. A brevet may not be a race, but it certainly does not tolerate laziness.
That day, I rode with like-minded friends, and that made all the difference. Cycling alone can be meditative, but cycling with a group adds something else—shared rhythm, quiet companionship, and the subtle pressure of not wanting to be the first person to complain.
When the wind grew stubborn, I found myself watching the others. Not in envy, but in reassurance. If they could keep their line steady, so could I. If they could pedal through the gusts without swearing loudly, I could at least swear silently.
***
By November, my body had begun to understand the demands of distance. The early rides had been full of surprises—sudden cramps, unexpected fatigue, mysterious aches in places I didn’t know could ache. But now, my legs had developed a kind of memory. They still protested, but less dramatically. They had learnt that I was serious.
I had also learnt the unglamorous habits that long rides demand. Eat before you are hungry. Drink before you are thirsty. Don’t wait for the body to send you polite signals, because by the time it does, it is already angry.
I kept nibbling through the ride, refilling bottles, stretching briefly at stops, and reminding myself that the goal was not speed. The goal was completion. At sixty, ambition has to be redesigned. It cannot be about proving anything to others. It has to be about proving something to yourself—and doing it without injury.
***
Somewhere along the highway, as the wind kept pushing and the kilometres kept falling behind us, I realised what was truly carrying me forward. It wasn’t just fitness. It wasn’t even the bicycle.
It was the simple fact of being surrounded by people who understood this strange hobby. People who didn’t ask, “Why are you doing this?” People who didn’t look at a 200-km ride as either madness or midlife crisis. They treated it as normal, which made me feel normal too.
In a small place like Sevagram, it is easy to feel that your life is made entirely of duty—wards, teaching, administration, decisions, responsibilities. Cycling gave me a parallel identity, one that had nothing to do with prescriptions or meetings. On the highway, I was not a professor. I was just a rider trying to reach the next checkpoint without losing my mind.
And the friendships that formed around cycling were unusually pure. There was no hierarchy on a bicycle. There were only legs, effort, and the shared struggle against weather and fatigue. On bad days, someone rode beside you. On good days, you returned the favour. It was simple, and therefore rare.
***
I completed the ride in about ten hours. When I reached home, tired and sun-touched, I felt that quiet, deep satisfaction that comes only after effort. Not the loud satisfaction of achievement, but the calmer one—of endurance, of staying with a plan, of not giving up when discomfort tries to negotiate.
The crosswinds had almost taken the winds out of my sails, but they also gave the ride its meaning. A smooth highway alone does not make a memorable day. A challenge does. That day, the challenge arrived in invisible gusts, and I met it without drama.
Later, sitting at home with sore legs and a content mind, I found myself doing what cyclists always do after a long ride: planning the next one. Two double centuries were now behind me, and the idea of a 300-km brevet began to hover at the edge of my thoughts—half temptation, half threat.
I did not decide immediately. Wisdom, I have learnt, is sometimes just fatigue speaking.
But I knew one thing clearly. With every long ride, I was not becoming faster. I was becoming steadier. And at my age, that felt like the better victory.
Three Hundred, One Shadow
After finishing my first 200-kilometre brevet, I should have been satisfied. Any sensible man would have framed the brevet card, eaten a celebratory jalebi, and returned to a life of shorter rides and longer breakfasts. But cycling has a peculiar way of altering the mind. It makes you forget discomfort quickly and remember only the glow that comes afterwards. It also introduces you to a dangerous thought: if I did that, perhaps I can do this.
That is how the idea of a 300-kilometre brevet crept into my head.
It was not a heroic plan. It was, if I am honest, a slightly impulsive one. The number looked impressive, and the route sounded manageable in conversation. The event was scheduled for 31 December 2016—an odd day for such an adventure. While the world prepared for parties and countdowns, I was preparing for the kind of celebration that involves electrolyte packets, bananas, and the steady humiliation of your own muscles.
The route ran from Nagpur to Deori in Gondia district and back, along Asian Highway 46. The time limit was eighteen hours. Eighteen hours is a long time to sit on a bicycle, long enough to discover which parts of your body are truly loyal to you and which ones are waiting for an excuse to rebel.
Fortunately, I had Abhishek Raut with me.
If long-distance cycling has taught me anything, it is that companionship matters, but not in the dramatic, Bollywood way. It matters in the small ways: a rider who stays close when you begin to slow, who notices your silence, who offers a banana at the right moment without making it sound like charity. Abhishek did not ride ahead to prove a point. He did not hang back like a babysitter. He simply stayed within reach—sometimes in front, sometimes behind—like a shadow that adjusts itself quietly to the changing light.
***
We began before dawn. The early morning cold had that sharp, clean quality that makes you feel awake even before your brain has agreed to participate. The city was still asleep, and the highway looked unusually polite, as if it had decided to behave for a few hours.
The first stretch of any long ride is always deceptive. The legs feel eager. The mind is cheerful. You begin to believe that perhaps the warnings about fatigue are exaggerated, perhaps people are simply weak, and perhaps you are—miraculously—an exception.
That optimism lasts until the body begins to do arithmetic.
At some point, the kilometres stop feeling like scenery and start feeling like currency. You begin to calculate time, speed, distance, and remaining energy the way a householder calculates expenses at the end of the month. If you waste too much early, you will pay later. If you under-eat, you will crash. If you under-drink, you will suffer. If you get too confident, the road will correct you.
I had no desire to be corrected again.
***
By this time, I had begun to respect the most unromantic rule of long-distance cycling: eat before you are hungry, and drink before you are thirsty. It sounds like something a grandmother would say, and yet it is the difference between finishing and collapsing into a melodrama at the roadside.
So I did what experienced riders do. I ate steadily. I drank regularly. I did not wait for hunger to announce itself. Hunger is an unreliable messenger; by the time it arrives, you are already in trouble.
I also learnt that a long ride is not won by heroic bursts of speed. It is won by avoiding mistakes. Cycling, at this distance, becomes less about strength and more about discipline. You do not chase excitement. You chase consistency.
***
Asian Highway 46 offered a mix of rolling roads and long, steady stretches. There were moments when the landscape felt repetitive, and yet repetition has its own comfort. The body likes predictability. It settles into rhythm. It stops protesting and begins cooperating, as if it has accepted that this is the day’s work and there is no escape.
The ride offered small sensory gifts that I had not expected to enjoy so much. The cold breeze in the early morning was bracing, almost medicinal. By afternoon, the winter sun became pleasantly warm, not harsh. The light changed slowly, turning the highway into a ribbon of shifting colours. There were lakes along the way that appeared suddenly, calm and indifferent, as if they had no idea that cyclists were suffering nearby.
I found myself watching the road surface too, with a kind of clinical attention. Smooth tarmac felt like kindness. Rough patches felt like betrayal. Even a mild slope could feel personal after enough kilometres.
***
Abhishek remained close. He moved in and out of my shadow, as if he was managing my morale without making it obvious. There is a particular generosity in riding with someone who is capable of going faster but chooses not to leave you behind. It is not pity. It is partnership.
We did not talk continuously. Long rides do not encourage constant conversation. They encourage brief exchanges, practical questions, small jokes, and long stretches of silence that feel comfortable rather than awkward. The silence itself becomes a form of companionship.
Every now and then, Abhishek would ask, “All okay?” and I would reply, “Yes,” even when I was not entirely sure. But I meant it in the larger sense. My body might complain, but my mind was still willing.
***
At some point in the ride, I began to eat with the seriousness of a man who has understood consequences. I drank like a fish, ate like a horse, and stopped feeling shy about it. There is no elegance in long-distance cycling. You eat because you must. You drink because you must. Pride has no role here. If you try to be dignified, you will be punished.
It is a strange thing, this business of fuelling. In the hospital, I have lectured students for years about metabolism, electrolytes, and energy balance. On the road, I discovered that the body does not care about your lectures. It cares about what you put into it at the right time. Knowledge is useful, but timing is everything.
***
As the day progressed, the ride began to feel longer. Not harder, necessarily, but longer. The sun started sliding down, and the light softened. The body, which had been cooperating, began to remind me that it had limits. There were moments when I felt a dull ache in the shoulders, a quiet soreness in the back, a growing heaviness in the legs. Nothing dramatic. Just the steady accumulation of effort.
This is where mental discipline becomes more important than physical strength. You do not think of the remaining distance in one chunk. You break it down. You ride to the next landmark. Then the next. Then the next. You learn to live in small victories: one more hour, one more checkpoint, one more stretch without stopping.
Somewhere in that long evening, I realised that a 300-kilometre ride is not a single event. It is a series of negotiations with yourself. Each negotiation ends with the same agreement: keep going.
***
When we finally rolled back towards Nagpur, I expected to feel dramatic. I expected a rush of emotion, perhaps even a cinematic moment where I would lift my hands, grin wildly, and declare victory to the sky.
Instead, I felt something quieter and more satisfying: relief mixed with disbelief.
The bicycle had held up well. My body, to my surprise, had held up well too. There was fatigue, yes, but not the crushing kind. There was soreness, but not injury. There was the dull ache of effort, but also the glow of completion. I had crossed a distance that once seemed absurd.
Ashwini drove us back to Sevagram, carrying our tired bodies and our bicycles home. It was nearly midnight, and the world was busy celebrating the new year. I was celebrating something else: the discovery that I could stretch myself further than I had assumed.
***
The 300-kilometre brevet did not make me a champion. It did not turn me into a faster cyclist. It did not erase my age or my vulnerabilities. But it taught me something important about endurance: it is not a talent you are born with. It is a habit you build, slowly, through repeated discomfort and small acts of discipline.
It also taught me the value of friendship on the road. Not the loud kind, not the performative kind, but the steady kind that rides beside you and makes the distance feel less lonely. If cycling has a secret ingredient, it is not speed. It is companionship.
When I lay down that night, the body was tired, but the mind was strangely calm. I had not just completed a ride. I had learnt how to last.
Four Hundred, and a Wall
After finishing the 300-kilometre brevet, I began to behave like a man who had discovered a new version of himself. It was a subtle arrogance, not the loud kind. I did not boast about it, but I started assuming that if I could do 300, then 400 was only a longer afternoon on the saddle.
That is how the 400-kilometre brevet entered my calendar.
The event was scheduled for 15 January 2017. The target was to complete 400 kilometres in 27 hours. Twenty-seven hours sounds generous until you realise it includes everything: riding, stopping, eating, stamping, fixing, thinking, and occasionally staring into space while your brain tries to remember why you signed up.
Abhishek V. Raut and I started at 5:30 a.m. from Zero Mile, Nagpur. The route ran along the Nagpur–Amravati road, a familiar highway that can be kind when it wants to be, and brutal when it decides to test your patience.
That morning, it was kind.
***
For the first 180 kilometres, everything went so smoothly that it made me suspicious. The morning was pleasantly cold, the kind of cold that keeps you alert without making your fingers numb. The afternoon sun was warm but not harsh. The wind was gentle, not the sort that humiliates you by pushing back every time you push forward.
Even the road behaved.
The four-lane highway had enough undulations to keep things interesting, but nothing that felt punishing. The climbs came and went. The descents offered small moments of joy, the tyres humming on smooth tarmac. We rode better than I had expected. We were not sprinting, but we were steady. We were not reckless, but we were confident.
At some point, I began to believe that this might be one of those rare days when everything aligns: weather, body, mind, road, and luck. The kind of day that makes you forget that cycling can also be cruel.
I should have known better. The road has its own sense of humour.
***
The problem arrived quietly, without drama.
At around the 180-kilometre mark, my body began to misbehave in a way that I could not explain at first. It started as a vague uneasiness—an internal discomfort that had no clear location. Then came nausea. Then sweating. Then dizziness. Then a sudden heaviness, as if someone had poured wet sand into my veins.
Within minutes, my confidence evaporated.
It was not a mechanical failure. It was not a puncture. It was not a broken chain or a snapped cable. It was something far more unsettling: the body itself had decided to pull the plug.
Later, I realised what had happened. I had run out of sodium. An electrolyte imbalance. The very thing I had taught medical students about for decades, the very thing I had corrected countless times in wards and ICUs, had quietly ambushed me on the highway.
The irony was sharp enough to puncture pride.
I had heard the long-distance cycling dictum often enough: eat before you are hungry, drink before you are thirsty. I had remembered the first half. I had forgotten the second. I had been drinking, yes, but not enough. Worse, I had not replenished electrolytes properly. I had an Electral-filled bottle, and yet I had treated it like a decorative accessory.
As a physician, I could diagnose it. As a cyclist, I was helpless inside it.
***
Abhishek stayed close. He did not panic. He did not lecture. He did not say, “I told you so,” which is what I deserved.
He simply watched me carefully and adjusted his riding to mine. He offered practical support, slowed down, and stayed near enough for me to feel safe. In those moments, friendship becomes a form of first aid.
I tried to pedal through it, because cyclists are stubborn creatures and doctors are not much better. I told myself it would pass. I told myself it was temporary. I told myself I had come too far to quit.
But the body was no longer negotiating.
I managed to pedal painfully for another 20 kilometres, but it was clear that continuing would be foolish. Not heroic—foolish. There is a difference, and it becomes obvious when your vision blurs and your stomach turns against you.
When we reached the 200-kilometre checkpoint at Zero Mile, I told the volunteers that I was quitting.
The words tasted bitter, but they were necessary.
***
Stopping in a brevet is not like stopping on an ordinary ride. In an ordinary ride, you can tell yourself you will continue tomorrow. In a brevet, stopping feels final. It feels like failure stamped in ink.
I had not even crossed the halfway mark of the full 400. I had started well. I had planned well—at least, I believed I had. The weather had been kind. The road had been kind. My legs had been cooperative. And yet, something inside me had simply run out.
I sat with that reality, and it humbled me.
I have spent years in medicine explaining to patients that the body has limits. I have told them that rest is not weakness. I have counselled them not to push beyond what is safe. But when it came to myself, I was still learning the same lesson.
That day, my body became my teacher.
***
The disappointment of a DNF is sharp, but what troubled me more was Abhishek. He had the strength to continue. He had time on his side. He could have finished the brevet. But he chose to stop with me.
At first, I felt grateful. Then I felt guilty.
It is not easy to accept such loyalty, because it comes with a price. Abhishek’s decision was generous, but it also meant he gave up his own chance at a personal milestone.
That night, after we returned, I wrote him an email. It was part apology, part confession, and part attempt to set a rule for the future.
***
16 January 2017
Dear Abhishek,
It makes me feel sad and disheartened to see that I made you quit the 400-brevet. You neither were tired nor were running out of time and yet, you chose to quit—only to accompany me.
Your camaraderie and friendship were of great value to me during the brevet. I appreciated the tremendous support that you offered to me when I began to feel uneasy. I will always treasure the memories of you slowing down to ride with me during the last 20 km of the first half of the brevet. I tried my best to muster the willpower and strength to continue, but I was too exhausted. I still cannot figure out why I suddenly became nauseous and lost my strength, especially since I was doing so well until 175 km. However, sometimes we have bad days and despite everything being in our favour—the weather, the winds, and the road—we are just not able to make it. That's fate.
Let's make an unwritten rule for the next brevet we ride together: you will not quit, no matter what. Brevets are all about personal accomplishments, and in the context of a brevet, when faced with a choice between personal milestones and friendship, personal accomplishments should always be the automatic choice. I would have been thrilled if you had continued and returned to Sevagram with another feather on your handlebar. I feel guilty for not conveying that to you. So, please continue to provide support, companionship, and ride together, but when unforeseen events happen during a brevet, please do not quit and keep going.
Thank you again for your company. Riding with you is always a pleasure, and this brevet was no exception, except for the 175-km nightmare. Let's do it again next time!
Best regards,
SP
He replied almost immediately, and his reply carried the kind of clarity that makes you pause.
16 January 2017
Dear Sir,
Thank you for your email. I am sorry that my decision to quit the brevet has caused you to feel guilty. However, I want to make it clear that the decision was entirely mine, and you did not coerce me in any way. I have a clear conscience that even if I had wanted to continue, my sports ethics would not have allowed me to do so, and it would have played on my mind.
If I had continued, I may or may not have completed the brevet. But even if I had completed it, I would have had a sour taste of victory and would have had to live with the guilt of choosing personal glory over team spirit. This goes against how I have been trained, particularly in mountaineering where we were taught that 'life is much more than just making the summit'. We were ingrained with the belief that if we ever had to choose between reaching the summit and the health of our teammates, we should prioritize the latter without hesitation. The mountains will always be there, and as a team, we can always come back stronger to reach the summit. It should never come at the cost of any of our teammates.
I cannot predict what I would do if a similar situation arises in the future. Still, I know it will be challenging for me to choose otherwise. So, please don't feel guilty or sad for any reason.
For now, I want to say that this was not our last brevet. Yesterday was just not meant to be our day. Let's not dwell on it too much. Let's return more prepared and stronger and make it happen next time. The taste of victory is much sweeter when achieved together.
Warm regards,
Abhishek
P.S - Hope you are feeling better now after taking much-needed rest.
Reading his words, I felt two things at once. First, relief—because he was not angry or resentful. Second, admiration—because he was guided by a principle larger than cycling.
In medicine, we often speak of ethics as if they belong only to hospitals and courtrooms. Abhishek reminded me that ethics also belong on highways, in darkness, and in moments when someone must choose between achievement and loyalty.
***
That 400-kilometre brevet ended in a DNF, and yet it did not feel like a wasted day. It gave me something that the successful rides had not: humility in its purest form.
It taught me that the body can collapse without warning, and that preparation is not only about training miles but also about respecting basics—hydration, electrolytes, pacing, and recovery. It taught me that being a doctor does not make you immune to mistakes. If anything, it makes your mistakes more embarrassing, because you know better.
It also taught me something more personal. There is a point where stubbornness stops being courage and becomes foolishness. The trick is to recognise that point before the road forces you to.
I did not finish the 400. But I returned home safe. I returned home wiser. And I returned home with the quiet assurance that I would try again—not to prove anything to anyone, but to test the limits more intelligently next time.
That, I realised, is also a kind of progress.
Ten Thousand Kilometres
Some numbers carry an odd magic. They sit quietly in the mind, round and complete, like a destination on a map. Ten thousand is one of those numbers. It looks solid, respectable, and slightly intimidating—like a mountain you do not plan to climb, until one day you realise you have already begun.

My fascination with “ten thousand” did not come from cycling at all. It came from cricket.
I can still see Sunil Gavaskar reaching his 10,000th Test run. It was March 1987, in Ahmedabad, against Pakistan. Gavaskar nudged a quick single through the slips, raised his bat, and the crowd rose with him. He was never a man who looked at the scoreboard too often, but that day even he seemed aware that something had shifted. A personal milestone had turned into a historical one, and the moment carried a quiet weight.
That memory stayed with me for decades.
So when my Garmin watch flashed a number on the morning of 21 October 2020, I smiled in a way that surprised me. The screen told me I had cycled 10,000 kilometres. Not in one dramatic expedition, not in a single heroic season, but in hundreds of small rides stitched together over time.
It was seven in the morning, and I was standing near Vinobaji’s Pavnar Ashram, a place that always has the air of calmness, even when your legs are not calm at all. The breeze was gentle, the sunlight clean, and the road familiar. Nothing about the scene looked like an achievement. And yet, the number made it feel like one.
***
Ten thousand kilometres sounds impressive until you break it down. It is not a Tour de France. It is not even a professional cyclist’s annual tally. Serious riders cover that distance the way some people cover newspaper pages—quickly, routinely, without thinking too much about it.
For me, it was different.

Those 10,000 kilometres came from 533 hours on the saddle and 441 sessions of cycling on the roads around Sevagram and Nagpur. That is what made it meaningful. It was not one grand act of endurance; it was repetition. It was turning up again and again, often without drama, sometimes without enthusiasm, but with enough stubbornness to keep the wheels moving.

There were mornings when the air was cold enough to sting the ears. There were afternoons when the sun felt like it was sitting directly on my helmet. There were days when the wind seemed to blow only against me, as if the universe had singled out my bicycle for special attention. There were also mornings of rare kindness—cool breeze, empty roads, and legs that felt light.
Over time, cycling became less about the ride itself and more about the ritual around it: the preparation, the familiar routes, the quiet start, the steady rhythm of breathing, the little negotiations with fatigue, and the small satisfaction of returning home having done something honest with the body.
***
When I began cycling seriously, I did not imagine it would change my life. It was supposed to be a modest fitness habit, something to balance a profession that demanded too many hours of sitting, thinking, and worrying.
But the bicycle has a way of doing more than you ask.

It gave me a sense of freedom that is difficult to explain to someone who has not experienced it. You are not inside a car, sealed away from the world. You are not walking slowly, limited by time. You are moving through the landscape at a human speed, fast enough to feel distance, slow enough to notice details.
You notice the smell of wet earth after rain. You notice the way villages wake up—tea stalls opening, schoolchildren appearing like clockwork, farmers moving with quiet purpose. You notice the small dramas of rural roads: a herd of cattle that refuses to negotiate, a dog that decides your tyre is an enemy, a motorcyclist who passes too close and then looks offended when you flinch.
Cycling also made me confront my own limits in ways that hospital life never did. In medicine, experience often gives you a sense of control. On a bicycle, control is an illusion. A puncture can reduce you to helplessness. A headwind can humble you. A missed bottle of electrolytes can turn a strong ride into a slow collapse.
The road does not care about your degrees.
***
Brevets entered my life like a strange new language. At first, I admired them from a distance. Then I tried them, failed, tried again, succeeded, and failed again. They gave me some of the best days of my cycling life, and also some of the most humbling.
A brevet is not a race, but it has rules. It is not competitive, but it demands discipline. You ride within a time limit. You stamp your card at checkpoints. You carry what you need. You manage your own mistakes.
There is no applause on the highway. There is only the quiet satisfaction of finishing, and the equally quiet sting of a DNF when you don’t.
I learnt that finishing a brevet is not just about fitness. It is about pacing, planning, eating, drinking, staying calm when things go wrong, and not wasting time at checkpoints because the khichdi is hot and your granddaughter looks delighted to see you.
I learnt these lessons the hard way, which is the only way they truly stick.
And yet, even the failures gave me something valuable. They taught me that a DNF is not a verdict on your worth. It is simply a data point. It tells you what went wrong: tyre trouble, time lost, hydration mismanaged, confidence misjudged. You go home, you rest, you adjust, and you return.
That, too, is a kind of success.
***
One of the most refreshing things about cycling was how anonymous it made me.
In the hospital, I was “Sir,” “Professor,” “Medical Superintendent,” a man with responsibilities and a reputation. On the road, I was just another cyclist in a helmet, squinting against the wind, negotiating potholes, and trying not to look foolish at traffic signals.
The villagers did not ask me about research papers. They asked me my age. They asked me where I was going. They asked me whether I was doing it for prize money. When I said no, they looked at me with a mixture of admiration and disbelief, as if I had confessed to a harmless madness.
Sometimes, they offered water. Sometimes, they offered directions. Sometimes, they offered unsolicited medical advice about their knee pain or blood pressure. I learnt to smile, answer politely, and keep riding.
There was a simplicity in those interactions that felt cleansing.
***
When the Garmin signalled 10,000 kilometres, there was no crowd. There was no certificate. No medal. No stage. No announcement.
There was just me, a road near Pavnar, and a quiet moment of gratitude.
I knew, even as I looked at that number, that professional cyclists would consider it trivial. I had seen riders half my age climb hills effortlessly, sprint through stretches that left me gasping, and finish brevets with an ease that I could not imitate. I had watched their speed, their commitment, their confidence, and I knew my own place in that universe.
But the value of a milestone depends on where you started.
When I began cycling seriously, I did not imagine I would ever reach 10,000 kilometres. I did not even know if my body would allow it. I had a stent. I had age. I had the ordinary wear and tear of a life lived in hospitals, meetings, and long working days. The bicycle did not erase those realities. It simply worked around them.
It gave me a path that felt less travelled, even though it was made of the same Wardha roads I had seen all my life.
***
After reaching 10,000 kilometres, the mind does what it always does. It looks ahead.
Once you have met a target, you feel tempted to set another. Twenty thousand. Thirty thousand. A new brevet. A longer ride. A different route.
But I also learnt that cycling cannot be reduced to numbers alone. The real reward is not the kilometre count. It is the habit. It is the way cycling turns the morning into something you look forward to. It is the way it gives you a small pocket of freedom before the day fills up with duties.
If you ask me now what my goal is, I can offer a dramatic answer—twenty thousand kilometres, perhaps. But the truth is simpler.
I want to keep riding.
Not because I have something to prove, but because the bicycle has become a quiet companion. It asks little. It gives much. And on most mornings, it still feels like the best way to begin the day.
A Life in Books
From a young age, I have been pulled towards books the way some people are pulled towards a cricket match on the radio. I don’t remember making a decision to read. It simply happened, quietly, in the corners of my childhood.
In the beginning, it was the familiar world of stories. The Ramayana and the Mahabharata arrived early, like visiting elders who stayed long and spoke in grand sentences. I didn’t understand every motive or moral complication, but I was mesmerised all the same—by exile, by vows, by battles that seemed to last forever. The Panchatantra followed, and I liked it for a different reason. It was clever. It had animals behaving like people, and people behaving worse than animals. Even then, it felt like a small education in human nature.
I read in bed, I read after homework, and I read when I was supposed to be doing something else. If I look back, that habit may have been my first act of rebellion—silent, harmless, and deeply satisfying.
***
As I grew older, my reading changed its flavour. I began leaning towards history. Not because I was planning to become a historian, but because history has a way of explaining the present without shouting. It makes today look less dramatic and more inevitable.
I liked how a single decision made in one decade could echo across generations. I liked how empires rose with arrogance and fell with routine mistakes. I liked the small details—what people ate, how they travelled, what they feared, how they justified themselves. History, I discovered, was not just about dates and dynasties. It was about people doing ordinary things and believing they were doing something extraordinary.
Over time, I started noticing something else. The more I read, the less certain I became. That, I realised, is one of the quiet gifts of books: they reduce your confidence just enough to make you decent company.
***
There is a paradox in my reading habits that still amuses Bhavana.
I have no artistic talent. I cannot sing—at least not in a way that should be inflicted on other human beings. I have never performed on stage. I don’t play an instrument. Even clapping in rhythm is not my strongest skill.
And yet, I keep picking up biographies of people who live by music, theatre, cinema, and applause.
Bhavana sometimes asks, quite reasonably, why I read about musicians when I could simply listen to their songs. The answer is embarrassingly simple. I am not chasing the performance. I am chasing the effort behind it.
A great singer’s voice may sound effortless, but the story behind it rarely is. A composer’s melody may feel like it was born in a moment, but the moment is usually built on years of practice, rejection, and stubborn persistence. Reading these lives reminds me of something I already know from medicine: excellence is mostly repetition, and glamour is usually the final layer of paint.
So yes, I have spent evenings reading about artists—sometimes one chapter at a time, sometimes in long greedy stretches. Not because I want to become one, but because I like seeing how people endure the long, unromantic middle of their lives and still keep going.
***
K.K. Birla once said that finance runs in the blood of a Marwari, just as chivalry runs in the blood of a Rajput. When I think of my father, I can see what he meant. My father had a natural sense for business. He didn’t need a book to tell him what was sensible and what was foolish. He could smell risk the way some people smell smoke.
I, on the other hand, took a detour. I chose a medical college, a hospital, and a life that revolved around wards, rounds, and teaching. It must have looked like a strange choice from the outside—especially to a family that understood trade more instinctively than textbooks.
But genes, I have learnt, can express themselves in odd ways.
In the last decade or so, I have found myself returning to finance—not as a businessman, not as a trader, but as a curious student. I began reading about value investing and long-term thinking. I liked the discipline of it. I liked the insistence on patience. I liked the warning, repeated in different words by different people, that your biggest enemy is not the market—it is your own emotions.
I won’t pretend I became wise overnight. I didn’t. But the reading gave me a framework. It also gave me something else: the pleasure of being a beginner again.
***
Of course, a large part of my library belongs to my profession. There are books on statistics, study designs, critical appraisal, and Evidence-Based Medicine. These are not the sort of books one reads for comfort, but they do offer a different kind of satisfaction. They make the mind sharper. They keep arrogance in check. They remind you that certainty must be earned, not assumed.
Over the years, I have read these books the way some people do crossword puzzles—slowly, repeatedly, sometimes with mild irritation, but always with the feeling that the effort is worth it.
And then there are the books that sit beside them, almost mischievously: biographies, memoirs, essays, and cricket writing. I like the mix. It feels like my mind has multiple rooms, and each room needs its own kind of light.
***
Cricket has always been my other addiction—cleaner than sugar, less expensive than travel, and far more difficult to explain to non-cricketing nations.
I have enjoyed reading about cricketers not because they were perfect, but because they were tested. A batsman facing a hostile spell is not very different from a young doctor facing a hard night in the ICU: you breathe, you focus, you try not to panic, and you do the next right thing.
There is also comfort in cricket’s long format. It respects patience. It rewards temperament. It punishes vanity. It reminds you that you can do everything right and still lose. That lesson, unfortunately, is also useful in medicine.
***
For decades, my reading life had a steady rhythm. I would visit a bookshop, scan the shelves, pick up a book, flip through a few pages, and carry it home like a small trophy. The book would then join its brothers and sisters on the shelf—some read immediately, some waiting their turn, some waiting far too long.
Then, in 2020, my children gifted me a Kindle.
I will admit it: the convenience is seductive. A book appears in seconds. No searching, no travelling, no “out of stock.” It feels like magic. It also feels faintly like cheating.
And yet, I remain an old-fashioned reader at heart. I still like paper. I like the weight of a book in my hands. I like underlining a sentence and returning to it years later. I like seeing books on shelves the way some people like seeing plants in their garden—quietly alive, waiting.
I also like the mild guilt that comes with it. My shelves are overflowing. There are books I bought with good intentions and never finished. Some have been waiting for years, staring at me patiently, like polite guests who have learnt not to expect too much.
***
Books have been my most dependable escape after a long day in the hospital. They have also been my most silent teachers. They do not interrupt. They do not argue. They simply wait.
Sometimes I read for knowledge. Sometimes I read for perspective. Sometimes I read for the simple pleasure of entering another life for a few hours. A good book has the power to make your own worries shrink to their proper size.
I may have stepped away from administrative responsibilities, but as long as there is a book nearby, I don’t feel retired in the mind. I feel unfinished—in the best possible way.
Cricket, and the Crowd
In the winter of 1969, I was thirteen and newly transplanted from Craddock High School to Swavalambi Vidyalaya in Wardha. Those were the years when television sets were rarer than a hat-trick in a Test match, and cricket reached most Indian homes the way gossip does: through voices, rumours, and the occasional grainy photograph. My cricket education was forged in the crackling devotion of radio commentary and the small black-and-white images in newspapers. I knew the names, the scores, and the heroes, but I had never seen a real pitch with real players moving across it. A live match, for a boy like me, was not a plan; it was a private fantasy that one didn’t even dare say aloud, lest it dissolve.
Then my father’s friend, Mr. Champalal Fattepuria, performed an act as generous as it was unexpected by offering to take me to Nagpur for the second Test match between India and New Zealand at the old VCA ground near Liberty Cinema. Jamtha, with its grand modern stadium, was still a distant future; this was the Nagpur of narrow roads, familiar squares, and a stadium that seemed enormous simply because I had never entered one. As we drove toward the ground in Mr. Fattepuria’s car, I felt a tightening in my stomach that had nothing to do with motion sickness—it was the anxious thrill of stepping into a world that had previously existed only in sound.
***
The stadium was buzzing long before the first ball was bowled, the air carrying a thick mixture of dust, sweat, and the smell of snacks. People looked serious, as if they were about to sit for an examination. I climbed the steps and suddenly saw the field open up below me—an oval of green so bright it looked almost artificial. Players in crisp white flannels moved like they belonged to a different class of human beings. I remember being spellbound not only by the game but by the presence of the men themselves. Mansoor Ali Khan Pataudi Jr. was there, marshalling his troops with that unmistakable air of command, and around him were names I had worshipped in print: Bishan Singh Bedi, Erapalli Prasanna, Farokh Engineer, Ajit Wadekar, and S. Venkataraghavan. Just watching them take their positions felt like witnessing history being assembled ball by ball.
Farokh Engineer fascinated me most. He stood deep behind the stumps to the medium pace of Syed Abid Ali and Rusi Surti, collecting the ball with an effortless flourish before whipping it to Wadekar at first slip as if it were a casual reflex. As a boy who had grown up watching cricket in his imagination, I could not believe that such elegance could be routine. That match also gave me a debut to remember: Ambar Roy, a left-hander, walked in after the seventh wicket and began cutting and pulling Hedley Howarth with a confidence that defied his position in the order. I can still see those strokes—sharp, clean, and slightly defiant—as if he had decided that if the seniors were failing, he would take responsibility for their dignity. India lost that match by 167 runs, but defeat felt irrelevant. I returned home convinced that the radio, for all its magic, could never recreate the collective gasp of twenty thousand people when a ball beat the bat by a whisker.
***
In the 1970s, tuning a transistor was an act of delicate surgery. The needle slipped and the signal wandered through static, meaning that finding the right frequency required a patience that felt almost spiritual. We would gather—shoulders touching—at a paan shop, a café, or a dusty street corner, creating a sudden, silent community around a single plastic box. These commentators were not merely narrators; they were architects of what Vikrant Pande and Neelesh Kulkarni describe as the "theatre of the mind." Because those words were the only eyes we had, men like Suresh Saraiya and Anant Setalvad had to paint the glare of the afternoon sun and the lengthening shadows across the pitch.
They were masters of the pause; the heavy silence on the radio wasn’t empty, but rather the tension before a delivery—a shared breath between the roaring stands of Chepauk and a small transistor in Wardha. As I moved from the classrooms of Craddock High to the hostels of GMC Nagpur, these voices—the baritone of Jasdev Singh, the excitement of Dr. Narottam Puri, and the rhythms of Dicky Rutnagur—became the soundtrack of my life. We weren't just listening to a match; we were watching a world being built inside our heads.
***
Six years after my first Test, I was a third-year medical student at GMC Nagpur. Diwali was approaching when my classmate Omprakash Singhania and I decided to watch the Irani Trophy final between Rest of India and Bombay. It had poured heavily the day before, leaving the ground wet, so we did what students do when they lack the luxury of cushions: we laid down sheets of The Indian Express and our handkerchiefs, hoping our trousers would survive the day. We had come for the famous names—Gavaskar, Vishwanath, Prasanna—but instead, we were served a lanky, unknown teenager called Dilip Vengsarkar. When he walked in, the crowd groaned with the impatience of those who believe they have paid for stars, not apprentices.

Then he began to bat. What followed was so unexpected that it still feels slightly exaggerated, even though it happened in front of my eyes. Vengsarkar played as if he had no respect for reputations, hitting seven sixes against an attack that included Bedi, Prasanna, and Venkataraghavan. It was a display of fearlessness that belonged to a later era, christening him “Colonel” in the eyes of the delighted Nagpur crowd. Years later, I found that Vengsarkar hit only 17 sixes in 116 Test matches; it appears he had spent almost half his lifetime quota on that one rainy afternoon, and I was lucky enough to be there for the spending.
***
Over the decades, my preferred seat became the East Stand. It began as a student’s choice—cheap tickets and no need to pretend you belong elsewhere—but I stayed for a different reason: the East Stand is real. It has no polish and no patience for pretence. You sit on concrete, you sweat, you inhale dust, and you discover that shade is a privilege. Yet it is there that the true pulse of cricket beats. The audience participates, offering unsolicited coaching tips to long-off fielders who cannot hear them and ridiculing misfields with the cruelty of experts who have never had to bend their own backs.
I learnt the value of the East Stand the hard way in 2010 when I was gifted passes to a Corporate Box at the new Jamtha Stadium. The box was magnificent—air conditioning, fine dining, and glass walls—but within a few hours, we became bored. The match felt sterile, like watching fish through glass in an aquarium. The crowd’s roar arrived muted and disinfected. We left shortly after lunch, mildly ashamed, as if we had betrayed cricket by expecting it to entertain us without the crowd’s heat. That day taught me that comfort is sometimes the enemy of experience.
***
The cricket I grew up with has transformed into a financial behemoth. Franchises are now bought for sums that could fund public health programmes for decades, and cricketers have become global brands with entourages larger than the team itself. When I look back at the receipts of the 1983 World Cup heroes—match fees of Rs 1,500 and a daily allowance of Rs 200—it feels like a different civilisation. Many players held bank jobs and lived carefully, counting money as middle-class families do. Today, the world applauds their “humility” for posting a photograph in economy class while they drive Audis. The game has grown richer, faster, and louder, but sometimes I miss the simple joy of watching cricket without knowing what a “brand value” is.
***
In January 2026, I watched an India–New Zealand T20 match at Jamtha with my son and my granddaughters—three generations and a mind full of old memories. It took me back to that first match in 1969, where I was a wide-eyed schoolboy counting every run. This time, the match became almost nameless. From our seats, the scoreboard was too far to read, and I spent the evening doing something doctors are not trained for: guessing. Only after it ended did I realize Sanju Samson had opened or that Axar Patel was even playing.
***
Yet something made up for the lack of data: the crowd, the roar, and the chants of “India Jeetega!” For four hours, thousands of strangers felt like family, and my granddaughters enjoyed every minute, oblivious to strike rates or partnerships. It took nearly an hour to walk a kilometre back to our car, and we reached home past midnight—tired, hoarse, and happy. Somewhere between Jamtha 2026 and Sadar 1969, I realized the game remains the same, but the world—and the eyes watching it—has changed.
Two Hundred Classmates, Six Hundred Pages
Sir Terry Pratchett once wrote, “If you do not know where you come from, then you don't know where you are, and if you don't know where you are, then you don't know where you're going.” I had read that line much later, of course, but it described exactly what I felt about my batch at Government Medical College, Nagpur.
It really did feel like yesterday when we walked through those imposing gates in 1973—two hundred and four young men and women, convinced that life was long, health was permanent, and the future was something that would politely wait for us. We threw ourselves into dissections and ward postings, into canteen arguments and late-night study sessions, behaving like people who had never heard of the word “deadline.” In those days, we worried about viva questions and internal marks. We didn’t yet worry about blood pressure, joints, or the quiet arithmetic of age.
That arithmetic became impossible to ignore in 1998, when we met for the first time after graduation. It was our Silver Jubilee reunion, and it arrived with the kind of shock you get when you suddenly see yourself in an unflattering mirror. We looked at one another and noticed the grey hair, the expanding waistlines, the new paunches, and the lines that twenty-five years of living had etched into familiar faces. We were still ourselves, but we were also—unmistakably—older. The spirit remained eager; the biology had started negotiating its own terms.
As a physician, I knew what those terms usually were. I knew what happened silently inside arteries and joints. I knew how memory could become selective, and how quickly names could slip away even when faces stayed stubbornly familiar. Somewhere in that unsettling realisation, a thought took root: before time blurred us into a fog of “I think he was in our batch,” I should try to preserve us properly. Not as a sentimental gesture, but as a record. A name attached to a face. A roll number attached to a life.
I didn’t want a dry directory of phone numbers and clinic addresses. I wanted a chronicle—something that captured what life had done to the Class of ’73 after it released us into the world. Who stayed in Vidarbha and served quietly in small towns? Who became professors and heads of departments? Who migrated across oceans, and why? Who left medicine altogether? And who had already left this world without giving us a chance to say a proper goodbye?
So, sometime around 2014, I began maintaining a database of my batch—methodically, almost obsessively—and started writing individual profiles of my classmates. It turned into a project that felt like equal parts detective work, census-taking, and affection. The profiles gradually piled up on my Google Drive, waiting patiently for the one thing every manuscript waits for: a publisher—or at least a generous funder.
***
Tracking down two hundred and four classmates would have been easy if we had graduated in the age of email and LinkedIn. But we belonged to a time when people simply disappeared. When we passed out, there were no mobile phones, no WhatsApp groups, no Facebook timelines, and certainly no digital breadcrumbs. A person changed cities, changed jobs, and vanished. The only evidence that he had once existed in your life was a faded photograph and a nickname that still made you smile.
I began with what I had: old lists, half-remembered addresses, a few phone numbers scribbled on paper, and a willingness to be embarrassed. I spent hundreds of hours making calls that began awkwardly and ended emotionally.
“Hello… is this Dr Deshpande who studied at GMC Nagpur in 1973?”
There would often be a pause. Then a sharp intake of breath. Then laughter, disbelief, and the sudden opening of a floodgate. Names came tumbling out. Incidents resurfaced. People I had not spoken to in decades began talking as if we had met last week. I listened more than I spoke. That, I realised, was the only way to do it properly.
The work was slow because I refused to outsource it. I wanted to hear voices, not just collect information. I took notes by hand, like a stubborn old-fashioned clerk, and then typed them out late at night. I checked dates, cross-checked spellings, verified details, and edited each profile until it read like a person rather than a list. Somewhere along the way, I stopped being merely a batchmate and became a reluctant archivist of my own generation.
***
No project like this survives on one person’s enthusiasm alone. I was the one doing the writing, but the work gathered momentum because others joined in—some deliberately, some accidentally, and some with the zeal of people who had been waiting for an excuse to reopen old memory trunks.
T. F. Badodekar became one of the unexpected heroes of this story. Ironically, during college, we had barely spoken. We shared Medicine as a discipline, but not friendship as a habit. Yet, in the summer of 2014, he became my right hand. He had a memory that worked like a steel trap and an energy that felt almost unfair for his age. Hardly a day passed without a phone call. He dug out contacts as if he were excavating fossils, dictated details to me, and followed up relentlessly. We ended up bonding more in our sixties than we ever did in our twenties.
He did not live long enough to see the project reach print. He passed away in the winter of 2014, leaving behind a silence where his daily enthusiasm used to be. But his presence remained embedded in the work. Every time I found a missing classmate because of a lead he had provided, I felt as if he was still quietly doing his rounds.
Manik Khune kept me going in a different way. If Badodekar was the relentless sleuth, Manik was the steady opening batsman who made sure the innings did not collapse. He knew the stories of classmates who had stayed back in small towns—the “now it can be told” details that never appeared in formal alumni notes. He read, corrected, edited, and gently pulled me back when I became too sentimental or too long-winded. In a project that threatened to become unwieldy, he provided rhythm.
Distance did not weaken the effort either. Harsha Sheorey in Melbourne and Sharad Jaitly in New York helped connect the international dots. They made the Class of ’73 feel like a global village long before we started using that phrase casually. Time zones did not stop them. They kept the momentum alive, and they made sure that the diaspora did not become invisible.
Raymond Maugham added another layer. He flew from Barbados for the 2013 reunion with the confidence of a man who knew how to frame a moment. A professional photographer with a large presence, he did not merely attend; he documented. At the VCA Stadium, he moved around with his camera as if he were collecting evidence of time itself. Many of the photographs that eventually found their way into the draft were his. He did not just take pictures; he captured expressions, hesitations, and that unmistakable mix of pride and disbelief that comes when old classmates meet after decades.
There were others too—Vinayak Sabnis, who had the gift of storytelling and a nose for the amusing scandal; Ravindra Jharia, Mohan Gupte, Vivek Deshpande, and many more. Each one helped locate a missing piece of the jigsaw.
***
Every long project has a silent sponsor. Mine was Bhavana.
When I began, she thought it was a harmless phase—some calls, some nostalgia, a few evenings spent laughing into the phone. She assumed it would fade away like most hobbies do. Instead, it expanded. Weeks turned into months. My evenings disappeared into long conversations with people I hadn’t seen in forty years. I monopolised the computer. I interrupted dinner to scribble down a forgotten nickname. I behaved like a man possessed by the fear that if he didn’t write something down immediately, it would vanish forever.
Bhavana endured it with the kind of patience that spouses acquire either through love or exhaustion. She tolerated my obsession, gave me the freedom to keep working, and pretended not to notice how often I said, “Just five more minutes.” If she had not absorbed the domestic inconvenience, this entire exercise would have died quietly in the recycle bin of my computer.
***
By the time the draft took shape, it had become more than a list. It carried the arc of lives—careers that soared, careers that stalled, personal tragedies, private triumphs, quiet service, and occasional reinvention. It reminded me that our batch did not produce one kind of doctor. It produced every kind of human being.
I circulated the draft during the reunion at the Vidarbha Cricket Association ground in Nagpur in December 2013. I watched classmates flip through pages, pause at photographs, widen their eyes, and break into laughter. Some pointed at faces and said, “Arre, look at him!” Others went quiet for a moment, reading about someone they had assumed was still around. It was then I understood that the work had value—not because it was impressive, but because it was necessary.
Since then, I had kept updating the database—phone numbers, addresses, family details, career changes—adding new profiles, refining old ones, and storing everything carefully on my Google Drive. The material waited, as manuscripts often do, for the right time and the right patron. It waited to be printed, bound, and held in hands that once held anatomy textbooks in 1973.
In the end, the Class of ’73 book was never meant to be a monument. It was meant to be a mirror and a map—showing us where we had come from, where we were, and how far we had travelled, often without even noticing.
If nothing else, it gave me one quiet satisfaction: before time could blur us into anonymity, I had tried to call each person by name.
Fifty on the Sixtieth
August 15, 2007. For the nation, it was the sixtieth Independence Day. For me, it was my fiftieth birthday.
Fifty is a peculiar milestone. In cricket, it earns a raised bat and polite applause. In real life, it earns something quieter — a moment of stock-taking that arrives uninvited at four in the morning. You look back at the steep climb of youth. You look ahead at the long, level road. You wonder, with a faint unease, whether the ratio is still in your favour.
I woke that morning with the usual jumble — gratitude for the life we had built in Sevagram, a residual warmth from my year at Berkeley, and the kind of restless curiosity that round numbers produce: what had I done right, what had I left undone, and how much runway remained?
I did not get the luxury of introspection. My family had been plotting.
For months, without my knowledge, Ashwini, Amrita, and Shaily had been running a quiet operation. Third-year medical student, school-going daughter, and family friend — between ward duties and examinations and the ordinary demands of their lives, they had reached out to a constellation of people from my past and present. Family. Childhood friends. Colleagues. Students. And the new friends I had collected, unexpectedly, in California.
None of them told me.
The reveal was theatrical in the way only families manage without trying too hard. They handed me a heavy, hard-bound book — sleek, black, with the letters SP embossed on the cover. It looked like something between a biography and a file from a detective's desk.
It was neither. It was a chorus.
Shaily had curated the photographs — an unbroken visual line from my knobbly-kneed childhood in Wardha to the convocation robes of Berkeley. Ashwini had edited and arranged the text despite the cruelty of exams and ward rounds. Amrita had coordinated the outreach with the persistence of someone who does not accept I'm busy as a final answer. They had printed it professionally in Nagpur. It had the weight of effort, not just paper.
When I opened it, I realised it was not a photo album. It was a mirror.
We assume we know who we are. We do not — not clearly — until someone holds up a different angle.
Bhavana wrote about our twenty-five years together. The beautiful stretches, the rough patches, the small quarrels that now looked almost comic in hindsight. She teased me about my stubbornness — including the famous names controversy when the children were born. But she also wrote about the one thing she valued most: the way I had made learning a shared habit in our home. Reading her piece, I understood something I had not quite articulated before. Our marriage had become, over time, an intellectual partnership. Two people learning how to grow without drifting apart.
Pushpa Jiji, my elder sister, took me back to the beginning. My early fascination with the Ramayana and Mahabharata. My strange childhood hunger for books. The steady pull I had always felt toward Sevagram. Reading her words, I realised something I often forget: many choices I thought were decisions had been, in some ways, destinations.
Dr MVR Reddy wrote about a chilly December night, years ago, when his son Shridhar was born. A difficult birth. He described how I had stayed through those long hours — pacing corridors, calling surgeons, hovering without fuss, doing the small things that matter when someone you love is frightened. In the rush of everyday life, I had forgotten that night entirely. His words returned it to me, intact.
Friendship, I learnt again, is often forged in hospital waiting rooms, not at celebratory dinners.
Dr Suhas Jajoo brought back my college days — my sketches, a hobby I had quietly abandoned; my widely acclaimed final MBBS practical exams; my early obsession with research. He called me shy and self-effacing. I smiled at that. I had spent years trying to outgrow shyness, only to discover that it does not disappear. It simply learns better manners.
Then came the students. That section made me laugh, wince, and soften — all within a few pages.
Dipesh, a bright young doctor, described a bedside clinic where I had lost my temper. The final-year students had arrived unprepared — clueless about even the basic causes of fever. I refused to teach. Go to the library, I told them, and walked out. He wrote about the terror of that moment. He also wrote about what happened next: I returned the following day and spent two hours teaching them properly — how to think, how to investigate, how to treat, and how to respect a patient's story before chasing the lab reports.
Dipesh also mentioned something oddly tender. He had noticed my signature, found it distinctive, and secretly started imitating it.
I had never imagined that a teacher's influence could travel through something as trivial as handwriting. But perhaps that is how teaching works. You do not just transfer knowledge. You leave behind habits, gestures, and tiny imprints you never planned.
The book then crossed the ocean.
Christine Ho, Maureen Morgan, and Joseph Ezoua — my Berkeley quartet, minus one — had each sent something from far away.
Christine wrote about the atmosphere of learning I had tried to create, and about how my small studio apartment on Channing Way had become a second home for the study group. She remembered the gelato after long exams, the trips down to Berkeley's Gourmet Ghetto for Indian food at the end of semester. She remembered, too, the 200 to 300 patients who had gathered at Sevagram's train station to see me off when I left for America — and said she had understood, from that single image, exactly what kind of person I was.
Maureen wrote about her thesis. Two months before it was due, her intended topic had collapsed. She was certain she would not graduate. When I heard, I sat down with her and we found a new direction. She not only completed the paper — we published it together months later. She wrote that this was the kind of loyalty that defined me, and that I had a gift for making people feel they had done everything themselves. I am not sure that is entirely true. But it is the kindest thing anyone has ever written about the way I try to help.
Joseph wrote the shortest tribute and, in some ways, the most lasting. Our friendship means too much to me to find the words. He wrote about our discussions, our shared ambitions for public health in our respective countries, and then he wrote something I have returned to many times since:
SP would share advice and then stand back to let you choose your own way. Then, he would lend a shoulder when it was your own heart you were losing.
Reading their words in Sevagram — thousands of miles from Shattuck Avenue, from the library steps, from Christine's living room floor covered in open textbooks — I felt the world contract into something manageable. The distances remained. The relationships did not.
And then came the voices that mattered in a different way.
Ashwini wrote something every father hopes to hear but rarely does. He admitted, with a kind of reluctant affection, that he was beginning to notice himself becoming more like me. Amrita thanked me for the one thing I valued most: trust. She wrote about how I had supported her decisions without hovering, and she remembered the nonsensical rhymes we used to make up when she was a toddler.
Shaily called me the cynosure of all eyes. That line made me blush — not because it was untrue, but because it was too generous.
Families, I realised, are often kinder than facts.
We cut the cake, laughed, and took photographs. But the real celebration happened later, when the house had settled and the noise had thinned. I sat with the black book in my lap, turning pages slowly, as if I might miss something important if I rushed.
Fifty is often described as the age of the midlife crisis — panic about time, anxiety about unfinished dreams, fear of irrelevance. But that evening, what I felt was not crisis. It was integration. Ashwini, Amrita, and Shaily had given me the gift of my own history. They reminded me that my life was not a sequence of events. It was a web of relationships.
The black book still sits on my shelf. It is more valuable than any degree or award I have collected. It is proof — not of achievement — but of something quieter and rarer:
That I have lived, loved, and been loved in return
The House That Took Its Time
For a doctor in a government-aided setup, living in “quarters” is not a temporary arrangement. It is a way of life. You learn to make peace with peeling paint you cannot fix, a cracked bathroom tile you can’t replace, and rooms you can’t expand even if the family expands. You also live with a quiet, persistent awareness: the roof over your head belongs to your job. The day the job ends, the house can politely ask you to leave.
Yet the instinct to build a nest is primal. Even the most disciplined professional, trained to accept uncertainty, secretly wants one stable corner in the world where nobody can issue a transfer order.
My journey towards owning a home was long, winding, and full of false starts. In 1991, full of optimism and slightly short on foresight, I bought a large plot in Warud village, barely three kilometres from the hospital. In those days, Warud was the preferred suburb for MGIMS doctors. It felt like a sensible decision—close enough for emergencies, far enough to feel like a “real” home.
I held on to that plot for more than a decade, as if possession itself would one day turn into construction. In 2003, I finally began behaving like a man who meant business. I sat down with architects—Mr. Anil Pandit from Wardha and Mr. Ramteke from Nagpur—and we drew plans with the seriousness of people who believe the future is obedient. We spent days discussing layouts, ventilation, the position of windows, the direction of sunlight, and the kind of home we imagined ourselves growing old in.
But as it often happens, the plans remained on paper. The Warud home never rose from the ground. The plot stayed a plot, and I stayed in quarters, telling myself that there was no hurry—while time quietly did what it always does.
***
The Aurangabad Decision
The turning point came in February 2007, at a wedding in Aurangabad. Weddings do that to you. Between the rituals, the laughter, and the relentless pressure to eat more than your stomach allows, people start talking about life. Not philosophy, but practical life—retirement, security, and the uncomfortable truth that a professional identity cannot serve as a permanent address.
In the festive chaos of my niece’s marriage, a group of us—friends and colleagues—began speaking about our future in Sevagram. The Kasturba Health Society had a large tract of vacant land on Ashram Road. It was quiet, close to the hospital, and steeped in that rare Sevagram calm that makes you lower your voice even when you don’t have to.
“Why don’t we build there?” someone suggested.
It wasn’t just my decision. It became a collective migration. Dr. A.M. Mehendale, Dr. Ajay and Smita Shukla, Dr. MVR Reddy, Dr. Virendra Vyas, Dr. Anshu and Subodh, and later Dr. S.C. Jain and Sudha—many of us decided to take the plunge together. It felt less like building individual houses and more like building a neighbourhood of friends. In a place like Sevagram, where work is intense and personal space is limited, that mattered. We weren’t merely buying land. We were buying companionship.
***
To design the structure, we engaged Mr. Girish Deshmukh, an accomplished architect from Pune. The connection was almost Sevagram-like in its coincidence—he was a classmate of my niece, Jyoti. Girish understood what we wanted without being told too many times: not a showpiece, not a city imitation, but a home that belonged to its surroundings.
He passed away prematurely in January 2023, presumably due to a heart attack. It was one of those sudden departures that leave you unsettled—not only because a life ends, but because the person remains present in the world through what he created. Every time I look at the structure of our house, I remember that Girish’s lines still stand, even though he does not.
The construction itself was not a smooth academic exercise. It was real life—cement delays, labour issues, material shortages, and the small-town version of logistical chaos. We were fortunate to have friends who helped us navigate the mess: Mr. P.L. Tapdiya, Bharat Doshi, and Iqbal Saifee. Their support was not dramatic, but it was crucial. In building a house, the most valuable help often comes not from expertise, but from steady presence.
***
If Girish gave the house its skeleton, Jyoti gave it a soul.
Jyoti—my elder brother’s daughter-in-law—was a Mumbai-based architect and interior decorator. When we mentioned the project to her, she didn’t just offer polite advice. She adopted it. There is a difference between helping and owning responsibility, and Jyoti chose the second.
Building a house tests budgets, patience, and relationships. It also tests your ability to remain civil over ridiculous matters—like the shade of a tile or the placement of a switchboard. Jyoti brought a professional rigour we were unaccustomed to. She listened carefully, drew diagrams, asked uncomfortable but necessary questions, and separated our unrealistic fantasies from practical realities with the gentle firmness of someone who knows the difference between a dream and a mistake.
Then she did something that still amazes me. She brought her own team of skilled workers from Mumbai to Sevagram. Suddenly, our dusty plot began buzzing with the efficiency of a metro construction site. The local workers watched, learnt, adapted, and improved. Jyoti did not merely supervise. She taught—what to do, why it mattered, and how it should be done.
I had spent my life teaching medicine. Watching Jyoti teach craftsmanship was humbling.
***
Jyoti’s design philosophy was simple: elegant and unpretentious. She understood instinctively that we didn’t want a palace. We wanted a home. Something airy, light-filled, functional, and calm. She created clean lines and open spaces, letting the house breathe. She handpicked every tile, every fixture, every colour—choices that Bhavana and I would never have made on our own, partly because we didn’t know such options existed, and partly because we would have been too frightened to experiment.
She respected our taste, but she also nudged it forward. Not with arrogance, but with quiet confidence. “This will age well,” she would say, and we learnt to trust that sentence.
Her role went far beyond design. She became, unofficially, our construction therapist. There were days when Bhavana and I argued—not about large issues, but about small, silly things that become large when you are tired. A shelf height. A wall colour. A window grill pattern. The stress of construction has a way of shrinking your patience.
Jyoti was the calm in that storm. She would smile, hear both sides, and then say something like, “Relax. Trust the process.” It was hard to argue after that. She balanced our wishes with the demands of design, ensuring that the house served our needs without turning into an exhibition.
***
In 2009, after two years of dust, noise, and the constant anxiety of unfinished work, we finally moved in. Stepping into the new house felt like exhaling after holding my breath for years. It was spacious, cheerful, and—most importantly—ours. Not allotted, not borrowed, not conditional.
A home is not defined by walls. It is defined by what happens within them. And this home has been a blessed witness.
It saw the weddings of Ashwini and Amrita, when the rooms filled with relatives, music, and the kind of laughter that makes you forget fatigue. It welcomed the next generation—our granddaughters, Diti and Nivi—whose footsteps turned the house into something warmer than architecture. Every time I sit in the living room and watch sunlight filter through windows that Jyoti designed, I feel a quiet gratitude: to friends who built next to us, to Girish who drew the lines, and to Jyoti, who turned a concrete structure into a sanctuary.
Not a showpiece. A shelter. A home.
My First Heart Attack
For years, I watched heart disease from the safe side of the bedrail. In the wards and the ICU, it arrived in familiar disguises—tightness in the chest, sweat on the forehead, a look of fear patients tried hard to hide. I knew the protocols. I knew the drug doses. I knew the rhythm of urgency. I had taught residents how not to miss the silent infarct. Like most doctors, I carried a private illusion: that this story belonged to other people.
When I looked at myself through risk calculators, the numbers felt reassuring. Cardiologists have several tools to estimate a person’s ten-year risk of cardiovascular disease, and most placed me in a low-risk category. The Framingham Risk Score suggested that only a small proportion of people like me would develop a cardiac event over a decade. The INTERHEART study described nine risk factors that accounted for most heart attacks worldwide. I did not seem to fit that profile. I never felt invincible, but I did feel protected by probability.
Then, one afternoon, the body delivered its own verdict.
I was in the hospital when the pain began. It was not the vague discomfort that allows you to bargain with yourself—perhaps it is gas, perhaps it is fatigue, perhaps it will pass. This pain had a sharp authority. It made me sit up and pay attention. It did not give me the luxury of denial.
I remember a strange split inside me. One part tried to behave like a calm physician. The other part shrank into the frightened simplicity of a patient. I did what I often advise others to do: I sought help quickly.
The response was swift and almost automatic. Aspirin. Clopidogrel. Heparin. Atorvastatin. Drugs I had prescribed hundreds of times were now entering my bloodstream. My ECG showed no infarction. The echocardiogram showed no damage to the heart muscle. These were good signs, but they did not settle me. When you are lying on a bed and the pain is still fresh, “good signs” feel like thin blankets in a cold room.
My ICU colleagues consulted one another and decided I should be shifted to a cardiac hospital about fifty miles away. Their faces were calm, but I could read the seriousness behind the calm. In medicine, urgency often comes wrapped in politeness.
By the time I was wheeled into the cardiac catheterisation laboratory, I had stopped thinking like a professor of medicine. I was thinking like a man who wanted the pain to stop and wanted to go home alive.
Until that day, the cath lab had been a place I visited as an observer—curious, respectful, slightly awed. Now I entered it flat on my back, draped from neck to toes, surrounded by machines that beeped in their own language. The room was bright, sterile, and oddly intimate. You feel exposed and covered at the same time. You are present, and yet you feel as if events are happening to someone else.
The cardiologist chose my radial artery. I felt the sting, the pressure, and the unsettling sensation of something moving inside a vessel. The catheter was threaded towards my coronary arteries. Dye was injected, and on the screen my heart’s private highways appeared—branching lines I had studied for decades.
The cardiologist smiled. “Good, you have no calcium lining the walls of your coronaries,” he said.
A few seconds later he added, “Your left main coronary artery is perfect.”
For a moment, I wanted to believe the story would end there. I wanted to be told it was a false alarm. I wanted to go home and laugh at my own anxiety.
But the dye moved forward and met its obstacle. In the left anterior descending artery, a plaque had grown large enough to bulge into the lumen. It was not a dramatic, total blockage. Perhaps that was the cruel part. It was subtle enough to escape prediction, yet significant enough to cause pain. Like a rock in a stream, it slowed the flow beyond a point. The cause now had a face.
The cardiologist explained the plan to the anxious cluster of family, friends, and colleagues outside. He would do balloon angioplasty and place a stent to keep the artery open. Someone asked, hesitantly, whether medical therapy could be tried first and angioplasty kept as a backup.
It was a reasonable question. I would have respected it instantly if it had come from a patient’s family in my ICU. Hearing it asked on my behalf, I realised how fragile judgement becomes when the body is frightened.
The cardiologist did not dismiss the doubt. He answered gently. The obstruction, he said, was compromising blood flow. He would rather open it now. Then he waited for approval.
Everyone nodded. So did I.
That nod was not an academic decision. It was surrender. In that moment I was not practising evidence-based medicine. I was living the oldest form of medicine: trust. Trust in the person standing at my wrist. Trust in my colleagues who had brought me there. Trust in the collective sense that this was the right thing to do.
The stent was mounted on the balloon and advanced carefully. It was positioned precisely at the narrowed segment and expanded under pressure. The balloon was deflated and withdrawn, leaving behind a mesh that would now become part of my anatomy. When the dye was injected again, it flowed smoothly into the distal bed.
Somewhere in the waiting area, a collective breath was released.
I was wheeled into the ICU with a drug-eluting stent inside my coronary artery. Two days later, I was discharged home. I carried a prescription, a new label, and a quiet disbelief.
During those days, my phone did not stop ringing. Calls. Emails. Messages. Most were affectionate. Some were anxious. A few were teasing in the way only friends can tease after the danger has passed. One message stayed with me because it asked something I had never asked myself so honestly: “What kind of a patient are you? Obedient or full of questions? Compliant or sceptical?”
I understood why my colleague asked. For years, I had urged people to ask questions. I had spoken against unnecessary interventions. I had lectured on balancing evidence with values. I had believed that knowledge protects you from confusion.
The truth was uncomfortable. When I became the patient, my mind did not behave like the mind of a professor. It behaved like the mind of a human being who did not want to die.
The pace of events—rapid triage, quick transport, the urgency of treatment—created an environment where the ideal informed-consent conversation becomes difficult. I was aware of that even as it was happening. Awareness, however, did not translate into control. I found myself accepting decisions that were being made with my body at the centre.
I understood, in a way I had never fully understood before, why patients nod even when they do not grasp everything. It is not ignorance alone. It is fear. It is hope. It is the desperate wish that someone else will carry the burden of uncertainty.
***
After I returned home, some colleagues suggested further tests. If traditional risk factors had failed, they said, why not look for newer biomarkers? Their concern was genuine, and I was touched by their affection. But I chose not to pursue additional testing.
Part of that decision came from a simple realisation. Medicine, for all its power, is still imprecise. Risk prediction rules are useful, but they are not destiny. Diagnostic certainty is often a polite illusion. The body has its own grammar, and it does not always follow our neat algorithms.
What I carried back from that episode was not only a stent and a set of medicines. I carried back a change in the way I looked at patients. I began to see the trembling inside their calm faces. I began to respect the messiness of decision-making. It is not a clean mathematical act. It is emotional. It is influenced by family. It is shaped by prevailing practice. It is often steered by the tone of the doctor’s voice.
I also saw, with new clarity, the privileges of being a doctor-patient. I did not have to wait in a queue. I did not have to struggle for an appointment. Colleagues cut through delays on my behalf. I received care with speed, respect, and attention. Most patients do not get that. The thought stayed with me long after the chest pain faded.
When people ask me now what my first heart episode taught me, I do not talk about angiograms and stents. I talk about humility. I talk about how quickly a confident physician becomes an anxious patient. I talk about how medicine must remain evidence-based, yes, but also patient-based—rooted in the mind that is trying to make sense of fear.
And I remember Pascal’s line, which feels less like philosophy and more like clinical truth: the heart has its reasons which reason knows nothing of.
Letters From the First Time
In July 2012, I had my first heart attack. I have written about that night separately. This page is about what arrived in my inbox afterward — emails from former students, family friends, and colleagues spread across four continents, all saying versions of the same thing in entirely different ways.
Reading them together, I noticed something that I have been turning over since. Almost nobody wrote about the illness. They wrote about me — what they remembered, what they feared losing, what they wanted me to know while they had the occasion to say it. A heart attack, it turns out, is one of the few events that gives people permission to say what they ordinarily keep to themselves.
I am recording some of these letters here not because they reflect well on me — I am aware of how that reads — but because they reflect well on the people who wrote them. And because they taught me something about the practice of medicine that no textbook had managed to.
My brother-in-law Dr. Vipin Zamvar is a cardiac surgeon in Edinburgh. He wrote with the precision you would expect from a man who operates on hearts for a living. He noted that I would probably be on Clopidogrel for a long time. He expressed surprise — "a bit shocked" — and then relief. Then, in a postscript, he asked me to use my recovery time to answer a clinical question: how long should a patient remain on Clopidogrel?
This is what it means to have a cardiac surgeon in the family. The concern and the clinical quiz arrive in the same email.
His brother Dr. Deoraj Zamvar, also a physician in the UK, wrote about Clopidogrel resistance and platelet aggregation inhibition — useful, precise, and characteristic of a man who cannot help being a doctor even when writing to a relative.
Dr. Uma Zamvar, a physician in California, wrote more simply. She was glad I was doing well. She mentioned lemon-flavoured fish oil capsules — apparently they do not have the smell. She said Raju would be coming to India in December and asked if I needed anything brought from the US.
The fish oil capsule detail is the one I remember. It is exactly how family writes.
***
The letters from former students arrived from Edinburgh, Canberra, Abu Dhabi, Lucknow, Mumbai, California, and Australia. They were written by intensivists, oncologists, rheumatologists, radiotherapists, and pathologists. They had different degrees after their names and different time zones behind their clocks. They were all, in their own way, saying the same thing.
Dr. Manoj Singh, from the class of 1990, now an intensivist in Canberra, wrote: "You have been and will remain a guiding star to a lot of students like me and are always remembered in our daily lives." He wished that the heart attack was "just one bump on the road."
Dr. Nitin Chavan, from the 1989 batch, now in Mackay, Australia, said he could have called — but thought I deserved a break from answering what, why, when, how, where, and who. This made me smile. He knows his teacher.
Dr. Arvind Ghongane, from the 1979 batch, wrote to say he was receiving a fellowship from the Geriatric Society of India, that his oration topic was "Adding Life to Years," and that he owed his achievements to me and to Sevagram. He said this in a postscript, quietly, as if he did not want to make too much of it.
Dr. Ragu Krishnan, an ophthalmologist in Mumbai from the 1985 batch, wrote in Hindi and English together — Ishwar ki icchhaa aur hum sabki shubh-kaamnaayein aapke saath hain — and observed that my students must be missing "the heady cocktail of poetry and art" that I imparted to the teaching of medicine, "almost a taboo in the land of prohibition." Dr. Rajesh Ingole, from the same batch, remembered the bedside teaching — the murmurs through the stethoscope, the supranuclear and infranuclear facial nerve palsy — "in the same land of prohibition."
Two letters from the same batch, the same phrase, ten years after they had sat in the same ward. I had not known they remembered.
***
Dr. Nilima Ragavan, a paediatrician at Stanford, wrote something that has stayed with me. She said it must have been "quite educational to be on the other side" — to experience the hospital as a patient. She said she would be very interested to hear how I coped with it.
I have thought about this question since. The honest answer is: not as well as I thought I would. A doctor who becomes a patient discovers very quickly that clinical detachment is a professional habit, not a personal one. When the ECG is yours, the numbers stop being numbers.
Dr. VK Gupta, from the 1976 batch and a pathologist in Allahabad, wrote with characteristic wit. He said I had been "very cold and clinical" about a matter related to the heart, which showed that my brain dominates my heart. "Ha ha!" he added. He had been speaking to a mutual friend who, when asked what caused this in a man with no risk factors, replied in a sufiyana spirit: "Everything created by God has a use by date."
I found this more comforting than any medical explanation.
***
Dr. Sunil Jayaswal, an intensivist in Abu Dhabi from the 1987 batch, wrote while still on duty in the ICU during the night shift. He said he could not hold himself back when he read my email. He had not yet told his wife Maya the news.
He recommended green pumpkin juice — a glass twice daily — for reducing atheromatous plaques over six months to a year. I have not verified this in the literature. But the image of a former student, sitting in an ICU in Abu Dhabi at some late hour, writing to his old professor about pumpkin juice while the monitors beeped around him — that image I have kept.
***
Dr. Maureen Morgan was a classmate during my MPH at Berkeley. She is American, not Indian, and did not know me as a teacher. She wrote with the directness that Americans bring to affection: "It's clear that you are someone who adds so much to this world." She said she was imagining my stent staying clean and patent and my heart continuing "to beat vigorously with all of the passion that you have for life."
I have had many cardiologists say reassuring things about my stent. None of them mentioned passion.
Dr. Sadhana Bose, from the 1985 batch, a public health professional in the UK, wrote that she had noticed during her last visit to Sevagram that I looked tired and worn out — "your poor heart was working extra hard without you realising it." She suggested pranayam. She also noted that angioplasty "is almost like an OPD procedure nowadays," which is exactly the kind of thing one doctor says to another when they are trying to be comforting and cannot quite stop being clinical.
***
Dr. Amit Bhatt, an oncologist from the 1997 batch, pointed me toward two books — one about Dr. Nitu Mandke's heart attack, and Majha Sakshatkari Hridayrog by Dr. Abhay Bang. He noticed I had posted birthday wishes on Facebook for mutual friends and correctly deduced I was recovering well. "PA is home," he wrote, using the abbreviation that students use.
Dr. Amulya Kulkarni, a psychiatrist in the UK from the 1982 batch, observed that it is "better to receive a warning from the heart rather than be surprised by a MI." He was impressed that I had texted Dr. Dilip Gupta at 6 AM about the successful angioplasty and then emailed everyone about the good news.
I did not think about that at the time. But reading it now, I think it says something true: that the first instinct, even after a night in the ICCU, was to tell people. Not because the news was good — though it was — but because the people were waiting.
These letters are why.
Republic day, Redux
Sevagram in January wakes up slowly. The air stays crisp even after sunrise, and the mornings feel quieter than they should. I woke at five, more out of habit than necessity, and sat down at my desk. Ashwini had reached Nagpur barely an hour earlier; his late-night flight from Pune had been delayed and finally landed at 3:30 a.m. By the time he got home, dawn was already softening the darkness.
I opened the news on my desktop, scrolling through the headlines with the calm attention of a man who had no reason to hurry. The Padma awards had been announced. I read the list casually until one name made me pause—Dr. Chandrashekhar Meshram, a neurologist from Nagpur and my classmate from GMC. The Padma Shri felt perfectly placed. It gave me the quiet satisfaction one feels when a good man is recognized without noise.
I called him immediately. The hour did not matter.
“SP!” he exclaimed, startled, as if the phone itself had delivered the award.
“Congratulations, Chandrashekhar,” I said. “The Padma Shri—well deserved.”
He laughed, still trying to make sense of it. We spoke for a few minutes, drifting into old teachers, old wards, and the long, uneven roads we had all travelled since 1973. When I hung up, I opened WhatsApp to share the news with our GMC Class of 1973 group.
That was when I felt it.
It did not arrive like a thunderclap. There was no cinematic clutching of the chest, no dramatic collapse, no warning siren. It came as a deep, dull discomfort that settled in the centre of my chest and stayed there, firm and unmoving. I stood up, walked a little, took a breath, lay down. The sensation remained. It was not sharp, but it was unyielding. It had the unmistakable stubbornness of something serious.
I woke Bhavana gently and told her we needed to go to the hospital. She looked at me closely, reading my face the way only a spouse can.
“Do you want to change into a formal shirt?” she asked.
For forty years, regardless of the hour or the destination, Bhavana had ensured I was presented to the world in a crisp shirt and well-pressed trousers. It was her signature act of care, a well-conditioned reflex that had never failed, and even on this morning, it remained her first line of defense against chaos. She asked as if the simple dignity of a formal shirt could somehow restore order to an unruly heart.
I shook my head. “Just get the car,” I said. “We need to move quickly.”
The realization that I was refusing the ritual—that we were leaving in whatever I had on—signaled the gravity of the moment more than the pain itself. She did not ask again. Ashwini was downstairs within moments. There was no panic in the house, only a brisk, silent efficiency that felt like muscle memory. Soon we were driving towards Sevagram Hospital, the familiar road suddenly sharper, as if the tyres were cutting through a different kind of air.
I had felt something like this once before, eleven years ago. That episode too had begun subtly, easy to dismiss, easy to rationalise. The angiogram then had revealed a severe blockage, and a stent had been placed in my left anterior descending (LAD) artery. This time, there was no ambiguity. The body was speaking a language I understood too well.
At the hospital gate there was no wheelchair. I did not wait. I walked up the ramp and straight into the ICU on the first floor. The residents looked up, momentarily confused. They assumed I had come to review a patient, perhaps to ask for an ABG, perhaps to scold someone gently about a delayed antibiotic.
I sat down at the nursing counter and said, calmly, that I was having chest pain and needed an ECG.
There was a brief hesitation. No beds were available. Someone suggested waiting. I shook my head and asked them to take me to the preparatory beds outside the cath lab and do the ECG there. When your own heart is misbehaving, you stop being polite about logistics.
The ECG confirmed what I already knew: early changes of an acute myocardial infarction. My coronary artery was blocked; my heart muscle was starving for blood. The resident holding the paper seemed to freeze for a second. She had seen heart attacks before. She had treated them. But she had never treated this one. This patient was her professor.
The pain intensified. Sweat began to pour down my forehead and soak through my shirt. Bhavana held my hand and stared at me with a mixture of worry and irritation—the irritation reserved for situations where fear has no other outlet.
“Why are you sweating so much?” she asked. “It’s January, and the ICU is air-conditioned.”
I knew the answer, but I had no strength to explain it. The body had turned into a furnace, and the mind had narrowed to a single point: endure.
For a few moments, uncertainty hung in the air. The residents hesitated, caught between protocol and urgency. Then the ICU male nurse stepped forward. He did not look confused. He looked calm, almost stern, as if he had decided that the heart could misbehave but the team would not. He gave aspirin, statins, anticoagulants—swiftly, without fuss. The room found its rhythm again.
Dr. Sumedh Jajoo arrived soon after and took charge instantly. The atmosphere changed the way it changes when a senior clinician walks in—less talking, more action. He ordered that I be shifted to the main cardiac ICU. The hesitation vanished. Decisions became crisp. The chaos, if there was any, moved out of the room.
I said, “Give reteplase.”
It was not a command from a professor. It was the desperate clarity of a patient who knew what minutes meant.
IV lines were secured, monitors began their steady beeping, and the clot-busting drug went in—one dose, then another ten minutes later. I glanced at the clock. Barely thirty minutes had passed since the onset of pain. The speed startled me even in that moment. Nowhere else could I have received treatment faster—not because of privilege, but because of proximity and familiarity. The hospital was two minutes away. The team knew me. There were no formalities to slow us down.
Yet the pain did not subside immediately. My blood pressure rose. Sweat pooled on my back. A resident listened to my chest and paused briefly, then continued as if her stethoscope was also trying to stay calm. Later she told me she had closed her eyes for a second and prayed.
I asked Ashwini to call Diti and Nivi. They arrived with Shaily—eleven and eight years old—standing quietly at the foot of the bed. Children, when frightened, become suddenly adult in their silence. They looked at the wires, the monitors, the unfamiliar stillness of their grandfather, and tried to make sense of it.
Then, without warning, the pain vanished.
Not gradually. Not in steps. It disappeared completely, as if someone had switched it off. The clot-buster had worked. The artery had opened. Blood flowed back into the heart muscle, and relief spread through the room like a soft exhale. I smiled. Bhavana squeezed my hand. The nurses exchanged glances that said, Yes, it has happened. We have crossed the worst part. The air felt lighter. I had made it through the first gate.
The rest of the day passed under vigilant care. Gini, the senior ICU nurse, took charge the way experienced nurses do—quietly, firmly, without drama. She had spent more than two decades in the ICU and shared a special bond with me. She kept visitors at bay, protected my rest, and ensured that the vigilance around me stayed unbroken.
My residents sat by my bedside, watching the monitors with an intensity that reflected both concern and familiarity. They were used to seeing me on the other side—walking, teaching, questioning. Now they watched my heart rate the way students watch a difficult viva: afraid of missing a sign, afraid of being wrong.
Amrita, seven months pregnant, was in Chandigarh when she received the news. She asked for my ECG to be sent to her father-in-law, Dr. Rajiv Rathi, a cardiologist at Max Hospital in Delhi. His response came quickly: the treatment was appropriate and timely. By midnight, to everyone’s surprise, he arrived in Sevagram. Some people show love not through words but through the sheer refusal to stay away.
The next morning, Ashwini drove Bhavana, Dr. Rathi, Dr. Sumedh, and me to Dr. Pramod Mundra’s cardiac hospital in Nagpur. The ninety-minute drive passed quietly. The road was familiar, but the silence inside the car felt different, as if all of us were listening for something that might go wrong again.
Dr. Mundra was ready. A decade earlier, he had placed my first stent and knew my heart well. The timing could not have been worse—his daughter’s wedding reception was scheduled the next day—yet he stepped away without hesitation. In medicine, the best people often disappoint their families to keep someone else’s family intact.
In the cath lab, the angiogram revealed a total occlusion of the LAD just above the previous stent, and significant disease in the circumflex artery. The images were stark, almost insulting. The heart had been quietly building its own problem while I was busy reading newspapers and making congratulatory calls.
Two new stents were placed. The procedure went smoothly. When it was over, Dr. Mundra smiled and said simply that my heart was pumping beautifully. It was not a poetic sentence, but it felt like poetry to me.
Two days later, I walked out of the hospital and returned home—alive, and quietly grateful in a way that did not need to be announced.
A week later, I walked back into the ICU, this time as a physician. My residents looked up, startled, as if they were seeing a ghost who had come back with a stethoscope. I told them I had resumed my routine, including cycling. One of them smiled, visibly relieved, as if my return restored a sense of normalcy in their world too.
That night, I wrote thank-you emails to Dr. Mundra and the ICU team. Some experiences leave you with no choice but gratitude—and the responsibility to acknowledge it.
Acknowledgements: The Hands that Held the Line
Survival is rarely a solo act. As a physician, I have spent decades on the right side of the stethoscope, but on that Republic Day, I was reminded of the vulnerability that defines the patient. This chapter reached its conclusion only because of a specific constellation of people who moved with quiet speed when the world went dark.
To Bhavana, who has stood by me through four decades of shared life and understood the rhythm of my heart long before the monitors began to beep. That morning, she did not need the confirmation of an ECG; she looked at me and simply knew. For forty years, she has been the silent architect of my stability, and in that hour of crisis, her presence was the only anchor that mattered. She has lived every beat of this journey with me.
To the ICU Team at Sevagram, specifically the residents who managed to look past their professor to see the patient, and the senior ICU nurse, Gini, whose twenty years of muscle memory provided a fortress of vigilance around my bed. To Shrikant, the male nurse who moved without hesitation when the room was suspended in doubt: you are the reason the "Golden Hour" remained golden.
To Dr. Sumedh Jajoo, whose arrival transformed chaos into clinical rhythm. In a profession often paralyzed by hierarchy, your ability to take charge with such crisp, unblinking authority saved more than just minutes—it saved a life.
To Dr. Rajiv Rathi, who proved that love is measured in miles traveled. Your refusal to stay away and your midnight arrival from Chandigarh remains a memory of profound comfort.
To Dr. Pramod Mundra, who, despite his daughter’s wedding reception being scheduled for the very next day, came straight to the cath lab to open my coronaries for the second time in a decade. You told me my heart was "pumping beautifully," and in that moment, no poet could have said it better.
I owe my return to the wards and my bicycle to these hands. Gratitude, I have learned, is not just a feeling; it is a heavy responsibility to acknowledge that we are all, at some point, at the mercy of each other’s competence and care.
Letters After the Heart Attack
On January 26, 2023, I was admitted to the MGIMS ICCU with a heart attack. The details of that night — the ECG, the thrombolysis, the second dose of reteplase, the moment the pain finally lifted — I have written about separately, in "The Republic Day, Redux." This page is about what came after.
When you survive something like that, people write to you. Not the polite, obligatory letters that institutions produce for retirements and farewells. Something rawer. Something that people normally keep to themselves because there is no occasion to say it — until suddenly there is.
I received dozens of emails. From former students in Liverpool and Memphis. From a Harvard professor who once sat in my ward. From a staff nurse who said the news was "indigestible." From a medicine resident who told me she had closed her eyes and prayed while I lay on the table, and that within a minute, my pain had subsided.
I did not know what to do with these letters at first. I still do not, entirely. But I know they deserve a page.
***
Dr. Shifa Guhagarkar was the resident on duty when I walked into the ICCU complaining of chest pain on the morning of January 26. She later wrote to me with an honesty that I found remarkable in someone she described as "the smallest right now in the profession."
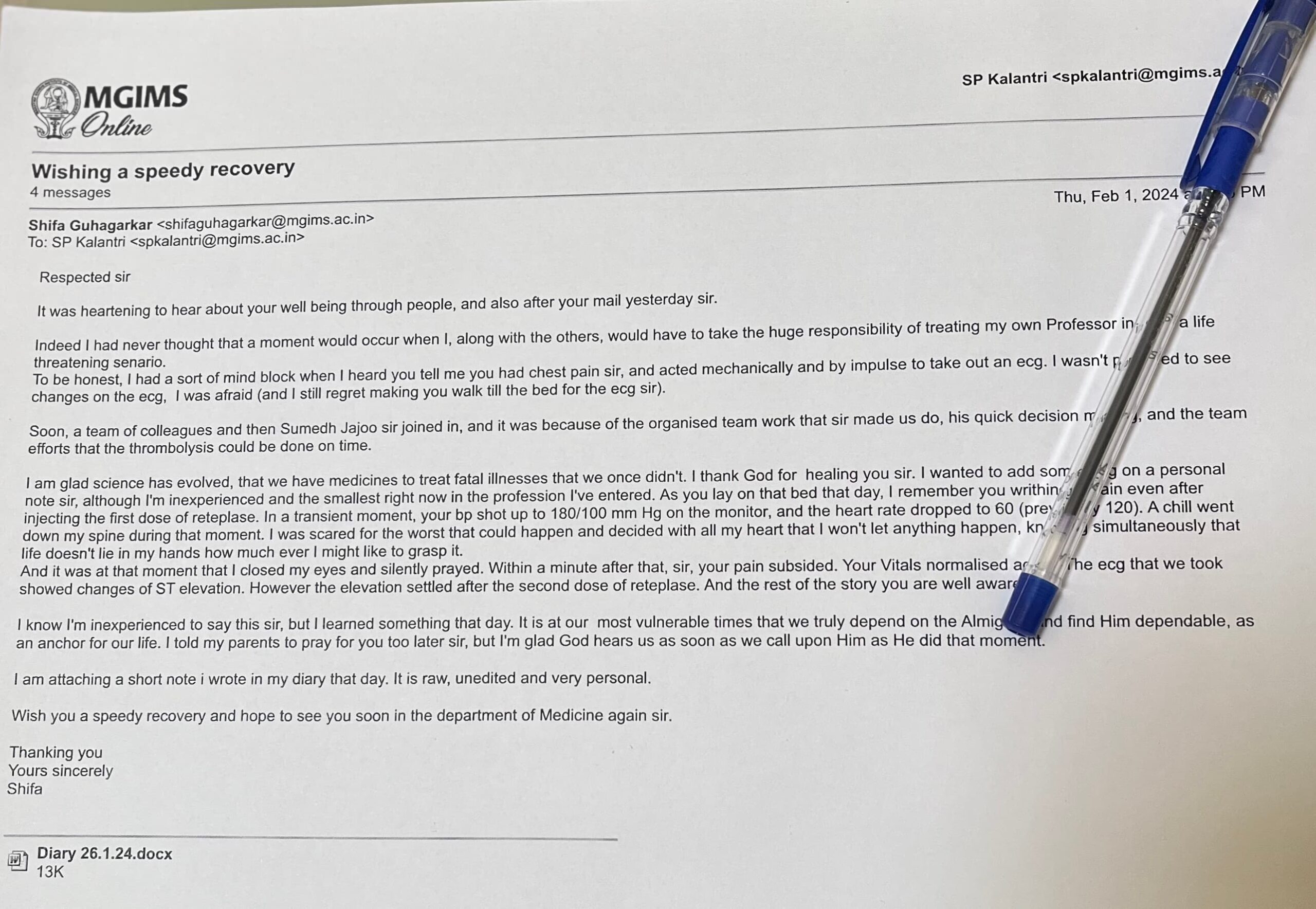
She wrote that she had a mind block when I told her I had chest pain. That she acted mechanically, by impulse, reaching for the ECG without thinking. That she regretted making me walk to the bed for it.
She described the moment when my blood pressure shot to 180/100 and my heart rate dropped to 60. "A chill went down my spine," she wrote. "I was scared for the worst."
And then: "I closed my eyes and silently prayed. Within a minute after that, sir, your pain subsided."
I have taught medicine for forty years. I have taught residents to examine evidence, to trust data, to follow the science. Dr. Shifa did all of that with calm efficiency on a morning when her teacher was the patient. And then, when the science had done what it could, she prayed.
I do not think those two things are in conflict. I have lived long enough to know they are not.
***
Ms. Nandini Patil works in the registration OPD of the Medicine department. She is not an alumnus. She has no publications. She wrote to me in the simplest English I received, and it was the most direct.
"The news is really indigestible that you are leaving."
She was not writing about the heart attack specifically. She was writing about the years before it — the times she had come to me with a sad face and left with a smile. "You will never leave our hearts," she wrote. "Hats off to your work sir you have another level of potential in you."
I have received letters from professors at Harvard and consultants in London. None of them landed quite the way Nandini's did.
***
The emails from former students followed a pattern I had not anticipated. Most of them did not dwell on the illness. They wrote instead about what they remembered — which told me more about what had mattered than anything I could have concluded myself.
Dr. Iada, from the 2001 batch, now at NEIGRIHMS Shillong, wrote that she still proudly tells people that her institute — the first rural medical college in India — has had a Hospital Information System since 2005 and went paperless in 2012. She remembers the clinical lectures. "Making the lectures so simple and putting everyone's brains into action in a very calm atmosphere."
Dr. Rishi Adhikary, from the 2006 batch, wrote something that I have read more than once. He said that if he were to make a slide deck of his life story, the introductory slide would carry the quote "It's not the destination, it's the journey" — with Ralph Waldo Emerson's name crossed out and mine written in its place.
I do not know what to do with a sentence like that either. I am recording it here because it happened.
Dr. Amulya Nadkarni, from the 1982 batch, had visited MGIMS recently and written with the eye of someone seeing the place after years away. He said the Institute was lucky to have me at the helm for twelve years. Then he added, almost as an afterthought: "The most controversial may have been the management of the pharmacy, but I hope that the Institute has the sense to persist with it, even if it isn't exactly beneficial for the bottom line."
That sentence pleased me more than the praise. He understood what the pharmacy policy was about — and why it mattered.
***
Dr. Mandeep Mehra holds the William Harvey Distinguished Chair in Advanced Cardiovascular Medicine at Harvard. He was once a student in Sevagram. He wrote that my legacy is "forever etched in the institutional fabric" of MGIMS — which is the kind of sentence that Harvard produces with ease.
But then he wrote something simpler: "You will now bring the talent of your experiences woven into the cloth of your exquisite expression to us all."
Dr. Thillainayagam Muthukumar, from the 1985 batch, a radiologist in the UK who told me he has no social media presence, wrote that he remembers me as a teacher who showed him that the role of a doctor is "a role of love and service." He said fresh vistas await. "Get the boots mended and ready for new adventures."
Dr. Ram Prakash, from the 1987 batch, now a consultant endocrinologist near Liverpool, wrote warmly and mentioned his nine-year-old son Rishi who loves art and writing, and his three-year-old daughter Reva who ensures every ounce of attention is directed at her. He invited me to visit. These are the details that stay.
Dr. Sanjay Pai, pathologist and head of department at Manipal Hospital Bangalore, wrote in the register I appreciated most: brief, precise, and ending with a PS about Ramanujam and cricket analogies that made me smile. "You are a test cricketer, not a T20 tamasha man."
He is right. I have always preferred the long game.
***
Sister Gini is an ICCU staff nurse. She wrote after the heart attack with a warmth that carried no professional distance at all.
"God is great," she wrote. "You reached ICCU on the 26th morning at the right time. So, you were able to get the right treatment at the right time by the right people. It made a great difference in your recovery. It was a miracle of God's love lavished on you through a competent team spirit of compassionate care."
I spent thirty years teaching my residents to be precise about causation. Sister Gini attributed my recovery to God, to competent teamwork, and to the right time — in the same sentence, without contradiction.
She may be right about all three.
***
Dr. Yogesh Kolkande, a former student, wrote the most philosophical letter. He read my farewell note multiple times, he said, "to understand how a wise man like you navigates life." He wrote about the rate of change of change, and the question of when to hang up one's boots, and the need to rediscover oneself every second of life.
I am not sure I am the wise man he describes. But I know what these letters, taken together, told me.
They told me that people remember the small things — a calm lecture, a sad face made to smile, a corridor conversation about a child's chest pain. They told me that the pharmacy policy mattered to people who understood what it was trying to do. They told me that a resident prayed at my bedside, and that a nurse in the OPD found the news indigestible, and that a pathologist in Bangalore compared me to a test cricketer — and meant it as the highest compliment.
I received these letters because I had a heart attack on Republic Day and survived it.
I am glad I survived it. Partly because of the ECG, the reteplase, and the angioplasty the next morning. Partly, perhaps, because Dr. Shifa closed her eyes for a moment and asked for help.
And partly because I had not yet written any of this down.
When the Soul Slipped Away
By January 2026, medical education in India had expanded beyond anything my generation could have imagined. The National Medical Commission had pressed hard on the accelerator. New colleges kept appearing on the map, approvals came in quick succession, and the country now had hundreds of medical colleges and well over a lakh MBBS seats. The numbers looked impressive—like a nation announcing, with pride, that it had built enough runways for the future.
Around the same time, I stepped down from the administrator’s chair and returned fully to the department. For years I had worn two hats—Medical Superintendent and Professor—and each day had demanded a different version of me. Now I wore only one. It should have felt like relief. In many ways it did. But it also gave me a clearer view of something I had sensed for a while: while the numbers had grown, the soul of the profession had quietly thinned.
The shift, of course, did not begin in 2026. It had begun much earlier, and like many large changes in India, it arrived under the banner of reform. In 2013, NEET—the National Eligibility cum Entrance Test—entered our lives. A single national entrance examination replaced the patchwork of state and institutional tests. On paper, it sounded fair and clean. One exam, one merit list, one rulebook for everyone.
But MGIMS was not like everyone else.
For four decades, MGIMS had marched to a different drummer, not out of arrogance, but out of conviction. We ran our own admission test. We included a paper on Gandhian thought. We wanted students who were not only academically capable, but also temperamentally aligned with the idea of rural service. We insisted on proximity to villages. We sent our postgraduates to village health centres for two years, not as punishment, but as training in reality. We offered our undergraduates a near-assured path to postgraduation within the institute, creating a closed and nurturing ecosystem that produced a certain kind of doctor—clinically sound, socially aware, and less dazzled by the glamour of urban medicine.
That ecosystem cracked in 2013.
The institute fought hard to retain its autonomy, even taking the matter to the Supreme Court, but we lost. The judgement was final. The old rules dissolved overnight, and the new ones arrived with the confidence of a policy that believes uniformity is the same as justice.
I often wondered what Dr Sushila Nayar would have felt if she had lived to see this. She had built MGIMS with a moral blueprint, not merely an administrative one. The new “merit-only” system—devoid of values, aptitude, or rural commitment—felt antithetical to the code she had woven into the institution’s DNA. There were days when I thought she might have preferred to close the gates rather than watch MGIMS become just another medical college on a long national list.
The casualties of the change were not abstract. They were immediate, personal, and painfully visible.
***
For years, a ward quota gave faculty members a sense of stability. If their children were qualified, they had a place at MGIMS. It was not charity; it was an anchor. It kept good surgeons and physicians in Sevagram when they could easily have moved to bigger cities with bigger pay and brighter lights. They stayed because their children’s education mattered, and because MGIMS, in return, offered them belonging. When NEET stripped that away, the glue that held many faculty members to Sevagram weakened. Recruitment became harder. Retention became harder still. The institution did not collapse, but the slow drift began.
***
Earlier, our undergraduates knew that if they worked well and served the system, the system would nurture them through postgraduate training. It was not an entitlement; it was a relationship. NEET broke that relationship. Suddenly, our students were thrown into a national pool with nearly two million competitors, uncertain not only about branch and college, but sometimes even about which state they might land in. Anxiety became the new normal. Gratitude became a luxury.
The students adapted quickly. Young people always do.
Their focus shifted from the patient to the paper. Why spend hours at the bedside learning the nuance of a murmur when the exam would not ask for nuance? Why attend long lectures on compassion when compassion carried no marks? Why go to villages when villages did not improve rank? Slowly, without any villain in sight, the art of medicine began to get traded for the mechanics of multiple-choice questions.
Coaching centres mushroomed. Online apps became the new teachers. The professor, once a mentor and model, became an optional extra. The clinical ward—once the beating heart of medical education—began to feel like a place students visited out of obligation, not curiosity. They still worked hard, but their hard work was aimed at cracking an exam, not understanding a patient.
What unsettled me most was the quiet breakdown of the teacher–student relationship.
For years, I had been an unofficial custodian of the MGIMS family tree. I knew thirty-five batches—nearly two thousand students—by their first names. I knew their backgrounds, their quirks, their ambitions, their parents’ illnesses, their marriages, their children. I had built a database with the stubbornness of a man who feared that memory, left unattended, would decay. Alumni often called me for a classmate’s number, a job reference, a word of advice, or sometimes simply a voice that reminded them of Sevagram.
I still remember June 2014. Dr Manoj Singh, a critical care specialist in Australia, landed in Nagpur. I had sent him a simple invitation for my daughter Amrita’s wedding. He had no conference to attend, no professional agenda, no work excuse. He flew across the ocean simply to be there. That kind of loyalty does not come from institutional branding. It comes from relationships built slowly, over years, in classrooms, wards, and shared meals.
That era, I realised, had passed.
With the MD Medicine intake increasing to twelve postgraduates a year, the department was busier than ever. The corridors were crowded. The ICU was full. The academic calendar was packed. And yet, oddly, I began to feel a kind of anonymity. I no longer knew the new residents well—where they came from, what shaped them, what frightened them, what they secretly dreamed of becoming. They were polite, competent, and efficient, but distant. The old warmth had cooled. The days of students coming home for a meal, asking for Bhavana’s cooking, lingering in conversation, and sharing their lives without a deadline—those days had quietly slipped away.
Perhaps this is what happens when systems scale up. Intimacy becomes the first casualty.
Tennyson wrote, “The old order changeth, yielding place to new.” I had quoted it often in speeches, but now I felt it in my bones. The river had changed its course, and standing on the bank with nostalgia would only make me bitter. I had to accept that the world my teachers gave me could not be recreated exactly for my students, and that the new generation would build its own version of medicine—different, faster, more digital, perhaps less human in the old ways, but not necessarily less sincere.
So I stopped looking back as often as I used to. I began to look inward instead, searching for small anchors—habits, friendships, hobbies—that could keep me steady in a changing world.
That, however, belonged to another page of my life.
The Final Prescription
I had spent four decades in medicine, long enough to see how death arrives in different disguises. Sometimes quietly, like a lamp going out at the end of a long evening. More often, dressed in tubes and monitors, escorted by alarms, surrounded by machines that keep a body going long after the person inside has begun to slip away.
I had worked in emergency rooms, ICUs, and medical wards. I had watched patients recover in ways that felt close to miraculous. I had also watched families cling to hope with the desperation of people clutching a floating twig — and I understood why. It was not cruelty. It was fear. Fear of regret, fear of judgment, fear of the sentence families whisper to themselves at funerals: we should have done more.
That sentence has destroyed more peace than disease ever did.
Over the years, something began to trouble me more than death itself: the way we so often refuse to let it be natural. Frail old men with skin like parchment, ribs cracking under CPR. Women who had lived full lives lying sedated, restrained, and ventilated, while their children hovered outside the ICU signing consent forms they did not fully understand and would never entirely forgive themselves for.
I decided I did not want my own ending to become such a spectacle.
***
One evening — not during an illness, not in a hospital corridor, but at home, when life was ordinary and calm — I asked Bhavana, Ashwini, Amrita, and Shaily to sit with me.
There was no drama in my voice. I was not announcing bad news. I was simply doing what doctors rarely do for themselves: planning ahead.
Bhavana looked at me with the quiet alertness she has developed over the years — the look that says she is listening not just to words but to what lies behind them. Ashwini and Amrita, both doctors, understood immediately where this was going. Shaily sat beside them, steady and attentive.
I told them I wanted to speak about the kind of care I would want if I could no longer speak for myself. Not in theory. Not in a vague "do your best" way. In clear terms that would protect them from doubt later.
I was not afraid of death. What I feared was leaving them with confusion — forcing them to guess, in the middle of panic and grief, what I would have wanted. Families do not only lose a person in the ICU. They lose their certainty. They keep asking: should we try one more thing? Should we wait one more day? What if he would have wanted this?
I wanted to spare them that torment.
***
I explained it simply.
If I had a condition from which meaningful recovery was not possible — if the body was being kept alive while the person I was had already slipped away — I did not want aggressive life-prolonging interventions.
I did not want my breathing handed to a machine if my lungs could not sustain me and there was no real chance of returning to an independent life. I did not want my ribs broken in the name of resuscitation if my heart had truly reached its end. I did not want artificial feeding forced into a body that could no longer swallow — not as nourishment, but as a ritual of postponement.
What I did want was comfort. Clean sheets. Relief from pain. A calm room. Familiar voices. A hand to hold.
I wanted the kind of care that does not fight death like an enemy but receives it as something that has arrived, uninvited but not unexpected, and cannot be turned away.
And if it was possible, I wanted to be at home.
Hospitals are excellent for saving lives. They are not always kind places to die.
***
When I finished, there was a silence at the table. Not the awkward kind — the quiet that comes when something truthful has been said and allowed to settle.
Bhavana nodded. She had seen enough with me to understand. She knew the cases that came home with me in the evenings — the ones where families could not let go, doctors could not say no, and patients remained trapped between the two.
Ashwini and Amrita understood it not only as children but as clinicians. They knew that a good death is not a poetic phrase. It is a practical mercy. Shaily's eyes held the same acceptance, the same steadiness.
No one said, "Don't talk like this." Instead, there was a quiet agreement — as if we had collectively decided to protect one another from a future storm.
That evening I felt lighter. Not because I had invited death into the room. Because I had taken fear out of it.
***
A living will is not a morbid document. It is an act of tenderness — what you leave behind for the people who love you. Not money, not property, but clarity.
We spend our lives writing prescriptions for others. This was the last one I wrote for myself.
Life is not something we own. It is something we are allowed to hold for a while. When the time comes to return it, I hope to do so with grace and a quiet namaste.
What the Ward Taught Me
A ward is not a place most people choose to enter. They come because they have run out of other options — because the surgery has been done, the chemotherapy endured, and the body has begun to say, quietly and without negotiation, that it is tired. The palliative care ward of the Department of Medicine at MGIMS Sevagram receives people in this condition every day. They come from small towns and smaller villages. They travel on buses, in auto-rickshaws, on the backs of motorcycles. They arrive with a diagnosis in a brown envelope and a family member who has taken leave from work to be there. Most are poor. Many are frightened. All of them are still, in every way that matters, human beings.
I have been caring for these patients for years, and I have been writing about some of them — their names changed, their dignity preserved — because I believe their stories deserve to be told. Not as case studies. Not as evidence. As lives.
***
When Dr Sankha Mitra, an oncologist, visited Sevagram some years ago, he said something that has stayed with me. In India, he observed, the poor die in agony in neglect, the middle class die in agony in ignorance, and the rich die in agony on a ventilator. Nobody, he meant, gets a dignified death. Fewer than one percent of those who need palliative care in India can access it. The country ranks among the worst places in the world to die — not because we lack doctors, but because we have never taught them, or ourselves, how to sit with dying.
This is what the palliative care unit at Sevagram tries, imperfectly and daily, to change. The ward has trained nurses. It has resident doctors who have written their MD theses on caregivers. It has a small stock of oral morphine. It has, above all, a conviction that the patient who cannot be cured still deserves to be cared for — that ease and dignity and company are not lesser forms of medicine but its very essence.
***
One evening, a man called me on the phone. He was in his late seventies, a cancer patient I had known for years. We talked about the cricket, his niece's wedding, the cold weather. Then, out of nowhere, he asked: How much time do I have?
It is the question every doctor fears and every patient deserves an answer to. We were not taught, in medical college, how to answer it. We were not taught to sit with the silence that follows. I gave him a number. He laughed — not from despair, but from relief. He told me he was tired. That he did not want more fighting. That he wanted peace. He knew nothing of living wills or advance directives, but he had arrived, through suffering, at the same wisdom.
The truth, I told him eventually, is that I did not really know. He laughed again. "So you were lying earlier," he said. "Now you're being honest." He was right on both counts.
***
A twenty-three-year-old man came to us with a brain tumour so large that three neurosurgeons, each experienced and senior, declined to operate. He arrived in the palliative ward barely able to speak, unable to swallow or move his left side. His family cycled through grief the way all families do — denial, anger, bargaining, a slow and painful acceptance. One morning, his father took me aside and asked if he could take the boy to a healer in rural Rajasthan, a man said to cure cancer with sacred ash and a thread on the wrist, on the condition that all modern medicines be stopped.
Years ago, I would have said no. I would have been categorical and, I think, wrong. I told him they could go. Try not to stop the seizure medicines, I said. But follow whatever else the baba advises. The father's eyes filled with relief. He needed permission to love his son in the only way he had left. Sometimes, the greatest medicine is the understanding we extend — a touch, a word, a bridge between worlds. Doctors are not the keepers of all meaning. We are only one voice in a conversation that families have been having, in their own language, for centuries.
***
A woman came from a village three hours away by bus. She was sixty, frail, and widowed. She had raised her son alone, through years of farming and firewood and labour. The cancer in her breast had spread to her liver, her lungs, her spine. No surgery, no chemotherapy, no radiation could help.
Her son brought her to the palliative ward. He had been sleeping on benches outside wards for days. Here, for the first time, there was a caregiver's bed beside hers. He lay down and slept. After three days, he came to me and asked if he could take her home. Not because she was better. Because she was dying, and the elders of the family were too old to travel, and they wanted to see her one last time. We waited until she was stable enough for the journey. Then we let her go.
Her illness was not only cancer. It was poverty, exhaustion, fear, and the weight of a system that could ease her pain but could not lift the burden of her circumstances. Palliative care felt, that day, like an imperfect science. But perhaps all we can offer, sometimes, is a fragile and deeply human space where families can say goodbye in their own way.
***
Pandurang is seventy-three years old, a daily-wage labourer from a village near Hinganghat. He never went beyond primary school. His wife, who weighs twenty-four kilograms, lies in the palliative ward with oesophageal cancer. He has walked the Pandharpur wari thirteen times — hundreds of miles each pilgrimage, always with her beside him. Now he feeds her through a tube, turns her in bed, massages her feet, sits awake through the night.
During rounds one morning, as we began to explain her condition, he interrupted us gently. "This is not in your hands," he said. "Nor mine. He decides when we come and when we go." His wife, her voice faint but clear, added: "I am not afraid of dying." She had a feeding tube. She could not swallow. And she was not afraid.
Pandurang has never read the Bhagavad Gita, but he lives its wisdom. He bowed to no one that morning. But I bowed, quietly, to him.
***
She arrived with a colostomy bag at her waist and a full laugh that silenced the monitors. Cancer had taken her cervix and colon and was looking for more. She had been an Anganwadi worker all her life — feeding children, vaccinating them, teaching mothers. She had endured chemotherapy and radiation and the burning of veins and the loss of her old life in the city.
What kept her going, she said, was hope. And food. She described, with the pleasure of a chef and the authority of a woman who has fed many people, the jowar bhakris she would cook on her chullah at home, the gharit mashed with onion and green chillies and mustard oil, the fresh green onions straight from the field. "Just give me strength," she told us. "Let me shame the cooks in five-star hotels." We laughed. She was not joking. For her, food was not nostalgia. It was resistance.
***
Shankar shut his welding workshop the day Lakshmi's cancer was confirmed. He spent money he did not have, at hospitals in Nagpur, waiting for a different answer. The answer was always the same. He became her nurse, her shadow, her whole world. He bathed her, dressed her, changed her diapers, cleaned her wounds, fed her through a tube. He never complained. He only asked: what more can we do?
In the palliative ward, away from the ICU's machines, the morphine eased her pain, the nurses spoke to her gently, and in the quiet hours of an early morning, Lakshmi died with Shankar's hand in hers. He had not slept for days.
Who looks after the caregiver? Two of my residents have written their MD theses on precisely this — the burden, the invisibility, the cost of devotion. Society calls it duty. We have begun to call it, more honestly, sacrifice.
***
Neha is in her second year of engineering college. She has been coming to this hospital for four years, accompanying her mother Pramila through twenty-five rounds of radiotherapy, three cycles of brachytherapy, and several lines of chemotherapy. Her brothers are unemployed. Her father, a mason, cannot bear the smell of hospitals. So Neha comes. She has come, she says, hundreds of times.
Pramila now has bone metastases and is on oral morphine. She does not want false hope. She wants her pain managed, her daughter allowed to sleep, her remaining time spent in peace. In the ward, pain and love live side by side — one growing, the other refusing to diminish.
***
She was thirty-three, from a village forty-five kilometres from Sevagram, and she put everyone else's illness before her own for so long that by the time she came back to us, the cancer had taken both lungs, the liver, the spine, the pelvis. For six months between diagnosis and return, she had cooked and cleaned and ferried her father-in-law — who was dying of alcoholic liver disease — back and forth to this same hospital on a scooter, three of them on it together, forty kilometres each way. She thought her own lump would go away. She thought her illness was less serious than theirs. Nobody told her the treatment could be free.
When she finally came back, coughing, unable to breathe, barely able to sit — the surgeon's file noted one word against her name: defaulter. Nobody had asked why she left. Nobody had followed up. Nobody had told her she mattered.
We washed her, placed her by the window, drained a litre of fluid from her chest, started her on morphine. For the first time in months, she said she felt human. "I am overwhelmed to see such kindness," she whispered.
We were the ones who felt the weight of that sentence.
***
These stories are not exceptional. They repeat themselves, with different names and different cancers and different families, every week in our ward. What they share is this: behind every dying patient is someone who has been carrying them, often in silence, often at enormous cost to themselves. And behind the silence, almost always, is a love that medicine did not create and cannot cure, but can, when it is paying attention, honour.
That is what this ward tries to do. It does not always succeed. But it keeps trying, one morning round at a time.
All patient names have been changed to protect confidentiality.
The Fragility of Hope
It was a typical Thursday in Sevagram, the kind of day where the heat seems to settle into the very marrow of the hospital’s brickwork. My outpatient department (OPD) was a hive of activity. Around me, medical residents hovered like expectant bees, pens poised over charts, waiting for the clinical wisdom I was supposed to dispense. The waiting hall was a sea of patient faces—anxious, hopeful, and weary. This is the routine of a rural teaching hospital: a constant cycle of healing and instruction.
We like to tell our students that medicine is a science, but in the crowded corridors of the OPD, one quickly learns it is more of an improvisational art. I had just finished a small lecture on the nuances of unexplained fevers when she entered.
She was twenty-four, a mother of two, with eyes that possessed a startling clarity despite the fear that shadowed them. She didn’t offer a greeting or a preamble. She simply said, "I have a hole in my heart. Can you fix it, sir?"
***
She clutched a file that told its own story of rural struggle. It was a battered thing, warped by monsoon rains and heavy handling. Inside were the remains of previous encounters with the medical machine: two handwritten discharge summaries where the ink had begun to bleed into the paper, an ECG strip that looked like a tangled skein of thread, and a damp echo report. Her husband stood behind her, his hands trembling as he urged me to look at the papers.
In the tradition of the best clinicians, I set the file aside. There is a specific kind of arrogance in modern medicine that suggests a machine knows more than a human voice. I wanted to hear her story first. She told me she had been diagnosed with an atrial septal defect—a hole in the heart—after her first child was born. Curiously, she felt fine. No breathlessness, no palpitations. To the casual observer, she was the picture of health.
When I examined her, the heart confirmed what the papers hinted at. There it was: the soft murmur, the wide "split" of the second heart sound. It was the sound of a door left ajar. Her heart was working, but it was inefficient, a mechanical flaw in an otherwise vibrant young woman.
***
The cardiac surgeon we consulted was the embodiment of what patients want in a doctor: calm, steady, and radiating a quiet authority. He looked at the reports and smiled. "It’s a simple hole," he said, with the casual air of a man describing a minor plumbing repair. "The surgery is straightforward. She’ll be home by the weekend."
We all believed him. Why wouldn't we? In the hierarchy of the hospital, the surgeon is the high priest of the tangible. He fixes what is broken. On the day of the surgery, the atmosphere was one of professional focus. The husband paced the hallway, clutching his mobile phone as if it were a talisman. Inside the theater, the heart-lung bypass machine—a marvel of engineering—took over the rhythm of life.
The surgeon worked with the precision of a master craftsman. He found the hole, about the size of a small coin, and began the process of sealing it. "I'll be done in less than three hours," he had said. But three hours became four. Four became five. In a hospital, silence has a different weight when it lasts too long.
***
When the surgeon finally emerged, he was unrecognizable. The mask of confidence had been stripped away, leaving a face pale and etched with exhaustion. His voice, usually so firm, was a mere thread.
"Air got into her brain," he whispered.
It was a mechanical failure—the most pedestrian and devastating kind. The oxygenator had run low on blood. A perfusionist—a human being, prone to the same lapses in concentration as any of us—had missed the drop in levels. Under pressure, a bubble of air was forced into her arteries. It traveled to her brain with the speed of a bullet.
"Her heart is beating," the surgeon said, his eyes glassy, "but her brain is gone."
The tragedy of the "successful" operation that kills the patient is a peculiar medical horror. The hole was closed. The repair was perfect. But the person was gone. The room fell into a heavy, suffocating silence. How do you explain to a man that his wife is dead because of a bubble of air?
***
The husband did not scream or accuse. He collapsed into a chair and wept with a quiet, soul-crushing intensity. The surgeon, to his credit, was honest. He admitted the error. In a moment of heartbreaking grace, the husband blamed destiny rather than the hands that held the scalpel.
The next day, she passed away. We waived the hospital fees and arranged for a vehicle to take her home—gestures that felt not just hollow, but almost insulting in the face of such a loss.
As doctors, we are taught to wear a suit of armor. We are told that "professionalism" means keeping our emotions in a neat, clinical box. If we felt every death, we were told, we could not function. For weeks, I carried this death like a cold stone in my pocket. I studied the literature, I spoke to colleagues, I analyzed the technicalities of air embolisms. I tried to intellectualize the grief away.
***
It didn't work. One evening, weeks later, I was sitting with my wife and my elder sister. We had been laughing, the house was warm, the world felt safe. Then, without warning, the stone in my pocket grew too heavy.
The tears didn't just fall; they erupted. I sobbed with a violence that shocked me. My sister and wife sat frozen, having never seen this version of me. "I lost a young mother," I told them through the gasps. "She had so much hope. And now those two little girls... they'll never know her because of us."
In that moment, the "us" wasn't just the surgical team; it was the entire profession. It was the fallibility of our science and the arrogance of our certainty.
***
Orwell once wrote that to see what is in front of one's nose needs a constant struggle. In medicine, what is in front of our nose is often a person, not a pathology. We cry because we care, and we care because, despite the white coats and the degrees, we are fundamentally fragile.
We return to the wards the next day because we must. We smile at the next patient because they need our hope, even if our own is tattered. But we carry the ghosts of the ones we lost. They sit in the empty chairs of our OPDs; they linger in the silence of the operating theaters.
Medicine is a profession of contradictions. It gives us the power to mend, but it also demands that we witness the unmendable. In the end, we are just humans trying to fix a hole in the world, one heart at a time.
The Captain’s Anchor
"Enough."
It was the only time I heard Mamta Tiwari refuse treatment.
For almost three years she had accepted everything that cancer demanded of her — major surgery, chemotherapy, repeated hospital admissions, drainage tubes into both kidneys, powerful antibiotics, pain, uncertainty, and nearly eighty journeys between Wardha and Mumbai. Each time a new complication arose, I would explain the options and ask, "Shall we go ahead?"
Her answer was always the same.
"Yes."
Then one afternoon in June 2026, she looked at me quietly and said, "Enough."
That single word brought back the story of an extraordinary woman and the family who stood beside her until the very end.
I first heard from her son, Sachin, in November 2025. His email was short and direct. His mother had advanced ovarian cancer. The oncologists at Tata Memorial Hospital had exhausted all treatment options and advised palliative care. While searching for a palliative care centre near Wardha, he came across my name.
He called later that day. The voice on the other end was composed, articulate, and entirely devoid of the panic that usually accompanies such a diagnosis. He asked if he and his brother-in-law could come to Sevagram.
"Come tomorrow at ten," I said.
The next morning he walked into my office carrying a neatly arranged file. He did not bring the usual chaotic bundle of loose papers and poorly labelled reports. He brought a flawless, chronological account of his mother's illness — when the cancer was diagnosed, how it had spread, every operation, every chemotherapy cycle, and what the family hoped to achieve now. By the time he left, I felt I already knew his mother.
A month later, I finally met her.
Mamta Tiwari was sixty-six. She had studied up to the tenth standard. She spoke little, listened carefully, and answered questions without fuss. She had inherited the steel-spined stoicism of her father, a respected police officer in Wardha whose name alone was enough to make local troublemakers straighten up.
At seventeen she married an Army soldier from Pulgaon who later rose to the rank of Captain — a practical, capable man who could strip down a rifle or a motor engine with equal ease. Army life took them across the country: Jalandhar, Sagar, Assam, NEFA, Arunachal Pradesh, Secunderabad, Ranchi, Ambala.
Mamta was the anchor of the family through all of it. She packed up their lives at each new posting and built a home wherever the Army sent them — raising three children in transient cantonments and somehow always finding space to grow vegetables and flowers. When her husband retired in 2005, they returned to Wardha. Later they bought sixteen acres of land near Anji, about twenty kilometres away. Mamta turned the farm into her new garden. Life had come full circle.
Then, in February 2023, her abdomen began to swell.
An ultrasound confirmed a large ovarian tumour. The following day, she and her husband flew to Mumbai.
The next two years were spent travelling between Wardha and Tata Memorial Hospital. When Sachin told me they had made nearly eighty trips, I asked him to repeat the number.
I had heard correctly.
Most journeys were made by the couple alone. They would leave Wardha by taxi for Nagpur airport, fly to Mumbai, spend a day or two in hospital, and return. Many patients find the journey harder than the treatment. Mamta never did.
She never asked, "Why me?"
She wanted the facts, understood the choices, and once she made up her mind she did not look back. There was no theatrical self-pity, no weeping, no bargaining with fate. She stood up to toxic chemotherapy regimens that would have unnerved patients half her age, walked into operating theatres without a flinch, and accepted bilateral drainage tubes into her kidneys without complaint.
By the time she came under our care, the cancer had spread beyond treatment. Our task had changed. We could no longer fight the disease, but we could still relieve pain, control infections, and help her live as comfortably as possible.
I told Sachin that if she needed admission in the middle of the night, he should come directly to the palliative care ward. There was no need to wait in long queues at the casualty department. The paperwork could wait until morning.
Over the next six months she was admitted eight or ten times.
My residents came to know her well. So did the nurses. Every admission followed the same pattern. I would greet her with a namaste. She would smile despite her discomfort. She thanked the nurses for every injection, every dressing, every glass of water. If there was a delay, she waited patiently. She never raised her voice.
In May 2026 she fell at home and fractured a bone. After that, the decline was rapid. The kidney drainage tubes became infected repeatedly. Each infection demanded stronger antibiotics.
Every time I explained the situation, I ended with the same question.
"Shall we continue?"
She would look at me and answer, "Yes."
Sachin would smile gently beside her. "Doctor," he said once, "my mother makes the decisions. We hide nothing from her."
Then came the day she changed her mind.
She had grown weaker. Eating had become difficult. Even speaking took effort. When I suggested another course of antibiotics, she looked at me and said, quietly, "Enough."
There was no anger in her voice. No despair. No fear. Only acceptance.
We stopped trying to prolong life and focused entirely on comfort. Morphine eased her pain. Intravenous fluids were stopped. She took very little by mouth.
I thought she would survive no more than two days.
She lived for another fifteen.
She remained calm almost to the end, surrounded by her family, free from pain, and at peace with her decision. She died in the last week of June 2026.
Doctors often describe the stages through which people respond to terminal illness — denial, anger, bargaining, depression, and acceptance. Real life is rarely so orderly.
Mamta seemed to arrive at acceptance long before her body was ready to leave. She never fought reality. She fought the disease for as long as treatment offered hope. When treatment no longer served a purpose, she let it go.
Patients teach doctors every day. Some teach us medicine. Others teach us something far more difficult.
Mamta Tiwari taught me that courage is not always found in fighting harder. Sometimes it lies in knowing when to stop, accepting what cannot be changed, and allowing death to arrive without fear.
Long after I have forgotten the details of her scans and blood tests, I will remember that quiet afternoon when she looked at me and spoke a single word.
"Enough."
The Midnight Ambulance
The headlights of the ambulance cut through the midnight darkness of our hospital courtyard. In a busy public hospital like ours, midnight arrivals are routine. Sirens wail, stretchers rattle, nurses hurry from one bed to another. We simply move from one emergency to the next.
This ambulance was different.
It had travelled nearly twelve hours from Solapur. Inside lay a thirty-four-year-old man whose lungs no longer worked on their own. A ventilator breathed for him, pushing air into his chest with a steady mechanical rhythm.
When I told my residents that a patient on a ventilator was being brought from so far away, they looked at me in disbelief.
"On a ventilator? From Solapur?" one of them asked.
None of us had seen such a journey before.
When the rear doors opened, I understood why everyone had taken the risk.
His name was Datta.
Datta had studied up to Class XII and came from a small village in Nandura taluka of Buldhana district. As a teenager, he found a clerical job at Shri Sant Gajanan Maharaj College Of Engineering in Shegaon and stayed there for the rest of his working life. His days followed a familiar routine. That summer, he and his wife planned their first pilgrimage to Pandharpur. Like thousands of other devotees, they looked forward to offering prayers to Lord Vitthal and Rukmini.
They never reached the temple.
Soon after arriving in Pandharpur, Datta noticed that his legs felt unusually heavy. By evening they had become weak. He blamed the long bus journey. Before midnight he could no longer stand. A few hours later he began gasping for breath.
His frightened wife rushed him to a nearby hospital.
The doctors quickly recognised Guillain-Barré syndrome, a rare illness in which the body's own immune system attacks the nerves. The weakness spread with frightening speed. Within a day, Datta was completely paralysed. His breathing muscles also failed.
He was shifted to a private hospital in Solapur. A tube was inserted into his windpipe, and a ventilator kept him alive.
Days turned into weeks.
The machine never stopped. Neither did the bills.
The doctors explained that recovery, if it came at all, would take months. No one could say whether he would ever walk again. For a college clerk, the cost of treatment was becoming impossible.
At that point, Datta's principal, Mr. Sunil Somani, and his wife, Manisha, stepped in to help. They travelled to Solapur to see him in the intensive care unit. It did not take Mr. Somani long to realise that the hospital bills were mounting rapidly and were far beyond what Datta's family could afford.
Manisha's brother, Govind Rathi from Wardha, knew me well. He called to ask whether we could accept Datta at Sevagram.
I hesitated.
Transporting a patient who depended entirely on a ventilator across western Maharashtra was risky. It was the peak of summer, and the journey to Sevagram would take nearly twelve hours. A mechanical problem, a power failure in the ambulance, or even a delay on the highway could prove disastrous. Our hospital had an excellent intensive care unit, but we were not a specialised neurological centre.
Govind paused before saying quietly, "They have nowhere else to go."
I agreed.
When Datta arrived that night, he could not move a single muscle below his neck. Not a finger. Not a toe.
The tube in his windpipe had silenced his voice. He answered every question with his eyes.
His wife stood beside the bed without saying a word.
For the next three weeks, Datta remained in our intensive care unit.
Patients who stay on ventilators for long periods often develop pneumonia or overwhelming infections. Every morning we looked anxiously at his chest X-ray and blood tests.
His lungs stayed remarkably clear. Yet his muscles did not.
Nothing changed.
Eventually we faced another problem. The ICU beds were needed for patients with fresh emergencies. We decided to shift Datta to our palliative care ward.
At first glance, it seemed an odd decision. The ward mostly cared for patients with advanced cancer or severe strokes. Yet it offered something the ICU never could—silence.
There were no alarms every few minutes. No rush. No crowd around the bed.
Every day our nurses and residents sat with him. They spoke to him even when he could not answer. They held his hand. They encouraged him through blinks and nods.
"These days will pass, Datta," they would tell him.
Throughout this time, his wife listened quietly.
Neither of them ever asked for another opinion. They never insisted on moving to Mumbai or Nagpur. They simply trusted us and waited.
Six weeks after he had reached Sevagram, something changed.
One morning a nurse noticed the toes of his right foot move.
The next day he could lift his foot.
Soon he was able to raise his hands.
The recovery was slow, almost too slow to notice from one day to the next. But week after week, strength returned.
When he finally left the hospital, he was still in a wheelchair. Yet he was going home.
Over the next six months, my phone came alive every week.
Datta would send me a short video.
In the first, he was sitting without support. Then he was standing with a walker. Later he was taking a few careful steps. A few weeks afterwards he climbed a staircase.
The last video made everyone in our ward smile.
Datta was riding a bicycle through the streets of Shegaon.
The nurses gathered around my phone. Residents who had cared for him months earlier watched the video again and again. They had seen him arrive without the ability to move a finger. Now he was balancing effortlessly on two wheels.
Nearly two years later, Bhavana and I happened to be travelling near Shegaon. We decided to visit Datta before going to the Gajanan Maharaj Temple.
When I called him, he could hardly contain his excitement. He immediately shared the news with his principal, Mr. Sunil Somani. A few minutes later, while we were driving from Jalgaon to Wardha, Manisha Somani telephoned us. "Please come to our home first," she said warmly. Datta's house was directly opposite theirs.
Mr. Somani welcomed us with great affection. Datta, his wife, and their young son were waiting for us. We spent more than an hour talking about those difficult months that had changed all our lives.
At one point, the conversation faded into silence.
Datta's wife quietly wiped away her tears.
Before we left, Datta smiled and said, "Doctor, I never had the chance to see Lord Vitthal in Pandharpur. But perhaps he was with me all along."
I have often thought about his words.
Over the years, we treated many patients with Guillain-Barré syndrome. Some recovered completely; others did not. Datta received no special treatment that others did not receive.
What set his story apart was something else: a principal who refused to abandon his employee, a wife who never left her husband's side, nurses who found time to sit quietly by his bed, and a young man who refused to surrender even when he could speak only with his eyes.
Whenever I think of Datta, I am reminded that medicines are only one part of healing. Hope, courage, and the support of those around the patient matter just as much.
Stetho in Sevagram
Dr SP Kalantri
MGIMS, Sevagram, Wardha
books.kalantri.co.in